Reduction of adverse effects from intravenous acetylcysteine treatment for paracetamol poisoning: a randomised controlled trial.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Reduction of adverse effects from
intravenous acetylcysteine treatment for
paracetamol poisoning: a randomised
controlled trial.
The Scottish and Newcastle Anti-emetic Pre-treatment for
Paracetamol Poisoning Study (SNAP).
James Dear
on behalf of the SNAP investigators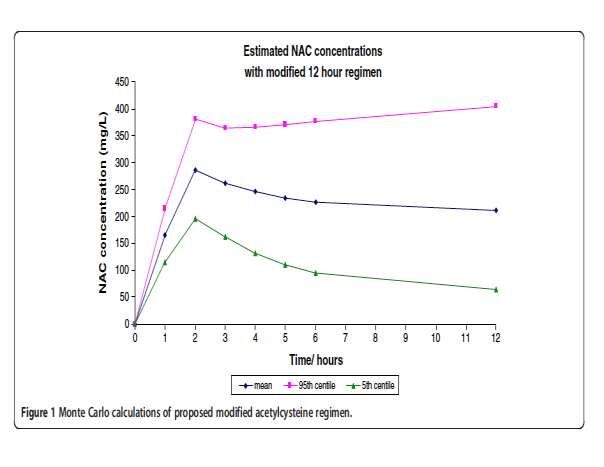
Paracetamol Toxicity •Commonest cause of acute liver failure in Europe and USA •Commonest single enquiry to Poisons Information Services in UK and USA •England 38,000 admissions 2011-12 Scotland ~ 8,000 admissions/annum
Hospital Episode Statistics
2010-11
Reason for admission Emergency admissions (England)
Paracetamol 38,464
Fracture of neck of femur 42,616
Congestive heart failure 37,148
Acute myocardial infarction 26,967
Acute exacerbation of COPD 44,969Mechanism of paracetamol hepatotoxicity
Oxidation by cytochrome
P450 enzymes – a minor route
in therapeutic doses
Paracetamol NAPQI
Conjugation – Reacts with SH-
the major route group in
of metabolism in glutathione
therapeutic dose
Paracetamol
conjugates
NAPQI
conjugateMechanism of paracetamol hepatotoxicity
Excess NAPQI binds to SH-
In overdose, oxidation by groups in structural protein
cytochrome P450s becomes
important
Paracetamol NAPQI SH-
Conjugation –
saturated in
overdose
Paracetamol
conjugates Glutathione supply
exhausted
NAPQI
conjugate
AcetylcysteineLancet 1977 BMJ 1979
Lancet 1979
ADRs to acetylcysteine and paracetamol
concentration at presentation (n=362)
Waring et al. Clin Tox 2008; 46: 496-500.Current problems with
acetylcysteine
• Complex regimen causes medication errors
• ADRs common
– Treatment interruption
– Treatment refusal
– Treatment denial (mistaken for true anaphylaxis)
• Time consuming
Ferner et al BMJ 2011,342:d2218The hypotheses 1. A modified regimen of acetylcysteine will reduce rates of anaphylactoid response 1. Pre-treatment with an anti-emetic will reduce N and V. Ondansetron chosen
Prescott et al. EJCP 1989; 37:501-
506
Thanacoody et al.
BMC Pharm Tox
2013; 14, 20TRIAL TREATMENTS Acetylcysteine- matching duration of infusions Conventional 20.25 h acetylcysteine regimen 150mg/kg in 200mL, 15 min; 50mg/kg in 0.5L, 4 h ; 100mg/kg in 1 L, 16 h (British National Formulary 2009) Modified 12 h acetylcysteine regimen 100mg/kg in 200 mL, 2h; 200mg/kg 1L, 10h infusion; followed by 0.5L 5% dextrose to 20.25 h for matching Ondansetron 4mg IV Pre-treatment with ondansetron v saline placebo
At least 80% power to detect a relative risk of 0.6 for the proportion of patients with vomiting within 2 hours . Requires 91 patients enrolled on ondansetron and 91 on placebo (significance level=0.025). 1:1:1:1 treatment allocation Aimed for 50 excess patients to account for drop outs
Matching: Minimisation program for treatment randomisation • Stated dose < 16g or 16g and over • Time to presentation < or > 8h • Risk factors for paracetamol toxicity – Chronic excess alcohol – Malnutrition – Debilitating disease – Enzyme inducing drugs
ENDPOINTS
The primary endpoint was:-
Absence of vomiting/retching or need for rescue
antiemetic at 2 h
(also assessed at 12 h)
Secondary endpoints included:-
i) Symptoms of anaphylactoid response, need for rescue
therapy or treatment interruption
ii) Hepatic toxicity: ALT (increase of >50% from baseline;
ALT >1000): INR (>1.3): miR-122Patients Screened Patients not requiring NAC treatment 1772
3311 (57.4% of screened)
Exclusion: Fulfil exclusion criterion or other reason
for non-participation:
490 staggered OD
Patients potentially 146 intoxicated, unable to consent
requiring NAC 116 presented beyond recruitment interval
90 unreliable history
1539 69 vomiting requiring antiemetic prior to randomisation
60 patient refused
(42.6% of screened) 57 previous participant in SNAP
89 other pre-specified exclusiona
53 other reasons (eg self-discharged) Total 1170
No clinician available to consent
Eligible 369 147
Failed to complete or withdrawn, time and
allocation
Randomised 222 4 before 2h (1 ond/mod, 1 ond/conv,
2plac/con)
(67% of eligible )
8 after 2h; 2 in each arm)
2 after 4h (ond/conv)
Included in 1ry 5 after 12h (1 ond/mod; 2 ond/ conv; 2 plac/
mod)
endpoint 217
Trial ran Sept 2010- Dec 31 2012
Completed Trial
203Assessments Clinical records of vomiting and retching, BP (fall of > 20 mm Hg systolic) and pulse (rise of > 20 bpm) Use of rescue therapy:- cyclizine for vomiting, symptomatic therapy for anaphylactoid reactions Self scored Likert scales:- Nausea, flushing, itchy skin, skin rash, chest pain, feeling breathless, feeling wheezy and tongue/lip swelling (positive 5 and over on 11 point scale) Hepatic Injury from lab results at end treatment
Baseline characteristics
Acetylcysteine Regimen Ondansetron
Modified Conventional Active Placebo
Randomised, n (%) 110 (100) 112 (100) 111 (100) 111 (100)
Ingestion to treat 64 (58.2) 64 (57.1) 65 (58.6) 63 (56.8)
< 8 h, n (%)
Age (y) (median, 32 (22-47 32 (22-45) 30 (21-44) 35 (26-47)
IQR)
Weight kg (median, 70 (60-84) 68 (60-80) 68 (57-83) 70 (62-80)
IQR)
Females, n (%) 64 (58.2) 67 (59.8) 65 (58.6) 66 (59.5)
Ingested 229 (167-328) 244 (184-357) 224 (167-327) 243 (169-353)
paracetamol
(median, IQR)
mg/kg
Any risk factor 51 (46.4) 52 (46.4) 50 (45) 53 (47.7)
present (%)Primary outcome:
Number of patients who did not vomit or
retch or take rescue medication at 2 h
Comparison Treatment Number Total Odds 97.5% confidence P-value
Group with 1ry number Ratio interval
outcome
NAC Regimen Conventional 38 109 0.260 0.130 to 0.518Absence of use of antiemetic rescue. Kaplan Meier analysis to 12 h
Pre-defined anaphylactoid
response severity
(based on World Allergy Association Classification)
Grade 1. A positive response in one of the domains on the
Likert scales, or change in blood pressure or pulse rate as
defined (> 20 mmHg BP systolic fall, >20 BPM rise).
Grade 2. Two or more positive symptom domains on Likert,
and/ or cardiovascular changes (BP, pulse), but no requirement
for specific treatment, or stopping NAC therapy.
Grade 3. Patients who had NAC treatment discontinued and/ or
an intervention with anti-allergy therapy.Anaphylactoid responses
(as proportion of all patients)
Overall responses
Grade 1 (1 domain) 79/208 (38%)
Grade 2 (2 domains) 18/208 (8.7%)
Grade 3 (rescue or interruption) 36/208 (17%)Anaphylactoid reaction:
Grade 3 responses – interruption or medication
(proportional odds regression)
Comparison Treatment Number Total Odds 97.5% P-value
Group with number Ratio confidence
outcome interval
NAC Modified 5 108 0.2 0.1-0.4Anaphylactoid responses- time to 1st use of rescue medication. Kaplan Meier analysis to 12 h
Hepatic Efficacy
50% rise in ALT at 20.25 h
Present in 22/201 (10.9%)
NAC modified v conventional OR 0.603, 97.5% CI 0.199-1.831
Ondansetron v placebo OR 3.295, 97.5% CI 1.013-10.723,
P = 0.0235
Other endpoints
ALT >1000 IU/L in 5/202 INR >1.3 in 25/201 NSOther hepatic markers miR-122 in subset Edinburgh patients (124) (median and IQR) NAC modified 1.1 (0.4-2.4) v conventional 0.5 (0.2-3.4) p = 0.789 Ondansetron 1.3 (0.4-3.4) v placebo 0.6 (0.2-2.0) p = 0.03 Doubling ALT (19/201) NAC modified (10) v conventional (11) OR 0.653 97.5 % CI 0.195-2.183 p=0.4283 Ondansetron (14) v placebo (5) OR 3.474, 97.5%CI 0.95-12.66 p=0.0309 Extra acetylcysteine beyond 20.25 h in 17 patients NAC regime, OR 2.2 (97.5% CI 0.6 to 7.8) P=0.18 Ondansetron, OR 0.4 (97.5% CI 0.1 to 1.3) P=0.08
Caveats • Large numbers of exclusions, in particular staggered overdose • Acetylcysteine not blinded but patient information on vomiting not anaphylactoid • Not powered to detect non-inferiority in hepatic outcomes
Conclusion 1
• A modified NAC regimen is associated with significant
reduction in both nausea and vomiting, and
anaphylactoid responses
• As a result significantly less interruptions to treatment
(4% v 30%)
• Ondansetron reduces nausea and vomiting, but does
not alter rates of anaphylactoid responses. It is
associated with a rise in ALT and miR-122 suggesting
hepatic toxicity in association with paracetamol OD.
• Hepatic outcomes are insufficiently powered, but
there was no indication of inferiority with the
modified regimen as judged by ALT or miR-222.Conclusion 2 • It is possible to do multi-centre clinical trials in poisoning in Europe, drop outs and refusals were low • The simpler shorter acetylcysteine regimen, linked to newer approaches of assessing risks of hepatic injury offers potential for reducing hospital length of stay and reducing medication errors
CONTRIBUTORS
•Edinburgh Clinicians • Site Co-ordinators
Nick Bateman Andrea Bell
James Dear Paul Hindmarsh
Michael Eddleston Jane Sheran
Alasdair Gray
Euan Sandilands •Research Nurses
Aravindan Veiraiah Margaret Dow
David Webb Moyra Masson
Janice Pettie
•Newcastle Clinicians
Simon Thomas •Statisticians
Ruben Thanacoody Steff Lewis
Simon Hill Aryelly Rodriguez
John Wright Izzy Butcher
•Aberdeen Clinicians •DMC
Angus Cooper Robin Ferner
Jamie Cooper Janine Grey
Kenneth Simpson
•Central Trial Management
Judy Coyle •FUNDING
Edinburgh Clinical Trials Unit CSO ScotlandYou can also read

















































