"It's just puppy fat" Tackling obesity in children and adolescents
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

“It’s just puppy fat”
Tackling obesity in children and
adolescents
Webinar, SPH, Usyd, September 2013
Louise A Baur
University of Sydney: Discipline of Paediatrics & Child Health, Sydney
Medical School, and Sydney School of Public Health
The Children’s Hospital at Westmead: Weight Management Services
Email: louise.baur@health.nsw.gov.au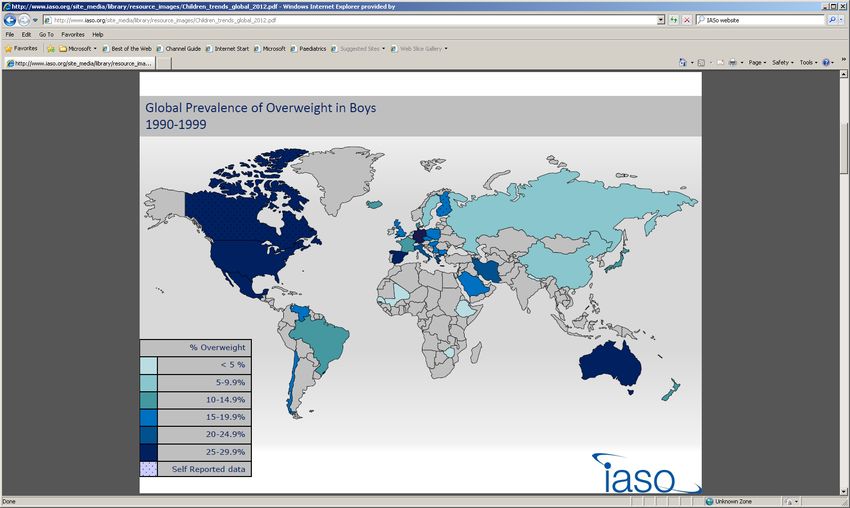
Descriptions of obesity • “… one of today’s most blatantly visible – yet most neglected – public health problems” http://www.who.int/dietphysicalactivity/childhood/en/ • “the public health equivalent of climate change” (Lang T, Rayner G. Obes Rev 2007; 8(Suppl 1):165-181) • “the Millennium Disease” http://www.iaso.org/iotf/ aboutiotf/
!
What I will cover in a whirlwind tour:
•How much of a problem is child/adolescent
obesity?
– Prevalence – globally, in Australia, in health systems,
waist vs BMI
•Treating those who are already affected by obesity
– Chronic disease care pyramid
•Early childhood obesity prevention
– The Healthy Beginnings Trial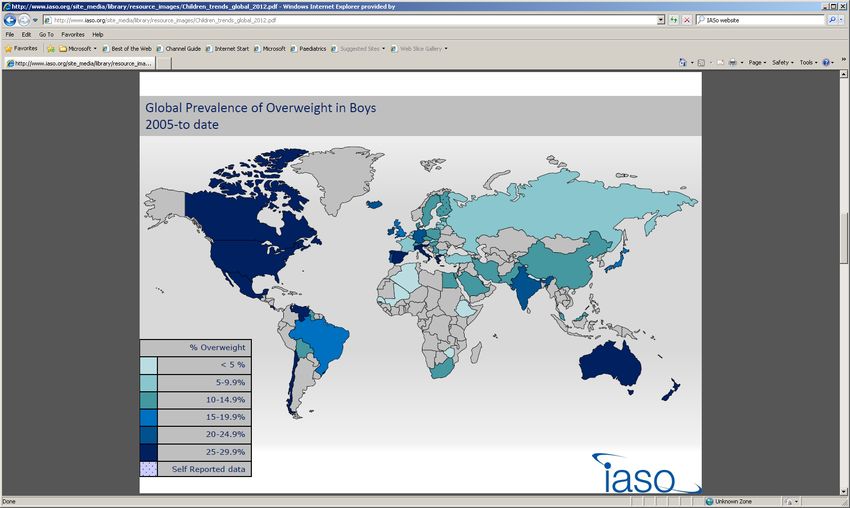
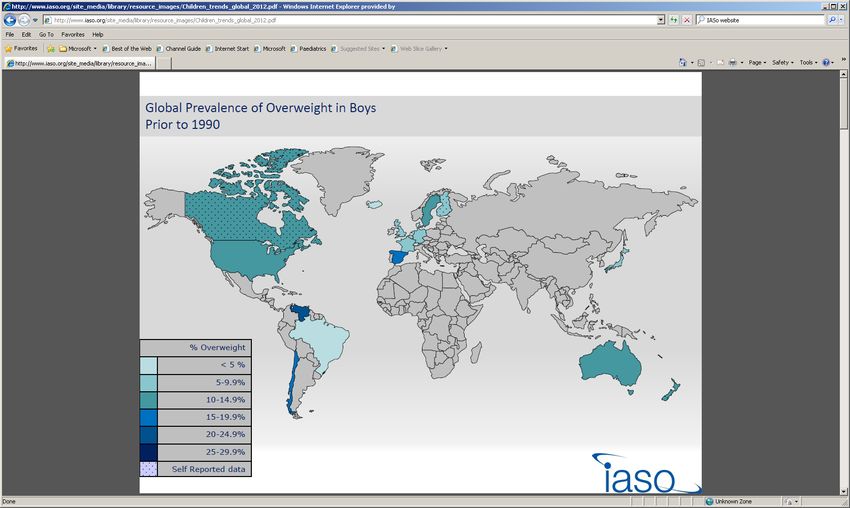
So, how much of a problem is
childhood obesity?
Global prevalence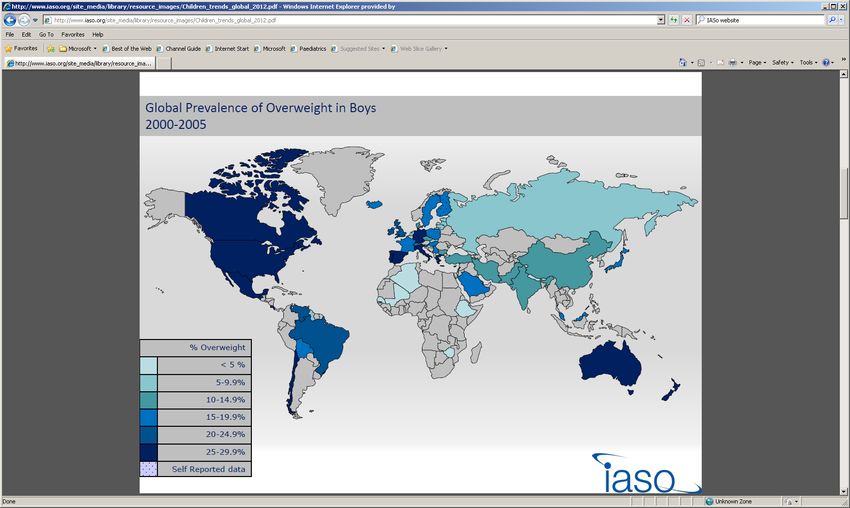
http://www.iaso.org/resources/obesity-data-portal/resources/maps/
http://www.iaso.org/resources/obesity-data-portal/resources/maps/
http://www.iaso.org/resources/obesity-data-portal/resources/maps/

http://www.iaso.org/resources/obesity-data-portal/resources/maps/
Like many other countries, obesity
prevalence in children and young
people in Australia is highFor a 100 year view of what has been
happening to the prevalence of obesity
in Australian children1900 – 2000: Prevalence of overweight and
obesity for 5 - 15 yr old Australian children
40
% overweight or obese
raw data
30 What happened in the 1980s?
all data
20
10
0
1900 1920 1940 1960 1980 2000
Year
Norton K et al, Int J Pediatr Obes 2006Over the past 25 years in school-aged
children →Prevalence of combined overweight and
obesity in 5-15 year olds in New South Wales –
based on body mass index (BMI)
Percentage overweight and obesity
30
Males
25 Females
20
15
10
5
0
1985 1995 2004 2010
Trends 1985-1995-2004-2010
Hardy LH et al 2012; http://www.health.nsw.gov.au/pubs/2011/pdf/spans_2010_summary.pdf; International
Obesity Taskforce (IOTF) cutpointsPrevalence of combined overweight and
obesity in 5-15 year olds in New South Wales –
based on body mass index (BMI)
Percentage overweight and obesity
30
Males
25 Females
Currently: 1 in 4 children &
20
adolescents overweight or obese
15
10 For obesity alone: 6-8% affected
5
Is it now plateauing?
0
1985 1995 2004 2010
Trends 1985-1995-2004-2010
Hardy LH et al 2012; http://www.health.nsw.gov.au/pubs/2011/pdf/spans_2010_summary.pdf; International
Obesity Taskforce (IOTF) cutpointsBut it seems that waistlines
(abdominal obesity) are changing more
rapidly than overall obesityChanging BMI and waist for Australian
children aged 7-15 years: 1985 to 2007
Garnett SP et al, Obes Rev 2011BMI z-score 7 to 15y 1985
25
Median
20
Percent
15
10
5 1985
0.07
-4 -2 0 2 4
BMI z-score Garnett SP et al, Obes Rev 2011
Z scores calculated using CDC 2000BMI z-score 7 to 15y 1985 1995
25
Median
20
Percent
15
10 0.31 1995
5 1985
0.07
-4 -2 0 2 4
BMI z-score Garnett SP et al, Obes Rev 2011
Z scores calculated using CDC 2000BMI z-score 7 to 15y 1985 1995 2007
25
Median
20
Percent
15 0.39 2007
10 0.31 1995
5 1985
0.07
-4 -2 0 2 4
BMI z-score Garnett SP et al, Obes Rev 2011
Z scores calculated using CDC 2000BMI z-score 7 to 15y 1985 1995 2007
30%
20%
25
Median 10%
20
13% 12% 22% 22% 25% 27%
Percent
15 0.39 2007
1985 1995 2007
% children with a BMI >85th centile
10 0.31 1995
Girls
Boys
5 1985
0.07
-4 -2 0 2 4
BMI z-score Garnett SP et al, Obes Rev 2011
Z scores calculated using CDC 2000Waist to height ratio 7 to 15y 1985
25
20
Percent
Median
15
10
5 1985
0.43
0.33 0.37 0.41 0.45 0.49 0.53 0.57 0.61 0.65 0.69
Garnett SP et al, Obes Rev 2011
WHtRWaist to height ratio 7 to 15y 1985 1995
25
20
Percent
Median
15
10
1995
0.44
5 1985
0.43
0.33 0.37 0.41 0.45 0.49 0.53 0.57 0.61 0.65 0.69
Garnett SP et al, Obes Rev 2011
WHtRWaist to height ratio 7 to 15y 1985 1995 2007
25
20
Percent
Median
15
2007 0.45
10
1995
0.44
5 1985
0.43
0.33 0.37 0.41 0.45 0.49 0.53 0.57 0.61 0.65 0.69
Garnett SP et al, Obes Rev 2011
WHtRWaist to height ratio 7 to 15y 1985 1995 2007
20%
25 10% 18% 18%
9% 14% 14%
20 9% 7%
6% 9%
Percent
Median
15 1985 1995 2007
2007 0.45 % children with WHtR ≥ 0.5
10
1995
0.44 Girls
Boys
5 1985
0.43
0.33 0.37 0.41 0.45 0.49 0.53 0.57 0.61 0.65 0.69
Garnett SP et al, Obes Rev 2011
WHtRWaist to height ratio 7 to 15y 1985 1995 2007
20%
Is there a disjunction
25
between waist 10% 18% 18%
20 circumference / 9%
9% 7%
6% 9%
14% 14%
waist:height ratio
Percent
Median
15
(abdominal obesity)
2007 0.45 and
1985 1995 2007
% children with WHtR ≥ 0.5
10 BMI (overall
1995
body
0.44 Girls
fatness)? Boys
5 1985
0.43
0.33 0.37 0.41 0.45 0.49 0.53 0.57 0.61 0.65 0.69
Garnett SP et al, Obes Rev 2011
WHtRAnd obese children and adolescents are presenting often to the health system
In Australia, of every 200 children presenting to their family doctor, 60 are overweight or obese (23 obese) – and 1 is offered weight management intervention BEACH data set, Annual national random survey of 1,000 family doctor surgeries (data on 100 consecutive patients, of all ages); 2002-2006, >40,000 children aged 2-17 years, Self-reported heights & weights; Cretikos M et al, Medical Care 2008; 46:1163-1169 ; background prevalence of O&O
In Australia, of every 200 children presenting to their family doctor, 60 are overweight or obese (23 obese) – and 1 is offered weight management intervention BEACH data set, Annual national random survey of 1,000 family doctor surgeries (data on 100 consecutive patients, of all ages); 2002-2006, >40,000 children aged 2-17 years, Self-reported heights & weights; Cretikos M et al, Medical Care 2008; 46:1163-1169 ; background prevalence of O&O
In Australia, of every 200 children presenting to their family doctor, 60 are overweight or obese (23 obese) – and 1 is offered weight management intervention BEACH data set, Annual national random survey of 1,000 family doctor surgeries (data on 100 consecutive patients, of all ages); 2002-2006, >40,000 children aged 2-17 years, Self-reported heights & weights; Cretikos M et al, Medical Care 2008; 46:1163-1169 ; background prevalence of O&O
In Australia, of every 200 children presenting to their
family doctor, 60 are overweight or obese (23 obese) –
and 1 is offered weight management intervention
So, overweight & obese children
and adolescents present
frequently to primary (secondary
& tertiary) care in Australia – but
they aren’t usually treated for
the problem
BEACH data set, Annual national random survey of 1,000 family doctor surgeries (data on 100
consecutive patients, of all ages); 2002-2006, >40,000 children aged 2-17 years, Self-reported heights
& weights; Cretikos M et al, Medical Care 2008; 46:1163-1169 ; background prevalence of O&OWhat can be done to treat those already affected by obesity?
Obesity and the
chronic disease care pyramid
Tertiary care facilities & special
obesity clinics; specialist teams; key
Complex patients
worker case manages & joins up care Level 3
Case management
Secondary level care facilities; Level 2
multidisciplinary teams;
High risk patients
group programs
Care management
Self-care supported
by primary care
doctors, other Level 1
primary care, 70-80% of overweight/obese patients
group programs Self-care & community based care
Primary prevention & health promotionObesity and the
chronic disease care pyramid
Tertiary care facilities & special
Services at all
obesity clinics; specialist teams; key
worker case manages & joins up care Level 3
Complex patients
Case management
levels are needed
Secondary level care facilities; Level 2
multidisciplinary teams;
High risk patients
group programs
Care management
Self-care supported
by primary care
doctors, other Level 1
primary care, 70-80% of overweight/obese patients
group programs Self-care & community based care
Primary prevention & health promotionIssues in health service delivery
• Many services are disjointed, with little
coordination between and across regions and
levels of care
• Paediatric obesity and its cardio-metabolic
complications are new morbidities for most
paediatric health care services
• Most health professionals are poorly trained in
managing paediatric obesity and its complications
• Issues of equity and access to services for affected
individuals eg only 3 of 6 states in Australia have a
multidisciplinary tertiary service*; many services have long waiting
lists (e.g. up to 12 months); similar situation in NZ, in parts of the
USA, and probably many other countries.
* Spilchak et al, J Paediatr Ch Health 2008Obesity and the chronic disease care
pyramid – some of the RCTs undertaken
RESIST
+ health
professional Metformin Trial Level 3
education
strategies
Level 2
High risk patients
Care management
Level 1
70-80% of o’wt/obese patients
Self-care & community based care
Primary prevention & health promotionTertiary care facilities & special
obesity clinics; specialist teams; key
Complex patients
worker case manages & joins up care Level 3
Case management
Secondary level care facilities; Level 2
multidisciplinary teams;
High risk patients
group programs
Care management
Self-care supported
by primary care
doctors, other Level 1
primary care, 70-80% of overweight/obese patients
group programs Self-care & community based care
Primary prevention & health promotionPreventing obesity in early childhood
The Healthy Beginnings Trial
• A staged, home-based early
intervention in the first two
years
• Delivered by early childhood
nurses
• Delivered in south-
• Aim: To compare the effect of a
western Sydney –
home-based early intervention
some of the most
for first-time mothers with
socially &
newborn babies, versus usual
economically
care, on:
– At age 6 & 12 months:
disadvantaged areas
Breastfeeding of Sydney
– At age 2 years: BMI, child • Funded by NHMRC x 2
and family eating patterns,
TV viewing, physical activityResults of the Healthy Beginnings Trial
BMI distributions of children at 2 years old by treatment
• At 12 months:
.25
PSo, what now?
• Follow-up at ages 3.5 and 5 years – with cost-
effectiveness analyses (LM Wen et al)
• Pilot study in Shanghai just finishing – use of SMS
and phone calls to support pregnant women and
new mothers (M Li et al)
• Early Prevention of Obesity in CHildhood (EPOCH)
prospective meta-analysis (L Askie et al)
– Combining individual patient data from 4 Australasian early
intervention trials.
– Approximate n=2000 at age 2 years; will allow sufficient
sample size to look at changes in obesity prevalence ratesSummary
• Child & adolescent obesity
– Globally prevalent, with the Asia-Pacific region affected
– Plateauing in Australia and some other countries?
– Central adiposity may be worsening
• Treating those who are affected
– Affected children & adolescent present frequently to
health care facilities – but are rarely treated for it
– Many barriers to provision of clinical care
• Early childhood obesity prevention
– Healthy Beginnings Trial provides evidence that early
intervention may be important in obesity prevention
– Many unanswered questions – cost-effectiveness?,
other modes of delivery?, how early is necessary? …A final comment!
Societal policies and processes influencing the population prevalence of obesity
INTERNATIONAL NATIONAL/ COMMUNITY WORK/SCHOOL/ INDIVIDUAL POPULATION
FACTORS REGIONAL LOCALITY HOME
Public Leisure
Transport
Transport Activity/
Facilities
Globalization
Energy
Urbanization Public Expenditure
of Safety Labour
markets
Health Infections
%
Health
Care OBESE
Development AND
Worksite
Social security Food & OVER-
Sanitation Activity Food WEIGHT
Media Media &
Most of the
intake :
Nutrient
programs
& advertising
Culture Manufactured/
Imported
Family &
Home
focus on
density
Education
Food
childhood
Agriculture/
School
Food &
obesity
Food &
Nutrition Gardens/
Local markets
Activity
interventions
National has been in
perspective this domain
Modified from Ritenbaugh C, Kumanyika S, Morabia A, Jeffery R, Antipatis V. IOTF website 1999: http://www.iotf.orgSocietal policies and processes influencing the population prevalence of obesity
The challenge will be in
INTERNATIONAL
FACTORS
NATIONAL/
REGIONAL
COMMUNITY
LOCALITY tackling
WORK/SCHOOL/
HOME
the upstream
INDIVIDUAL POPULATION
determinants of obesity
Public Leisure
Transport
Transport Activity/
Facilities
Globalization
Energy
Urbanization Public Expenditure
of Safety Labour
markets
Health Infections
%
Health
Care OBESE
Development AND
Worksite
Social security Food & OVER-
Sanitation Activity Food WEIGHT
intake :
Media Media & Nutrient
programs Culture Manufactured/ Family & density
& advertising Imported Home
Food
Education
School
Food & Agriculture/ Food &
Nutrition Gardens/ Activity
Local markets
National
perspective
Modified from Ritenbaugh C, Kumanyika S, Morabia A, Jeffery R, Antipatis V. IOTF website 1999: http://www.iotf.orgAcknowledgements
• Members of The Children’s • PIs, CIs and members of the
Hospital at Westmead Weight following research teams:
Management Services team, and Healthy Beginnings, HIKCUPS,
the CHW Obesity Research LEAP, Metformin trial, PEACH,
Group RESIST, Loozit
• Specific CHW, USyd & SSWAHS • Members of the Prevention
colleagues: Dr Shirley Research Collaboration at the
Alexander, A/Prof Lisa Askie. University of Sydney
Prof Adrian Bauman, Prof Ian
Caterson, Prof Chris Cowell, Dr • Members of the Australasian
Sarah Garnett, A/Prof Tim Gill, Child & Adolescent Obesity
Dr Louise Hardy, Ms Lesley Research Network
King, A/Prof Mu Li, Prof Chris
Rissel, Prof Kate Steinbeck, Dr
Li Ming Wen ….. • International Association for
the Study of obesityThank you
Acknowledgements
• Members of The Children’s • PIs, CIs and members of the
Hospital at Westmead Weight following research teams:
Management Services team, and Healthy Beginnings, HIKCUPS,
the CHW Obesity Research LEAP, Metformin trial, PEACH,
Group RESIST, Loozit
• Specific CHW, USyd & SSWAHS • Members of the Prevention
colleagues: Dr Shirley Research Collaboration at the
Alexander, A/Prof Lisa Askie. University of Sydney
Prof Adrian Bauman, Prof Ian
Caterson, Prof Chris Cowell, Dr • Members of the Australasian
Sarah Garnett, A/Prof Tim Gill, Child & Adolescent Obesity
Dr Louise Hardy, Ms Lesley Research Network
King, A/Prof Mu Li, Prof Chris
Rissel, Prof Kate Steinbeck, Dr
Li Ming Wen ….. • International Association for
the Study of obesityYou can also read

















































