Associations between pre-pregnancy obesity and asthma symptoms in adolescents
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research report
Associations between pre-pregnancy obesity and
asthma symptoms in adolescents
Swatee P Patel,1,2 Alina Rodriguez,2,3,4 Mark P Little,2 Paul Elliott,2,5 Juha Pekkanen,6
Anna-Liisa Hartikainen,7 Anneli Pouta,8 Jaana Laitinen,9,10 Terttu Harju,11
Dexter Canoy,12 Marjo-Riitta Järvelin2,10,13
< Additional tables are ABSTRACT indicating that asthma in children is a substantial
published online only. To view Background The high prevalence of children’s asthma disease burden for society.13
these files please visit the
symptoms, worldwide, is unexplained. We examined the The reasons for the rise in asthma are obscure. A
journal online (http://jech.bmj.
com/content/66/9.toc). relation between maternal pre-pregnancy weight and difference in diagnostic criteria over time is one
body mass index (BMI), and asthma symptoms in explanation. Partly for this reason, the Interna-
For numbered affiliations see
end of article. adolescents. tional Study of Asthma and Allergies in Childhood
Methods Data from 6945 adolescents born within the (ISAAC) set up uniform diagnostic criteria.14
Correspondence to Northern Finland Birth Cohort 1986 were used. Research has shown that both genetic suscepti-
Professor Marjo-Riitta Järvelin, Prospective antenatal and birth outcome data, including bility and environmental factors contribute to
Department of Epidemiology maternal pre-pregnancy weight and BMI, and asthma symptoms.15 Genetic predisposition is unlikely to
and Biostatistics, Imperial
College London, Norfolk Place, symptoms in adolescent offspring at age 15e16 years, have changed over such a short period so environ-
London W2 1PG, UK; were employed. Logistic regression analyses were mental factors are more likely to play an important
m.jarvelin@imperial.ac.uk performed to examine the associations between relevant role in the prevalence of asthma symptoms.
prenatal factors and asthma symptoms during The prenatal environment is of special concern
SPP and AR contributed equally
to this work.
adolescence. because disruptions during this critical stage of
Results Current wheeze (within the past year) was development can result in structural and func-
Accepted 13 June 2011 reported by 10.6% of adolescents, and physician- tional disturbances evident in later life. Prenatal
Published Online First diagnosed asthma by 6.0%. High maternal pre-pregnancy exposure to maternal smoking has been found to
15 August 2011 BMI was a significant predictor of wheeze in the contribute to asthma and wheeze in children
adolescents (increase per kilogram per square metre beyond the effect of postnatal environmental
unit; 2.7%, 95% CI 0.9 to 4.4 for ever wheeze; 3.5%, tobacco smoke.16 17 Nonetheless, the rise in chil-
95% CI 1.3 to 5.8 for current wheeze), and adjusting for dren’s asthma symptoms is unlikely to be attrib-
potential confounders further increased the risk (2.8%, utable to a higher prevalence of women smoking
95% CI 0.5 to 5.1; 4.7%, 95% CI 1.9 to 7.7, respectively). during pregnancy as the reverse is generally true in
High maternal pre-pregnancy weight, in the top tertile, most Western societies.15 In contrast, maternal
also significantly increased the odds of current wheeze in weight entering pregnancy has increased dramati-
the adolescent by 20% (95% CI 4 to 39), and adjusting cally in the last decades18 and has been associated
for potential confounders further increased the risk with a number of negative outcomes in infants and
(OR¼1.52, 95% CI 1.19 to 1.95). Results were similar for children.19e22 Two recent cohort studies reported
current asthma. Furthermore, these significant an association between increasing maternal pre-
associations were observed only among adolescents pregnancy body mass index (BMI) (in kilogram per
without parental history of atopy but not among those square metre) and child wheeze.23 24 One study
with parental history of atopy. found the association only for 8-year-olds with
Conclusions The association demonstrated here a prior disposition to asthma23 and the other
between maternal pre-pregnancy overweight and examined symptoms in 18-month-old infants.24
obesity, and asthma symptoms in adolescents suggests Two further US studies showed the relationship in
that increase in asthma may be partly related to the 3-year-olds, but only looked at urban popula-
rapid rise in obesity in recent years. tions.25 26 Therefore, we investigated whether
maternal pre-pregnancy weight and BMI
contribute to the risk of developing asthma
symptoms in light of other prenatal and life course
INTRODUCTION exposures to better understand the nature of the
Prevalence of children’s asthma symptoms has associations. We studied a large cohort born in
increased substantially, worldwide, since the Northern Finland and prospectively followed from
1970s,1e10 although international differences early pregnancy until adolescence. Use of this
between countries have reduced in the last cohort gives a powerful opportunity to examine
decade.11 Up to 37% of teenagers are affected by the associations because the population is homo-
asthma symptoms, making it one of the most geneous and stable over time without any marked
common chronic diseases in childhood.12 Absence increase in environmental pollutants. This
from school and limitations in activities are some of geographical region was encompassed by ISAAC
This paper is freely available
online under the BMJ Journals the common consequences of asthma. In 2004, the studies, which also provided us with the oppor-
unlocked scheme, see http:// estimated cost of asthma symptoms among chil- tunity to monitor possible changes in prevalence of
jech.bmj.com/site/about/ dren in the European Union was V3000 million, asthma symptoms.
unlocked.xhtml
J Epidemiol Community Health 2012;66:809e814. doi:10.1136/jech.2011.133777 809Research report METHODS reported for wheezing, in the main paper (and for asthma in The Northern Finland Birth Cohort 1986 (NFBC1986) consists supplementary tables) to facilitate comparability with other of all births between 1 July 1985 and 30 June 1986 in the two studies. The symptoms are more comparable indicators of northernmost provinces of Finland, Oulu and Lapland, totalling respiratory disorder because of varying diagnostic criteria of the 9432 live births (response rate: 99%). The purpose was to asthma. We performed unadjusted and adjusted analyses, and prospectively study medical and psychological health outcomes. further stratified the data by parental history of atopy to explore The ethics committee of Northern Ostrobotnia Hospital District potential interactions. Covariates in the regression models were approved the study, and both parents and adolescents gave all categorical except for birth weight and adolescents’ BMI at written informed consent. age 15 years (continuous). The severity of adolescents’ wheezing Pregnant women were recruited at their first prenatal visit on in the past year was used in ordinal regression where the cate- the 12th gestational week when a questionnaire on maternal gories were coded as 0¼never, 2¼1e3 times, 8¼4e12 times, demographics, social background, education level, disease 14¼more than 12 times. The analyses were conducted by SP history, and lifestyle including parental smoking was distrib- using SPSS V.18.0. uted. Women returned the form by 24th gestational week if still pregnant. Women reported smoking status for themselves and RESULTS the expectant father. Data from official medical records, recorded At age 15e16 years, the prevalence of ‘ever wheeze’ and ‘current by midwives at first antenatal visit, included maternal pre- wheeze’ was 20.4% and 10.6%, respectively, and prevalence of pregnancy weight, height, and disease history for both parents. ‘ever asthma’ was 11.5% (10.6% when confirmed by a doctor), During the visit, women reported their weight before pregnancy, and 6.0% had ‘current asthma’ (supplementary table 1). The 38% stated their height, but the rest were measured. Pre-preg- association between reported doctor-diagnosed and self-reported nancy BMI before was calculated (in kilogram per square metre). ever asthma was very strong (c2 (1)¼4005.5, p
Research report
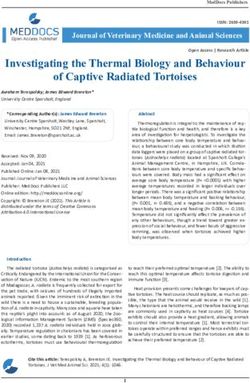
Table 1 Prevalence and unadjusted ORs for adolescents’ wheeze (self-reported) at age 15 years in relation to demographic, adolescent, and parental
factors
Ever wheeze Current wheeze
Population
distribution (%) % OR (95% CI) % OR (95% CI)
Background and demographics
Gender (n¼9065)
Girls (reference) 48.5 22.0 12.2
Boys 51.5 18.7 0.81 (0.72 to 0.91)* 8.9 0.70 (0.60 to 0.82)*
Birth weight, g (n¼9066)Research report
Table 1 Continued
Ever wheeze Current wheeze
Population
distribution (%) % OR (95% CI) % OR (95% CI)
$30 (obese) 3.8 20.9 1.07 (0.78 to 1.48) 14.5 1.52 (1.04 to 2.21)*
Continuous predictor \(% per BMI unit) 2.7% (0.9% to 4.4%) p¼0.002* 3.5% (1.3% to 5.8%) p¼0.002*
Adolescent BMI at age 15 yrs (n¼6669)
Continuous predictor (% per BMI unit) 4.8% (2.9% to 6.6%) pResearch report
Table 3 Adjusted ORs for maternal pre-pregnancy obesity and adolescents’ wheeze at age 15 years, stratified by parental history of atopy
Adjusted* OR (95% CI), p Value
Ever wheeze Current wheeze
Factors No parental atopy Parental atopy No parental atopy Parental atopy
Maternal pre-pregnancy weighty (n¼8874)
First tertile 35e54 kg Reference Reference Reference Reference
Second tertile 55e61 kg 1.27 (0.95 to 1.68), p¼0.10 0.95 (0.74 to 1.22), p¼0.70 1.78z (1.20 to 2.64), p¼0.004 0.97 (0.69 to 1.37), p¼0.88
Third tertile 62e130 kg 1.51z (1.13 to 2.02), p¼0.005 1.02 (0.80 to 1.31), p¼0.87 2.00z (1.34 to 2.98), p¼0.001 1.25 (0.90 to 1.74), p¼0.19
Maternal pre-pregnancy BMI (n¼8838)
19e24.9 (normal) Reference Reference Reference ReferenceResearch report
Funding The study was supported by the grants from the University of Oulu, Finland; 17. Pattenden S, Antova T, Neuberger M, et al. Parental smoking and children’s
Oulu University Hospital, Finland; the Academy of Finland; the European Commission respiratory health: independent effects of prenatal and postnatal exposure. Tob
(Framework 5 award QLG1-CT-2000-01643), and by Medical Research Council, UK. Dr Control 2006;15:294e301.
Rodriguez received support from VINNMER (P32925-1). 18. Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US
adults, 1999-2008. JAMA 2010;303:235e41.
Competing interest None declared. 19. Catalano PM, Ehrenberg HM. The short- and long-term implications of maternal
obesity on the mother and her offspring. BJOG 2006;113:1126e33.
Patient consent Obtained.
20. Cnattingius S, Bergstrom R, Lipworth L, et al. Prepregnancy weight and the risk of
Ethics approval This study was conducted with the approval of the ethics adverse pregnancy outcomes. N Engl J Med 1998;338:147e52.
committee of Northern Ostrobotnia Hospital District. 21. Rodriguez A, Miettunen J, Henriksen TB, et al. Maternal adiposity prior to
pregnancy is associated with ADHD symptoms in offspring: evidence from three
Provenance and peer review Not commissioned; externally peer reviewed. prospective pregnancy cohorts. Int J Obes (Lond) 2008;32:550e7.
22. Rodriguez A. Maternal pre-pregnancy obesity and risk for inattention and negative
emotionality in children. J Child Psychol Psychiatry 2010;51:134e43.
REFERENCES 23. Scholtens S, Wijga AH, Brunekreef B, et al. Maternal overweight before pregnancy
1. Aberg N, Hesselmar B, Aberg B, et al. Increase of asthma, allergic rhinitis and and asthma in offspring followed for 8 years. Int J Obes (Lond) 2010;34:606e13.
eczema in Swedish schoolchildren between 1979 and 1991. Clinic Exp Allergy 24. Haberg SE, Stigum H, London SJ, et al. Maternal obesity in pregnancy and
1995;25:815e19. respiratory health in early childhood. Paediatr Perinat Epidemiol 2009;23:352e62.
2. Burr ML, Butland BK, King S, et al. Changes in asthma prevalence: two surveys 15 25. Reichman NE, Nepomnyaschy L. Maternal pre-pregnancy obesity and diagnosis of
years apart. Arch Dis Child 1989;64:1452e6. asthma in offspring at age 3 years. Matern Child Health J 2008;12:725e33.
3. Peat JK, van-den-Berg RH, Green WF, et al. Changing prevalence of asthma in 26. Kumar R, Story RE, Pongracic JA, et al. Maternal pre-pregnancy obesity and
Australian children. BMJ 1994;308:1591e6. recurrent wheezing in early childhood. Pediatr Allergy Immunol Pulmonol
4. Burney PGJ, Chinn S, Rona RJ. Has the prevalence of asthma increased in children? 2010;23:183.
Evidence from the national study of health and growth 1973-86. BMJ 27. Davidson R, Roberts SE, Wotton CJ, et al. Influence of maternal and perinatal
1990;300:1306e10. factors on subsequent hospitalisation for asthma in children: evidence from the
5. Ninan TK, Russell G. Respiratory symptoms and atopy in Aberdeen schoolchildren: Oxford record linkage study. BMC Pulm Med 2010;10:14.
Evidence from two surveys 25 years apart. BMJ 1992;304:873e5. 28. Gale CR, Javaid MK, Robinson SM, et al. Maternal size in pregnancy and body
6. Robertson CF, Heycock E, Bishop J, et al. Prevalence of asthma in Melbourne composition in children. J Clin Endocrinol Metab 2007;92:3904e11.
schoolchildren: changes over 26 years. BMJ 1991;302:1116e18. 29. Figueroa-Munoz JI, Chinn S, Rona RJ. Association between obesity and asthma in
7. Toelle BG, Ng K, Belousova E, et al. Prevalence of asthma and allergy in 4-11 year old children in the UK. Thorax 2001;56:133e7.
schoolchildren in Belmont, Australia: Three cross sectional surveys over 20 years. 30. von Mutius E, Schwartz J, Neas LM, et al. Relation of body mass index to asthma
BMJ 2004;328:386e7. and atopy in children: the National Health and Nutrition Examination Study III. Thorax
8. Goren AI, Hellman S. Changing prevalence of asthma among schoolchildren in Israel. 2001;56:835e8.
Eur Respir J 1997;10:2279e84. 31. Shaheen SO, Sterne JAC, Montgomery SM, et al. Birth weight, body mass index
9. Asher MI, Montefort S, Bjorksten B, et al. Worldwide time trends in the prevalence and asthma in young adults. Thorax 1999;54:396e402.
of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC 32. Domali E, Messinis IE. Leptin in pregnancy. J Matern Fetal Neonatal Med
Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2002;12:222e30.
2006;368:733e43. 33. Hendler I, Blackwell SC, Mehta SH, et al. The levels of leptin, adiponectin, and
10. Shaw RA, Crane J, O’Donnell TV, et al. Increasing asthma prevalence in a rural New resistin in normal weight, overweight, and obese pregnant women with and without
Zealand adolescent population: 1975-89. Arch Dis Child 1990;65:1319e23. preeclampsia. Am J Obstet Gynecol 2005;193:979.
11. Pearce N, Ait-Khaled N, Beasley R, et al. Worldwide trends in the prevalence of 34. Gnanalingham MG, Mostyn A, Gardner DS, et al. Developmental regulation of
asthma symptoms: phase III of the International Study of Asthma and Allergies in the lung in preparation for life after birth: hormonal and nutritional manipulation
Childhood (ISAAC). Thorax 2007;62:758e66. of local glucocorticoid action and uncoupling protein-2. J Endocrinol
12. ISAAC Steering Committee. Worldwide variation in prevalence symptoms of 2006;188:375e86.
asthma, allergic rhinoconjunctivitis and atopic eczema: ISAAC. Lancet 35. Hersoug SG, Linneberg A. The link between the epidemics of obesity and allegic
1998;351:1225e32. diseases: does obesity induce decreased immune tolerance? Allergy
13. van den Akker-van Marle JM, Bruil J, Detmar SB. Evaluation of cost of disease: 2007;62:1205e13.
assessing the burden to society of asthma in children in the European Union. Allergy 36. Jaakkola JJ, Jaakkola MS. Effects of environmental tobacco smoke on the
2005;60:140e9. respiratory health of children. Scand J Work Environ Health 2002;28:71e83.
14. Asher MI, Keil U, Anderson HR, et al. International Study of Asthma and Allergies in 37. Jaakkola JJ, Gissler M. Maternal smoking in pregnancy, fetal development, and
Childhood (ISAAC): Rationale and methods. Eur Respir J 1995;8:483e91. childhood asthma. Am J Public Health 2004;94:136e40.
15. Peat JK, Mellis CM. Early predictors of asthma. Curr Opin Allergy Clin Immunol 38. Haahtela T, Tuomisto LE, Pietinalho A, et al. A 10 year asthma programme in
2002;2:167e73. Finland: major change for the better. Thorax 2006;61:663e70.
16. Lannero E, Wickman M, Pershagen G, et al. Maternal smoking during pregnancy 39. ISAAC Steering Committee. Worldwide variations in the prevalence of asthma
increases the risk of recurrent wheezing during the first years of life (BAMSE). Respir symptoms: the International Study of Asthma and Allergies in Childhood (ISAAC). Eur
Res 2006;7:3. Respir J 1998;12:315e35.
PAGE fraction trail=5.75
814 J Epidemiol Community Health 2012;66:809e814. doi:10.1136/jech.2011.133777You can also read