Sleep Disorders Guidance for Primary Care - National Advisory Group for Respiratory Managed Clinical Networks
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Sleep
Disorders
Guidance for Primary Care
National Advisory Group
for Respiratory Managed Clinical NetworksPresentation
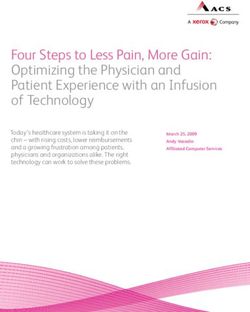
Patient complaining of difficulty sleeping, ongoing fatigue, poor concentration and/or irritability
Assessment
Patient History
In diagnosing patients with sleep problems it is important to take a good history (Appendix I)
Diagnostic Tools
Sleep Diaries (Appendix II)
Epworth Sleepiness Scale (ESS) to measure day time sleepiness can be useful to support
diagnosis and inform onward referral, the questionnaire can be accessed via the British Lung
Foundation Website (http://www.blf.org.uk/Page/Epworth-Sleepiness-Scale)
Diagnosis
Sleep disorder linked to adjustable factors
w prescribed medication w use of stimulants (such as caffeine, alcohol, cigarettes, drugs)
w vigorous exercise before bed w important recent life events (such as bereavement)
Sleep disorders linked to depression, worry and anxiety, nocturnal panic attacks
Sleep disorder linked to parasomnias
Sleep disorder linked to obstructive sleep apnoea
Management
Sleeping disorder linked to adjustable factors
Sleep hygiene
Sleep disorders linked to depression, worry and anxiety, nocturnal panic attacks
Treat depression or anxiety e.g. drug or cognitive behavioural therapy
Management of patients with secondary insomnia
Sleep hygiene
Sleep disorder linked to parasomnias
For restless legs check ferretin, consider non-drug based measures or non-ergot dopamine
antagonist drugs for severe cases
For other parasomnias consider referral to sleep service as per local protocol
Sleep disorder linked to obstructive sleep apnoea
Referral on to sleep service as per local protocol
2 Sleep Disorders - Guidance for Primary CareInsomnia
Patients with insomnia may report difficulty falling asleep, trouble staying asleep or frequent wakening,
wakening too early and being unable to get back to sleep, or still feeling tired after waking. Insomnia
can be grouped into primary and secondary (or co-morbid) insomnia. Patients can have more than one
diagnosis. Depression and anxiety underpin insomnia in up to 50% of cases, and they frequently co-
exist. Primary insomnia is a sleep disorder which is usually diagnosed after excluding other causes such
as a medical, psychiatric, or environmental cause.
Secondary causes of insomnia and appropriate treatments
Secondary Cause Treatment
Depression Treat depression (antidepressants, cognitive
behavioural therapy)
Anxiety Treat anxiety (drug or psychological therapies, eg CBT)
Obstructive CPAP or mandibular advancement device
Sleep Apnoea (Refer to Respiratory Medicine if history compatible)
Excess alcohol Interventions to reduce intake or promote abstinence
Physical health problems Treat symptoms
(such as pain or dyspnoea)
Delayed sleep phase disorder Change work hours; melatonin in the evening and light box
(a circadian rhythm abnormality) in the morning
Illicit drug use Interventions to reduce drug use
Parasomnias For restless legs check ferritin, consider non-drug-based
(restless legs, other abnormal measures, or non-ergot dopamine antagonists for severe
activities during sleep) cases; for other parasomnias refer to sleep medicine
Taking a good history is important for diagnosing insomnia and identifying underlying causes. Sleep
diaries can be useful to provide patients with insight in to their actual sleep habits, and also in reflecting
sleep trends, such as erratic schedules, or identifying predominant sleep patterns such as taking a long
time to fall asleep, frequent awakenings, or early morning awakenings. They can provide a starting
point for the management of sleep problems in a personalised manner, and can be used to monitor
progress of certain treatments.
Sleep Disorders - Guidance for Primary Care 3Management of insomnia
For all patients, following the basic principles of good sleep hygiene may be beneficial. For patients
in whom a cause for insomnia is identified, begin by treating the underlying condition. About 30% of
patients with primary insomnia will improve with basic sleep hygiene alone.
Cognitive behavioural therapy (CBT) has been shown to be an effective treatment for insomnia. It
aims to address the various cognitive and behavioural aspects of insomnia using a combination
of interventions such as behavioural strategies (bedtime restriction, stimulus control therapy, and
relaxation), education (sleep hygiene), and psychological therapies (including CBT).
Pharmacotherapy and psychological or behavioural interventions result in similar short-term
improvements, but psychological or behavioural treatments have persisting benefits that can also
improve with time.
Although drugs have their place in the management of insomnia, CBT or other non-
drug based interventions should be considered first. Hypnotic drugs are often used in the
management of insomnia in general practice. Different classes of sleep medication are often prescribed.
Local prescribing guidelines may vary and should be followed.
Drugs commonly used for insomnia
Drug Dose Side-effects
Melatonin M/R 2mg Usually well tolerated
Temazepam 10-20mg Sedation, confusion, amnesia, impaired
co-ordination, disinhibition
Zolpidem 5-10mg As for temazepam
Zopiclone 3.75-7.5mg As for temazepam
Melatonin is a pineal hormone that is naturally secreted in darkness. It is thought to signal sleep
onset and has some sleep promoting effects. It is licensed for use in adults aged greater than 55
years old for periods of 13 weeks at a time. Please note that this has not been approved by SMC.
Hypnotic drugs (benzodiazepines or ‘z’ drugs such as zopiclone) are often prescribed for
insomnia. Tolerance and dependence are common concerns despite the contradictory evidence in
many clinical trials.
Shorter acting hypnotics (zolpidem) are preferred for insomnia with delayed sleep latency
(difficulty getting to sleep).
Medium acting hypnotics (temazepam or zopiclone) are preferred for patients who wake in
the middle of the night. To limit risk of dependence or tolerance, prescribers can tell patients to
use hypnotics ‘as needed’, with a maximum frequency per week (ie no more than three nights
per week).
Benzodiazepines have significantly fewer side effects than sedating anti-depressants and
sedating antipsychotics.
Sedating anti-depressants and anti-psychotics are often used as they generally do not result
in physical dependence, tolerance, or misuse. They do however have more side effects, and are
more toxic in overdose. There is also less evidence for their use in insomnia.
4 Sleep Disorders - Guidance for Primary CareObstructive sleep apnoea/hypopnoea syndrome
Obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is a disorder characterised by excessive
daytime sleepiness resulting from disturbed breathing during sleep; the primary causative factor is
obstruction of the airway. It affects about 4% of those reporting poor sleep in primary care and is more
common in people who are obese. In the absence of intrusive daytime sleepiness (ESS25Kg/m2
Neck size 17 inches or larger
Nasal congestion/blockage (permanent)
Receding lower jaw
Other causes of daytime sleepiness (in addition to primary and secondary insomnia):
Shift work
Sleep deprivation (quantity of sleep)
Narcolepsy
Hypothyroidism
Prescribed medication
Neurological conditions
Episodic partial or complete upper airway obstruction is usually associated with oxygen de-saturations
and arousals from sleep. Symptoms include chronic snoring, insomnia, gasping and breath holding,
un-refreshing sleep and daytime sleepiness. The Epworth Sleepiness Scale (ESS) is a useful tool to use
to see if people have excessive daytime sleepiness. It is important to remember that the ESS is only a
guide, and that patients can still be sleepy, with a normal ESS score.
There is an obligation for health professionals to advise professional drivers and machine operators of falling
asleep at work. Informing patients that they should never drive, or operate machinery, whilst sleepy is
important until the diagnosis is made. Once the diagnosis is confirmed, it is the patient’s legal responsibility
to inform the DVLA and their insurance company. Once on treatment, and using it with good effect, there
will be no issue with them driving. The diagnosis is usually made from a home sleep study, although a
minority of patients will require a more complex in-patient sleep study to confirm the diagnosis.
Management of obstructive sleep apnoea/hypopnoea syndrome
The treatment of OSAHS depends on the severity of the abnormality on the sleep study and how
symptomatic the patient is. For all overweight patients, weight reduction is of utmost importance, as
reducing weight can reduce the severity of the OSAHS. For patients with mild symptoms and a mildly
abnormal sleep study, a combination of weight reduction and a custom made mandibular advancement
splint would be the first line treatment. For those with severe symptoms, and a compatible sleep study,
continuous positive airways pressure (CPAP) at night would be the mainstay of therapy.
Sleep Disorders - Guidance for Primary Care 5Complex sleep disorders
Many complex sleep disorders are seen at the tertiary Sleep Clinics. Many patients present with
sleepiness, and so Respiratory Physicians have gained experience in investigating and treating these
conditions, even though these disorders may well have a neurological basis. These conditions include
Narcolepsy, Circadian Rhythm abnormalities and Parasomnias.
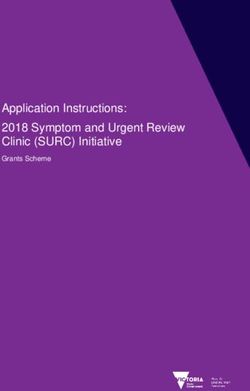
Referral for specialist assessment
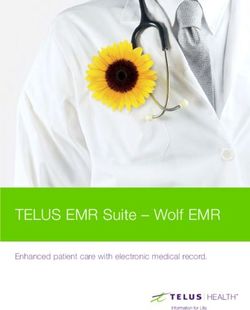
When referral on for support or further investigation is required, the flow chart below is intended to
steer referral to the most appropriate service.
Patient
presentation
possible adult
sleep disorder
GP assessment
Features of Features of Underlying Snoring, possible Other sleep problems
primary insomnia neurological disease condition evident apnoeas, or daytime (dream sleep
(e.g. parkinsons, (e.g. anaemia, sleepiness symptoms, shift
myotonic dystropy) hypothyroid, work, restless legs)
sedative medications
Exclude symptoms Refer neurology Assess and treat BMI? Refer sleep medicine
of other sleep Cardiovascular
disorder profile?
Discuss sleep Driving or
hygiene occupational issues?
Avoid caffeine Discuss associated
Consider anxiety/ sleep symptoms*
depression Patient complete
ESS questionnaire
Consider referral w Snoring w ESS ≥11 and/or
to Community w Occasional witnessed w Significant associated
Mental Health Team pauses in breathing sleep symptoms
w ESSAppendix I:
History taking questions
Can you describe your problem with sleeping?
Does it interfere with your function the next day (for example, feeling unrefreshed in the morning,
fatigued, having poor concentration or irritability)?
Can you tell me about your bedtime routine starting with the time you get into bed?
Time that you get to bed
Time to fall asleep
Awakenings (number, duration, do you know what causes you to awaken? Do you have any
associated symptoms, such as heartburn, coughing, shortness of breath, pain, anxiety or full bladder?)
Last awakening time in the morning
Time of rising from bed
Usual duration of sleep
How is your routine different at the weekends or during holidays? Do you have the same bedtime?
Do you do vigorous activity in the evening?
Information gained
Some patients think they do not get enough sleep but function well the next day. Technically
they do not have insomnia because the definition of insomnia includes “results in some form of
daytime impairment”.
Frequent changes in routine and vigorous activity just before bedtime can cause sleep problems.
Physical health problems are a significant cause (43%) of insomnia in primary care and will
require attention.
If the time in bed greatly exceeds the time asleep (for example, by a few hours), the patient may
have primary insomnia if no other causes are present. Spending less time in bed can lead to a
dramatic improvement in sleep quality and may decrease the fragmentation of sleep. Exposure to
computer screens in the hours before bed can delay sleep onset.
Sleep Disorders - Guidance for Primary Care 7How do you feel on awakening? Unrefreshed and still sleepy? Any symptoms such as headaches or dry mouth? Day sleepiness – falling asleep in waiting rooms, as a passenger in a car, or during lectures. Information gained Needs to consider obstructive sleep apnoea. Considering asking the patient to fill out the Epworth Sleepiness Scale, which measures levels of daytime sleepiness. Are there any symptoms of obstructive sleep apnoea (ask bed partner too if possible)? Such as heavy snoring, pauses in breathing, and gasping. Information gained Provides information on obstructive sleep apnoea. What other factors may interfere with sleeping? Use of stimulants (such as caffeine, alcohol, cigarettes, drugs). Other drugs may interfere with sleep. Important recent life events (such as bereavement). Information gained Ideally avoid use of stimulants after 6pm and if appropriate refer to smoking cessation. Oral decongestants (e.g. pseudoephedrine), asthma medications (e.g. short and long-acting bronchodilators), amphetamines and anti-depressants can cause insomnia. A trial without them is simple and can be potentially diagnostic. Do you take any naps? Ask about frequency, timing and duration. Where are you sleeping when you have the problem? Is the problem persistent when you sleep elsewhere (for example, when on holiday?) Is it persistent throughout the week and year? Information gained Long naps during the day can affect the quality of sleep at night. If the patient sleeps better when on holiday or at weekends, think of delayed sleep phase disorder, especially if he or she goes to bed after midnight. 8 Sleep Disorders - Guidance for Primary Care
Do you experience any of the following:
Low mood or lack of pleasure in some or most activities
Worrying a lot
Nocturnal panic attacks
Restless sleep
Leg or body twitching
Leg jerking (consider restless legs syndrome)
Shaking fits
Sleep walking or talking
Waking up in terror
Unusual night time behaviours
Information gained
Patients who answer yes to the first question may have depression and anxiety; consider using the
formal inventories for case finding.
The other symptoms may be related to parasomnias.
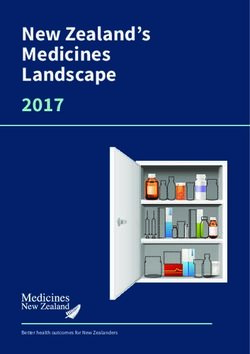
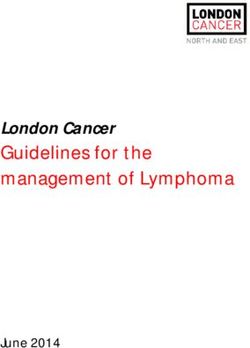
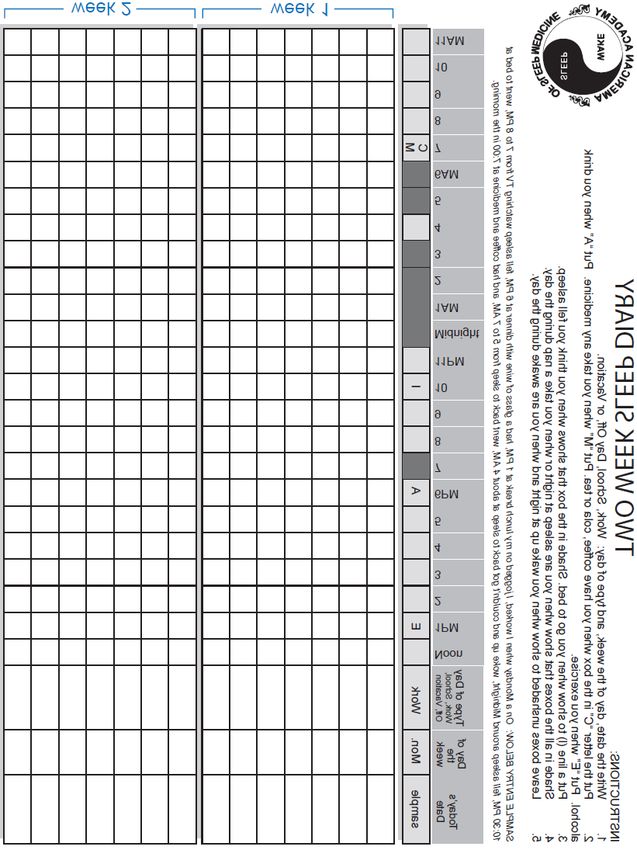
Sleep Disorders - Guidance for Primary Care 9Appendix II: Two week sleep diary
Instructions
1. Write the date, day of the week and type of day: Work, School, Day off or Vacation.
2. Put in the letter ‘C’ in the box when you have coffee, cola or tea. Put ‘M’ when you take
any medicine. Put ‘A’ when you drink alcohol. Put ‘E’ when you exercise.
3. Put a line (|) to show when you think you fell asleep. Shade in the box that shows when you think
you fell asleep.
4. Shade in all the boxes that show when you are asleep at night or when you take a nap during the day.
5. Leave boxes unshaded to show when you wake up at night and when you are awake during the day.
Type of day
Noon
1pm
6pm
Today’s date Day of
2
3
4
5
7
8
9
Work, School, Off,
the week Vacation
Sample Mon Work E A
10 Sleep Disorders - Guidance for Primary CareSample entry below: On a Monday when I worked, I jogged on my lunch break at 1pm,
had a glass of wine with dinner at 6pm, fell asleep watching tv from 7 to 8pm, went to bed
at 10.30pm, fell asleep around midnight, woke up and couldn’t get back to sleep at about
4am, went back to sleep from 5 to 7am and had coffee and medicine at 7am in the morning.
Reprinted with permission from the American Academy of Sleep Medicine, www.aasmnet.org
Midnight
11pm
11am
1am
6am
10
10
9
2
3
4
5
7
8
9
C
|
M
Week 1
Week 2
Sleep Disorders - Guidance for Primary Care 11Design - Medical Illustration, NHS Lanarkshire
Pub. date: July 2015
Review date: July 2017
Issue No: 03
Authors: Dr Eric Livingston,
NHS Greater Glasgow and Clyde;
Dr Tom MacKay, NHS Lothian
Sleep Studies Working Group
(NAGRMCNs)
PIL.SLEEPC.02663.OYou can also read