Recurrent UTIs and cystitis symptoms in women - RACGP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Focus | Clinical
Recurrent UTIs and
cystitis symptoms
in women
Karen McKertich, Uri Hanegbi URINARY TRACT INFECTIONS (UTIs) are an Complicated UTIs occur in women
extremely common problem in women who have underlying abnormalities of
and are a cause of great personal morbidity their urinary tract anatomy or physiology
Background
Recurrent urinary tract infections (rUTIs)
as well as cost to the health system. While (Table 1). Women with complicated rUTIs
and recurrent cystitis symptoms without an occasional UTI is simple to treat, require referral for further assessment.
infection occur commonly in women and recurrent UTIs (rUTIs) and cystitis with
present frequently in general practice. variable or negative urine cultures are
a complex diagnostic and therapeutic Definitions of UTI
Objective
The aim of this article is to provide
challenge. In this article, the term ‘cystitis’ Controversies exist regarding the
a management approach to the is defined as irritative voiding symptoms bacteriological definition of UTI. In 1960,
assessment and treatment of recurrent that are related to infection, non-infective Kass defined significant bacteriuria as
cystitis symptoms in women with rUTIs inflammation and symptoms in the >105 CFU/mL,3 but it is now recognised
as well as women who have negative absence of bladder inflammation. that in symptomatic women, E. coli counts
urine cultures. of >102 CFU/mL can accurately confirm
Discussion bladder bacteriuria.4 The dilutional effect
Five common clinical scenarios are Classification of UTIs in women of a high fluid intake at the time of UTI
discussed with different approaches to An rUTI is defined as ≥2 episodes of UTI on the accuracy of culture results and
treatment: true rUTIs with positive urine within six months or ≥3 or episodes of concentration threshold for UTI is not
cultures, women with variable urine
UTI within 12 months with the isolation well understood. E. coli in mixed flora in
cultures (some positive and some
of >103 CFU/mL.1 midstream urine (MSU) is also predictive
negative), women with negative urine
cultures who have pyuria +/– haematuria, of bladder bacteriuria in symptomatic
women with completely normal urine Non-complicated versus women and should not be considered
cultures and women with ongoing complicated UTIs a contaminant.4 This finding merits
symptoms after a definite UTI. Red flags UTIs can also be categorised as treatment in symptomatic women.
signalling the need for early referral to complicated or non-complicated. The aim Asymptomatic bacteriuria is the term
a urologist for further assessment are
of investigations is to define and correct used when the standard urine culture
discussed. Both non-antibiotic and
antibiotic-related strategies to treat
complicating factors that predispose to detects a uropathogen >105 CFU/mL
women with rUTIs are available. recurrence of UTIs. in an individual with no lower urinary
In general, an episode of acute tract symptoms.
non-complicated UTI occurs in an otherwise The importance of the MSU in
healthy, non-pregnant woman who is not rUTIs cannot be underestimated. The
known to have an abnormality in her urinary MSU defines whether the patient has
tract (Table 1). The most common cause of a bacterial UTI as opposed to other
acute uncomplicated cystitis is Escherichia potential causes of cystitis (Table 2)
coli in 70–95% of cases.2 and is also fundamental to ensure
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 4, April 2021 199Focus | Clinical Recurrent UTIs and cystitis symptoms in women
optimal and accurate treatment with assessment and management of rUTIs.6 simple non-invasive test such as renal
the appropriate antibiotic. The results of urine cultures confirm the ultrasonography will identify the small
diagnosis, provide antibiotic sensitivities, proportion of women who have an
allow targeted treatment of the UTI, anatomical abnormality.
Five common clinical scenarios confirm whether the treatment approach Women who fall outside the
of ‘cystitis’: Is it a recurrent UTI? is effective and guide choice of antibiotics category of uncomplicated rUTIs
Cystitis refers to irritative voiding for prophylaxis. A lack of correlation (Table 1) and who have a suspicion of
symptoms (dysuria or pain after between MSUs and the clinical diagnosis complicating factors should have renal
micturition), frequency, urgency, cloudy also raises a red flag to consider alternative tract imaging commencing with renal
or offensive urine and discomfort or pain diagnoses (Box 1). tract ultrasonography, which provides
in the bladder, urethra or vagina. It is recommended that each UTI information about both the kidneys and
There are five clinical scenarios episode is clinically evaluated as a separate bladder emptying.
that general practitioners (GPs) face event requiring culture, with consideration
when treating women with cystitis, given to a catheterised specimen if a Cystoscopy
each requiring a specific approach to question of contamination of the urine Cystoscopy can be performed under local
diagnosis and management (Figure 1): specimen is raised by a high epithelial anaesthesia as an ambulatory procedure
1. Women with confirmed rUTIs cell count.6 in the urologist’s rooms or under general
(positive urine cultures) anaesthesia.
2. Women with symptoms of cystitis Urinary tract imaging Cystoscopy is of low yield in the index
with variable urine cultures (both While investigations in an otherwise patient (an otherwise healthy adult
positive and negative urine cultures) healthy women with uncomplicated non-pregnant premenopausal woman)7
3. Women with symptoms of cystitis rUTIs have a low diagnostic yield,6 a with uncomplicated rUTIs but should be
and negative urine cultures with
microhaematuria +/– micropyuria
4. Women with symptoms of cystitis Table 1. Complicating factors in urinary tract infection
with normal urine cultures (no pyuria Structural abnormalities Congenital • Vesicoureteral reflux
or haematuria) of the urinary tract • Pelviureteric junction obstruction
5. Women with ongoing symptoms after • Polycystic kidney disease
a definite UTI (positive urine culture)
Obstruction • Calculi – renal, ureteric or bladder
who now have a negative urine culture.
• Bladder outlet obstruction
• Ureteric/urethral stricture
1. Women with confirmed recurrent Neoplastic • Bladder tumour
UTIs (positive urine cultures) Functional • Urinary tract instrumentation
A. Assessment of women with • Foreign body eg urethral catheter,
confirmed recurrent UTIs ureteric stent
History • Intermittent self-catheterisation
The acute onset of dysuria and frequency • Urinary diversion
in a young woman in the absence of • Urinary or faecal incontinence
concomitant vaginal irritation or vaginal • Poor bladder emptying/increased
discharge gives a 90% probability of UTI.5 post-void residual
History-taking should elucidate red Neurological • Neurological disease affecting the
flags for rUTIs (Box 1) as well as factors urinary tract eg:
causing complicated UTIs. – multiple sclerosis
– Parkinson’s disease
Physical examination – spinal cord injury
Abdominal and pelvic examination should – peripheral neuropathy
be performed to look for anatomical or – diabetes
functional abnormalities of the urinary General conditions • Pregnancy
tract including atrophic vaginal change • Diabetes
and pelvic organ prolapse.6 • Immunosuppression
• Renal failure
Urine cultures • Renal transplant
Performance of urine cultures when
Demographic factors • Hospital-acquired infection
women are symptomatic is crucial in the
200 Reprinted from AJGP Vol. 50, No. 4, April 2021 © The Royal Australian College of General Practitioners 2021Recurrent UTIs and cystitis symptoms in women Focus | Clinical
considered even in the index patient when
Table 2. Differential diagnosis of cystitis symptoms in women with negative
atypical features are present or the patient
urine cultures
fails to respond to treatment.
Cystoscopy should be considered early in Urinary tract infection • Low bacterial count below the threshold for laboratory
the assessment process for all other patients with false-negative reporting
midstream urine • Low bacterial count due to dilution from high fluid intake
with complicating factors or with red flags
(MSU) test • Specimen interpreted as contaminated
for early referral to a urologist (Box 1).
• Difficult-to-culture urinary pathogen
• Antibiotics taken prior to MSU
Urodynamic studies
Other tests such as a urodynamic study Infectious • Urethritis
are reserved for women in whom other • Sexually transmitted infection eg Chlamydia trachomatis,
diagnoses are considered, including Neisseria gonorrohoea, herpes simplex
neurogenic bladder, and in those at • Vulvovaginitis
high risk of bladder complications from • Cervicitis
previous treatments (eg bladder outlet Dermatological • Atrophic vaginitis
obstruction from previous incontinence • Dermatitis – contact or irritant
surgery and pelvic radiotherapy). • Lichen sclerosus
• Psoriasis
B. General advice for prevention • Other vaginal skin conditions
of recurrent UTIs Non-infectious • Excessive fluid intake
It is recommended that the patient and • Stone eg distal ureteric calculus or bladder calculus
doctor engage in a shared decision- • Overactive bladder syndrome
making process that includes a • Interstitial cystitis/bladder pain syndrome
discussion of the risks and benefits of all • Pelvic floor muscle dysfunction
management options before embarking • Endometriosis
on a management plan tailored to the • Urethritis eg reactive arthritis/Behçet’s disease
individual woman.6
Neoplastic • Bladder cancer – transitional cell carcinoma or carcinoma in
situ of bladder
Increased fluid intake • Renal cancer causing haematuria
While the advice to increase fluid intake • Urethral cancer
to prevent infection is frequently given, • Metastatic cancer
there is little evidence to support it.8 • Adjacent cancer infiltrating bladder
It is, however, a low-cost and low-risk • Vaginal or vulvar cancer
intervention.
Structural – within • Urethral diverticulum
the urinary tract • Periurethral/Skene’s duct cyst
Sexual practices
• Urethral irritation after intercourse
Postcoital voiding – The relationship • Urethral stricture
between intercourse and UTI is • Pelvic organ prolapse – high-grade cystocele or other prolapse
controversial, with variable study
Structural – adjacent • Gastrointestinal tract pathology – diverticulitis, diverticular
findings.9,10 A simple measure such as
to the urinary tract abscess, vesicoenteric fistula
postcoital voiding can be recommended in
• Ovarian tumour
women who note intercourse as a trigger
• Other pelvic mass
for their UTIs.
Contraceptive use – Spermicide or Trauma/Iatrogenic • Ureteric stent
diaphragm contraceptive device usage • Foreign body in the urinary tract related to previous pelvic
surgery eg mesh sling procedure, mesh prolapse repair, suture
should be avoided as these have been
from Burch colposuspension
shown to increase UTI risk.11
• Genitourinary surgery or instrumentation eg urinary catheter
• Pelvic radiation
Risk factors that cannot be changed
• Perineal trauma eg post-intercourse, associated with bike
Genetic predisposition – There is riding or horseback riding
evidence for a genetic predisposition
Medication related • Spermicides
to rUTIs in some women with risk
• Topical deodorants or detergents
factors including age at first infection
• Cyclophosphamide cystitis
ofFocus | Clinical Recurrent UTIs and cystitis symptoms in women
Anatomical factors – A shorter distance year was 0.15 favouring antibiotics.15 Patient-initiated antibiotics (with
between the urethral meatus and anus Another way of stating this is that a prior performance of an MSU) should be
has been shown in some young women woman with a history of rUTIs on considered in a compliant patient with
with rUTIs.13 antibiotic prophylaxis is 6.67 times less appropriate follow-up.
likely to have a UTI in a one-year period.
C. Antibiotic treatment options for The number needed to treat is 1.85. The D. Non-antibiotic treatment options for
women with confirmed recurrent UTIs effect was not well maintained, with women with confirmed recurrent UTIs
Antibiotic prophylaxis is a highly effective two studies showing that UTIs recurred Vaginal oestrogen – The use of topical
way of managing rUTIs. and equalled the placebo arm after vaginal oestrogen in postmenopausal
Three management regimens of prophylaxis was ceased.15 Unfortunately, women helps reduce the rate of rUTIs.
antibiotic usage can be considered in no clear evidence is available on Vaginal oestrogen protects against
women with rUTIs (Table 3).2,14 the optimal duration of continuous colonisation by uropathogens via an
The choice of antibiotic should be prophylaxis, how often it should be increase in protective vaginal lactobacilli.16
based on confirmed urine culture and repeated, the benefits post-prophylaxis, Methenamine hippurate – This has
sensitivity results wherever possible, the threshold number of UTIs for starting a bacteriostatic effect in the urine.
regional antibiotic resistance patterns as prophylaxis or the optimal doses of A Cochrane review in 2012 showed
well as patient preferences and tolerance. different antibiotics. that short-term usage prevented
A Cochrane review of 10 studies In women with rUTIs associated with rUTIs in women without urinary tract
of continuous low-dose antibiotic sexual intercourse, postcoital prophylaxis abnormalities or neuropathic bladder
prophylaxis showed that the relative risk seems to be as effective as daily intake and was well tolerated with few adverse
of clinical recurrence of UTI per patient of antibiotics. effects.17 The recommended dosage
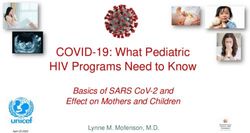
Suspected recurrent UTIs
MSU
Variable cultures some Negative cultures with pyuria Normal MSU with no
Positive cultures
positive/some negative or haematuria pyuria/haematuria
Consider alternative
diagnosis (Table 2)
Any red Yes
Suspect other
flags
pathology (Table 2)
(Box 1)? Refer for imaging and
cystoscopy
No
Ongoing UTIs
Non-antibiotic
prophylaxis
Resolved
Prophylactic antibiotics
Monitor
Figure 1. Management pathway in women with recurrent cystitis
MSU, midstream urine; UTI, urinary tract infection
202 Reprinted from AJGP Vol. 50, No. 4, April 2021 © The Royal Australian College of General Practitioners 2021Recurrent UTIs and cystitis symptoms in women Focus | Clinical
of methenamine hippurate is 1 g twice the marked variability in preparations, Alternative differential diagnoses
daily, but studies have not defined which makes standardisation and for rUTIs (Table 2 and Figure 1) should
optimal duration. comparison difficult. also be more strongly considered and
Cranberry products – The evidence for Vaccines against urinary tract bacteria – investigated for with renal tract imaging
use of cranberry products is conflicting There are various oral, nasal and and cystoscopy.
and may reflect the extreme variability intravaginally administered vaccines that
in products and dosage and lack of have been developed against E. coli. These
standardised regimen. A Cochrane have shown variable efficacy. OM-89 is an 3. Women with symptoms
review in 2008 concluded that cranberry oral preparation of 18 different serotypes of cystitis and negative urine
products could potentially decrease the of heat-killed uropathogenic E. coli. It is the cultures with microhaematuria
frequency of symptomatic UTIs, but a only vaccine recommended in guidelines1 +/– micropyuria
re-analysis with further studies in 2012 as it has been shown to be more effective This group of women has definite bladder/
did not show a significant benefit.18 than placebo in reducing the rate of rUTIs urethral irritation that is less likely to
D-mannose – D-mannose is thought in women in several randomised trials; be due to standard bacterial infection
to have an antibacterial activity by however, its long-term efficacy is unclear. if multiple urine cultures fail to show
inhibiting the adherence of bacteria bacteria. They should not be treated
to urothelial cells and has been shown with multiple courses of antibiotics
in limited randomised prophylaxis 2. Women with symptoms unless other features on their assessment
trials to reduce with the rate of UTI of cystitis with variable urine (eg cystoscopic findings) are suggestive
recurrence in women. Further studies cultures (both positive and of rUTI.
are required before making definite negative urine cultures) The alternative differential diagnoses
recommendations.1 Most of these women have true rUTIs and for rUTIs (Table 2 and Figure 1) must
Probiotics (Lactobacillus spp.) – should be treated as for group 1 (women be more strongly considered including
A recent Cochrane review showed with confirmed rUTIs) but may require urinary tract malignancy, calculus
no convincing benefit of lactobacillus more extensive investigation to ensure that disease such as a vesicoureteric junction
products in the prevention of rUTI.19 structural urinary tract problems (Table 1) calculus and abnormalities of pelvic
Further studies are needed because of are not present. anatomy (eg high-grade pelvic organ
prolapse, urethral diverticulum, other
pelvic pathology).
Box 1. Red flags for early referral to a urologist for further assessment in women As a result of the lack of diagnosis,
with recurrent urinary tract infections and cystitis symptoms these women require further investigations
including upper tract imaging (renal
• Urine cultures and symptoms do not match tract ultrasonography +/– computed
• Persistent haematuria despite adequate control of infections tomography scan) and cystoscopy to
• Persistent sterile pyuria exclude bladder and urethral pathology.
• Ongoing pain
• Persistent bacteriuria despite appropriate antibiotic therapy
• Presence of urea-splitting bacteria (such as Proteus spp. and Pseudomonas spp.) on repeat 4. Women with symptoms of
cultures, which are associated with calculus disease cystitis with normal urine cultures
• A proven bladder or renal calculus on imaging (no pyuria or haematuria)
• Recurrent pyelonephritis In women who have completely normal
• Prior urinary tract surgery, incontinence surgery (eg sling procedure) or urinary tract trauma urine tests with ongoing irritative voiding
• Prior abdominal or pelvic malignancy symptoms, alternative differential
• Prior pelvic radiation diagnoses apart from rUTI must be
• Neurological disease eg spinal cord injury, multiple sclerosis considered (Table 2 and Figure 1),
• Obstructive voiding symptoms eg poor stream, hesitancy, incomplete emptying especially urethral irritation after
• Poor bladder emptying on ultrasonography (especially residuals >150 mL) intercourse, sexually transmitted
• Known renal tract abnormalities that may be contributing to recurrent infection
infections, overactive bladder syndrome,
eg vesicoureteric reflux, high-grade cystocele or prolapse, bladder outlet obstruction bladder hypersensitivity, interstitial
• Immunocompromised patient cystitis/bladder pain syndrome,
• Symptoms of a fistula between bladder and bowel eg pneumaturia (air in urine) or
pelvic floor muscle dysfunction and
faecaluria (faeces in urine) abnormalities external to the urinary tract.
• Women who have not responded to preventive measures Further investigations should be
• When the diagnosis of recurrent uncomplicated urinary tract infection is uncertain considered to rule out bladder, urethral
and functional abnormalities; these
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 4, April 2021 203Focus | Clinical Recurrent UTIs and cystitis symptoms in women
investigations include urinary tract imaging, Conclusion • Women with rUTIs benefit from the use
cystoscopy and urodynamic studies There are many potential causes of of non-antibiotic measures to prevent
depending on the woman’s symptoms. recurrent cystitis symptoms in women infection as well as the considered use
apart from rUTIs. MSU testing provides of antibiotic prophylaxis.
confirmation of bacterial infection in
5. Women with ongoing symptoms women to make the diagnosis of rUTIs. Authors
after a definite UTI (positive urine Both non-antibiotic and antibiotic-related Karen McKertich MBBS, FRACS (Urol), Urological
culture) who now have a negative measures can be used in the treatment Surgeon, Australian Urology Associates, Vic; Cabrini
urine culture of women with rUTIs. Other diagnoses Health, Vic; The Alfred Hospital, Vic
Uri Hanegbi MBBS (Hons), FRACS (Urol), Urological
After a prolonged or particularly must be considered in women with cystitis Surgeon, Australian Urology Associates, Vic; Cabrini
symptomatically severe UTI, some women symptoms and sterile urine cultures, who Health, Vic; The Alfred Hospital, Vic
can have persistent urinary symptoms also warrant further investigation. Competing interests: None.
Funding: None.
due to bladder hypersensitivity, which
Provenance and peer review: Commissioned,
can be associated with pelvic floor externally peer reviewed.
muscle dysfunction. It is hypothesised Key points Correspondence to:
that ongoing pain may be triggered by • Repeated antibiotic treatment of reception@aua.com.au
peripheral sensory and central nervous presumed rUTIs without urine culture
References
system sensitisation.20 should be avoided.
1. Bonkat G, Bartoletti R, Bruyère F, et al. EAU
When ongoing negative urine cultures • Repeat urine testing is important in Guidelines on urological infections. Arnhem, NL:
are confirmed, treatment should focus on establishing the diagnosis and good EAU Guidelines Office, 2020.
2. Expert Group for Antibiotic. Antibiotic choice for
avoidance of further antibiotics, minimising antibiotic stewardship.
urinary tract infection in adults. In: eTG complete
intake of recognised bladder irritants • Early investigation of the urinary [Internet]. West Melbourne, Vic: Therapeutic
such as caffeine, use of medications tract should be considered in women Guidelines Limited, 2020.
3. Kass EH. Bacteriuria and pyelonephritis of
to reduce bladder hypersensitivity with complicated UTIs, women with pregnancy. Arch Intern Med 1960;105:194–98.
(eg low-dose amitriptyline), and pelvic uncomplicated UTIs who have atypical doi: 10.10001/archinte.1960.00270140016003.
floor physiotherapy to treat the abnormally features or who are not responding 4. Hooton TM, Roberts PL, Cox ME, Stapleton AE.
Voided midstream urine culture and acute
high-tone pelvic floor muscles/pelvic floor to treatment, and women with red cystitis in premenopausal women. N Engl
muscle dysfunction. flag features. J Med 2013;369(20):1883–91. doi: 10.1056/
Further investigations can be • It is important to consider diagnoses NEJMoa1302186.
5. Bent S, Nallamothu BK, Simel DL, Fihn SD,
considered if a woman’s symptoms other than rUTIs in women with Saint S. Does this woman have an acute
persist despite these measures. symptoms and negative cultures. uncomplicated urinary tract infection?
Table 3. Antibiotic regimens used for recurrent urinary tract infections2,14
Duration Dosing regimen Antibiotics used Advantages/disadvantages
Continuous low-dose Three to six months Nightly low-dose • Trimethoprim 150 mg orally • Antibiotic side effects
prophylaxis or longer antibiotic at night • Potential antibiotic resistance
• Cephalexin 250 mg orally • Rare adverse reactions to long-
at night term use of nitrofurantoin*
• Nitrofurantoin 50 mg orally
at night*
Postcoital antibiotic Indeterminate Single dose of • As above • Reduces overall antibiotic
antibiotic to be taken usage
within two hours post-
intercourse
Patient-initiated Standard short Therapeutic dose of • Trimethoprim 300 mg daily • Reduces overall antibiotic
treatment (3–5 days) course of antibiotic to be used for three days usage
therapeutic antibiotic after MSU performed • Cephalexin 500 mg 12 hourly • Requires compliance with
for five days MSU testing
• Nitrofurantoin 100 mg six
hourly for five days
*Care must be taken with long-term nitrofurantoin usage because of rare adverse effects such as pulmonary toxicity, hepatotoxicity and peripheral neuropathy2
MSU, midstream urine
204 Reprinted from AJGP Vol. 50, No. 4, April 2021 © The Royal Australian College of General Practitioners 2021Recurrent UTIs and cystitis symptoms in women Focus | Clinical
JAMA 2002;287(20):2701–10. doi: 10.1001/
jama.287.20.2701.
6. Anger J, Lee U, Ackerman AL et al. Recurrent
uncomplicated urinary tract infections
in women: AUA/CUA/SUFU guideline.
J Urol 2019;202(2):282–89. doi: 1097/
JU.0000000000000296.
7. Dason S, Dason JT, Kappor A. Guidelines for the
diagnosis and management of recurrent urinary
tract infection in women. Can Urol Assoc J
2011;5(5):316–22. doi: 10.5489/cuaj.11214.
8. Nygaard I, Kinder M. Thirst at work – An
occupational hazard? Int Urogynaecol J Pelvic
Floor Dysfunct 1997;8(6):340–43. doi: 10.1007/
BF02765593.
9. Kunin CM, Polyak F, Postel E. Periurethral
bacterial flora in women. Prolonged intermittent
colonization with Escherichia coli. JAMA
1980;243(2):134–39.
10. Nicolle LE, Harding GK, Preiksaitis J, Ronald AR.
The association of urinary tract infection with
sexual intercourse. J Infect Dis 1982;146(5):579–83.
doi: 10.1093/infdis/146.5.579.
11. Hooton TM, Scholes D, Hughes JP, et al.
A prospective study of risk factors for
symptomatic urinary tract infection in young
women. N Engl J Med 1996;335(7):468–74.
doi: 10.1056/NEJM199608153350703.
12. Scholes D, Hooton TM, Roberts PL, Stapleton AE,
Gupta K , Stamm WE. Risk factors for recurrent
urinary tract infection in women. J Infect Dis
2000;82(4):1177–82. doi: 10.1086/315827.
13. Hooton TM, Stapleton AE, Roberts PL,
et al. Perineal anatomy and urine-voiding
characteristics of young women with and without
recurrent urinary tract infections. Clin Infec Dis
1999;29(6):1600–01. doi: 10.1086/313528.
14. Australian Medicines Handbook. Anti-infectives-
drug choice for selected infections. Adelaide, SA:
Australian Medicines Handbook, 2020. Available
at https://amhonline.amh.net.au [Accessed
25 February 2020].
15. Albert X, Huertas I, Pereiró II, Sanfélix J,
Gosalbes V, Perrota C. Antibiotics for preventing
recurrent urinary tract infection in non-
pregnant women. Cochrane Database Syst Rev
2004;(3):CD001209. doi: 10.1002/14651858.
CD001209.pub2.
16. Perotta C, Aznar M, Mejia R, Albert X, Ng CW.
Oestrogens for preventing recurrent urinary
tract infection in postmenopausal women.
Cochrane Database Syst Rev 2008;(2):CD005131.
doi: 10.1002/14651858.CD005131.pub2.
17. Lee BS, Bhuta T, Simpson JM, Craig JC.
Methenamine hippurate for preventing urinary
tract infections. Cochrane Database Syst Rev
2012;10(10):CD003265. doi: 10.1002/14651858.
CD003265.pub3.
18. Jepson RG, Williams G, Craig JC. Cranberries
for preventing urinary tract infections. Cochrane
Database Syst Rev 2012;10(10):CD00132.
doi: 10.1002/14651858.CD001321.pub5.
19. Schwenger EM, Tejani AM, Loewen PS. Probiotics
for preventing urinary tract infections in adults
and children. Cochrane Database Syst Rev
2015;(12):CD008772. doi: 10.1002/14651858.
CD008772.pub2.
20. Rosen JM, Klumpp DJ. Mechanisms of
pain from urinary tract infection. Int J Urol
2014;21 Suppl 1(0 1):26–32. doi: 10.1111/iju.12309.
correspondence ajgp@racgp.org.au
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 4, April 2021 205You can also read