Reflections of COVID-19 - CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE Summer 2020 - Chartered Physiotherapists working ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Summer 2020
Reflections of COVID-19
Agility Summer 2020 Contents EDITORIAL ..............................................................................................................................................................1 Abi Hall – Agility Editor AGILE NATIONAL EXECUTIVE OFFICERS ................................................................................................................2 PRESIDENT’S ADDRESS...........................................................................................................................................3 Joyce Williams, AGILE Honorary President CHAIR’S ADDRESS ..................................................................................................................................................4 Sarah De Biase - AGILE Chair (2019-2021) GUIDELINES FOR POTENTIAL AUTHORS ..............................................................................................................5 INPATIENT OLDER ADULTS THERAPY SERVICE - EMBRACING CHANGE THROUGH COVID-19 ........................6 Beth Sykes, Clinical Specialist Physiotherapist for Older People INTO THE UNKNOWN - PERSONAL REFLECTIONS DURING COVID-19..............................................................8 Elizabeth Booth & Hannah Wood, Advanced Physiotherapists WORKING ON AN ACUTE MEDICAL WARD DURING COVID-19.......................................................................12 Kerry Hunt, Complex Care Physiotherapy Team Lead EVOLUTION OF THE ROLE OF PHYSIOTHERAPY IN A CARE HOME DURING THE COVID-19 PANDEMIC: A VIEW FROM THE FRONT LINE ............................................................................14 Susanne Syme, Private practitioner CARE HOME RESIDENTS AND ASSESSMENTS IN THE FACE OF COVID-19 ........................................................19 Amy Souster, Senior Physiotherapist FROM RESEARCH TO ICU – REFLECTIONS OF REDEPLOYMENT ........................................................................20 Matthew Prescott - Physiotherapist & HERO Trial Manager COVID 19 – FROM THE EXPERIENCES OF A RESEARCH MANAGER....................................................................23 Kathryn Bamforth, Doctoral Research Fellow Clinical Research Team Leader EXPERIENCING COVID-19 AS A STUDENT ..........................................................................................................24 Caroline Williamson, Physiotherapy Student A STUDENT’S EXPERIENCE OF COVID-19............................................................................................................25 Leesha Aileen Naisbitt, University of Huddersfield WORKING WITHIN AN OLDER PEOPLE’S MENTAL HEALTH SERVICE DURING COVID-19 ...............................26 Heidi Thomas, Highly Specialist Physiotherapist, Older Peoples Community Mental Health JOURNAL REVIEW .................................................................................................................................................29 Rachel Malthouse, Physiotherapist & Hilary Gunn, Associate Professor in Physiotherapy Data Protection Act Members’ details are held on a computer database. Questionnaires may be sent by students undertaking dissertations – this will be via the membership secretary. The database address list may also be provided to a third party if the National Executive believe it would be beneficial to members’ interest in older people. Please write to the membership secretary if you do not want your details disclosed in either of these circumstances. Copyright The material in this Journal is copyright to Agility and may not be published in another journal without the permission of the editor. Authors will be advised of any requests to reprint their articles in other journals. Opinions expressed in this Journal are not necessarily those of the Editor of Agility, AGILE or the publisher. i CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Agility Summer 2020
Editorial
Agility Editor: Abi Hall @abijhall
Welcome to the “Agility: reflections of COVID-19” a useful experience. I hope it also breaks down the
edition for summer 2020. As my first edition as Editor barriers of clinicians “fearing” writing for journals.
I had various exciting (I thought) plans, but like for the As a clinician, I always felt that it was something that
whole of the world, COVID-19 intervened. It seemed researchers did – but actually, often articles from
only appropriate to reflect this in the topic for Agility clinicians are the most powerful. I really hope you all
this summer and use this as an opportunity to gain a go on to write more!
deeper understanding about how our profession has
We start our exploration of COVID-19 from
experienced this pandemic. Therefore, this edition
physiotherapists working in acute settings. The challenges
focuses solely on COVID-19 and aims to explore
ranging from wearing PPE to completely changing the
different perspectives of the pandemic as well as to
status and purpose of wards are clear. We then move
realise what positive things have been learnt. This
to the community and have two contributions from
edition will be much less “academic” than you would
physiotherapists who work in care homes. The plight
perhaps be expecting, but in such times I hope the
of care homes has been widely documented, so these
types of article will have a deeper meaning to you all.
reports offer some fascinating insight into working
Before I introduce the articles, I’ll briefly introduce within this setting. We then have contributions from two
my experiences. As a clinical lead physiotherapist in a physiotherapists who, prior to COVID-19, were working
community rehabilitation cluster, I experienced having in research roles. The redeployment from such roles into
to completely change our service, our practice, our frontline services is fascinating to hear.
patients and focus solely on urgent response to try and
Students are vital to our profession moving forwards
get patients home and prevent people being admitted
and therefore I felt it was important to understand how
wherever we could. I can only say how fortunate we
they have experienced the pandemic. I don’t think
have been in the South West and so far, we have had
anybody, experienced or not, could have prepared for
low levels of cases. Despite this, it was certainly a
the pandemic, so their viewpoint offers a real insight.
challenging time and I reflect on the hardest period
Last, but certainly not least, our final clinical report is
of my career, not due to the expected overwhelming
relating to mental health. All of our contributors have
demand of our service, but more the responsibility I felt
referenced mental health, so it felt appropriate to round
having to ask my team to put themselves at risk, when all
off our clinical experiences with an insight into working
I really wanted to do was tell them to stay at home and
in mental health settings during this time. What has
stay safe. The fear of sending them into the unknown
also been highlighted by our contributors has been the
will live with me for a long time. However, despite this,
development of new ways of working, including using
my predominant feeling, when I reflect on the last few
more virtual means of treatment. Therefore, it felt only
months, is what a truly remarkable response there was
appropriate that our journal review this edition focused
from the teams I lead. I won’t name them, they know
on this. Virtual treatments are being used much more
who they are, but every member of each team adapted
readily than ever before in an attempt to reduce face to
in a way that I didn’t know we could and for that I will
face contacts with patients and therefore research into
forever be grateful – and immensely proud.
the effectiveness of such technologies will play a vital
Now onto the experiences of our contributors. First role in the development of our profession.
we hear from AGILE’s Honorary President, Joyce, who
I hope that you will enjoy reading some amazing
reflects on previous challenges that our profession has
contributions and accept the less formal or “academic”
faced and discussed COVID-19 from the perspective
nature of this edition. Reading these articles makes
of an “older person”. Our Chair, Sarah, is next and she
me realise one very important thing – how incredibly
gives a very personal reflection of her experiences of
proud I am to call myself a physiotherapist. My final
working during COVID-19 and the challenges that she
remark is to thank everybody for their contributions
has faced – many I’m sure we can all relate to. These
and to wish you all a safe rest of 2020. I hope the next
two addresses then lead us onto the contributions
Editorial address I write will be able to reflect on the
from our members. Many of our contributors have not
end of COVID-19 and a “new normal” that feels a lot
written for a journal before, so I want to congratulate
less strange than the current one!
you all on embracing the challenge. I think a lot of
people have found the experience of writing such Stay safe,
reflections quite cathartic, I certainly hope it has been
Abi - AGILITY Editor
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 1
Agility Summer 2020
AGILE National Executive Officers
PRESIDENT Joyce Williams agilehonpres@gmail.com
CHAIR Sarah De Biase agile.physiotherapy.chair@gmail.com
VICE CHAIR Laura Cook agile.vicechair@gmail.com
SECRETARY Susanne Finnegan secretary.agile@gmail.com
MEMBERSHIP SECRETARY Christine Haggarty agile.membership@gmail.com
TREASURER Gemma Mayled agiletreasurer@gmail.com
STUDENT OFFICER Leesha Naisbitt studentofficer.agile@gmail.com
JOURNAL EDITOR Abi Hall agilejournal@gmail.com
RESEARCH OFFICER Annabelle Long researchagile@gmail.com
WEBSITE OFFICER Lynsey Ferguson website.agile@gmail.com
EDUCATION OFFICER Sarah Lambert agile.educationofficer@gmail.com
AGILE Regional Representatives
EAST Justine Musiiime agileeast@gmail.com
NORTH Lynn Sutcliffe agilenorthrep@gmail.com
NORTHERN IRELAND Lisa Hughes agile.northernireland@gmail.com
SCOTLAND Emma Roberts agilescottishrep@gmail.com
WEST AND WALES Kate Bennett agile.rep.west@gmail.com /
agile.wales.region@gmail.com
AGILE Project Officers
PARKINSON’S Danielle Brazier
PARKINSON’S Fiona Lindop
IPTOP Lauren Stenhouse
FALLS Sarah De Biase
2 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Agility Summer 2020
President’s address
Author: Joyce Williams, AGILE Honorary President @JoyceWilliams_
COVID-19 and lockdown, a time of react, rethink Today post COVID-19 the profession must again
and change: rapidly. Much sad and much bad, but concentrate on rehabilitation. And this time we
for Physiotherapy services, the NHS and older people have an additional option, moving on line. And
generally, some good things are emerging. interestingly, the opportunity to join in exercise
groups is once again showing its psychological
Physiotherapists have always been able to respond
effectiveness. Different this time! The growth of TV
to new developments. Possibly because their role
and Zoom activity classes has altered the world for
as experts in dealing with and preventing problems
many older people. No need for Lycra or worrying
of human movement is always relevant. Strength,
what others will think of you. Just join in and enjoy.
flexibility, balance and mobility have now been
Dance, yoga, Tai Chi or a Chair exercise group. No
recognised as essential to both bodily and mental
need for transport either!
health. Apply to everything don’t they? From
childbirth to old age we need the know how of At 84 I was of course in lockdown. Like many, at first
physiotherapists. a worrying thought, loneliness, lack of exercise...Not
at all! We have all been surprised.
It has been intriguing to see the profession once again
coping with a sudden change in demand, and new There had been an issue of older people and their
problems. The rapid response to realign service was reluctance to use IT**. COVID-19 has significantly
superb. New skills or updating in place and then so changed that. Or rather, Zoom has. Families have
many difficulties to overcome. With great delight I coerced older relatives into regular family Zoom
listened to my grandson, also a Physio, who works sessions. Churches, clubs, and hobby classes were
in GP practices, telling me that within a few days of suddenly easy to get to! Coffee and chat with friends
COVID-19 starting they had moved on to phone and were possible on a regular basis, and no need to go out.
video triage. Obvious for some time that use of new
Bridge and Bingo all rapidly moved online and so did
technology made sense, but why did it take a virus to
theatre, museums and the art world. Life became rich
break the system and do it?
and busy. Not only that, if felt free. The choice was
Dramatic emergencies allow ‘rules’ to be broken yours, peace and time for new interests, cooking and
don’t they? Perhaps it was the last major test, just looking, reflecting without pressure. It has been
the Second World War that truly brought the an exciting surprise to discover what we could do,
profession as we know it into being. The War plus all the fresh things we had to learn and take pride in
the nightmare Polio and TB epidemics meant that managing them! Many have said what a valuable life
we had to move quickly into major chest work, experience it has been. Even to the point of wishing it
plastic surgery, the detailed anatomy required to to continue!
treat polio and of course, in a big way, trauma and
Breakthroughs like this have given our profession the
rehabilitation. We were so in demand that the Army
chance to really reflect on and rethink services for
ran a Physio course itself. Army recruits were in
older people. Or should I be saying “ With Older
effect put into lockdown for nine months hard labour
People”? How can we maximise this chance to
- ten hour days, seven day weeks with a Sergeant
abandon old rules and push the boundaries? What
Major. They had to learn everything! And top class
will later years and the profession look like when you
they were too. My husband* subsequently Principal
are 85? Over to you....Enjoy.
of the Sheffield School was one of them.
Joyce
Post war, rehabilitation was the growth area. Huge
gyms, specialist residential rehab units and hydro AGILE Honorary President
pools were created. Patients were treated with very
few staff by using big regular classes. Patients were *Subsequently he became Vice President of the WCPT (World
expected to come 3 x per week, often daily and Confederation of Physiotherapists) hence the CSP prize, for WCPT
usually for 6 weeks. Interestingly that proved to be Level research bearing his name.
a good of way of solving the motivation problem! ** It may be of interest to read the blog I wrote on this.
Much to be said for the psychological power of
https://grandmawilliams.com/2017/04/24/can-oldies-cope-with-
communal exercise?
the-digital-future-yes-if-the-teaching-is-right-for-us
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 3
Agility Summer 2020
Chair’s address
Author: Sarah De Biase - AGILE Chair (2019-2021) @sarahdebiase
I wish I was starting this address with a sense of feel more comfortable. I have found COVID-19 an
unanimous relief – relief that we had surfaced incredibly lonely time. There have been times in recent
beyond COVID-19 and that our work, home and months when I have felt a disconnect at work and from
(most importantly!!) social lives would resume some my work place colleagues (and still do feel this, due to
semblance of what it was like before; whilst recognising working from home) – a feeling heightened due to me
this would not be a resumption of ‘normality’, because being relatively new in role. Working from home was
so much has now changed. But instead, COVID- and still is making it extremely difficult to create the
19 continues to influence how we are living our connections which are necessary for us, as individual’s,
lives, across all domains and is likely to do so for the to feel ‘psychological safe’ at work.
foreseeable; and so I am not sure relief is a feeling
I did find fulfilment during COVID-19 – I found comfort
being experienced at scale (yet).
in helping the clinicians I provide leadership to provide
Nor will I start this address by reiterating messages high quality care despite the uncertainties and ever-
about what we (as a professional) have learned and changing landscapes they encountered. The clinicians
decided to take forward as a clinicians, a profession or were my buddies. As AGILE chair I had opportunity
even as an organisation (AGILE); nor will I summarise for reward (and possibly impact) such as seeing in print
or highlight what physiotherapists working with older in Age and Ageing a co-written commentary on the
people have stopped doing as a result of COVID-19 COVID-19rehabilitation pandemic (1). Interestingly, in
– because, if you are anything like me, you will have writing this commentary, I found it easier to ask for help
read umpteen documents highlighting the innovations, over email (possibly because there is a time lag before
learning and challenges posed by the virus locally, a response) than over the unforgiving virtual world of
nationally and internationally… Microsoft Teams (which has, often, so many watchful
eyes present). What I have found less comforting,
Instead I will kick off this “AGILITY: Reflections of
although I now feel connected to them having had to
COVID-19” edition with my own discoveries. I have
look at them so often during video calls, is my frown
found the last four months chaotic and this is significant
lines! There is no shame in turning off the camera, even
because I personify organised chaos. My brain capacity
if only every now and then.
reached a ceiling during COVID-19. We often talk
about ‘wearing many hats’ but I have never had to To survive COVID-19, I tried to be true to my
change my hats so frequently and quickly in a single principles – by talking openly and honestly; I adopted
day, hour even, as I have done during the COVID- the “double tap” method (https://twitter.com/
19 response. One minute I would be influencing sbattrawden/status/1180502756462923777?s=11)
senior leaders to roll out physical observation and with colleagues and friends (and was honest when
NEWS training for all staff to support assessment and asked myself); I did what I said I was going to do
management of the deteriorating patient; when in the and held myself to account if I didn’t; and i tried to
next minute, I would be contemplating how I could do it all with kindness and compassion. I built new
match the intensity of the home schooling being shared partnerships, for myself and for AGILE – in the simplest
on my son’s school friends’ mum’s Whatsapp group. terms this is demonstrated through the mutual support
The juxtapositions I continuously found myself in were I received from the AGILE administration support
(and at times still are) exhausting… But I learned new person, Sandi Newman. Sandi helped me create an
ways to cope – by intentionally pausing between ‘hat electronic signature – it sounds so trivial now, but at the
changes’ to take stock, and remind myself what it is I time, I was almost in tears trying to work out how to get
was doing or why I was there. I worked hard to make an official AGILE signature onto an online document.
myself be present for every task and worked harder It really is a case of the simple things i.e. those things
to prevent distraction/creep across the different roles I which take five seconds now, but could save someone
fulfil in my day to day life. else fifteen minutes of time (and resolve) later (see Dr
Rachel Pilling and Dan Wadsworth’s YouTube video on
Like others reading this, I wasn’t always in the thick of
Creating Joy at Work here: https://www.youtube.com/
things i.e. on the frontline or on ITU during the acute
playlist?list=PLbLl0DxfoQL5PAbrcT0oU6_gjP-Pf7CLs).
COVID-19 response. But I took comfort from being in
a role which enabled other positive impacts - even if One of the most stand out papers I read during
this was doing something small to make a colleague COVID-19 (of those which were non-clinical in
4 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Agility Summer 2020
nature) was a King’s Fund blog by Suzie Bailey and restrictions to live their lives to the full, with the care
Michael West’s ‘Learning from staff experiences and support they need to do so. No one person is
during COVID-19: letting the light come shining in’ going to solve the problem of COVID-19. I suppose this
(see https://www.kingsfund.org.uk/blog/2020/06/ is why as a committee AGILE NEC are always reaching
learning-staff-experiences-covid-19). The author’s out to you, our members, and asking you to contribute
talk about the need for compassionate and collective to what we do now and in the future. We will continue
leadership (individually and institutionally) as being to do this, as what we do needs to be informed by
core to ensuring staff have the right support. I suppose our members. We need you to talk to us and work
this gave me the reassurance I was in the right place with us, so we can support you in letting your own
when listening to the clinicians and those I lead, and by physiotherapy light shine through.
putting myself in their shoes. Empathy isn’t easy and if, I have one more important thing to say, and that is
like me, you think of yourself as being an empathetic ‘Thank You’. I’d like to take this opportunity to thank
person, hold that thought… I watched this https:// each and every AGILE member for their contribution
youtu.be/1Evwgu369Jw by Brennie Brown and then to caring for older people (and others) within local
had to regroup and think about my own actions when communities during this unprecedented pandemic.
empathising with others. Going forward, we have more to do as we begin to
realise the scale and impact of not just the virus but the
What I now need to do is to take responsibility for
restrictions imposed upon us all to manage and contain
a legacy of collective and compassionate leadership
its spread. Therefore, don’t forget to be kind to yourself
in the work I do going forwards, including as AGILE
as you continue to adapt, respond and care for others.
Chair. With AGILE colleagues we collectively strive to
help you, physiotherapists working with and caring for Sarah
older people to deliver the high-quality care you wish AGILE Chair (2019-2021)
to deliver and will continue to do so. Why? Because
together we can bring greater value and our combined REFERENCES
efforts can shine on beyond COVID-19– efforts De Biase, S., Cook, L., Skelton, D.A., Witham, M. and Ten Hove,
which will help those impacted by the virus and it’s R., 2020. The COVID-19 rehabilitation pandemic. Age and Ageing.
GUIDELINES FOR POTENTIAL AUTHORS
Please submit the article via email as an attachment to AUTHORS PLEASE NOTE
the editor: agilejournal@gmail.com and include an email Manuscripts should be English language.
address for correspondence purposes.
Submissions will be acknowledged.
The following guidelines should be considered:
Material published becomes copyright to AGILE.
• References, where appropriate, should be in the Authors will be advised of any requests to reprint
Harvard style their articles in other journals.
• In the text – one surname followed by date of Author’s name will be published; however,
publication (Jones et al, 2003) professional or academic qualifications are not
• In the reference lists – for journals: names and initials usually indicated. Post titles may sometimes be
of all authors, title of article, full name of journal, relevant.
volume number, issue number and first and last Reports and articles for inclusion in the journal
page numbers. For books: names and initials of all should reach the editor by the deadline for
authors, followed by year of publication, title, place submissions.
of publication and chapter or page numbers or both
Articles should, if possible, be submitted well in
• Articles should be about 2,000 words long. Reports
advance of the deadline. Authors should bear in mind
should be as short as possible (usually not more than
that editing and reviewing takes time. For this reason,
one page when printed in Arial, 10 point, on A4 size
inclusion in the next issue cannot be guaranteed.
paper). However, exceptions can be made accordingly
and at the editor’s discretion. Thank you for considering contributing to Agility
Next edition submission deadline - 1st December 2020
Autumn 2020 – “Advancing and developing roles for physiotherapists working with older people”
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 5
Agility Summer 2020
Inpatient Older Adults Therapy Service - embracing change
through COVID-19
Author: Beth Sykes, Clinical Specialist Physiotherapist for Older People @bethywethy4
In my role as Clinical Specialist Physiotherapist for of physiotherapists from critical care transitioned
Older Adults, I was worried that our older adults’ wards with the patients and went on to form a phenomenal
at Queen Elizabeth Hospital Birmingham (University multidisciplinary team responsible for the rehabilitation
Hospitals Birmingham UHB) would be full of frail of these patients. For me, this was a significant change,
patients, whose treatment escalation had been limited in that although older adult rehabilitation forms a
to ward based care. I imagined wards full of patients large part of my work, recovery from critical illness
who were critically unwell, with extreme oxygen was something I had not been exposed to clinically
demands, and that my team would need to change for a number of years. I felt confident in my core skill
our focus from comprehensive geriatric assessment to set as a physiotherapist and the foundations of our
solely respiratory intervention. Observing the events practice around patient centeredness, comprehensive
unfolding in Italy, I was concerned that my team would assessment, problem lists and goal setting. I was certain
be exposed to a rate of death that would be difficult that approaching these patients as individuals and
to comprehend, and that I was unsure how to prepare utilising clinical reasoning would ensure treatment was
them, and myself, for what was heading our way. appropriate. My professional curiosity resulted in me
spending hours finding resources on twitter and via
The physiotherapy team commenced 7 day working at
the Chartered Society of Physiotherapy, networking
the beginning of lockdown in anticipation of meeting
with other Trusts and accessing webinars, seeking
high clinical demand. Initially this felt premature, as
lessons learned from countries who had already
workload on the wards had reduced as a result of
faced their peak, attempting to rapidly grasp a better
the over 70 population shielding and a reduction in
understanding of the presentation of these patients.
presentations to hospital. Across the wards, there was
Learning the brachial plexus all over again took me
an apprehension that this was a quiet before the storm,
back to student days, and reminded me how much
and for some in itself was anxiety provoking. Keeping
more we can do to embed musculoskeletal knowledge
up to speed on PPE updates and Trust communications
in an inpatient setting.
became a daily occurrence, and it was obvious that the
pace of change meant that continual updates had the The majority of the COVID-19 critical care step down
potential to confuse staff further. patient’s required two therapists to treat, and thanks
to some brilliant physiotherapy assistants, we were
Our first challenge was the movement of patients
able to offer daily high quality rehabilitation. During
between different wards and bed spaces, awaiting
this time our older adult admissions also seemed to be
swab results but requiring physiotherapy treatment.
more dependent, and required a lot of co-ordination
These patients were moved into various side rooms and
between the team to meet the demand for patients
wards where patients pending results were cohorted.
who all required two pairs of hands. Full days
This meant that maintaining the accuracy of handovers
providing rehabilitation in PPE were extremely tiring
became more complex, and alongside staff working a
for therapists, and where possible we maximised use
rota pattern meant that we needed to pay particular
of our gym space and office to allow for hydration
attention to our processes. The team agreed on the
and rest away from the ward environment. We were
creation of an electronic handover, and successfully
particularly grateful for the goodies donated by UHB
implemented this with continual improvement and
Charity and many local and national businesses which
refinements. Looking back, this was a time where the
helped to keep the workforce going.
team felt more empowered as individuals and a team
to make changes and innovate due to the urgency, and As the peak in COVID-19 admissions began to subside,
I wonder moving forward how we can achieve this as a reconfiguration of the trauma service across the
an essential element of service development long term. Trust meant that the older adults’ wards also became
the location for rehabilitation for fractured neck of
Towards the end of April, one of our older adults’
femur (NOF) patients post-operatively. In a short time
wards had become part of the pathway for COVID-
frame, our numbers of NOF rehab patients increased
19 patients leaving critical care. This ward became
significantly, many of whom were only two or three days
the COVID-19 rehab ward, receiving patients with
post-surgery. Many of the rotational physiotherapists in
profound physical and cognitive impairments. A group
the team had no experience of rehabilitation following
6 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Agility Summer 2020
hip fracture, yet did an excellent job of utilising existing past four months, and arguably with leadership from
training and teaching materials to increase their Dr Thomas Jackson, we have created the rehabilitation
knowledge and competence. Senior physiotherapists MDT, culture and ward that we have always strived
completed teaching, and I provided clinical specialist to achieve. We have gathered national and local
reviews alongside staff, to facilitate learning in practice resources and videos into a single document, and
and address any immediate concerns. Close working considered changes and improvements should we be
with Occupational Therapy colleagues has also been met with a second wave.
essential, and seemingly the addition of hip fracture
Collectively as a physiotherapy team we have felt this
rehabilitation was another change that saw the team
has been a time of personal challenges yet professional
respond with determination to provide patient centred
opportunities. For every challenge there has been
treatment.
an improvement, for every new symptom there has
Since waving off the majority of our rehabilitated been learning, and for every upsetting story there has
COVID-19 patients, we have entered a phase of been a patient who has left to return to their family.
debrief and reflection. Each member of the team has Although now feeling the after-effects of four difficult
recognised how much they have learnt in this short months, we are planning to consolidate our learning,
time, and how when under pressure, brilliant things and maximise the development and progress that has
can happen. We have undertaken a COVID-19 clinical happened in this time. Now that I have seen what can
quality review, benchmarking ourselves and the be achieved, I am excited not to return to normal, and
service we provided against guidance that has been excited the see how the NHS can use innovation to
published. We have achieved exceptional things in the recover post pandemic.
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 7
Agility Summer 2020
Into the unknown - personal reflections during COVID-19
Author: Elizabeth Booth & Hannah Wood, Advanced Physiotherapists @Liz46420600
@HannahWoodPT @UHS_Therapy
At the University Hospital Southampton (UHS), the and dignity. We decided that we wanted to capture
acute medicine for older people department rapidly some more information about patients with COVID-
transformed itself to be our initial COVID-19 unit. 19 in recognition of the unique situation we were
Watching the media coverage of the pandemic in. To do this, we implemented a range of holistic
unfold, seeing the impact this was having on therapeutic outcome measures.
international healthcare, was daunting and posed
many unanswered questions. TUG BARTHEL
As therapists we have a strong interest in the evidence
FATIGUE RATING SCALE 40 STEP TEST
base, understanding how patients with various
conditions present and how the signs and symptoms
4AT HADS
affect a patient’s occupational performance. But this
was different. This was something new, something that
BORG
none of us had experienced before. This is an account
of our personal experiences and reflections as acute
older person’s specialists stepping into the unknown, a We gathered these outcome measures on admission
global pandemic where learning came on the job. to the ward, prior to discharge and then two weeks
post discharge via telephone. Our data collection is
ongoing, and it will be many months before we can
fully analyse the data. However, by gathering this
information we ensured a comprehensive holistic
approach to assessments and patient care. As our
experience of working with patients with COVID-19
developed, we often found that young, seemingly
‘fit’ patients were suffering with silent hypoxia
or struggling to wean from oxygen, especially on
exertion. Our older patients were often affected in
similar ways, but with the added complexity of frailty,
sarcopenia and the effects of deconditioning. The
efforts of the team of therapists helped to co-ordinate
rehab and work towards SMART goals for discharge,
whilst also going someway to better understand the
physiological impacts of the disease.
End of life
As experienced practitioners in older people’s care
in the acute setting, we often encounter patients
receiving end of life care. One of the biggest
Holistic care at the heart challenges was to see our patients acutely short of
breath, scared, delirious and knowing that some of
Understanding the symptoms that COVID-19 was our usual treatment options were unavailable due to
causing in our patients was a steep learning curve. the risk attached. It is difficult to try and offer support
Some were expected: shortness of breath, fatigue, and comfort whilst wearing full PPE, but we remained
coughing. Others were unexpected, or worse than we hopeful that holding a hand, and speaking words of
were anticipating: silent hypoxia, overwhelming and comfort helped to calm and reassure the patients we
long lasting fatigue, delirium, sudden deterioration, had come to know. On the occasions of absence of
anxiety. We regularly saw seemingly stable patients their loved ones, we hope the patients knew they
suddenly deteriorate and escalated to intensive care, were cared for, and that their relatives knew the care
or have the focus of their care changed to comfort and compassion they received.
8 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLEAgility Summer 2020
Apart from being hot and uncomfortable to wear, the
Patients first difficulties with effective communication in PPE was
something we rapidly learnt to manage, especially as
lip reading had been taken away. Our voices were
muffled and our smiles hidden —conveying empathy
and engagement with patients with cognitive
Always improving impairment more challenging. One thing we have
developed recently is our ability to read people
through their eyes and body language, significantly
enhancing our compensatory communication skills.
Working together
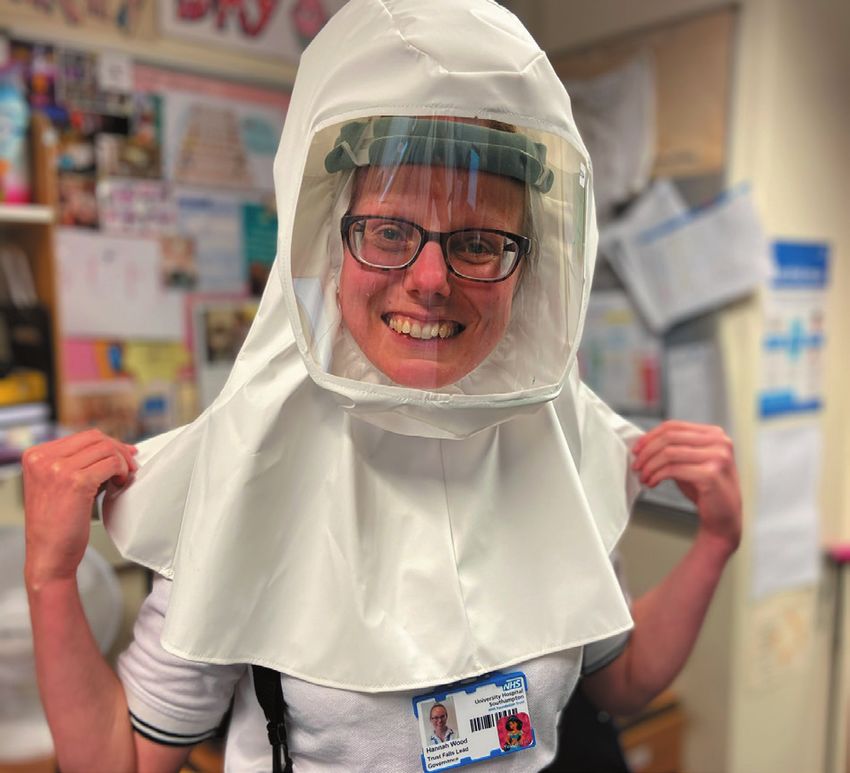
The development of the PERso hoods revolutionised
our PPE experiences. Initial humour, and various
‘descriptions’ helped to raise team moral. We have
PPE been ‘spacemen’, ‘Teletubbies’, ‘deep sea divers’ and
many more. There were some challenges but the
PPE has long been used in healthcare but perhaps positives were so valuable. To be able to smile with
not previously with such significance. UHS was swift patients and share facial expressions was something to
to respond to the demands of PPE, and kept us treasure. We recognise this was a unique experience
informed of any supply chain issues and solutions. for us at UHS, and it’s a privilege to have been
Each ward had PPE stations with supplies, and a involved in this developing technology.
hugely supportive MDT ready to tie you into gowns,
check you were ready to enter a bay, or assist with
doffing. As supplies of FFP3 masks changed, re-testing
was available to ensure we always had the correct
protection available, especially for doing respiratory
interventions. We also had a trial of new PerSO
hoods that could be used.
There was a lot of information on PPE throughout the
pandemic, and keeping abreast of the most recent
updates was a challenge. Our Trust ensured there
were training sessions and resources available to
support us through this part of the journey.
Leadership
As physiotherapy team leaders on a large, busy
COVID-19 unit, our overwhelming feeling of this
experience is pride. Proud of ourselves and all our
healthcare colleagues on the frontline for navigating
through unknown challenges despite fear and
anticipation. Leading a team in a rapidly evolving
situation, with multiple updates of information (often
several times a day), changes to practice guidelines,
PPE guidelines, managing sickness, supporting each
other and our team through unsettled and anxious
times has been demanding and exhausting. Upon
reflection, we feel that we faced this situation with
courage, dignity and strength in our professional
relationship.
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 9Agility Summer 2020 We are incredibly proud of our team’s courage Learning and commitment to our patients and the way we supported each other. We had staff redeployed to Rapid upskilling training sessions for all of the team us who weren’t experienced in working with older focused on respiratory skills: particularly palpation, adults. New graduates joined us who were advanced observation and subjective questioning. Specialised to the HCPC temporary register plus support from respiratory colleagues, and those in non-clinical team members working non-clinically. All staff roles, supported with enhancing these skills. Many contributed greatly in some way. The teams’ bravery, staff undertook training in anticipation to support our professionalism and enthusiasm during this time nursing colleagues if the need required. Likewise, has been remarkable. We have never seen such we shared our holistic older person skills, particular exceptional team work, flexibility and camaraderie around falls, frailty, delirium and dementia care. with everyone pulling together to develop knowledge Whilst there were many challenges working through and skills, share learning, and support each other this pandemic, the opportunity to learn new, or through this journey. refresh skills has been helpful. Teamwork Delirium The hospital’s bed occupancy was reduced in We often see delirium in elderly patients, but we anticipation of a COVID-19 surge, and so therapists saw delirium in people of all ages during COVID-19. from other teams joined us. We learned new Post ITU syndrome was common: a multi-factorial assessment and treatment techniques and drew on effect of sedative medications, lack of contact with their specialist skills to develop our own practice. families to help tie patients to a sense of reality, Likewise, we shared ours. A wave of medical staff and all staff wearing PPE may have contributed. from different parts of the hospital supported the unit Patients often presented with silent hypoxia and we - nurses from clinic settings, professors in academia, witnessed younger patients remove their oxygen to as well as our geriatricians. The whole MDT walk to the bathroom without symptoms prompting supported each other – from assisting each other to a requirement. Did this contribute to delirium in don/doff PPE, to detailed conversations about clinical younger patients? We engaged with our valued OT presentations, learning and sharing together. There colleagues with assessment and treatment strategies was a real sense of us all being in this together. As for these patients. We assessed for delirium in all a staff group we recognised the value of teamwork patients with use of the 4AT, and worked hard to across the MDT and the support that comes with instil daily the value of orientation for all patients we knowing your team well. worked alongside. 10 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE
Agility Summer 2020
Conclusion people post COVID-19, thanks to our experiences
and challenges whilst working through a global
The UHS Trust’s core values are ‘patients first’, pandemic.
‘working together’ and ‘always improving’. On The whole experience has been one of exploration
reflection, the COVID-19 journey thus far has and learning. We are lucky to work in a Trust with
epitomised these more than any of us appreciated at such a dynamic and forward thinking research
the time. Often during those early weeks, we were department and yet the day to day learning through
out of our comfort zones, yet the focus of our efforts this process should not be underestimated. Together
was our patients. As older persons specialists we are we explored when to implement self-proning, how
flexible and dynamic therapists, often responding to progress complex oxygen weaning, how to better
to unexpected clinical presentations and unplanned communicate through our PPE and how to promote
situations, but the COVID-19 pandemic has acute rehab and develop new pathways to support
highlighted just how versatile our skill set is. Whilst this. None of which would have been possible
there were many unknowns the one thing for certain without sharing and learning with our colleagues and
is the sustained belief that the patient is the centre of wider professional networks. Our knowledge and
all actions and decisions. What matters to you? How skills have evolved during the COVID-19 pandemic,
can we help you? and highlighted just how important it is for all of us
As older persons specialists we are privileged to to be continuously learning and looking for ways to
be a part of a great MDT, but the team work and improve to provide the best service possible for all
camaraderie experienced during these times has been our patients.
unbelievable, not only within the immediate therapy The COVID-19 journey has a long road ahead. Now
team and the whole MDT, but with the wider local more than ever we must all keep our patients at the
community. The team have been on this journey forefront, be open to change to enable us to improve,
together from day one - celebrating the small victories adapt and work together as a system to achieve the
as one, whilst wiping each other’s tears when things best outcomes for all.
didn’t turn out as planned. We will all be different
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 11Agility Summer 2020
Working on an acute medical ward during COVID-19
Author: Kerry Hunt, Complex Care Physiotherapy Team Lead @kerryHu83346946
Four years ago, I took on the role of becoming the struggled to catch her breath to communicate is a
complex care physiotherapy lead, moving away sight we all will remember. The high-pitched wheeze
from respiratory medicine to seek new avenues ringing in our ears as we attempted to support her
and challenges in the varied, fast paced world of to do something as simple as reposition in bed. The
medicine. In March 2020, when COVID-19 lock realisation that her oxygen demand was increasing
down commenced, I was being pulled back towards minute by minute but a reassuring holding hand
respiratory, teaching teams in the expected patient and sorting her hearing aid batteries at the time
presentation and being earmarked to become was important to bring her back into the room and
part of the respiratory ward mega team, or as we give her half the chance of hearing us over the PPE
were calling it, Tier Two. At this time the focus had masks and visors strapped tightly to our faces. This
turned away from delivering falls prevention groups, first encounter developed our first modification
rehabilitation of Parkinson’s patients and acute to working, a realisation that to patients we were
medical assessments, and moved towards an acute bodies in plastic moving around them like people
respiratory phase followed by discharge as soon as from a nightmare, leaving them wondering who
possible out of the risk area of the hospital. What was was behind the mask. We put into action laminated
left behind was a remodelled therapy team, small in pictures of us as “normal people.” They say a smile
numbers to focus on what was being predicted as means a thousand words and we were willing to try
small numbers requiring rehabilitation. At the time I anything to reassure our patients at a time of need.
often wondered what would happen to the general Life working on the COVID-19 positive ward wasn’t
consistent flow of medical patients frequenting my always bad. I remember vividly a day in the depths
beds daily, as I believed that frailty wouldn’t go away of the pandemic enjoying a time to celebrate with
with COVID-19, and that people weren’t facing less one of the rotational members of my team. A patient
risk of falls. Ironically, I never moved to COVID- was turning 100, a worthy milestone in anyone’s life
19Tier Two. The pull of medicine, and in particular but to be COVID-19 positive, fighting and still able to
older persons’ medicine, was always present. The celebrate an even bigger one! COVID-19 had taken
steady stream I had predicted kept coming, and away the family part, the opportunity to share this
the benefit of a consistent therapist in a patient’s event with her nearest and dearest. However, in true
care was highly valued by medical teams who had NHS family style, a celebration was had. The patient
been pulled together into mega teams from a variety got her big 100 balloon, was sung happy birthday
of backgrounds. We became the profession who from the lungs of emotional staff and enjoyed a
could help with equipment set up, support patients pre-lunch drink of sherry, along with her birthday
throughout their inpatient pathway and beyond. The cake. That moment gave me a sense of the personal
consistent person at the beginning, middle and end as strength of an older person. The ability to look at
always but COVID-19 highlighted our diverse skill set. any threat head on and focus on the key event for
The ability to move between specialities using our today, a sense that life was going on away from the
clinical lead colleagues if extra expertise was needed, pandemic, birthdays were still to be celebrated and
demonstrating our leadership and teaching skills for laughter was a great medicine.
the whole organisation to appreciate. Ultimately, we
The headlines would ring daily with ICU numbers
were providing the best care and advocating for all
and our ICU was celebrating patients discharging
our patients.
from them and entering a new phase – rehabilitation.
In those early configurations one of the wards I As a complex medical bed base we started to receive
covered turned into a COVID-19 positive ward, with many of these patients with one common theme, an
no plans for ward escalation above wall oxygen. It age over 60. Physiotherapists providing rehabilitation
was painted as a bleak place to work, with a high to those who have developed ICU acquired
expected mortality. The actual reality was a ward weakness, fatigue, breathlessness and anxiety were
where age literally was just a number. Patients all tools we hold in the tool box. The excitement in
from all ages and backgrounds were fighting back. the team was palpable. The opportunity to get back
Admittedly, there were patients who didn’t survive, to celebrating small milestones and utilising some of
one being the first COVID-19 patient my team our other skills away from the respiratory skill set was
and I treated. Watching the fear in her eyes as she exciting. We were ready with our outcome measures,
12 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLEAgility Summer 2020
goal setting laminates and patient experience activity boxes, sit-to-stand challenges, and exercise
colleagues to enable patients to reconnect with booklets to continue with at home have become
families outside of the hospital walls. At no point did the new acute ward environment. We are using
we contemplate the devastating effect this virus would our knowledge to promote exercise the same as
have psychologically. The physical impact we could pre COVID-19, however the changes to the way
see, through significant weakness, embolitic damage, we deliver enforced by COVID-19 is increasing
scarring on CT, but naively we weren’t prepared for adherence, as exercise isn’t a separate task, rather it
the PTSD, the night terrors, and the patients struggling is embedded in all aspects of a daily routine, aiming
to engage with rehabilitation. The reality was some to improve functional enablement. COVID-19, in a
did great, progressing and keen to move forward weird way, has given us time to reflect and enforced
as fast as possible, taking the Motomed by storm. changes in our behaviours and practices, making
Others, however, needed acute physiotherapy to rehabilitation move away from tick box activities such
provide something different, a discharge away from as a stair assessment and more about focusing on
the memories of a building where they arrived in what makes each one of us feel independent.
extremis and somewhere different to start a new
COVID 19 cases are significantly reducing in my
chapter. Our role became more focused on liaising
hospital currently, and a ‘new normal’ has resumed
with community planning to enable rehabilitation at
to life on the wards. However, the older persons
the right time and in the right environment for the
complex care team continues to deal with the
patient. This is something we still have work to do to
secondary effects of COVID 19. The numbers of cases
get right. Watching patients struggle psychologically
admitted for falls secondary to the prolonged period
brought home that catching the virus was only the
of reduced mobility are rising. This has been a new
start. The reality is that some of these patients may
area for us in physiotherapy to focus on with our
frequent our doors for months, maybe even years, to
community partners meeting the demand of acute
come to terms with the secondary effects of catching
hospital flow along with breaking the cycle of falls
COVID-19. Links with psychology and chronic fatigue
re-strengthening using new ways and technology to
services have been loosely formed already, with plans
reach out to a large population of at risk service users.
to firmly identify these referral pathways in the future
Mental health is a topic we are also learning fast with,
alongside modified falls groups and the right to rehab.
as the negatives of social isolation are, as ever, present
Ways of delivering services to older people where
in our patient population, often causing self-harm
technology may not be freely available is also an area
admissions. Ensuring we optimise rehabilitation
we are focusing on. COVID-19 felt like something
pathways and utilising support network groups is our
we couldn’t fully plan for in its initial wave, and we
next phase of focus. As a team lead I put a quote up
continue to learn through each individual case of
in the quiet reflection base of my team, and for me it
how best to support this group to prevent further
is as relevant as ever; as T Roosevelt once said focus
deconditioning and social isolation.
on “doing what we can, with what we have, where
Adaptability is one of nature’s strongest advantages. we are.”
During this period of acceleration within the
pandemic, I observed first-hand how people were
adapting. Patients and staff modified communication
away from verbal to non-verbal cues. The ability to
follow instructions with sign language is now second
nature. The reality is we are all brought up on sign
language. Those early developmental years when
we were younger, the ability to understand stop
with a raised hand and, well done with thumbs up.
We are continuing to adapt now, bringing the gym
to the ward as we are currently unable to access
our rehabilitation gyms due to limiting movement
between different areas. We are relighting the
interest for older people in exercise, giving them
the support and expertise they need to make it part
of their everyday routine. Rather than sporadic
rehabilitation sessions where patients slotted in with
gym capacity and staff availability, every opportunity
is now utilised to keep our patients moving. Exercises
whilst brushing your teeth, walking challenges,
CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLE 13Agility Summer 2020
Evolution of the role of physiotherapy in a care home during
the COVID-19 Pandemic: A view from the front line
Author: Susanne Syme, Private Practitioner @SusanneSyme
Five months ago I was an experienced private and “Caring”. The advice from the CSP at the start
practitioner working with older people in care homes, of the pandemic on priority groups for physiotherapy
retirement villages and their own homes in Somerset. and minimising Face to Face contacts was timely and
The impact of the COVID-19 pandemic required enabled me to be clear who I could see directly and
me to change my practice overnight but has led to a who I could support remotely through staff report
rare learning opportunity to work as part of the team and where necessary observation. Systems to enable
at a Residential and Nursing home and a Dementia professional networking quickly came online such
Specialist home. This article aims to reflect on issues as the South West Forum webinars. For many of
facing the care sector before the pandemic and some us webinars and checking daily updates from the
of the issues now in the spotlight to enable therapists CSP and PHE after a day’s work became normal
to see the difference we can make should services be and enabled me to keep abreast of developments
funded during and beyond the pandemic. including debates over PPE. Information from the
physiotherapy profession was shared with the senior
Before the whole country went into lockdown, the
leadership team at the care home. In addition, the
care sector had already been massively impacted.
early work on identification of atypical presentation of
The speed of these changes was unprecedented. It
COVID-19 in people living with frailty from the BGS
was apparent that the national priority was to release
was discussed between the senior team, nurses and
hospital capacity to manage the COVID-19 pandemic
myself in relation to each resident and built into their
which led to rapidly discharging people to care
daily review. The complexities of care planning in the
homes and also trying to prevent people from being
context of delirium, increased falls and generalised
admitted or readmitted to hospital, or increasing
weakness coupled with the high prevalence of
demand on GPs and primary care teams. At the
dementia meant staff knowing residents well was
same time relatives were trying to get their family
critical to anticipatory care. I was given access to data
members placed in care homes, as they themselves
from the electronic records relevant to my practice.
began to shield, and community support structures
were uncertain. The effect in care was that some of Procedures for managing staff, residents and
the new residents were more able than usual, others visitors were put in place including hand washing,
came in for care at the end of the lives who may temperature checks and screening questions before
otherwise have been able to stay at home and people anyone entered the building and the team was given
had more unmet rehabilitation needs than usual. appropriate training such as donning and doffing. As
Large numbers of staff began to self-isolate and the a staff group we supported each other to understand
COVID-19 status of residents and their visitors was why and how things were changing in order that we
unknown. could keep the residents and their families informed
as the pandemic progressed and this helped to
Managing the risk of infection reduce the anxiety amongst staff. Residents and
families then received the difficult news that visiting
The priority personally was to work out which of my was suspended and it was unclear for how long this
therapy skills would add value during the pandemic would be.
whilst managing the risk of infection. I reduced Care staff going “above and beyond” has been
my clinical practice to one location by choosing documented during the pandemic. One particular
to talk to the owner and manager of a care home moment will stay with me, when at a team meeting
I already had a relationship with. I knew some of one of the carers asked, “Does that mean I can’t visit
the residents and was trusted by the residents, their my own mum, what if she needs care?” Handling of
families and the care home team. The care home these issues by the senior leadership team including
has a 32-bedded Residential and Nursing Home supporting staff with increased hours to help maintain
with a 50-bedded Dementia Specialist Home. The household incomes avoided the Emergency Measures
residents are almost all frail and the majority are living that were having to be put in place in other care
with dementia. The care home has an overall CQC homes. In spite of the national news about care
rating of outstanding in the domains of “Well Led” homes the senior team managed to continue to
14 CHARTERED PHYSIOTHERAPISTS WORKING WITH OLDER PEOPLEYou can also read

















































