Helicobacter pylori Eradication Does Not Exacerbate Reflux Symptoms in Gastroesophageal Reflux Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
GASTROENTEROLOGY 2001;121:1120 –1126
Helicobacter pylori Eradication Does Not Exacerbate Reflux
Symptoms in Gastroesophageal Reflux Disease
PAUL MOAYYEDI, CHANDU BARDHAN, LYNNE YOUNG, MICHAEL F. DIXON, LORNA BROWN, and
ANTHONY T.R. AXON
The General Infirmary at Leeds, Leeds, West Yorkshire, England
Background & Aims: Observational studies have sug- have recommended that H. pylori should be treated in
gested that Helicobacter pylori may protect against gas- GERD patients in whom long-term antisecretory ther-
trointestinal reflux disease (GERD), but these results apy is planned.
could be due to bias or confounding factors. We ad- Case control studies, however, have suggested that H.
dressed this in a prospective, double blind, randomized, pylori eradication may result in an increased incidence of
controlled trial. Methods: H. pylori–positive patients with GERD in duodenal ulcer patients,5,6 although results are
at least a 1-year history of heartburn with a normal conflicting.7,8 The severity of GERD has also been re-
endoscopy or grade A esophagitis were recruited. Pa-
ported to be lower in H. pylori–infected patients.9 H.
tients were randomized to 20 mg omeprazole, 250 mg
pylori infection may enhance the ability of PPIs to reduce
clarithromycin, and 500 mg tinidazole twice a day for 1
week or 20 mg omeprazole twice a day and identical
intragastric acidity,10 and patients with H. pylori–posi-
placebos. A second concurrently recruited control group tive esophagitis heal faster with PPIs than uninfected
of H. pylori–negative patients were given open label 20 individuals.11 Furthermore, rebound acid hypersecretion
mg omeprazole twice a day for 1 week. All patients has been observed in H. pylori–negative subjects after
received 20 mg omeprazole twice a day for the following stopping PPI therapy.12 There are concerns, therefore,
3 weeks and 20 mg omeprazole once daily for a further that treatment of H. pylori in GERD patients may exac-
4 weeks. Omeprazole was discontinued at 8 weeks and erbate the disease, reduce the ability of PPIs to treat
patients were followed up for a further 10 months. A symptoms effectively, and promote rebound acid hyper-
relapse was defined as moderate or severe reflux symp- secretion once the drug is discontinued.
toms. H. pylori eradication was determined by 13C-urea The suggestion that H. pylori may protect against
breath test. Results: The H. pylori–positive cases were GERD has been derived from case control or cohort
randomized to antibiotics (n ⴝ 93) or placebo (n ⴝ 97). studies, and the results could be due to bias or confound-
Relapse of GERD occurred in 83% of each of the anti- ing factors. We have therefore evaluated the effect of H.
biotic, placebo, and H. pylori–negative groups during the pylori eradication on reflux symptoms in GERD patients
12-month study period. Life tables revealed no statisti- in a prospective, double blind, randomized, controlled
cal difference between the 2 H. pylori–positive groups
trial.
(log rank test, P ⴝ 0.84) or between the 3 groups (log
rank test, P ⴝ 0.94) in the time to first relapse. Two
patients in each group developed grade B esophagitis
Materials and Methods
at 12 months. Conclusions: H. pylori eradication ther- This was a double blind, single dummy, parallel group
apy does not seem to influence relapse rates in GERD randomized trial performed by 2 centers (Leeds and Rother-
patients. ham) in the United Kingdom between July 1995 and August
1998. Patients over the age of 17 years were considered for
recruitment if they had recurrent heartburn for at least 1 year
he relationship between Helicobacter pylori infection,
T acid suppression, and gastroesophageal reflux disease
(GERD) is complex.1 Patients with H. pylori infection are
as a dominant complaint and at least moderate symptoms for
a minimum of 2 days each week for the previous 2 weeks.
Subjects with grade A esophagitis or a normal endoscopy were
at risk of developing gastric mucosal atrophy, and a enrolled. Exclusion criteria included grades B–D esophagitis,
cohort study suggested that long-term proton pump
inhibitor (PPI) therapy for GERD may accelerate this Abbreviations used in this paper: GERD, gastroesophageal reflux
process.2 This work has been supported by randomized disease; PPI, proton pump inhibitor.
© 2001 by the American Gastroenterological Association
controlled trials,3,4 although not all have given statisti- 0016-5085/01/$35.00
cally significant results.4 Some investigators therefore doi:10.1053/gast.2001.29332November 2001 H. PYLORI THERAPY & SYMPTOMS IN GERD PATIENTS 1121
past or present peptic ulcer, previous esophageal or gastric and 500 mg tinidazole twice a day or to 20 mg omeprazole
surgery, pregnancy, and alcohol dependence. Patients taking twice a day and identical antibiotic placebos (Figure 1). All
warfarin or phenytoin, allergy to study drugs, treatment with patients were then given 20 mg open label omeprazole twice a
antibiotics, or bismuth salts within the previous month and day for 3 weeks and 20 mg omeprazole once a day for a further
PPIs, H2 receptor antagonists, sucralfate, or prokinetic agents 4 weeks. Randomization was performed using a computer-
within a day before randomization were also excluded. generated list, and the investigators assessing the patient were
not involved in administering the medication. A further group
Assessment of H. pylori Status of H. pylori–negative GERD patients were given 20 mg open
One antral and 1 corpus biopsy specimen was obtained label omeprazole twice a day for 4 weeks and 20 mg omepra-
for rapid urease test and 2 antral and 2 corpus biopsy speci- zole once a day for the subsequent 4 weeks. The relative
mens for histology. The histology biopsy sections were stained proportion of H. pylori–infected subjects in this trial does not
with H&E for classification of gastritis according to the Sydney reflect the prevalence in the population because recruitment of
system and with Alcian Blue/periodic acid–Schiff for intestinal H. pylori–negative subjects was discontinued after 61 unin-
metaplasia. A modified Giemsa stain was used to assess H. fected patients were enrolled. These individuals were aware of
pylori status. Participants were invited to attend for 13C-urea their H. pylori–negative status, so this additional arm of the
breath test up to 7 days after the endoscopy. Four grams of study was not masked. This uninfected cohort was analyzed
citric acid was dissolved in 200 mL of water, and the fasted separately and acted as a second but unrandomized control
patient was given 150 mL of the solution to delay gastric group. Omeprazole was discontinued in all groups after 8
emptying. A baseline breath sample was obtained in duplicate weeks. Patients were given Maalox antacid preparation
and then the patient was given the remaining 50 mL of citric (Rhône-Poulenc Rorer, Kings Hill, Kent, UK) to take as
acid solution, to which 100 mg of 13C-urea (Boston Isotopes, rescue medication. No other antacid, antisecretory, or proki-
Boston, MA) had been added. A further duplicate breath netic therapy was permitted.
sample was obtained at 30 minutes in exetainers, and the
samples were analyzed by mass spectrometry (ABCA-NT Outcome Assessment
Europa Scientific, Crewe, Cheshire, UK) at the Leeds General Participants were followed up every month for the first
Infirmary. The 13C-urea breath test was considered positive if 3 months and every 3 months thereafter until month 12
there was a greater than 5 per 1000 of 13CO2 difference over (Figure 1). The presence of heartburn, epigastric pain, acid
baseline. This protocol has a sensitivity of 96% and specificity regurgitation, and dysphagia was assessed by questionnaire.
of 98% in our population.13 Patients were defined as H. pylori These were classified as mild if the patient was aware of the
positive if the 13C-urea breath test and at least 1 biopsy-based symptom but it was easily tolerated, moderate if the discom-
test was positive, and defined as negative if all tests were fort was sufficient to interfere with normal activities, and
negative. severe if the patient was unable to perform normal activities.
All symptom assessments were obtained by a face-to-face
Study Design interview.
GERD patients infected with H. pylori were random- GERD symptoms were assessed by questionnaire at each
ized to 1 week of 20 mg omeprazole, 250 mg clarithromycin, visit using the same questionnaire that was administered at
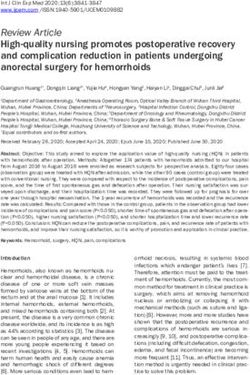
Figure 1. Summary of the trial
design.1122 MOAYYEDI ET AL. GASTROENTEROLOGY Vol. 121, No. 5
baseline. A 13C-urea breath test was performed at 3 and 12 remission curves of the groups were compared using the log
months (Figure 1). An endoscopy was also performed at 12 rank test. A secondary endpoint was relapse rates at 12–18
months to evaluate the presence of esophagitis. months. Patients that had relapsed in the first 12 months but
A relapse was defined as the recurrence of moderate or severe had remained asymptomatic on 20 mg omeprazole once daily
GERD symptoms for 2 or more days per week. This was the were asked to discontinue therapy, and the 12–18-month
primary endpoint of the trial. Patients that relapsed were given relapse rate of this group was analyzed separately. The propor-
20 mg omeprazole twice a day for 1 month followed by 20 mg tion of patients discontinuing because of relapse on 20 mg
omeprazole once daily until month 12. Patients were with- omeprazole once daily and the proportion of participants with
drawn from the trial if they continued to have at least mod- esophagitis at 12 months was compared using the 2 test. The
erate symptoms despite PPI therapy, and a 13C-urea breath test GERD symptom scores were compared between the random-
and endoscopy were performed at the exit visit. Participants ized groups at the beginning and end of the study using the
that failed to attend follow up were censored at the time of Mann–Whitney U test. All analyses were intention-to-treat,
their last visit. and a P value of ⬍ 0.05 was taken as statistically significant.
All patients in remission at 12 months were followed up for
a further 6 months. Patients prescribed 20 mg omeprazole
once daily for symptom relapse were instructed to discontinue
Results
therapy, and this group was analyzed separately as a prospec- Two hundred fifty-one patients were recruited to
tively planned subgroup analysis. Relapse rates were compared the study; 190 were H. pylori positive and 61 were H.
between the antibiotic, placebo, and H. pylori–negative arms of pylori negative. The H. pylori–positive cases were ran-
the trial during the 12–18-month phase of the trial. The domized to antibiotics (n ⫽ 93) or placebo antibiotics
rationale for this part of the trial is that rebound acid hyper- (n ⫽ 97). The baseline characteristics were similar be-
secretion may occur in H. pylori–negative subjects and this tween the 2 groups (Table 1). Four patients in the
could increase relapse rates in patients discontinuing PPI
placebo arm, 8 from the antibiotic arm, and 7 from the
therapy.
Local ethics committees approved the study and all partic-
H. pylori–negative arm were excluded from the inten-
ipants gave written informed consent. tion-to-treat analysis (Figure 2) because of disagreements
between tests as to H. pylori status, no study drug taken,
Statistical Analysis or no efficacy data after baseline. The H. pylori eradication
We assumed that 80% of the patients receiving anti- rate was 82% in the antibiotic arm according to the
13C-urea breath test at 3 and 12 months. An H. pylori
biotic placebos would have relapsed by the 12-month visit.14 A
total of 188 H. pylori–positive GERD patients (94 in each eradication rate of 13% was observed in the placebo arm,
group) would give the power to detect a 20% difference in but this may be artefactual because some patients were
relapse rates at the 80% power and 5% significance level taking omeprazole before the 13C-urea breath test.
assuming a 20% drop out rate. A smaller number of H.
pylori–negative patients were also recruited to the study. This Relapses From 0 to 12 Months
group was not randomized or masked and was not used in the
primary statistical analyses. The data from this group was for The relapse rates at 12 months were 83% in each
descriptive purposes, so the results from the H. pylori–infected of the placebo, antibiotic, and H. pylori–negative groups.
groups randomized to antibiotics or placebo could be put into Life tables revealed no statistical difference between the
perspective. 2 H. pylori–positive groups (log rank test, P ⫽ 0.84) or
The primary endpoint of the trial was time to first relapse. between the 3 groups (log rank test, P ⫽ 0.94) in the
The data were analyzed using life table methods and the time to first relapse (Figure 3). Eleven of 85 (13%) of the
Table 1. Baseline Characteristics of the Intention to Treat Antibiotic, Placebo, and H. pylori–Negative Groups
Variable Placebo group (n ⫽ 93) Antibiotic group (n ⫽ 85) H. pylori–negative group (n ⫽ 54)
No. of males (%) 45 (48%) 38 (45%) 29 (54%)
Grade A esophagitis (%) 19 (20%) 20 (24%) 18 (33%)
Overall GERD symptoms
Moderate (%) 80 (86%) 72 (85%) 41 (76%)
Severe (%) 13 (14%) 13 (15%) 13 (24%)
Current smoker (%) 32 (34%) 27 (32%) 14 (26%)
Current alcohol consumption 71 (76%) 56 (66%) 43 (80%)
Body mass index (mean SD) kg/m2 27.1 (3.9) 26.5 (4.6) 26.7 (4.0)
Age (mean SD) yr 50.8 (11.6) 47.4 (12.5) 45.0 (12.3)
Corpus atrophy present 20 (23%) 15 (18%) 0 (0%)
Intestinal metaplasia present 4 (5%) 1 (1%) 0 (0%)November 2001 H. PYLORI THERAPY & SYMPTOMS IN GERD PATIENTS 1123
Table 2. Comparison of GERD Symptoms and Endoscopic
Diagnosis at 12 Months Between the Antibiotic,
Placebo, and H. pylori–Negative Groups
Placebo Antibiotic H. pylori–negative
Variable group group group Pa
Heartburn
None 37 33 20 1.0
Mild 7 4 8
Moderate 2 1 1
Severe 1 3 1
Regurgitation
None 43 34 24 0.66
Mild 2 4 4
Moderate 1 1 1
Severe 0 2 1
Overall symptoms
None 32 26 19 0.88
Mild 12 11 9
Moderate 2 2 1
Severe 1 2 1
Esophagitis
None 41 34 24 1.0
Grade A 0 2 2
Grade B 2 2 2
aMann–Whitney U test in antibiotic vs. placebo groups only. H. pylori–
Figure 2. Flow diagram of the progress of participants. negative group shown for comparison.
antibiotic group, 11 of 93 (12%) of the placebo group, tients having no or mild symptoms. Results for the H.
and 10 of 54 (19%) of the H. pylori–negative group pylori–negative group were also similar (Table 2).
withdrew from the study within the first 2 months
Relapses From 12 to 18 Months
because of relapse of symptoms during this period.
Patients without GERD symptoms or esophagitis
Symptom and Endoscopy Assessment at 12 months including patients who had relapsed and
at 12 Months been restarted on omeprazole were eligible for further
There were no statistically significant differences follow up. Fifty-six participants remained in remission at
in heartburn, regurgitation, overall GERD symptoms, or 12 months (placebo group, n ⫽ 20; antibiotic group,
rates of esophagitis between the randomized H. pylori– n ⫽ 22; and H. pylori–negative group, n ⫽ 14). The
positive groups at 12 months (Table 2) with most pa- relapse rates in these patients were 12% in the placebo
Figure 3. Gastroesophageal
remission curves from 0 to 12
months for the antibiotic, pla-
cebo, and H. pylori–negative
groups.1124 MOAYYEDI ET AL. GASTROENTEROLOGY Vol. 121, No. 5
Figure 4. Remission curves
from 12 to 18 months for the
antibiotic, placebo, and H. py-
lori–negative groups in patients
with no previous relapse.
group, 23% in the antibiotic group, and 37% in the H. the antibiotic and placebo groups. This relapse rate is
pylori–negative group (Figure 4). consistent with the previous literature14 and was also
Fifty-nine patients had relapsed during the previous seen in the H. pylori–negative controls. These data sug-
12 months but had then remained asymptomatic on 20 gest that H. pylori infection does not have a clinically
mg omeprazole once daily (placebo group, n ⫽ 20; important impact on relapse rates in Los Angeles grade A
antibiotic group, n ⫽ 20; H. pylori–negative group, n ⫽ esophagitis or endoscopy-negative reflux disease. The
19). In these groups, omeprazole was discontinued and results may not be applicable to patients with more
the patients were followed up for a further 6 months. The severe esophagitis, although our study is representative
relapse rates were 82% in the placebo group, 55% in the of the majority of patients presenting in primary care
antibiotic group, and 70% in the H. pylori–negative with reflux symptoms.
group (Figure 5). The drop out rates were relatively high, and this may
reduce the power of the trial to show a difference between
Discussion the H. pylori eradication and placebo antibiotic groups.
This is the first randomized controlled trial to All analyses were intention-to-treat using life table
evaluate the effect of H. pylori eradication on reflux methods, so patients contributed to the results until the
symptoms and esophagitis in GERD patients. There was point that they were lost to follow up or withdrawn. The
an 83% relapse rate in GERD symptoms at 12 months in remarkably similar relapse rates in all 3 arms of the study
Figure 5. Remission curves
from 12 to 18 months for the
antibiotic, placebo, and H. py-
lori–negative groups in patients
with previous relapse.November 2001 H. PYLORI THERAPY & SYMPTOMS IN GERD PATIENTS 1125
suggest there is little difference between the groups for have been included in the study.24 A positive response to
this primary outcome. PPI therapy may be a more accurate method of identi-
Rebound acid hypersecretion has been reported in H. fying GERD patients.25,26 There was no difference in
pylori–negative patients after discontinuation of high- relapse rate when patients not responding to PPI therapy
dose omeprazole given for 8 weeks.12 This is not seen in were excluded at the 2-month visit.
all H. pylori–positive individuals, with some showing The putative protective effect of H. pylori on GERD is
persistent acid suppression.12 The clinical importance of said to be more marked in cagA-positive27 and vacA S1
this observation is uncertain. Our data do not support a strains.28 We did not assess this and it is possible that
clinically significant increase in relapse rates in infected more virulent strains of H. pylori have a protective effect
GERD patients allocated to antibiotic therapy after re- in GERD patients. We evaluated patients with GERD
ceiving 20 mg omeprazole twice daily for 4 weeks fol- and it remains possible that H. pylori eradication therapy
lowed by once daily for a further 4 weeks. It remains may change the risk of GERD in non-ulcer dyspepsia or
possible that rebound hypersecretion may be more pro- peptic ulcer patients. A systematic review, however,
nounced in H. pylori–negative patients given longer found no evidence that H. pylori eradication therapy
course of acid suppression. We found no statistically increase esophagitis in non-ulcer dyspepsia patients,29
significant difference in relapse rates in H. pylori–positive and we found no increase in reflux symptoms in a large,
patients allocated to antibiotic or placebo after the ome- double blind, randomized, controlled trial of H. pylori
prazole was discontinued at 12 months in those requiring eradication in the general population.30
long-term acid suppression. This, however, was a second- H. pylori infection can cause gastric mucosal atrophy
ary outcome measure and the numbers of patients eligi- leading to reduced gastric acid output, which in turn
ble for this part of the trial were relatively small. We may reduce reflux esophagitis.31 This is likely to be more
therefore cannot exclude the possibility that H. pylori of a problem in elderly patients, and this was confirmed
eradication therapy may cause a modest change in relapse by a case control study.32 Patients enrolled in this trial
had a mean age of 48 years, and it is possible that results
rates once long-term PPI therapy is discontinued.
would have been different in an older population with a
Intragastric pH is positively correlated with healing of
greater proportion of pan-gastritis and gastric atrophy.
reflux esophagitis,15 and PPI therapy is more effective at
H. pylori eradication leads to a recovery of acid secretion
reducing acid output in the presence of H. pylori.10
in a proportion of these individuals, and this could
Treatment of H. pylori may therefore be expected to
increase reflux in predisposed patients.
reduce the efficacy of PPI in GERD patients. Some
We have shown that H. pylori eradication therapy does
studies have suggested that healing rates are higher in H.
not increase relapse rates in endoscopy-negative reflux
pylori–positive esophagitis patients compared with unin- disease and Los Angeles grade A esophagitis patients.
fected controls after antisecretory therapy,11,16 whereas We have also demonstrated that treating H. pylori infec-
others have not found this relationship.17–19 These con- tion does not dramatically impair the efficacy of PPI
tradictory results may be caused by confounding factors therapy. Therefore, the decision as to whether H. pylori
because there are differences in age and socioeconomic eradication therapy should be offered to infected GERD
circumstances between H. pylori–positive and –negative patients rests on the individual beliefs of clinicians about
patients.20 These studies also cannot exclude the possi- the risks of developing corpus atrophy and intestinal
bility that an independent factor may cause a decrease in metaplasia during prolonged acid suppression.
the prevalence of H. pylori infection and an increase in
GERD. Bile reflux, for example, inhibits H. pylori21 and References
has been associated with GERD.22 A randomized con- 1. Dent J. Helicobacter pylori and reflux disease. Eur J Gastroenterol
trolled trial overcomes these problems, and we found the Hepatol 1999;11(suppl 2):S51–S57.
symptomatic response to omeprazole was similar in H. 2. Kuipers EJ, Lundell L, Klinkenberg-Knol EC, Havu N, Festen HP,
Liedman, Lamers CB, Jansen JB, Dalenback J, Snel P, Nelis GF,
pylori–positive patients randomized to antibiotic therapy Meuwissen SG. Atrophic gastritis and Helicobacter pylori infec-
compared with placebo. H. pylori eradication is therefore tion in patients with reflux esophagitis treated with omeprazole or
unlikely to reduce the efficacy of PPI therapy in GERD fundoplication. N Engl J Med 1996;334:1018 –1022.
3. Moayyedi P, Wason C, Peacock R, Walan A, Bardhan K, Axon AT,
patients. Dixon MF. Changing patterns of gastritis in long-standing acid
The majority of patients in this study had a normal suppression: effect of Helicobacter pylori eradication. Helicobac-
endoscopy and the diagnosis of GERD mainly relied on ter 2000;5:206 –214.
4. Lundell L, Dalenback J, Hattlebakk J, Janatuinen E, Levander K,
symptoms. These have been shown to be reasonably Miettinen P, Myrvold HE, Pedersen SA, Thor K, Junghard O,
accurate,23 although some patients without GERD may Andersson A. Outcome of open antireflux surgery as assessed in1126 MOAYYEDI ET AL. GASTROENTEROLOGY Vol. 121, No. 5
a Nordic multicentre prospective clinical trial. Nordic GORD Study Epidemiology of Helicobacter pylori in an asymptomatic popula-
Group. Eur J Surg 1998;164:751–757. tion in the United States. Effect of age, race, and socioeconomic
5. Labenz J, Blum AL, Bayerdorffer E, Meining A, Stolte M, Borsch G. status. Gastroenterology 1991;100:1495–1501.
Curing Helicobacter pylori infection in patients with duodenal 21. Graham DY, Yamaoka Y. H. pylori and cagA: relationships with
ulcer may provoke reflux esophagitis. Gastroenterology 1997; gastric cancer, duodenal ulcer, and reflux esophagitis and its
112:1442–1447. complications. Helicobacter 1998;3:145–151.
6. Fallone CA, Barkun AN, Friedman G, Mayrand S, Loo V, Beech R, 22. Wilmer A, Tack J, Frans E, Dits H, Vanderschueren S, Gevers A,
Best L, Joseph L. Is Helicobacter pylori eradication associated Bobbaers. Duodenogastroesophageal reflux and esophageal mu-
with gastroesophageal reflux disease? Am J Gastroenterol 2000; cosal injury in mechanically ventilated patients. Gastroenterology
95:914 –920. 1999;116:1293–1299.
7. Vakil N, Hahn B, McSorley D. Recurrent symptoms and gastro- 23. Klauser AG, Schindlbeck NE, Muller-Lissner SA. Symptoms in
oesophageal reflux disease in patients with duodenal ulcer gastro-oesophageal reflux disease. Lancet 1990;335:205–208.
treated for Helicobacter pylori infection. Aliment Pharmacol Ther 24. Moayyedi P, Axon AT. The usefulness of the likelihood ratio in the
2000;14:45–51. diagnosis of dyspepsia and gastroesophageal reflux disease.
8. McColl KE, Dickson A, El-Nujumi A, El-Omar E, Kelman A. Symp- Am J Gastroenterol 1999;94:3122–3125.
tomatic benefit 1-3 years after H. pylori eradication in ulcer pa- 25. Fass R, Ofman JJ, Sampliner RE, Camargo L, Wendel C, Fennerty
tients: impact of gastroesophageal reflux disease. Am J Gastro- MB. The omeprazole test is as sensitive as 24-h oesophageal pH
enterol 2000;95:101–105. monitoring in diagnosing gastro-oesophageal reflux disease in
9. Wu JC, Sung JJ, Chan FK, Ching JY, Ng AC, Go MY, Wong SK, Ng symptomatic patients with erosive oesophagitis. Aliment Phar-
EK, Chung SC. Helicobacter pylori infection is associated with macol Ther 2000;14:389 –396.
milder gastro-oesophageal reflux disease. Aliment Pharmacol 26. Ofman JJ, Gralnek IM, Udani J, Fennerty MB, Fass R. The cost-
Ther 2000;14:427– 432. effectiveness of the omeprazole test in patients with noncardiac
10. Labenz J, Tillenburg B, Peitz U, Idstrom JP, Verdu EF, Stolte M, chest pain. Am J Med 1999;107:219 –227.
Borsch G, Blum AL. Helicobacter pylori augments the pH-increas- 27. Vicari JJ, Peek RM, Falk GW, Goldblum JR, Easley KA, Schnell J,
ing effect of omeprazole in patients with duodenal ulcer. Gastro- Perez-Perez GI, Halter SA, Rice TW, Blaser MJ, Richter JE. The
enterology 1996;110:725–732. seroprevalence of cagA-positive Helicobacter pylori strains in the
11. Holtmann G, Cain C, Malfertheiner P. Gastric Helicobacter pylori spectrum of gastroesophageal reflux disease. Gastroenterology
infection accelerates healing of reflux esophagitis during treat- 1998;115:50 –57.
ment with the proton pump inhibitor pantoprazole. Gastroenter- 28. Fallone CA, Barkun AN, Gottke MU, Best LM, Loo VG, Veldhuyzen
ology 1999;117:11–16. VZ, Nguyen T, Lowe A, Fainsilber T, Kouri K, Beech R. Association
12. Gillen D, Wirz AA, Ardill JE, McColl KEL. Rebound hypersecretion of Helicobacter pylori genotype with gastroesophageal reflux dis-
after omeprazole and its relation to on-treatment acid suppres- ease and other upper gastrointestinal diseases. Am J Gastroen-
sion and Helicobacter pylori status. Gastroenterology 1999;116: terol 2000;95:659 – 669.
239 –247. 29. Moayyedi P, Soo S, Deeks J, Forman D, Mason J, Innes M,
13. Moayyedi P, Braunholtz D, Heminbrough E, Clough M, Tompkins Delaney B. Systematic review and economic evaluation of Heli-
DS, Mapstone NP, Mason S, Dowell AC, Richards ID, Chalmers cobacter pylori eradication treatment for non-ulcer dyspepsia.
DM, Axon AT. Do patients need to fast for a 13C-urea breath BMJ 2000;321:659 – 664.
test? Eur J Gastroenterol Hepatol 1997;9:275–277. 30. Moayyedi P, Feltbower R, Brown J, Mason S, Mason J, Nathan J,
14. Dent J, Yeomans ND, Mackinnon M, Reed W, Narielvala FM, Richards IDG, Dowell AC, Axon ATR. The effect of population H.
Hetzel DJ, Solcia E, Sharman DJ. Omeprazole v ranitidine for pylori screening and treatment on dyspepsia and quality of life in
prevention of relapse in reflux oesophagitis. A controlled double the community: results of a randomised controlled trial. Lancet
blind trial of their efficacy and safety. Gut 1994;35:590 –598. 2000;355:1665–1669.
15. Bell NVJ, Burget D, Howden CW, Wilkinson J, Hunt RH. Appropri- 31. Koike T, Ohara S, Sekine H, Iijima K, Kato K, Shimosegawa T,
ate acid suppression for the management of gastro-esophageal Toyota T. Helicobacter pylori infection inhibits reflux esophagitis
reflux disease. Digestion 1992;52(suppl 1):59 – 67. by inducing atrophic gastritis. Am J Gastroenterol
16. Hatlebakk JG, Hyggen A, Madsen PH, Walle PO, Schulz T, Mow- 1999;94:3468 –3472.
inckel P, Bernklev T, Berstad A. Heartburn treatment in primary 32. Haruma K, Hamada H, Mihara M, Kamada T, Yoshihara M, Sumii
care: randomised, double blind study for 8 weeks. BMJ 1999; K, Kajiyama, Kawanishi M. Negative association between Helico-
319:550 –553. bacter pylori infection and reflux esophagitis in older patients:
17. Klinkenberg-Knol EC, Nelis F, Dent J, Snel P, Mitchell B, Prichard case-control study in Japan. Helicobacter 2000;5:24 –29.
P, Lloyd D, Havu N, Frame MH, Roman J, Walan A, Group LT.
Long-term omeprazole treatment in resistant gastroesophageal
reflux disease: efficacy, safety, and influence on gastric mucosa.
Gastroenterology 2000;118:661– 669. Received April 2, 2001. Accepted July 26, 2001.
18. Peters FT, Kuipers EJ, Ganesh S, Sluiter WJ, Klinkenberg-Knol EC, Address requests for reprints to: Paul Moayyedi, Ph.D., FRCP, Gas-
Lamers CB, Kleibeuker JH. The influence of Helicobacter pylori on troenterology Unit, City Hospital NHS Trust, Dudley Road, Winson
oesophageal acid exposure in GERD during acid suppressive ther- Green, Birmingham, B18 7QH England. e-mail: p.moayyedi@bham.
apy. Aliment Pharmacol Ther 1999;13:921–926. ac.uk; fax: (44) 121-414-6571.
19. Tefera S, Hatlebakk JG, Berstad A. The effect of Helicobacter Supported by a research grant from AstraZeneca.
pylori eradication on gastro-oesophageal reflux. Aliment Pharma- Dr. Moayyedi is currently funded by a UK Medical Research Council
col Ther 1999;13:915–920. Training Fellowship in Health Services Research.
20. Graham DY, Malaty HM, Evans DG, Evans DJJ, Klein PD, Adam E. Dr. Brown is an employee of AstraZeneca.You can also read