Symptomatic pulmonary regurgitation secondary to redundant transvenous lead prolapse
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Case Rep Images 2020;11:101121Z01GC2020. Cortes et al. 1
www.ijcasereportsandimages.com
CASE REPORT PEER REVIEWED | OPEN ACCESS
Symptomatic pulmonary regurgitation secondary to
redundant transvenous lead prolapse
Guillermo Andres Cortes, Rahul N Doshi, Philip M Chang
ABSTRACT excessive TVLs slack. Challenges remain with long-
term TVLs management in young patients. Proactive
Introduction: The use of cardiac implantable lead management is recommended to ensure CIED
electronic devices (CIEDs) with transvenous leads benefit while reducing TVLs complications. When
(TVLs) in young patients continues to increase. extraction is considered, a superior/inferior approach
Challenges persist, particularly related to TVLs can afford tremendous versatility to maximize success.
complications. We present a unique case of redundant
lead prolapse into the right ventricular outflow tract Keywords: Congenital, Heart block, Pulmonary
(RVOT) causing symptomatic pulmonary regurgitation regurgitation, Slack, Transvenous lead
(PR). Case Report: A 23-year-old female with
congenital heart block underwent initial transvenous How to cite this article
(TV) pacemaker implant at age 9 years, followed
by new lead implants at age 20 due to lead fracture. Cortes GA, Doshi RN, Chang PM. Symptomatic
The original TVLs were abandoned. She developed pulmonary regurgitation secondary to redundant
progressive exercise intolerance and exertional transvenous lead prolapse. Int J Case Rep Images
dyspnea. Catheterization showed normal pulmonary 2020;11:101121Z01GC2020.
pressures; exercise testing indicated worsening
PR and limited LV functional increase. Imaging
confirmed significant lead prolapse of the original Article ID: 101121Z01GC2020
right ventricular (RV) lead causing PR. Extraction with
cardiac resynchronization therapy-pacemaker (CRT-P) *********
upgrade was recommended. A superior/inferior
extraction approach was employed for extraction doi: 10.5348/101121Z01GC2020CR
of all TVLs with CRT-P implant using the retained
venous access post-extraction. Post-implant imaging
revealed appropriately positioned leads, normalization
of left ventricular (LV) function, and trace tricuspid INTRODUCTION
regurgitation (TR) and trace-mild PR. Conclusion:
This case highlights an unusual complication of The use of cardiac implantable electronic devices
(CIEDs) with transvenous leads (TVLs) in pediatric
and congenital heart disease (CHD) patients has
Guillermo Andres Cortes1, MD, Rahul N Doshi1, MD, FHRS, substantially increased over the last three decades [1–
Philip M Chang1, MD, FHRS 3]. Despite their benefits, challenges remain that are
Affiliation: 1Department of Medicine, Division of Cardiology/ inherent to TVLs, their implantation and follow-up in
Electrophysiology, University of Southern California/Keck growing patients, mainly those with unconventional
Medical Center of USC, Los Angeles, California 90033, USA. cardiac structural anatomy [3, 4]. In young patients,
Corresponding Author: Guillermo Andres Cortes, MD, it is common practice to introduce additional slack to
Department of Medicine, Division of Cardiology/Electro- compensate for anticipated growth; however, redundant
physiology, University of Southern California/Keck Medi- lead slack can result in mechanical and hemodynamic
cal Center of USC, Los Angeles, California 90033, USA;
complications [1–5].
Email: andrescortes.md@gmail.com
We present a unique case of a patient with TVLs
prolapse into the right ventricular outflow tract (RVOT)/
Received: 02 April 2020 proximal pulmonary artery resulting in significant
Accepted: 15 April 2020 symptomatic pulmonary regurgitation (PR).
Published: 13 May 2020
International Journal of Case Reports and Images, Vol. 11, 2020. ISSN: 0976-3198
Int J Case Rep Images 2020;11:101121Z01GC2020. Cortes et al. 2
www.ijcasereportsandimages.com
CASE REPORT echocardiogram on day 1 post-procedure revealed
normalization of LV function, trace TR, and only trace to
A 23-year-old female with history of congenital mild PR (Figure 4). The patient has maintained regular
complete heart block underwent dual chamber follow-up in cardiology clinic with reported complete
transvenous pacemaker implant at age 9 years. At age resolution of symptoms and normalization of exercise
20, during routine follow-up and device interrogation, capacity.
evidence of lead fracture was found. New transvenous
atrial and ventricular leads were implanted along with
pulse generator replacement; the original TVLs were
capped and abandoned. Over the next two years, the
patient developed progressive exercise intolerance
and was referred to our institution for evaluation.
Transthoracic echocardiogram (TTE) showed mild left
ventricular dilation with mildly reduced systolic function
ejection fraction (EF 45%), moderate right ventricular
enlargement, moderate tricuspid regurgitation (TR), and
moderate-severe PR with prominent lead slack prolapsing
into the RVOT and across the pulmonary valve (PV)
(Figure 1). Exercise stress echocardiography revealed
worsening PR and limited left ventricular (LV) functional
augmentation with overall decreased functional capacity
for her age and gender.
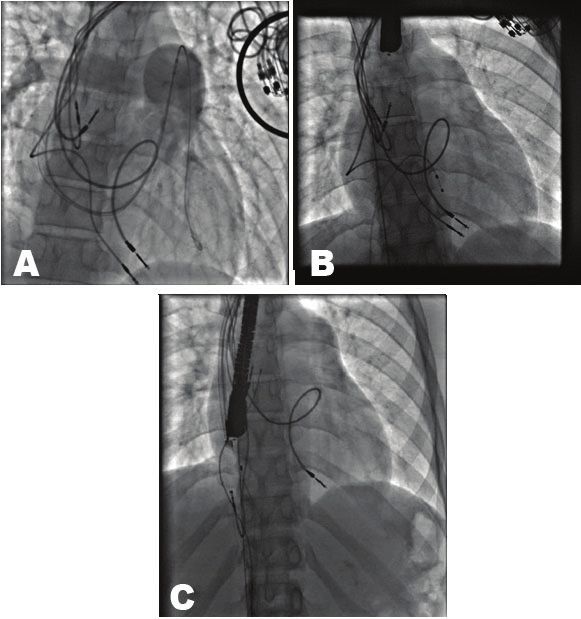
Diagnostic right heart catheterization with
Figure 1: Transthoracic echocardiogram. Short axis view at the
pulmonary angiography was recommended. Fluoroscopy base, revealing moderate pulmonary regurgitation.
demonstrated a total of four TVLs, two right atrial and two
right ventricular, with one ventricular lead prolapsing into
the RVOT (Figure 2A and B). Pulmonary artery (PA) and
left and right ventricular filling pressures were normal
at a baseline heart rate of 60 bpm and with increasing
the paced heart rate to 120 bpm. Pulmonary angiography
exhibited moderate PR (Figure 2A). Transesophageal
echocardiogram (TEE) further confirmed that one of the
RV leads was prolapsing into the RVOT with resultant
moderate PR.
The findings were extensively reviewed with the
patient and her family. Removal of the redundant lead
slack was considered the best way to address PR. Given
the patient’s chronic, high right ventricular pacing burden
and left ventricular dysfunction, biventricular pacing was
recommended for cardiac resynchronization therapy-
pacemaker (CRT-P). The family was in agreement to
proceed with TVLs extraction and CRT-P implant. For
the procedure, femoral venous and arterial access were
obtained. Temporary ventricular pacing, transesophageal
echocardiography, and invasive blood pressure
monitoring were used during extraction (Figure 2B). A
combined superior and inferior approach was integrated
for extraction of all four TVLs. Powered sheath-assisted
extraction from the left subclavian vein was performed
with the GlideLight laser (Spectranetics Corporation,
Figure 2: Fluoroscopy. (A) Pulmonary angiography with
Colorado Springs, CO) while the Byrd Workstation™
evidence of mild to moderate pulmonary regurgitation. (B)
Femoral Intravascular Retrieval Set (Cook Medical Inc, Prior to extraction, right femoral vein temporary transvenous
Bloomington, IN) via right femoral vein was used to pacemaker was placed in right ventricle: 2 atrial and 2 ventricular
remove the redundant loop from the RVOT (Figure 2C). leads can also be visualized. (C) GlideLight laser (Spectranetics
The two approaches were employed in concert to free the Corporation, Colorado Springs, CO) inserted via left subclavian
adhered leads and maintain as much coaxial dissection vein and Byrd Workstation™ Femoral Intravascular Retrieval
as possible. After successful extraction, a CRT-P device Set (Cook Medical Inc, Bloomington, IN) inserted via right
was implanted afterward (Figure 3). A transthoracic femoral vein.
International Journal of Case Reports and Images, Vol. 11, 2020. ISSN: 0976-3198
Int J Case Rep Images 2020;11:101121Z01GC2020. Cortes et al. 3
www.ijcasereportsandimages.com
CHD population is significantly increasing for the adult
electrophysiologist [7].
This case represents an uncommon complication of a
common practice in the pediatric population. Extra lead
slack in anticipation of somatic growth has been described
by multiple authors and largely avoids problems related
to mechanical lead stretch and resultant lead dysfunction
over time [2, 8–11]. However, this technique can have
potential complications related to failure of slack to
properly release and migration of excessive slack.
Furthermore, either lack of serial follow-up or timely
interventions to address these complications can lead
to irreversible sequelae related to cardiac and adjacent
organ dysfunction [7].
This case also highlights the unique challenges of
integrating extraction techniques into the long-term care
of CIEDs in these patients. Smaller patient and vascular
size, prior cardiothoracic surgery, considerably longer
TVLs, age since implant, and the psychological challenges
for both patients and their families, add significant
complexities to extraction procedures in young patients.
In our patient’s case, multiple atrial and ventricular leads
Figure 3: Fluoroscopy. Successful retrieval of 2 atrial and 2
ventricular leads, with placement of new CRT-P device.
were present, and the original abandoned leads were over
12 years old at the time of extraction. Increased duration
following implantation of TVLs is associated with an
increased requirement of powered/assisted extraction
techniques and increased risk of complications with
extraction [6, 10–14]. In addition, the redundant lead
slack in the RVOT required unique considerations for the
extraction approach given the difficulty in maintaining
coaxial sheath dissection [3, 5, 6]. A combined approach
including extraction from the femoral vein allowed for
better alignment with the lead body in the RVOT.
This patient’s symptoms were felt to be largely due to
baseline PR that was further accentuated with exercise
secondary to the prolapse TVLs slack across the PV. To our
knowledge, this is the first published case of this unique
complication due to excessive slack and unexpected
migration out to the RVOT. Removal of the prolapsed
Figure 4: Transthoracic echocardiogram on day 1 post- lead eliminated the mechanical disruption across the
procedure. Short axis at the base (same level than Figure 1).
PV, leading to prompt resolution in both symptoms and
Trace pulmonary regurgitation.
valvular dysfunction. It is important to acknowledge that
failure to recognize and treat this complication could
DISCUSSION result in irreversible cardiac dysfunction. This must also
be balanced with the risk associated with TVL extraction.
The number of CHD CIED implants has steadily grown
over the last few decades [1]. New techniques and more
sophisticated devices have played an important role in the CONCLUSION
expanded application of these devices in the care of these
patient population [4, 6]. Different from adults where This case emphasizes the importance of close follow-
infection has a major role; lead malfunction/fracture is the up in this population and the need for an expanded
most common indication for TVL extraction in congenital approach to long-term CIED management in order to
population. Atallah et al., in the PLEASE study, reported avoid complications. Serial radiographic imaging should
independent predictors of lead failure including younger be standard in pediatric patients while somatic growth
age of implantation 18 years is occurring. Greater consideration should be given
old, and Sprint FidelisÒ ICD leads [5]. to proactive lead management strategies in order to
Awareness of long-term complications and risk factors address potential or active complications with TVLs. An
related to CIEDs that are unique to the pediatric and integrated and experienced approach to lead extraction
International Journal of Case Reports and Images, Vol. 11, 2020. ISSN: 0976-3198
Int J Case Rep Images 2020;11:101121Z01GC2020. Cortes et al. 4
www.ijcasereportsandimages.com
in these patients affords the best results while minimizing 14. Alexander ME, Cecchin F, Walsh EP, Triedman JK,
complications. When extraction is considered, a combined Bevilacqua LM, Berul CI. Implications of implantable
superior and inferior approach can afford tremendous cardioverter defibrillator therapy in congenital heart
versatility to maximize success. disease and pediatrics. J Cardiovasc Electrophysiol
2004;15(1):72–6.
*********
REFERENCES
1. Berul CI, Villafane J, Atkins DL, et al. Pacemaker lead Author Contributions
prolapse through the pulmonary valve in children. Guillermo Andres Cortes – Conception of the work,
Pacing Clin Electrophysiol 2007;30(10):1183–9. Design of the work, Acquisition of data, Analysis of data,
2. Ceresnak SR, Perera JL, Motonaga KS, et al. Ventricular Interpretation of data, Drafting the work, Revising the
lead redundancy to prevent cardiovascular events
work critically for important intellectual content, Final
and sudden death from lead fracture in pacemaker-
dependent children. Heart Rhythm 2015;12(1):111–6. approval of the version to be published, Agree to be
3. O’Sullivan JJ, Jameson S, Gold RG, Wren C. accountable for all aspects of the work in ensuring that
Endocardial pacemakers in children: Lead length questions related to the accuracy or integrity of any part
and allowance for growth. Pacing Clin Electrophysiol of the work are appropriately investigated and resolved
1993;16(2):267–71.
Rahul N Doshi – Conception of the work, Design of the
4. Williams WG, Izukawa T, Olley PM, Trusler GA, Rowe
RD. Permanent cardiac pacing in infants and children.
work, Analysis of data, Interpretation of data, Revising
Pacing Clin Electrophysiol 1978;1(4):439–47. the work critically for important intellectual content,
5. Atallah J, Erickson CC, Cecchin F, et al. Multi- Final approval of the version to be published, Agree to be
institutional study of implantable defibrillator accountable for all aspects of the work in ensuring that
lead performance in children and young adults: questions related to the accuracy or integrity of any part
Results of the Pediatric Lead Extractability and of the work are appropriately investigated and resolved
Survival Evaluation (PLEASE) study. Circulation
2013;127(24):2393–402.
Philip M Chang – Conception of the work, Design of the
6. Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead work, Analysis of data, Interpretation of data, Revising
extraction: Heart Rhythm Society expert consensus the work critically for important intellectual content,
on facilities, training, indications, and patient Final approval of the version to be published, Agree to be
management: This document was endorsed by the accountable for all aspects of the work in ensuring that
American Heart Association (AHA). Heart Rhythm questions related to the accuracy or integrity of any part
2009;6(7):1085–104. of the work are appropriately investigated and resolved
7. Carlson SK, Chang P, Doshi RN. Prolapse of pacemaker
leads resulting in complete IVC obstruction in an
Guarantor of Submission
adult congenital patient. The Journal of Innovations
in Cardiac Rhythm Management 2015;6(9):2117–20. The corresponding author is the guarantor of submission.
8. Kratz JM, Toole JM. Pacemaker and internal
cardioverter defibrillator lead extraction: A safe Source of Support
and effective surgical approach. Ann Thorac Surg None.
2010;90(5):1411–7.
9. Arujuna A, Williams S, Whittaker J, et al. Trends, Consent Statement
indications and outcomes of cardiac implantable Written informed consent was obtained from the patient
device system extraction: A single UK center for publication of this article.
experience over the last decade. Int J Clin Pract
2012;66(2):218–25.
10. Love CJ, Wilkoff BL, Byrd CL, et al. Recommendations Conflict of Interest
for extraction of chronically implanted transvenous Authors declare no conflict of interest.
pacing and defibrillator leads: Indications, facilities,
training. North American Society of Pacing and Data Availability
Electrophysiology Lead Extraction Conference All relevant data are within the paper and its Supporting
Faculty. Pacing Clin Electrophysiol 2000;23(4 Pt Information files.
1):544–51.
11. Ghosh N, Yee R, Klein GJ, et al. Laser lead extraction:
Copyright
Is there a learning curve? Pacing Clin Electrophysiol
2005;28(3):180–4.
© 2020 Guillermo Andres Cortes et al. This article
12. Roux JF, Pagé P, Dubuc M, et al. Laser lead extraction: is distributed under the terms of Creative Commons
Predictors of success and complications. Pacing Clin Attribution License which permits unrestricted use,
Electrophysiol 2007;30(2):214–20. distribution and reproduction in any medium provided
13. Greenspon AJ, Patel JD, Lau E, et al. Trends in the original author(s) and original publisher are properly
permanent pacemaker implantation in the United States credited. Please see the copyright policy on the journal
from 1993 to 2009: Increasing complexity of patients website for more information.
and procedures. J Am Coll Cardiol 2012;60(16):1540–5.
International Journal of Case Reports and Images, Vol. 11, 2020. ISSN: 0976-3198
Int J Case Rep Images 2020;11:101121Z01GC2020. Cortes et al. 5
www.ijcasereportsandimages.com
Access full text article on Access PDF of article on
other devices other devices
International Journal of Case Reports and Images, Vol. 11, 2020. ISSN: 0976-3198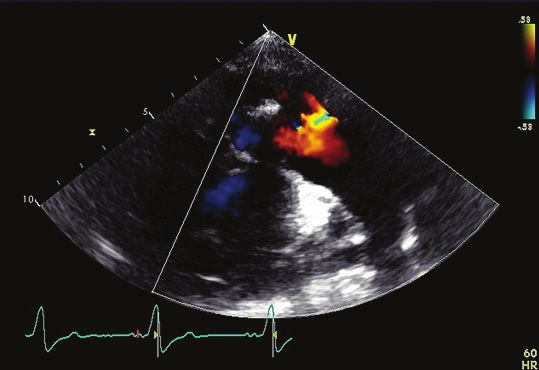
Submit your manuscripts at www.edoriumjournals.com



You can also read

















































