ROBERT BREVING, MD The Newest AMS Trustee Shares a Remarkable Story of Giving - DECEMBER 2014 - Arkansas Medical Society
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vol.111 • No. 7 DECEMBER 2014 ROBERT BREVING, MD The Newest AMS Trustee Shares a Remarkable Story of Giving NUMBER 7 DECEMBER 2014 • 121

WHEN IT COMES TO YOUR PATIENTS’ HEALTH C ARE,
YOU HELP CALL
THE PLAYS
Encourage Blood pressure check
your patients to Flu shot
schedule important Cholesterol screening
preventive care: Colorectal cancer screening
Mammogram
Cervical cancer screening
Preventive care can detect
problems early and help keep
122 •your patients
THE JOURNAL healthy.
OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111
THIS MATERIAL WAS PREPARED BY THE ARKANSAS FOUNDATION FOR MEDICAL CARE INC. (AFMC) UNDER CONTRACT WITH THE ARKANSAS DEPARTMENT
OF HUMAN SERVICES, DIVISION OF MEDICAL SERVICES. THE CONTENTS PRESENTED DO NOT NECESSARILY REFLECT ARKANSAS DHS POLICY. THE ARKANSAS
DEPARTMENT OF HUMAN SERVICES IS IN COMPLIANCE WITH TITLES VI AND VII OF THE CIVIL RIGHTS ACT. MP2-AMS.PREVHLTH.AD,4-12/14
ON THE COVER
ROBERT BREVING, MD
128 The Newest AMS Trustee Shares
a Remarkable Story of Giving
by CASEY L. PENN
COMMENTARY
BY ISSAM MAKHOUL, MD
126
WHAT HAVE WE DONE FOR YOU LATELY?
DAVID WROTEN, EXECUTIVE VICE PRESIDENT
124
SCIENTIFIC ARTICLE
A Closer Look
at Quality 132 Back Pain – An Ominous Harbinger
of Spinal Cord Infarction
Winner of the ASAE Excellence
Vidya Pai, MD; Yogita Rochlani, MD; Kinshuk Sahaya, MD 134
in Communications Award
CASE STUDY 136
Falls and Comorbid Conditions among
Volume 111 • Number 7 December 2014 Community Dwelling Arkansas Older Adults
from a Population-based Survey
Established 1890. Owned and edited by the Arkansas Medical
Society and published under the direction of the Board of Masil George, MD; Gohar Azhar, MD; Greta Kilmer, MS;
Trustees. Sabra Miller M. Ed; LaTonya Bynum, BS; Appathurai Balamurugan, MD, MPH
Advertising Information: Penny Henderson, (501) 224-8967 or
penny@arkmed.org. #10 Corporate Hill Drive, Suite 300,
Little Rock, Arkansas 72205.
Postmaster: Send address changes to: The Journal of the Polymethylmethacrylate Pulmonary Embolism
Arkansas Medical Society, P.O. Box 55088, Little Rock, Arkansas
72215-5088. as a Complication of Percutaneous
Subscription rate: $30.00 annually for domestic; $40.00, Vertebroplasty in Cancer Patients
foreign. Single issue $3.00.
The Journal of the Arkansas Medical Society (ISNN 0004-1858)
is published monthly, except twice in the month of August by the
Arkansas Medical Society, #10 Corporate Hill Drive, Suite 300,
Natasa Milojkovic, MD; Samer Homsi, MD
140
Little Rock, Arkansas 72205. (501) 224-8967.
142
Printed by The Ovid Bell Press Inc., Fulton, Missouri 65251.
Periodicals postage is paid at Little Rock, Arkansas, and at
additional mailing offices. PEOPLE+EVENTS
Articles and advertisements published in The Journal are for the
interest of its readers and do not represent the official position
or endorsement of The Journal or the Arkansas Medical Society. Join us to stay updated on health care news in Arkansas.
The Journal reserves the right to make the final decision on all
content and advertisements.
© Copyright 2014 by the Arkansas Medical Society.
facebook.com/ArkMedSoc twitter.com/ArkMedSoc ArkMed.org
www.ArkMed.org Feature Articles
NUMBER 7 DECEMBER 2014 • 123
WHAT HAVE WE DONE FOR YOU LATELY?
Medical Board
Legal Issues? The Countdown Begins.
DAVID WROTEN
EXECUTIVE VICE PRESIDENT
Call
Pharmacist/Attorney In one month, the 90th General As- The “Private Option” alternative to Medicaid
expansion will undoubtedly take up a tremendous
Darren O’Quinn sembly of the State of Arkansas will
amount of time and political capital in order to con-
convene into regular session. The elec- tinue its course. Currently over 210,000 previously
1-800-455-0581 tions are over, and thankfully so are the nasty cam- uninsured Arkansans, mostly employed and earning
paign ads that dominated our airwaves for most of less than 138% of the federal poverty level are now
the past six months. I’m reminded of the words covered by private health insurance. It takes a dif-
www.DarrenOQuinn.com we look forward to hearing each time our television ficult 75% vote in both the house and senate to obtain
watching is interrupted by breaking news, “we now the appropriation to fund the program. It will take
return to our regularly scheduled programming.” exceptional leadership from the “new” governor and
Thank goodness. the leaders of both political parties to continue this
program.
Your physician and staff leadership in the AMS
are hard at work preparing for the legislative ses- Telemedicine continues to grow both in Arkansas
sion. There are priorities to set and bills to draft. and nationally. However, there are licensure issues
Little Rock, Arkansas While I cannot tell you today what those priorities and reimbursement issues that must be addressed.
are, I can tell you some of the issues we already Expect AMS to lead the charge to get this done.
know will be on the table for consideration. The Physician Orders for Life Sustaining Treatment,
session is setting up to be very difficult as you will
Mercy Clinic Fort Smith or “POLST,” is an effort to address the current short-
see from the issues that follow. comings in our current system of end of life planning.
Communities seeks Family
Certified Registered Nurse Anesthetists Currently, patient wishes cannot always be honored
Medicine Physicians to even with an advance directive due to the lack of a
(CRNA) will once again seek to remove the require-
work in Fort Smith, AR. ment that they practice “under the supervision of”
physician’s order. The use of a POLST form, which
focuses on conversations between the patient their
Please send CV and cover letter to: a physician or dentist.
family and their physician, allows the patient to docu-
Mary Margaret Pratt
Advanced Practice Registered Nurses are ment their wishes in the POLST form, which translates
Mercy Physician Recruiter
again seeking to require Medicaid and other payers the shared decisions into actionable medical orders.
to recognize them as qualified to be the head of pa-
Continuation of the ACA primary care enhanced
Mercy Clinic Fort Smith tient centered medical homes. We expect another
payment for Medicaid services. The Affordable Care
Communities seeks attempt to require payers to reimburse them at
Act increased Medicaid reimbursement for primary
Internists to work in rates equal to that of physicians despite their lack
care up to Medicare amounts (about a 25% increase)
of equal education and training.
Fort Smith, AR. for 2013 and 2014, fully funded by federal dollars. Pri-
Naturopaths are asking to be officially recog- mary care groups are asking the state to continue this
Please send CV and cover letter to: enhanced reimbursement under the normal 70/30
nized by creating a state licensure system.
Sarah Wilson match, meaning the state puts up 30% of the funds,
Mercy Physician Recruiter A group representing “certified” surgical tech-
which translates into about $12 million per year. The
nologists and surgical assistants are seeking to reason is justifiable, currently Medicaid pays primary
require that anyone performing those duties must care services at about 55% of private insurance. The
attend a formal educational program, pass a na- hurdle is finding the dollars to fund this program.
tional certification exam and obtain a license from
There…that is just a handful of what we are go-
a state licensing body such as the Arkansas State
Mercy Clinic Fort Smith ing to be dealing with. Buckle up and let the count-
Medical Board.
2901 S. 74th St, Fort Smith, AR 72903 down begin.
124 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111
David Wroten Free your mind to think about
Executive Vice President
something other than med-mal.
Nicole Richards
Communications Coordinator
Jeremy Henderson
Art Director
EDITORIAL BOARD
Frankie Griffin, MD
Orthopedic Surgery
Robert Hopkins, MD
Pediatrics/Internal Medicine Since we’re singularly focused on medical
malpractice protection, your mind is free to go LAMMICO is proud to support the
David Hunton, MD other places. LAMMICO is not just insurance. Arkansas Medical Society’s
Surgery We’re a network of insurance and legal Annual Meeting May 2-3, 2014
professionals experienced in medical liability
claims. A network that closes approximately 90%
Laura Sisterhen, MD
of all cases without indemnity payment.
Pediatrics A network of robust in-person and online Risk
Management educational resources to help you
Sandra Johnson, MD avoid a claim in the first place. LAMMICO’s a
partner - so that when you insure with us, you’re Building Enduring Partnerships
Dermatology 800.452.2120 www.lammico.com/AMS
free to do your job better. And that’s a very
peaceful place to be.
Issam Makhoul, MD
Oncology
EDITOR EMERITUS
Alfred Kahn Jr., MD (1916-2013)
ARKANSAS MEDICAL SOCIETY
2014-2015 OFFICERS
Alan Wilson, MD, Crossett
President
G. Edward Bryant, MD, West Memphis
President-elect
William D. Dedman, MD, Camden
Vice President
Omar T. Atiq, MD, Pine Bluff CLINIC MANAGERS & PHYSICIANS:
Immediate Past President
Chad Rodgers, MD, Little Rock ARKANSAS-BASED URINALYSIS LAB
Secretary • OWNED BY PHYSICIANS
Frankie Griffin, MD, Van Buren • CLIA CERTIFIED & COMPLIANT
Treasurer
• SUPPLIES PROVIDED
Michael Saitta, MD, Fayetteville • FOUNDED IN 2012
Speaker, House of Delegates PHYSICIANS’ • PERSONALIZED DRUG SCREEN TESTING
Anthony D. Johnson, MD, Little Rock LABORATORIES • ONLINE REPORT ACCESS
Vice Speaker, House of Delegates
OF AMERICA, LLC • ARKANSAS BASED BILLING CO
Dennis Yelvington, MD, Stuttgart
Chairman of the Board of Trustees
PLALLC.COM • 501.603.1751
NUMBER 7 DECEMBER 2014 • 125
COMMENTARY
Surviving Cancer as “Myself”
BY ISSAM MAKHOUL, MD Not as a Face of the Disease
W
ith the improvement of nected and do not hear the rest of the discus- care team and engagement of the family to
sion. It is not uncommon for me to answer the address these issues are paramount.
our cancer diagnostic
same questions several times in the immediate
“I want to become myself again,” one pa-
and therapeutic tools period after a diagnosis is given. The presence
tient said “I am not only a successful cancer
the number of cancer survivors of a family member makes this task easier by
case.” Many patients express the feeling that
is expected to reach 18 million providing someone who is able to comprehend
they are not understood or that nobody listens
and remember important details that the pa-
by the year 2022 while the exist- tients do not even hear. The role of the family
to them. Unfortunately, it is not uncommon that
the system ignores their voices because “they
ing structures of our health care only expands from this point forward with all
have survived” and that should be enough. It
system are not well adapted to the logistics required for the treatment phase –
has become clear from our experience with
i.e. transportation, house chores, employment
address their multifaceted needs. cancer survivors that this phase will last for a
changes, etc.
Screening for recurrence and new cancers, long time; it carries its own specific problems
identifying and caring for late and long-term But most importantly, family members and solutions, but it receives the least focus
side effects of the cancer or its treatment offer the emotional and spiritual support that and attention from care providers. Hence the
and managing the psychological and spiritual only a family can provide. Past the acute need for a specific “cancer survivorship pro-
needs of survivors are the mainstay of health- phase of treatment, patients struggle to return gram” that looks at patients as whole persons
care after acute cancer treatment has ended. to “normal life” before cancer became a part and not a disease or affected organ. This is
Patients are seen by many specialists and of their daily existence. While this is possible a program that provides a navigation system,
tests are ordered, and yet many of their es- for most patients from a physical standpoint, helping patients in their journey by addressing
sential needs are not met. What is missing is many patients cannot achieve this goal. Their their general and specific survivorship needs,
the focus on these new needs and communi- lives have changed forever due to the loss of being sure the latest screening guidelines are
cation and coordination between their doctors a limb, a colostomy or the inability to speak met, and improving communication and co-
and, most importantly, with the patients and or to walk. Many patients fall into depression. ordination between their providers, all while
their families. Others have protracted pain and fatigue or keeping the overall well-being of the survi-
Stress, missed work days and financial lose their ability to concentrate and remem- vor in sharp focus. This program will help our
burden imposed by a cancer diagnosis are ber, a condition called by the patients “chemo patients retrieve their “new norm” by provid-
going to be experienced by family members brain.” Interestingly, patients who had only ing them with appropriate rehab support and
too. Weak family relationships may lead to surgery and never received chemotherapy reeducating them about healthy living. Elec-
failure of treatment and strong family ties may suffer from the same condition, which un- tronic medical records offer the promise of
be the bridge to the cure. When the patients derlines the impact of this traumatic experi- improving communication between providers
are overwhelmed by a diagnosis, terrorized by ence on brain functioning. But invariably they and with patients but without a well-designed,
the prospect of failure to cure it and tired from all suffer from a smoldering anxiety and fear patient and family centered program geared
the numerous tests and different treatments, of the return of cancer, some sense of loss of toward addressing the unique needs of can-
a strong family structure will help them pick control and lack of trust in the future that be- cer survivors we will not make substantial
up the pieces and move forward. The state comes visible at transition times such as scans progress. Our ultimate goal should be to allow
of shock, typical for this diagnosis phase, or office visits or with any new symptoms, no them to overcome the constant reminders of
explains the “selective hearing” that many matter how trivial they are. Sometimes, the cancer and regain their place in their social
cancer patients experience. Once the word family is ready to move on but the patients are network to become again themselves not the
“cancer” is uttered they are no longer con- not. Here again, an active intervention by the face of a disease.
126 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111
CYBER LIABILITY PROFILE
PHYSICIAN/DENTAL PRACTICES
Why would my practice need cyber/privacy insurance?
A large majority of doctors and dentists are not aware that their standard insurance coverages (Malpractice, GL,
Property) typically don’t provide proper coverage for cyber and privacy liability. Most also don’t know that they
(along with their practice) have an exposure to cyber and privacy risk, especially given the presence of personal
health information that they and their vendors have access to and the laws that exist to protect this.
Any medical practice that… Financial Threats to Your Practice:
• Obtains social security numbers, personal health information, drivers • Costs to comply with federal and/or state required notification.
license numbers, bank account numbers of patients Data breaches in 2010 cost their companies an average of $214/
• Is in the process of going paperless or stores paper files record.*Ponemon Institute Study
• Provides online access for payment • Various regulatory proceedings (including fines and penalties) as a result
• Has a website of a privacy breach, including alleged HIPAA violations.
• Relies on their computer network on a daily basis • Patients/affected individuals suing your organizations for damages as a
…carries a significant exposure to cyber risk. result of a privacy breach or network intrusion
• Liability for the transmission of malicious code to an outside party
• Business interruption expenses as a result of your network or server going
down due to a denial of service attack or similar action
• Intellectual property/privacy lawsuits. These include libel/slander arising
out of content that is on your internet or intranet sites
• Destruction to your ‘brand’ as a result of a privacy breach (lost patients)
Given our expertise in underwriting small to medium- Claim Scenarios for physicians/dentists:
sized companies’ insurance… • A physicians assistant brings a laptop home to update patient records.
We recently developed a cyber product that: While on her way home, she stops at the grocery store and her car
is broken into and the laptop is stolen. Files on the laptop contained
• Is modular. You are able to pick and choose appropriate coverage lines
patient names, social security numbers, dates of birth, addresses, phone
• Is on PHLY’s admitted A++ paper
numbers, and medical condition information
• Provides industry leading coverage for both 1st party and 3rd party exposures
• In an effort to go paperless, employees organized medical information
• We can help you understand. At any point, a cyber underwriter can help
(to be shredded) and non-medical information (to be thrown out.) The
explain the coverage to you, and/or your agent
person responsible for discarding the information inadvertently switched
the two types of information and the medical information was thrown into
Information needed for a Non-Binding Indication: an unsecured dumpster without being shredded. Personal information and
• PHLY Cyber Application (online adobe fill-able) or PHLY Indication Application personal health information of patients is compromised and those affected
join a class action suit against the practice
• A hacker gained unauthorized access to a surgery center’s computer
system. The practice’s failed to timely notify its patients whose personal
health information was contained on the computer system. The practice
suffered fines and penalties for not adhering to HIPAA laws and regulations
• A practices’ computer network is down for 4 days as a result of a Trojan
horse attack and are unable to access billing software, appointment
scheduler or patient files, resulting in a need to hire experts to come in
and correct the system and get it back to where it was functioning
• A practice has a website and posts testimonials from patients. As a
“Serving Conway & Faulkner County since 1903” result of the practice not obtaining proper authorization to use one of the
Farris Agency is endorsed by AMS Benefits, Inc. patient’s comments, they are sued for invasion of privacy
www.farrisagency.com | Office 501.329.1221
800.873.4552
Philadelphia Insurance Companies is the marketing name for the insurance company subsidiaries of the Philadelphia Consolidated Holding Corp., a Member of the Tokio Marine Group. Your insurance
policy, and not the information contained in this document, forms the contract between you and your insurance company. If there is a discrepancy or conflict between the information contained herein
and your policy, your policy takes precedence. All coverages are not available in all states due to state insurance regulations. Certain coverage(s) may be provided by a surplus lines insurer. Surplus
PHLY.com
lines insurers do not generally participate in state guaranty funds and insureds are therefore not protected by such funds. | © 2007-2012 Philadelphia Insurance Companies, All Rights Reserved.
Ed. 020812
NUMBER 7 DECEMBER 2014 • 127
ROBERT BREVING, MD
The Newest AMS Trustee Shares
a Remarkable Story of Giving
by CASEY L. PENN
A
good story tends to travel. son and changed the course of their life, is Prior to her schizophrenic break, the late
When Robert (“Bert”) Brev- uplifting and rare.” Mrs. Breving was regimented, smart and
devoted. “My mom was incredible … com-
ing, MD, spoke of his asso- Dr. Breving, a board-certified general
surgeon and chief of staff at National Park pletely devoted. She didn’t work outside the
ciation with the late S. Truett
Medical Center, is a prominent member of home, but she was interested in our educa-
Cathy, founder and CEO of Chick-fil-A, tion. We went to school and did a lot of home
the medical profession in Arkansas. Since
friends listened intently. Soon, one felt moving to the state in 2004, he has practiced schooling as well.
moved to deliver the story to the local paper, in Hot Springs. He has also been a member “When I was 10, everything changed,”
The Sentinel-Record, which covered it in its of the Arkansas Medical Society and just this said Dr. Breving, recalling how the disease
September 14, 2014 edition. When The Jour- month, became the newest member of the firmly took hold of his mother. “Because of
nal caught wind of the story, it seemed ap- AMS Board of Trustees. Dr. Breving is excited her disease process, she couldn’t hold down
propriate to share it with you, his physician
about the opportunity to serve, and he says a job, nor would she accept financial assis-
colleagues in Arkansas.
he would not be the man he is today without tance.”
Upon Cathy’s recent passing, Dr. Brev- the generosity Cathy extended to him in the
ing could not help but reflect and speak of the early part of his life. In response, 16-year-old Breving went
philanthropist’s important role in his life – as to work. That sounds brave and mature for
a mentor, friend, father figure and sometimes A Modest Start a very young man, but he indicates another
benefactor. Dr. Breving’s life began modestly, in Cin- motivation. “There was no other choice,” he
cinnati, Ohio, where, from a young age, he and said, simply. “My sister, Becky, was too young
This isn’t a story he shares to puff him-
his younger sister lived with a mother who suf- to work. Child support wasn’t what it is now.
self up, he stressed. However, it’s a story he
fered from mental illness. His father was not Frequently, there was no money coming in.
cannot forget – one for the books, as they
around much. “My mother and father were Everything I made went to keep the family
say, especially in a world where bad news
abounds. “Seems like today when you open divorced,” said Dr. Breving. “I can’t blame him fed and alive. We rarely had more than one
the paper or turn on the TV, it’s [bad news],” for that. Living with a person with untreated of our utilities on. I’ll tell you, taking baths in
he said. “To see an exceptional story about a schizophrenia will drive you crazy if you don’t zero degree weather, in the Cincinnati winter,
complete stranger, who helped another per- separate yourself from the situation.” without hot water, is a chilly experience.”
128 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111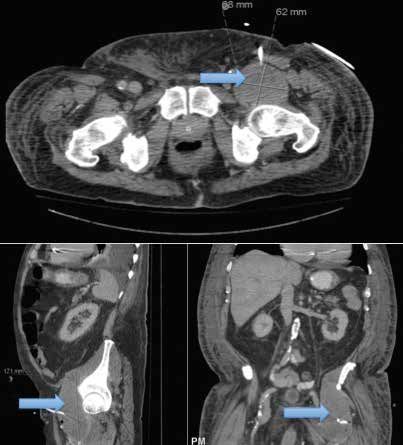
Enter Truett Cathy in him. “He invited me to his farm in Atlanta,” Within minutes, son Dan Cathy had pulled
Without considering the fairness of it, said Dr. Breving, who was not used to such up outside in one of the first popular minivans
young Breving forged ahead. The year was attention. “We spent the weekend, rode mo- of the time. “It was a Voyager I think,” said
1980, and he was growing up fast. He kept up torcycles, walked the farm and talked about Dr. Breving, who, still stunned by this act of
his schoolwork and worked two jobs, the main life. He was an energetic, vibrant, genuine generosity, managed to help remove car seats
one being at the new Chick-fil-A restaurant person.” and toys before taking over the vehicle. “They
that opened up just outside walking distance. gave me the keys, and I drove away. It was
The man must also have been quite de-
“It sounds trite, but it’s true,” smiled Dr. Brev- surreal. I drove that thing until the tires just
termined by trait, judging by one of Dr. Brev- about came off of it.”
ing. “I literally walked to work … uphill …
ing’s favorite memories. Cathy truly wanted to
sometimes even in the snow. Luckily, it was For many years to come, Cathy’s gener-
fill a need for young Breving – one way or an-
often only one way. There was usually some- osity continued. “There were times when he
other. “First, he offered to adopt me,” recalled
one to give me a ride home at closing time.” helped with utilities – that was an issue for
the doctor, who politely declined out of loyalty
He had worked at Chick-fil-A for a couple a number of years,” said Dr. Breving. “And
to his own family, whom he wanted to provide
of months by the time the establishment held through Chick-fil-A, he helped me get a schol-
for.
its Grand Opening. CEO S. Truett Cathy was arship that helped me attend undergraduate
among the executives who attended the fes- That settled, Cathy pressed onward, ana- school at Ohio State.” (At that time, employees
tive occasion, which represent a new begin- lyzing the situation and quickly arriving upon who worked for Chick-fil-A for a certain period
ning not only for Chick-fil-A in the community, a need he could fill. of time, could earn partial scholarships to help
but for Breving as well. with school.)
Decision made, Cathy picked up the
The store operator, knowing of Breving’s phone. “He called his son – also an executive “My grades were good,” said Dr. Breving,
difficult circumstance, made a point to tell for Chick-fil-A,” recalled Dr. Breving. “And he who procured a number of scholarships and
Cathy about the hard-working young em- says ‘Son, I got Bert here, and he needs a car. school loans that allowed him to work toward
ployee. In turn, Truett took a personal interest Will you give him your car?’” an undergraduate degree and, later, attend
Mercy Clinic Fort Smith Let us Keep IT
Communities seeks Under Control
• Network Design
Hospitalists BC or BE in • Managed Services
• IT Consulting
Internal Medicine to • Peace of Mind
work at Mercy Hospital
in Fort Smith, AR.
Applicants must reference
job code H1981 and mail c.v.
and cover letter to:
Sarah Wilson
Mercy Physician Recruiter
Mercy Clinic Fort Smith We work to be
2901 S. 74th St the best in the
state of Arkansas
Fort Smith, AR 72903
501.907.4722 www.pcassistance.com
NUMBER 7 DECEMBER 2014 • 129
medical school. Even so, Cathy’s financial as-
sistance was what set him solidly on his future
Put your business or
course. “If not for his help, I would not have
been a doctor. [It] wasn’t even on my radar
screen before I met Cathy. My goals were
service in the hands short-term at that time – ‘how are we going
to survive the next two months? ‘How will we
of 4,400 Arkansas
keep the water on?’
“Now I’m a surgeon.”
physicians. Forging His Own Trail
While attending Ohio State, Dr. Breving
worked as a ward clerk and OR scheduler in
the operating room. He was touched by the
excitement of the environment, the strive for
excellence he witnessed there, and the need
he saw in the surgeons to “fix” things. In the
years since, he has put himself in that same
environment, giving his all day after day for the
betterment of his own patients. “I have to be
at the top of my game,” he said. “With every
operation, I have someone’s life in my hands.”
Dr. Breving graduated from medical school
in 1993 and practiced in Birmingham, Ala-
bama, until moving to Arkansas in 2004. He is
married to Internist Nannette Vowell, and the
two have three children.
As the newest trustee for the Arkansas
Medical Society, Dr. Breving looks forward to
House of Delegates meetings and other oppor-
tunities to learn more and contribute more to
the legislative process. During medical school,
he was involved in the American Medical Soci-
ety as a student, and he looks forward to work-
ing with AMS on issues of medical politics and
decision-making.
“The next few years are going to be chal-
lenging – with the proliferation of electronic
medical records, the shrinking health care dol-
lar, increased stress placed upon health care
providers and with people’s increasing expec-
tations of quality related to their medical care,”
said Dr. Breving. “When you put stress on the
system, sometimes it will break. Physicians
For advertising information, will still need to provide medical care if it does.
contact Penny Henderson at We’re going to encounter challenges that will
require due diligence by the AMS as well as the
501.224.8967 or penny@arkmed.org state medical board more and the physicians
of our state.”
130 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111Time to Pay it Forward Dr. Breving hopes someday to affect brother made for her, and the help he received
Cathy gave Dr. Breving much that was another person through the type of kind- from Truett Cathy. “I told myself, ‘if Bert can
vital to his early life. High on a list of gifts ness and generosity Cathy showed to him. In get into college by working hard and making
that included financial support, a car, and preparation, he believes he must focus first smart decisions, I can, too,’” she said. “Bert
even Breving’s first tailored suit, was time. on himself. “I think you’ve got to get your was clever and funny, and he kept my spirits
“It’s easy for people to write a check when own life straight before you can help some- up with laughter. He did the responsible thing:
there’s a cause that they want to support,” body else’s life,” he said. “Truett picked me, he stayed with me to provide for me. I’m
a complete stranger to him. He found me at eternally grateful to Mr. Cathy for recognizing
said Dr. Breving. “Sometimes, the most valu-
a pivotal point in my life. The assistance that Bert’s character and intelligence and giving
able thing is time. We spent time together.
he provided changed the course of my life. him a helping hand. Mr. Cathy’s generosity
There was some mentoring that went along
had a profound effect; he steered Bert onto a
with that – he would talk to me, educate me “I was thinking of that when he died.
course of success.”
about life, about the way people should act.” What have I done? Sure, I’m trying to provide
the best patient care, and be nice to people, The Journal appreciates Robert Breving,
Cathy made a habit of helping others.
but I can’t say I’m mentoring someone right MD, for sharing his inspirational story of cour-
The restaurateur and philanthropist was also
now. It’s something I owe it to him to try to age, commitment and a generous “hand up.”
an author, educator, Sunday School teach-
do, and I’d like to do that for somebody else.” Learn more about Truett Cathy at truettcathy.
er, scholar, mentor and supporter of those com. Among other things, you will find Cathy’s
around him. “Hundreds –literally thousands Perhaps he has been more of a mentor “Eleven Dos and Don’ts of Proven Entrepre-
– of people were affected by his generosity,” already than he gives himself credit for. Sis- neurial Success,” as well as information about
reflected Dr. Breving. “His family is like this ter Rebecca Rogers called her brother Bert WinShape Foundation, which he bore out of
too ... genuine and interested in providing her “role model” growing up. A realtor in the his desire to “shape winners” by “helping
a wholesome, quality product and creating luxury residential market of Saddle River, young people succeed in life through scholar-
wholesome, quality people.” New Jersey, Rogers recalls the sacrifices her ships and other youth-support programs.”
Grow.
Office and Medical space available for
lease at The Village at Rahling Road.
live play work Office sites from 1 to 20 acres available
throughout Chenal Valley.
Reasons to work in Chenal Valley,
a live, work and play community:
• 34 neighborhoods as well as
apartment and condominium
communities
• Arkansas’ best shopping at
The Promenade at Chenal
• Restaurants, banks, Baptist Health,
Wal-Mart, Kroger Marketplace,
St. Vincent West
• Chenal Country Club and two
championship golf courses
shop chenal.com | 501.821.5555
NUMBER 7 DECEMBER 2014 • 131A C L O S EA CLOSER
R L O O K
LOOK A T
AT QUALITY Q U A L I T Y
EDITORIAL PANEL
Lynda Beth Milligan, MD, FAAFP, CPE, CHCQM; Michael Moody, MD; David Nelsen, MD, MS;
Steven Strode, MD, MEd, MPH; J. Gary Wheeler, MD, MPS
Engage patients for better
health care, lower costs
reputation.1 According to the study, practice’s current level of engage-
BY LYNDA BETH MILLIGAN, MD,
FAAFP, CPE, CHCQM “hospitals with low patient experience ment as well as the range and type of
scores are four times more likely patients’ engagement habits. Starting
I
t seems like everyone is talking to have poor reputation scores.” with a comprehensive plan for the
about patient and family There is solid data that practice will save time and resources in
engagement. But providing demonstrate that more actively the long term.
effective patient engagement that engaged patients incur lower While no provider could oper-
achieves better, more cost-effective costs. One study found patients ate without the telephone, patient
outcomes can be a challenge. with lower “patient activation communication has expanded with
Patient engagement — ongoing scores” had a 21 percent higher email and other electronic formats. A
and constructive dialog between the health care cost the following year, patient portal — an online web-based
patient, patient’s family and provider when compared with patients with connection that facilitates information
with the aim of improving overall higher patient activation scores.2 sharing and two-way communication
health — is a cornerstone of several Improving patient engagement in a secure format — is the next step.
of the Centers for Medicare and provides an opportunity to access About 40 percent of office-based physi-
Medicaid Services’ (CMS) current bonus Medicare payments. The cians currently have a portal through
initiatives, including patient-centered CMS requires providers to meet several their EHR system. Cleveland Clinic
medical homes (PCMH) and Stage 2 patient engagement benchmarks says its portal is crucial in coaching
of Meaningful Use (MU). to improve quality. Stage 2 of MU patients and eliminating unnecessary
requires that, for providers to earn office visits.3
WHY ENGAGEMENT MATTERS bonus Medicare payments, 5 percent A patient portal allows a patient
As the PCMH model becomes of patients must log onto and upload to access his or her personal health
more widely used, it is increasingly data via a patient portal; more than 50 information securely and reliably from
important to include the patient’s percent of a clinician’s patients must a personal computer, cell phone or tab-
voice. Patients who are engaged receive timely online access to health let. Be certain your EHR system is op-
with a health care provider and information, including diagnostic test timized for mobile devices, because us-
can communicate easily regarding results and medication lists; and more age is increasing. Overcoming patient
their care can be expected to than half of patients receive a clinical resistance to using your patient portal,
achieve better outcomes and summary of his or her office visit especially among older, less tech-savvy
have higher levels of satisfaction within one business day. patients, will be crucial to its success.
with their providers. A National Research published in the Annals of
Research Corporation study shows ENGAGING EFFECTIVELY Family Medicine4 reports that a prac-
a direct correlation between patient Providers who want to increase pa- tice must both actively promote and
experience and an organization’s tient engagement must first assess the integrate portals into routine patient
THE ARKANSAS FOUNDATION FOR MEDICAL CARE, INC. (AFMC) WORKS COLLABORATIVELY WITH PROVIDERS, COMMUNITY GROUPS AND OTHER STAKEHOLDERS TO PROMOTE
THE QUALITY OF CARE IN ARKANSAS THROUGH EDUCATION AND EVALUATION. FOR MORE INFORMATION ABOUT AFMC QUALITY IMPROVEMENT PROJECTS, CALL 1-877-375-5700.
132 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111A C L O S E R L O LOOK
A CLOSER O KAT QUALITY
A T Q U A L I T Y
care. Small- to medium-size practices Cleveland Clinic is experimenting n Health management apps that
are unlikely to engage in large-scale with a series of pilot projects that allow provide more comprehensive
promotion; however, success has been patients to enter data into their own information such as WebMD
reported with low-cost methods. health records via the portal. The data n Chronic disease management apps
Eight small practices that used become part of the clinical work- to help manage the treatment
an interactive preventive health flow, and let physicians track patient of a specific condition such
record (IPHR) were studied for over progress and potentially modify care as asthma or hypertension
two years.4 The IPHR provided between visits.3
patients with personally tailored Look for other opportunities As technology advances and more
recommendations and resources to engage patients outside of usual information becomes available, it will
for chronic conditions and preven- business hours. Modern technology be increasingly important to simplify
tive services. More than 25 percent makes this relatively simple and data so a patient can understand and
of patients created an IPHR ac- inexpensive for most providers. Social easily apply it to his daily life. Most pa-
count. The high utilization rate was media options such as Facebook, tients want to know what to do to help
credited to using these methods: Twitter, YouTube and Instagram are themselves. Patients are more likely to
n Use a team approach to notify popular and successful ways to educate make positive health changes if they
and encourage patients about and message patients. take responsibility for their health and
the benefits of the IPHR, Providers can use these channels feel invested in health care treat-
not just the physician to address general health issues and ment and services. The more patients
n Provide the ability to topics without increasing overhead. understand, the more likely they are
view lab results The Center for Social Media at the to ask questions, learn, and obtain the
n Stress the importance of Mayo Clinic reports zero cost for the care that meets their specific needs.
the IPHR for patients with Mayo Clinic’s social media (Facebook, Providers can encourage this by team-
chronic conditions YouTube and Twitter) and $75 annu- ing up with patients, encouraging and
n Customize treatment plans ally for a customized blog. enabling them to take responsibility for
n Include the imprimatur of the Mobile device “apps” are increas- their health and quality of life. s
patient’s personal clinician. Online ingly popular with younger, more
personal health records offered by highly educated urban/suburbanites. Dr. Milligan is vice president, corporate
Internet companies or health plans An app is software designed for mobile medical director with the Arkansas
did not provide this important ele- devices such as cellphones and tablets Foundation for Medical Care.
ment of gravitas. that extends the device’s capabilities.
Apps are increasingly the standard REFERENCES
Cleveland Clinic says that allowing pathway to connect to the Internet for 1. Davies E. Cleary D. Hearing the pa-
patients to log on through the patient mobile computing. tient’s voice? Factors affecting the use of
patient survey data in quality improve-
portal, view their provider’s schedule A November 2011 Pew Research ment. Quality and Safety in Health
and make their own appointments was Center study reported that 34 percent Care 2005; 14: 428-432
one of the Clinic’s earliest and most of adults with a cell phone or tablet 2. Hibbard J. Greene J. Overton V. Pa-
successful changes.3 computer had downloaded an app. tients With Lower Activation Associ-
ated With Higher Costs. Health Aff
Ongoing patient education en- However, only two-thirds reported Feb. 2013 vol. 32 no. 2 216-222
sures patient satisfaction and ongoing actually using apps; about half on a 3. Rowe J. 5 ways Cleveland Clinic
engagement.3 Patient education should weekly basis.5 improved its patient engagement strate-
gies. Healthcare IT News Oct. 1, 2013
actively involve family members and Apps that are currently being used
blog post
caregivers. Providing clear and concise successfully in clinics include: 4. Hirsch M. Study: Tailored team ap-
written instructions after each visit n Dietary apps for food proach to portal promotion boosts
will ensure the best outcome. Cleve- education, calorie tracking patient engagement. FierceEMR.com
Sep. 15, 2014
land Clinic found that patients want to and weight management
5. Purcell K. Pew Research Center Half of
know two things: what’s going on with n Exercise apps to track walking, adult cell phone owners have apps on
them and what’s going to happen next. exercise and activity levels their phones. Pewinternet.org Nov.2, 2011
NUMBER 7 DECEMBER 2014 • 133SCIENTIFIC ARTICLE
Back Pain – An Ominous Harbinger
of Spinal Cord Infarction
Vidya Pai, MD1; Yogita Rochlani, MD2; Kinshuk Sahaya, MD3
1
Department of Internal Medicine-Pediatrics, UAMS
2
Department of Internal Medicine, UAMS
3
Department of Neurology, UAMS
A
50-year-old, right-handed and proprioception with a sensory level up (SCI) (Figure 1A-E). Additional laboratory in-
Caucasian man with a his- to T12 to pinprick testing. Ankle reflexes and vestigations were negative for autoimmune,
sphincter tone were absent with mute plantar infectious, inflammatory or neoplastic causes.
tory of diabetes mellitus,
reflexes. Emergent magnetic resonance im- Subsequent computed tomography angio-
hypertension, liver cirrhosis and age (MRI) of the spine with and without con- gram of the chest, abdomen, and pelvis was
hepatitis C presented to an out- trast demonstrated intramedullary T2 hyper- negative for aortic dissection. He was started
side hospital with bilateral lower intensity in the spinal cord at T10-11 level. For on low dose aspirin and aggressive physical
further delineation, T2-diffusion weighted im- therapy with only minimal improvement and
extremity weakness. One week prior
ages were obtained which showed restricted eventually discharged two weeks later to a re-
to presentation he stepped off a porch stair
diffusion in the central portion of the spinal habilitation facility with persistence of inconti-
which resulted in sudden onset left hip pain.
cord consistent with spinal cord infarction nence and neurologic deficits.
He had a dull continuous pain in his left hip
that worsened the following day with radia-
tion from the mid back down the posterior as-
pect of his left knee. Over the upcoming three
days his symptoms progressed to significant
weakness with involvement of the right lower
extremity. He reported taking large quantities
of non-steroidal anti-inflammatory drugs as
well as smoking both marijuana and meth-
amphetamines for alleviation of pain during
this time. He denied intravenous drug abuse,
fevers, night sweats, chest pain, recent upper
respiratory infection, or bowel or bladder in-
continence. Upon presentation to the outside
hospital, basic laboratory investigations were
normal. He underwent CT imaging of the cer-
vical, thoracic and lumbar spine without con-
trast that was negative for any acute process
and was subsequently transferred to our ter-
tiary care center for further management.
At the time of admission he was hemody-
namically stable and in no acute distress but
appeared anxious. The initial general physical
and systemic examinations were unremark-
able; however, his neurological examination
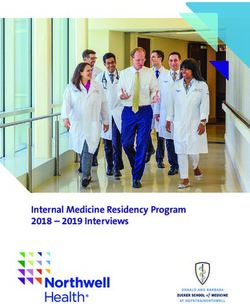
was significant for flaccid paralysis of both Figure 1 A-B: Sagittal T2 images of thoracic and lumbar spine showing T2 hyper-intense single in
lower extremities. He had normal vibration lower thoracic spinal cord through conus.
134 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111Figure 1C: Axial T2 hyper-intensity through the conus at T12-L1. 1D: High intensity signal on diffusion weight imaging (DWI) within the central spinal cord.
1E: Low intensity signal on apparent diffusion coefficient (ADC) indicating restricted diffusion.
DISCUSSION: cular supply for the anterior two thirds of the at supportive care and prevention of com-
Back pain is a frequent reason for outpa- spinal cord. Vascular compromise anywhere plications associated with immobility such
tient primary care visits. Although most cases along the anterior spinal artery distribution as decubitus ulcers, recurrent urinary tract
are due to musculoskeletal injury, the clinician clinically presents as acute paraparesis, loss infections and venous thromboembolism. The
should be alerted to symptoms of life threat- of pain and temperature below the level of psychological impact of spinal cord infarction
ening conditions particularly back pain asso- infarction with concurrent preservation of should also be addressed, as up to 25% of
ciated with either weakness or paralysis. The vibration and proprioception, and impair- patients will have some heightened level of
causes of bilateral lower extremity weakness ment of bowel and bladder function.1 Once anxiety or depression.3
can be divided into the following classifica- the suspicion for SCI arises, MRI is the initial In conclusion, SCI should be considered
tions: spinal cord disease, peripheral nerve diagnostic modality of choice. Abnormali- in the differential diagnosis of any patient
disease, brainstem stroke, neuromuscular ties on T2 weighted sequences are seen in presenting with back pain and acute paraple-
disorders, and muscular disease. As with all more than 90% of SCI cases but these are gia. Early recognition and risk factor modifi-
neurologic conditions, a thorough history and not specific. Sagittal MRI of anterior spinal ar- cation is essential to slowing the progression
physical examination are crucial to accurate tery infarction demonstrates isolated “pencil- of the disease.
diagnosis and should be supported by labo- like” area of T2 hyper-intensity involving the
ratory data and imaging. Important clues in central medullary region often encompassing ACKNOWLEDGEMENTS:
the medical history include initial presenting more than 2 vertebral segments. Axial T2 se- The authors would like to thank Drs. Rohan
symptoms (pain vs. weakness and numb- quences may show bilateral hyper-intensities Samant and Jennifer McCarty of the Depart-
ness), chronicity (acute vs. chronic), and pro- most confined to anterior horns giving the ment of Radiology at the University of Arkan-
gression of symptoms (step-wise vs. progres- “owl eye” appearance.2 Etiologies of SCI may sas for Medical Sciences for providing inter-
sive). A systematic physical examination can include trauma, hypotension, atherosclerosis, pretation of the radiological images.
often provide clues for the underlying etiology fibrocartilaginous embolization, vasculitides
of back pain. Severe neurologic compromise and prothrombin mutations; however, the REFERENCES:
indicated by a loss of sphincter tone, acute true etiology in most cases remains unclear. 1. Satran R. Spinal cord infarction. Stroke.
urinary retention or saddle anesthesia war- Our patient had multiple vascular risk fac- Apr 1988;19(4):529-532.
rants emergent intervention. Furthermore, tors including poorly controlled diabetes, hy-
arthralgias may suggest a rheumatologic 2. Nogueira RG, Ferreira R, Grant PE, et al.
pertension, and polysubstance abuse — all
origin while cutaneous findings such as livedo Restricted diffusion in spinal cord infarc-
of which we hypothesize contributed to his
reticularis and purpura may suggest systemic tion demonstrated by magnetic resonance
stroke. Furthermore, his clinical presentation
disease such as vasculitides. line scan diffusion imaging. Stroke. Feb
of weakness and numbness with preserva-
2012;43(2):532-535.
Despite being less common than cerebral tion of the posterior column function, in addi-
strokes, spinal cord infarction (SCI) accounts tion to T2 hyper-intensity on MRI was highly 3. North NT. The psychological effects of spi-
for approximately 1.2% of all strokes.1 These suggestive of spinal cord infarction. While nal cord injury: a review. Spinal Cord. Oct
infarctions frequently occur in the distribution only a small fraction of patients show clinical 1999;37(10):671-679.
of the anterior spinal artery - the primary vas- improvement, treatment is primarily aimed
NUMBER 7 DECEMBER 2014 • 135CASE STUDY
Falls and Comorbid Conditions among
Community Dwelling Arkansas Older Adults
from a Population-based Survey
Masil George, MD;1 Gohar Azhar, MD;1 Greta Kilmer, MS;2 Sabra Miller M. Ed;3 LaTonya Bynum, BS;3 Appathurai Balamurugan, MD, MPH3,4
1
Department of Geriatrics, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR,
2
Research Triangle Institute, Atlanta, GA, 3Arkansas Department of Health, Little Rock, AR,
4
Department of Family and Preventive Medicine, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR
ABSTRACT one day.1 Falls among older adults can lead to METHODS
The prevalence of self-reported falls death, disability, and admission to a long-term
and associated comorbid conditions among care facility and substantial medical costs.2, 3 In Data Sources
community dwelling Arkansas older adults 2010, there were 10, 407 hospitalizations among The Behavioral Risk Factor Surveillance System
(ages 65 years and older) was estimated us- Arkansas older adults with an average length of (BRFSS).
ing data from the 2010 Behavioral Risk Fac- stay of about 5 days. The average charge for
The BRFSS is the world’s largest telephone
tor Surveillance System survey. 1,653 Ar- falls-associated hospitalization was $22, 412. 4 survey used to track health risks of Americans
kansas older adults were surveyed. Eighteen Several risk factors for falls among older adults aged 18 years and older. Since 1984, it has been
percent of them had sustained a fall at least have been studied, including older age, white administered by the 50 states in the US through
once in the past three months prior to the race, history of falling, use of special equipment funding from the Centers for Disease Control and
survey period. After adjusting for age, gen- such as cane or walker, abnormalities in gait or Prevention (CDC) to a random sample of non-
eral health, coronary heart disease, diabetes balance, muscle weakness, visual impairment, institutionalized community dwelling adults. The
status and quality rest or sleep in a multino- use of psychotropic drugs and sleep disorders. survey uses the disproportionate stratified random
mial logistic regression, we found that older 5, 6
Currently, there is no clinical consensus on digit dialing methodology; additional information on
adults with visual impairment (OR=1.47; a standardized screening instrument to assess survey design and methodology can be found in
95% CI: 1.02, 2.12), and those who use the risk of falls among older adults.7 Multiple BRFSS Users Guide (Chapter Seven).14
special equipment (OR=2.85; 95% CI: 1.94, strategies or guidelines for the prevention of falls
The BRFSS survey collects information on
4.19) were more likely to have sustained a among older adults have been recommended,
survey respondents’ demographic and behavioral
fall. An integrated multidisciplinary approach including exercise (tai chi, flexibility and strength
characteristics, and co-morbid conditions (pres-
in caring for older adults is imperative for training exercise), vitamin D supplementation,
ence of coronary heart disease, stroke, diabetes),
preventing falls and fall-related injuries. This and multifactorial interventions.8-10
overall general health, visual impairment (difficulty
can also reduce fall-related hospitalizations
Although, many risk factors for falls among seeing or recognizing a friend across the street), use
and potentially result in substantial cost sav-
older adults have been studied, only a few stud- of special equipment (i.e. cane, wheel chair, special
ings as well as improve the quality of life of
ies have evaluated the association of falls and bed or a special telephone), quality rest or sleep,
older Arkansans.
the co-morbid conditions such as presence of hours of sleep, and daytime sleepiness. The survey
coronary heart disease, stroke, diabetes, qual- has been continuously administered in Arkansas
INTRODUCTION ity rest or sleep, and overall general health.11-13 since 1993. In the years 2003, 2008 and 2010, a
Falls are the leading cause of injury re- Using the population-based behavioral risk fac- falls core section which consists of two questions
lated deaths among older adults. According to tor surveillance system (BRFSS) survey, we as- was asked among adults age 40 years and older
the Centers for Disease Control and Prevention, sessed the association between the falls among in Arkansas. The questions specific to core section
15.9% of all US adults 65 years and older (older older Arkansans and some selected co-morbid on falls are: “In the past three months, how many
adults) fell at least once during the preceding conditions that can predispose to falls. We also times have you fallen?,” and “How many of these
three months and approximately 31.3% of those set the stage for a discussion of some of the falls caused an injury? By an injury, we mean the
who fell sustained an injury that resulted in a prevention strategies to combat this frequently fall caused you to limit your regular activities for at
doctor visit or restricted their activity for at least devastating condition among our older adults. least a day or to go see a doctor?”
136 • THE JOURNAL OF THE ARKANSAS MEDICAL SOCIETY VOLUME 111Statistical Analysis Approximately 18.0% of the older adults 65 sleep (21.2%, p=0.0239), had history of coronary
Statistical analysis was carried out with SAS years and older had fallen at least once in the past heart disease (25.0%, p=0.0163), diabetes (24.3%,
version 9.3 (SAS Institute, Cary, NC) and SUDAAN 3 months. When demographic characteristics of p=0.0106), had difficulty seeing a friend across the
version 11.0 was used specifically to account older adults who had fallen in the past 3 months street due to visual impairment (24.9%, p=0.0010),
for variable weights and stratified design. We re- were assessed (Table 1), a higher proportion of and those who used a special equipment (34.8%,
stricted our analysis to the 2010 BRFSS survey those between 85 years of age or older had fallen p 50K 14.9 (2.5)
Wald F test was used to assess statistical (OR=2.85; CI: 1.94, 4.19) had nearly
Education 0.9786
significance of odds ratios. three times higher odds of sustaining a
Some high school or less 17.2 (2.7)
fall compared to those who did not use
High school graduate 17.9 (1.9)
RESULTS special equipment. Use of special equip-
Some college 18.4 (2.4)
A total of 1,653 older adults 65 ment such as cane or wheel chair for mo-
College graduate 18.6 (2.3)
years and older were surveyed. Higher bility may indicate some degree of physi-
Current Smoker 0.1529
proportion of those surveyed were 65-74 cal impairment or disability among older
Yes 14.1 (2.9)
years of age (53.8%), females (57.2%), adults and puts them at an increased risk
No 18.6 (1.2)
whites (93.1%), those who had an annual of falls. Also, older adults who had visual
Exercise 0.0936
household income less than twenty five impairment (OR=1.47; CI: 1.02, 2.12) had
Yes 16.5 (1.4)
thousand dollars (41.7%), and those who fifty percent higher odds of sustaining a
No 20.5 (2.0)
were high school graduates (37.2%). fall than those who did not have a visual
* - Standard error
NUMBER 7 DECEMBER 2014 • 137impairment. Evaluating older adults for visual im- phones, or those residing in nursing homes, long REFERENCES
pairment should be part of routine clinical visits to term care facilities or other institutions. Second, the 1. Centers for Disease Control and Prevention.
prevent debilitating effects of falls. self report design of the BRFSS could have affected Self-reported falls and fall-related injuries
our results because socially desirable responses among persons aged > 65 years– United
The observations from our study emphasize
tend to be over reported and, therefore, less accu- States, 2006. MMWR Weekly. March 7,
the need for an integrated approach to prevent falls
rate. Third, because of the cross-sectional nature of 2008/57(09); 225-229.
among older adults. Currently, there is no clinical
the survey, one must use caution in making infer- 2. Stevens JA. Falls among older adults – risk
consensus on a standardized screening instrument
ences suggestive of causality based on the results. factors and prevention strategies. In: Falls free:
to assess the risk of falls among older adults. 15
Fourth, our study and its findings are limited to promoting a national falls prevention action
Screening for physical functioning/impairment, vi-
community dwelling Arkansas older adults. It does plan. Washington, DC: The National Council on
sual impairment and quality rest or sleep should be
not apply to Arkansas older adults residing in hos- the Aging; 2005.
an essential part of falls assessment. This can as-
pitals, nursing homes, long term care institutions 3. Stevens JA, Corso PS, Finkelstein EA, Miller TR.
sist in formulating strategies to prevent falls among
or any other facilities. Finally, survey respondents The costs of fatal and nonfatal falls among older
older adults. Multiple guidelines for the prevention
could be subject to recall bias and possibly could adults. Inj Prev 2006; 12: 290-5.
of falls among older adults have been recom-
have misinterpreted the wording of the question 4. Arkansas Hospital Discharge Data System,
mended, including exercise (tai chi, flexibility and
used to identify falls or insufficient rest or sleep. Health Statistics Branch. Arkansas Department
strength training exercise), vitamin D supplementa-
of Health. Accessed at www.healthyarkansas.
tion, and multifactorial interventions.16-18 In conclusion, our study demonstrates an as-
com on February 3, 2014.
sociation between falls and co-morbid conditions
The findings in this report are subject to a few
(use of special equipment, and visual impairment) 5. Fuller GB. Falls in the elderly. American Family
limitations. First, BRFSS is a telephone survey and
in a random, population-based study. Our findings Physician 2000; 61: 2159-68, 2173-4.
does not include persons without landline tele-
also suggest that assessment of sleep quality may 6. Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ.
be a useful aspect of fall pre- Will my patient fall? JAMA, January 3, 2007 –
Table 2. Co-morbid conditions among older adults with
vention strategies, although Vol 297, No. 1, 77-86.
falls, Arkansas, 2010 (N=1653).
this requires further evaluation. 7. Gates S, Smith LA, Fisher JD, Lamb SE. Sys-
Characteristics With Falls (% (SE*) P-value
For every older adult who falls tematic review of accuracy of screening instru-
Quality rest or sleep 0.0239
Yes 15.9 (1.5) and sustains injuries, a care- ments for predicting fall risk among indepen-
No 21.2 (1.8) giver is also impacted in some dently living older adults. JRRD. Vol. 45, No. 8,
Hours of sleep 0.4485 way, often increasing the over- 2008: 1105-1116.
Less than 6 21.8 (4.1) all stress. Because of the tre- 8. Guideline for the prevention of falls in older per-
6 or 7 16.5 (1.7) mendous physical, emotional sons. JAGS, 49: 664-672, 2001.
8 or more 18.2 (1.6)
and economic burden of falls 9. Gillespie LD, Robertson MC, Gillespie WJ, Lamb
Daytime sleepiness 0.0937
and fall-related injuries, strate- SE, Gates S, Cumming RG, Rowe BH. Interven-
Yes 19.7 (1.8)
No 15.8 (1.5) gies to streamline assessment tions for preventing falls in older people living in
General Health 0.0023 of fall risk and fall prevention the community. Cochrane database of system-
Excellent/Good 15.5 (1.3) is a priority and an integrated atic reviews 2009, Issue 2. Art. No.: CD007146.
Fair/Poor 23.4 (2.3) multidisciplinary approach in DOI: 10.1002/14651858.CD007146.pub2.
caring for older adults is there- 10. Chang JT, Morton SC, Rubenstein LZ, Mojica
Coronary heart disease 0.0163
fore essential. This can also WA, Maglione M, Suttorp MJ, Roth EA, Shekelle
Yes 25.0 (3.3)
No 16.5 (1.2) reduce fall-related hospital- PG. Interventions for the prevention of falls in
Stroke 0.1448 izations and potentially result older adults: systematic review and meta-anal-
Yes 23.4 (4.0) in substantial cost savings as ysis of randomized clinical trials. BMJ, Vol. 328,
No 17.5 (1.2) well as improve the quality of 20 March 2004: 1-7.
Diabetes 0.0106 life of older Arkansans. 11. Lawlor DA, Patel R, Ebrahim S. Association be-
Yes 24.3 (2.9)
tween falls in elderly women and chronic dis-
No 16.2 (1.2)
ACKNOWLEDGMENT: eases and drug use: cross-sectional study. BMJ
Difficulty seeing 0.0010
The authors would like to 2003, Sep 27; 327 (7417): 712.
Yes 24.9 (2.6)
No 15.4 (1.2) acknowledge the funding 12. Schwartz AN, Vittinghoff E, Sellmeyer DE et al.
Use special equipmentYou can also read