Telehealth and Autism Prior to and in the Age of COVID 19: A Systematic and Critical Review of the Last Decade
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Child and Family Psychology Review (2021) 24:599–630
https://doi.org/10.1007/s10567-021-00358-0
Telehealth and Autism Prior to and in the Age of COVID‑19:
A Systematic and Critical Review of the Last Decade
Kimberly S. Ellison1 · Jerrica Guidry1 · Paige Picou1 · Paige Adenuga1 · Thompson E. Davis III1
Accepted: 30 May 2021 / Published online: 10 June 2021
© The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature 2021
Abstract
There has been growing interest in the use of telehealth; however, the COVID-19 pandemic and the subsequent isolation and
restrictions placed on in-person services have fast-tracked implementation needs for these services. Individuals with autism
spectrum disorder (ASD) have been particularly affected due to the often-intensive service needs required by this popula-
tion. As a result, the aim of this review was to examine the evidence base, methodology, and outcomes of studies that have
used telehealth for assessment and/or intervention with children and adolescents with ASD as well as their families over the
last decade. Further, the goal is to highlight the advances in telehealth and its use with this special population. A systematic
search of the literature was undertaken, with 55 studies meeting inclusion criteria and quality analysis. Specified details
were extracted from each article, including participant characteristics, technology, measures, methodology/study design,
and clinical and implementation outcomes. Services provided via telehealth included diagnostic assessments, preference
assessments, early intervention, applied behavior analysis (ABA), functional assessment and functional communication
training, and parent training. Findings, although still emerging, encouragingly suggested that services via telehealth were
equivalent or better to services face-to-face. Results support the benefits to using telehealth with individuals with ASD.
Future research should continue to explore the feasibility of both assessments and interventions via telehealth with those
having ASD to make access to assessment services and interventions more feasible for families, while acknowledging the
digital divide it could create.
Keywords Autism Spectrum Disorder · ASD · Autism · Telehealth · Assessment · Intervention
Introduction via telehealth has been found to be cost-effective and can be
delivered across vast geographic regions which would oth-
“Telehealth” is an all-encompassing term for the use of erwise prevent access to care (Baweja et al., 2021; Shulver
various modes of technology to provide medical and men- et al., 2016). Additionally, the further integration of technol-
tal health care services in place or in addition to in-person ogy in clinical practice has become more widely accepted
methods (American Psychological Association, 2013). Ser- due to increased convenience, decreased stigma, improved
vices can be implemented via synchronous or asynchronous patient outcomes, and reduced expenses (Luxton et al.,
modalities, such as telephone calls, video-teleconferencing, 2016). As telehealth evolves, improves, and gains further
email electronic applications, or video and audio record- acceptance, clinicians have also begun to explore the imple-
ings (American Psychiatric Association, 2013). The use mentation of telehealth psychological and behavioral ser-
of telehealth as a tool for implementing intervention and vices to individuals with autism spectrum disorder (ASD).
assessment services has grown recently particularly with the
impacts of COVID-19 on in-person access to services. As Telehealth Applications for Autism Spectrum
technology has improved, the implementation of services Disorder
* Thompson E. Davis III Autism spectrum disorder (ASD) is a neurodevelopmental
ted@lsu.edu disorder characterized by deficits in social communication
and interactions and restricted, repetitive behaviors, inter-
1
Department of Psychology, Louisiana State University, 236 ests, or activities (American Psychiatric Association, 2013).
Audubon Hall, Baton Rouge, LA 70803, USA
13
Vol.:(0123456789)600 Clinical Child and Family Psychology Review (2021) 24:599–630
As ASD is a lifelong disorder with significant and cascading interventions, functional behavior assessment and commu-
developmental implications, early identification and inter- nication training, web-based education and consultation,
vention have been found to be critical (Hyman et al., 2020). and language interventions. Their study sought to extend
However, gaining access to intervention programs through- the findings in the previous review by Boisvert et al. (2010)
out the community is often a challenge for families who where eight studies were included in their telehealth review
live in rural or remote areas, have limited or no transporta- and concluded that telehealth is a promising mode to treat-
tion, are of lower socioeconomic status or experience other ment for individuals with ASD. Overall, the findings of the
logistical difficulties (Sutherland et al., 2019). For example, Sutherland et al. (2019) review supported the implementa-
children who are at or below the poverty line or live in rural tion of telehealth services, highlighting an improvement in
areas are diagnosed with ASD much later than those children fidelity, reduction of behavior problems, an increase in par-
who are of high socioeconomic status or live in more urban ent satisfaction, and an increase in program acceptability.
areas (Antezana et al., 2017), which further delays their The studies were a mixture of repeated measures designs,
access to needed services. This disparity was likely even pre- and post-intervention studies, randomized controlled
further impacted by the effects of the COVID-19 pandemic, trials, mixed-methods, multiple-baseline designs, case stud-
where individuals who are below the poverty line are more ies, and observational data (Sutherland et al., 2019).
at risk for experiencing health disparities and are advised to With advances in technology, the literature using tel-
remain at home (Dahiya et al., 2020). Furthermore, many ehealth has grown significantly. Since the last systematic
children with ASD had disruption to their services due to review in 2018, a search using PsycINFO with the terms
the COVID-19 pandemic, which was not only exacerbated “telehealth OR telepractice” yielded 1,429 articles. Based
by the state-wide mandatory shutdowns across the country on this sharp increase, and due to the imminent and ongoing
but was also impacted by the decrease in staffing at these impact of the COVID-19 pandemic since the last review, and
service providers (Eshraghi, 2020). Telehealth services, if the increasingly expansive improvements in telehealth plat-
effective and appropriate, may be able to address some of forms and technology, there is a need for a current update
these concerns, as well as have the potential benefit of not and review of the literature on the use of mental health ser-
disrupting a child with ASD’s routine and daily schedule to vices with the ASD population to understand the utility and
the same degree with additional travel, time-lost, etc. It may efficacy of this service modality for the “new normal” (e.g.,
also benefit the families as telehealth services have been ongoing social distancing, the wearing of masks, recurring
found to be more cost-effective than in-person services and ever-changing restrictions on in-person gatherings and
(Camden & Silva, 2021). While the effects of telehealth for activities, etc.). The aim of this review was to provide an
children with ASD should not be assumed to be equivalent overview of the literature regarding telehealth for children
to those seen with in-person services or those seen in neu- and adolescents with ASD over the last decade, with regards
rotypical individuals using the medium for other concerns, to the type, recipients, and outcomes of the services and
it remains to be seen if a consistent body of literature has provide a recent evidence base upon which professionals
begun to accrue to suggest telehealth may or may not be a and researchers alike might base ongoing and future services
viable option in this population. Despite the increased need and research.
for access to mental health services, the literature regarding
the use of telehealth for assessment and intervention services
with children with behavioral needs, such as ASD, is limited. Method
The most recent systematic review of research focusing
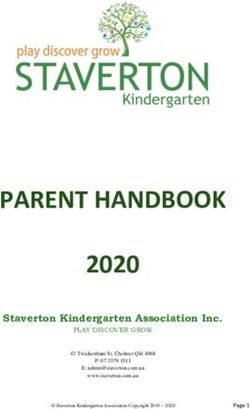
on ASD and the use of telehealth was conducted by Suther- The Preferred Reporting Items for Systematic Reviews and
land et al. (2019). Sutherland et al. (2019), sought to review Meta-Analyses (PRISMA) was used to guide the systematic
articles to inform the speech-language pathology field, and review process (see Fig. 1) based on its use in the previ-
found only 14 studies that met their inclusion criteria: the ous review (Sutherland et al., 2019). A systematic search
inclusion of at least one person with ASD, implementation of the literature was conducted using the Medline, Psy-
of a telehealth system for the purpose of an intervention or cINFO, ERIC, and CINAHL databases. These databases
assessment, the use of a design that allows for experimen- were selected based on the previous review by Boisvert et al.
tal control or comparison conditions, measurement of fac- (2010) and Sutherland et al. (2019). Titles and abstracts were
tors associated with telehealth implementation (e.g., child searched using key words to describe telehealth and ASD
outcomes, feasibility, parent outcomes), and published in a (“telehealth” OR “telemedicine” OR “telepractice” OR “tel-
peer-reviewed journal. There were 284 participants involved ecare” AND “Autis*” allowing searches for Autism, Autistic,
in the 14 studies with an age range of 19 months to adult- Autisms, etc.). Similar to the previous reviews, the search
hood. The services included in those studies consisted of was limited to English and only articles from peer-reviewed
diagnostic assessment services, early interventions, anxiety journals were included. No eligible articles were found prior
13Clinical Child and Family Psychology Review (2021) 24:599–630 601
title and abstract, 143 articles remained. These articles were
Records identified through independently read in full by the first and second authors to
database searcing (n = 472) determine eligibility. The two reviewers then discussed the
articles to resolve any disagreements about inclusion of a
study. Following the review, 60 papers remained that met
Records after duplicates
removed all inclusion criteria.
(n = 315) A quality review of the articles that met the inclusion
criteria was conducted using the Scientific Merit Rating
Scales (SMRS; National Autism Center, 2015). The review
Records screened
separately by two authors included the process of rating the studies on five separate
(n = 315) criteria for experimental rigor, including research design,
measurement of dependent and independent variables, par-
ticipant ascertainment, and generalization. The scientific
Full-text articles assesed Studies exlcuded based on merit score was obtained by combining the ratings of each
for eligibility by two incluson criteria (n = 83)
separate authors (n = 143) criterion. Studies that met a score of 3, 4, or 5 indicated
that scientific rigor had been utilized and firm conclusions
can be drawn, while a score of 2 indicated initial evidence
Studies excluded based on the of intervention effects but more scientific rigor should be
Studies included in the qualitative synthesis (n = 5)
qualitative synthesis (n = 60) utilized to confirm these effects. Lastly, a score of 1 or 0
indicated that insufficient scientific rigor was applied to the
studies. The studies were split between the second, third, and
fourth authors to be rated based on the five criteria, while
Studies included in the the first author independently rated all included studies. The
review (n=55) ratings were then compared to the first author’s ratings to
ensure reliability. Articles were discussed if the absolute
Fig. 1 PRISMA summary of paper screening process
value of any of the individual variables and/or overall SMRS
score was equal to one or greater; any discrepancies were
discussed and resolved. After the ratings were completed,
to 2010 that were not included in the previous reviews (Bois- five studies were excluded from the review due to receiv-
vert et al., 2010; Sutherland et al., 2019). Based on the previ- ing a SMRS score of 1.9 or lower, which indicated a lack
ous findings, this review included articles between Decem- of scientific rigor. A total of 55 papers were included in the
ber 2010 and March 2021 as a review of the last decade. review as a result of these processes.
A total of 472 articles that included both the telehealth
and autism search terms were found across the four data-
bases. After duplicates were removed, a total of 315 Results
remained. Titles and abstracts were screened separately by
the first and second authors based on the predetermined All 55 papers reviewed were published between January
inclusion criteria: (a) inclusion of one individual with autism 2010 and March 2021, across a range of disciplines. The
or parent of a person with autism; (b) implementation of a first section of this review examines articles that emphasized
telehealth system for the purpose of assessment or interven- the use of telehealth for either the assessment of ASD or
tion; (c) the use of a design that allows for experimental other common assessments used to inform treatment of indi-
control (e.g., intervention studies) or comparison condi- viduals with ASD (i.e., functional assessment, speech and
tion (e.g., diagnostic studies); (d) measurement of factors language assessment, preference assessments). Details of the
associated with implementation (e.g., outcomes, feasibility, papers included in the assessment section of this review are
acceptability); and (e) published in a peer-review journal. summarized in Table 1. The next section outlines the differ-
Synchronous (e.g., real time consultation) and asynchronous ent interventions utilized via telehealth for individuals with
(e.g., images, videos, applications) modalities were consid- ASD. Details of the papers included in the intervention sec-
ered as telehealth services. Web-based materials used to tion of this review are summarized in Table 2. Within both
train parent, teacher, or clinicians without any consultation the assessment and intervention sections, studies included
were not included. General review articles and articles using in this review are organized by the telehealth participant in
software such as virtual reality or wearable sensors were the following order: the individual with ASD him or herself,
excluded per previous reviews (Boisvert et al., 2010; Suther- parents of individuals with ASD, and other intervention-
land et al., 2019). After screening the 315 papers based on ists/staff/teachers of individuals with ASD. The intervention
13Table 1 Results of the systematic review for Assessment via Telehealth
602
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Sutherland et al. 13 children diagnosed Children VC with laptop and Face to Face adminis- Method comparison Language assessment No difference between
(2019) with ASD (10 webcam; applica- trations of language design scores (core subtests conditions, all parents
males, 3 females, tion was developed assessments, fol- of the CELF-4), were comfortable
9–12 years of age) by Coviu (formerly lowed by telehealth behavior observa- with assessment
National Informa- speech-language tion scores adapted
tion Communica- assessment from the CELF-P2,
tions Technology parent satisfaction
Australia—NICTA) questionnaire
Reese et al. (2013) 21 parent–child dyads Parents and their VC equipment includ- Comprehensive Random assignment ADOS module 1, No differences in diag-
(3–5 years of age; children ing high-definition Autism assessment to either in-person ADI-R, satisfaction nostic consistency
11 children with monitors and cam- either through VC or interactive VC survey between groups or
ASD and 10 with era that clinicians or in-person: clini- assessment inter-rater agree-
developmental could control the cian administered ment on the ADOS
delay) angles of from ADI-R; the clinician items or ADI-R
another room coaches the parents between groups,
to complete the parents reported high
ADOS presses with satisfaction with VC
their child group
Wacker et al. (2013) 20 parent–child dyads Parents VC at teleconsulta- Parents were trained Multi-element design Children’s behaviors, Behavior analysts were
(age ranged from tion centers using over VC for 2, IOA, the procedural effective in conduct-
29 to 80 months, all Windows-based PCs 1-h sessions on integrity, cost of ing FAs effectively
with ASD) and webcams (no the principals of treatment and efficiently via
specific VC program behavior analysis, telehealth, the remote
reported) 1 h session outlining FA successfully
procedure (e.g., identified social func-
preference assess- tions, implementation
ment, FA), then via telehealth is cost-
coached through effective treatment
conducting the FA strategy
in four assessment
conditions
Corona et al. (2021) 51 total children, Parents and child VC using wall Adaptation of the Randomized assign- TELE-STAT, TELE- Remote assessors
35 children were mounted speakers TELE-STAT ment to either the ASD-PEDS, Parent accurately diagnosed
diagnosed with and video platform (remote assessor TELE-STAT or questionnaire 33 of the 35 children
ASD (1–3 years of (Cisco Systems) provided prompts to TELE-ASD-PEDS with ASD; Overall,
age), 10 develop- parents) and utiliza- groups, examined diagnostic agreement
mental delays, and 6 tion of TELE-ASD- diagnostic accuracy was 86%. Parents
typically developing PEDS (parent-led and parent percep- (77%) reported they
social tasks) to tion and satisfaction would prefer to play
assess symptoms and observe during
of ASD to inform the remote assess-
diagnosis ment. Most feedback
(25%) involved
technology issues
Clinical Child and Family Psychology Review (2021) 24:599–630Table 1 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Machalicek et al. Three teacher–child Teachers VC using iChat from Phase 1: Realtime Teacher implementa- Steps performed Phase 1: teachers
(2009) dyads (male, a remote site using coaching of teach- tion comparisons, correctly by teacher, implement paired-
34 months, two a MacBook Isight ers administering participant compari- IOA, teacher fidel- choice preference
males 5–7 years of camera, Isight video paired-choice pref- sons ity, procedural assessment with
age with ASD) conference, and erence assessments, integrity 100% accuracy, satis-
headsets including where fied with VC Phase
to begin trials and 2: children preferred
immediate correc- items selected in
tive feedback Phase Phase1, indicating
2: did not have VC that VC maybe a
component successful strategy in
providing feedback
for preference assess-
ments
Machalicek et al. Six Teacher–Child Teachers VC using iChat from Baseline: teachers Multiple-baseline FA, maintenance High levels of treat-
Clinical Child and Family Psychology Review (2021) 24:599–630
(2010) dyads (with ASD; a remote site using conducted FAs with design across observations, IOA, ment fidelity to FA
age from 4 to a MacBook Isight instruction via VC participants with treatment integrity procedures taught
10 years of age) camera, Isight video but without feed- embedded multi- questionnaire, social teacher’s-maintained
conference, and back Intervention: element designs validity ability to successfully
headsets teachers receive implement FA proce-
immediate feedback dures up to 9 weeks
through VC Mainte- post-initial training;
nance: FA without socially acceptable
VC feedback
Higgins et al. (2017) Three staff, three chil- Direct-care staff VC using Adobe Con- Training: multi- Nonconcurrent Correct implementa- Efficacy and social-
dren with ASD (two nect and webcams media presenta- multiple-baseline tion of component validity showed
males, 4–5 years (sessions were tion, descriptive design MSWO skill, IOA, telehealth-training
of age, one female, recorded) feedback, and social validity ques- was feasible and
5 years of age), immediate feedback tionnaire effective for all
confederates during scripted
role-plays, each ses-
sion consisted of 14
MSWO trails with
a confederate, with
instruction via VC
13
603604 Clinical Child and Family Psychology Review (2021) 24:599–630
section also includes two studies that feature the telehealth
New Zealand, FA Functional Assessment, IOA Interobserver Agreement, MSWO Multiple Stimulus Without Replacement, TELE-STATScreening Tool for Autism in Toddlers and Young Chil-
ASD Autism Spectrum Disorder, ADOS Autism Diagnostic Schedule, ADI-R Autism Diagnostic Interview-Revised, BASC-2 Behavior Assessment System for Children-Second edition, CELF-4
Clinical Evaluation of Language Fundamentals-Fourth Edition, Australia and New Zealand, CELF-P2 Clinical Evaluation of Language Fundamentals-Preschool, Second Edition, Australia and
telehealth was accept-
able, the training pro-
satisfaction with tech
cedure was effective,
time feedback, High
procedural integrity
participant as being a parent and a teacher together. Lastly,
Percentage of MSWO Increased procedural
integrity after real-
ASD at follow-up,
Reported outcomes
and staff reported
limitations and future directions for the use of telehealth
with child with
with individuals with ASD are discussed.
setup
Assessment
A total of eight studies implemented assessment procedures
social validity ques-
treatment integrity,
skills implemented
via telehealth for individuals with ASD. All of these stud-
correctly, IOA,
ies used video conferencing (VC) to deliver the assessment
procedures and utilized a variety of different VC systems
tionnaire
Measures
(e.g., Cisco Systems, Isight via MacBooks, Adobe Connect,
VidyoDesktop) (Ausenhus & Higgins, 2019; Corona et al.,
2021; Higgins et al., 2017; Machalicek et al., 2009, 2010;
Reese et al., 2013; Wacker et al., 2013). One study, used
multiple-baseline
an application, Coviu, that was created for VC (Sutherland
Design/method
Nonconcurrent
et al., 2019).
design
Telehealth Participant: Children with ASD
Only one study utilized VC to administer four subtests of
assessments through
MSWO preference
a speech and language assessment (Clinical Evaluation of
remote, real-time
given training on
VC using VidyoDesk- Confederates were
conducting brief
Language Fundamentals, 4th Edition) remotely by a speech-
language pathologist to children with ASD; this telehealth
feedback
procedure was compared to in-person administrations of the
Service
same four subtests. The assessment scores were reportedly
high in agreement between in-person and telehealth imple-
mentation, but no differences between the procedures were
Surface Pro tablet
top, Dell Laptop,
found (Sutherland et al., 2019). Parents’ satisfaction with
the telehealth assessment was high; they also indicated that
Telehealth participant Technology
their children felt either “somewhat or definitely” comfort-
able with the procedures as well (Sutherland et al., 2019).
Telehealth Participant: Parent of Child with ASD
Two studies utilized the parents of individuals with ASD to
implement diagnostic autism assessments. One study (Reese
et al., 2013), randomly assigned participants to either the
Trainees
in-person administration group or VC administration group.
Both groups were administered the Autism Diagnostic
Interview-Revised (Rutter et al., 2003). Video conferenc-
Participant character-
one female, 4 years
of age with ASD),
ing was utilized to coach parents in implementing modi-
23 years of age),
Ausenhus and Higgins Four trainees (19–
fied Autism Diagnostic Observation Schedule (Lord et al.,
confederates
2002)-Module 1 activities and presses with their children
compared to an in-person autism assessment utilizing these
dren, VC Video Conferencing
istics
same presses. No difference between diagnostic consistency
was found between groups; inter-rater agreement was not
significantly different on the ADI-R and only one significant
Table 1 (continued)
difference for an item on the ADOS was found. Further,
high parent satisfaction was reported for both conditions.
Another study utilized telehealth assessment procedures to
(2019)
assess autism in young children (Corona et al., 2021). After
Article
randomized group assignment, remote assessors provided
13Table 2 Results of the systematic review for Interventions via Telehealth
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Hepburn et al. (2016) 33 families with chil- Children and their Therapist used VC 10 session Telehealth Repeated measure SCARED, PSOC, Results supported the
dren with ASD (17 parents using OoVoo Facing Your Fears ANOVAs for pre- participant monitor- feasibility and effi-
in the intervention, throughout the intervention in a and post-interven- ing form, parent and cacy of a CBT inter-
mean of 11.5 years intervention ses- small-group format tion youth satisfaction vention for anxiety in
of age and 16 in sions using web- consisting of 4–6 ratings, treatment youth with ASD over
the waitlist control, cams and headsets parent youth dyads, fidelity checklist telehealth; significant
mean of 12 years individualized to fit difference in scores
of age) the needs of each on SCARED pre to
group post-intervention;
therapist fidelity was
strong, and all parents
rated high levels of
satisfaction
Ferguson et al. (2020) Six children with Children VC using Zoom 5 days per week, Nonconcurrent Primary and second- All participants learned
ASD (males probe and teaching multiple-baseline ary responses, primary and second-
Clinical Child and Family Psychology Review (2021) 24:599–630
3–7 years of age) sessions of discrete design primary observa- ary responses, and
trial teaching (pro- tional responses and five participants
vided instructive or secondary obser- acquired primary and
corrective feedback) vational responses, secondary observa-
IOA tion responses, high
levels of attending
and engagement dur-
ing teaching
McCrae et al. (2020) 17 children with Children and their VC using Zoom Eight (50 min) ses- Single arm study Clinical interview, Improvement on chal-
ASD and insomnia parents sions of CBT-CI electronic sleep lenging behaviors
(6–12 years of age) diary (SOL, TWT, and SOL, TWT, and
TSTS), ABC, HRV, TSTS; Treatment
treatment satisfac- integrity was high;
tion questionnaire, treatment was rated
treatment credibility 100% moderately to
questionnaire very helpful, 87.5%
indicated CBT-CI
was autism-friendly
13
605Table 2 (continued)
606
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Cihon et al. (2021) Three children with Children VC using Zoom One session per day Nonconcurrent Probe sessions to doc- All participants reached
ASD (males, (10 min), 2–5 days multiple-baseline ument if participant master criterion (all
4–5 years of age) a week (depend- design engaged in a step; 7 steps) during inter-
ing on child); IOA; social validity vention condition; 2
Interventionists questionnaire out of 3 participants
administered Cool continued to reach
Versus Not Cool mastery during
procedure (chang- generalization condi-
ing the conversation tion; all 3 continued
when someone was to engage in all steps
bored—7 steps) correctly during
maintenance (7-day
follow-up); interven-
tion was found to be
acceptable
Baharav and Reiser Two parent–child Parents VC using Skype on Speech and language Single-subject Vineland-2, S, Children made gain
(2010) dyads (children laptops intervention (6-week time series: A–B MacArthur-CDI, in some aspects
4.6–5.2 years of period): Control repeated measures video analyses of of communication
age) Period: 2 weekly, design therapy sessions, (Vineland-2 and Mac-
50-min sessions parent satisfaction Arthur CDI scores)
in-person, Experi- questionnaire, and in both intervention
mental Period: one fidelity measures models, and parents
in-person (50 min) reported telehealth
followed by remote intervention was as
coaching via VC as valuable as in-person
needed (50 min)
Vismara et al. (2012) Nine parent–child Parents VC using webcam 12-week,1-h/week Single-subject, Child social com- High levels of treat-
dyads (all children on laptops (no VC ESDM parenting multiple-baseline munication (e.g., ment fidelity that
diagnosed with program specifically intervention with design with random language, imitation), were maintained,
ASD and were reported) coaching and DVD assignment ESDM Fidelity parents reported
36 months or learning module, Scale, MBRS and high satisfaction and
younger) Follow up: three-1-h CBRS, feasibility ease of use, some
sessions 2 weeks an acceptability child communication
apart questionnaire behaviors increased
(e.g., language, use
of language and
gestures)
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Vismara et al. (2013) Eight parent–child Parents VC on self-guided 12 weekly, 1.5-h Single-subject, Measure of parent sat- Parent fidelity and total
dyads (children with website using a lap- parent coaching ses- multiple-baseline isfaction, P-ESDM engagement increased
ASD and younger top and webcam sions to teach parent design with random Fidelity tool, from baseline through
than 48 months of training strategies, assignment MBRS, MacArthur- intervention, and
age) access to P-ESDM CDI, behavioral maintained during
learning mod- coding and parent follow-up, reported
ules, and 3, 1.5-h reporting of child increased understand-
monthly follow-up behaviors ing and appreciation
sessions for helping their child
learn skills at home
Wacker et al. (2013) 17 parent–child Parents VC at teleconsulta- 60-min sessions, Nonconcurrent multi- Child problem Reduction in problem
dyads (16 males, 1 tion centers using received lived ple-baseline design behaviors based on behaviors, Parents
female with ASD; Windows PCs and coaching from across children FA (at baseline and can be coached to
ranged from 29 to webcams Behavior Analysts intervention), IOA, administer FCT, par-
80 months in age) on FCT (baseline acceptability and ents rated treatment
Clinical Child and Family Psychology Review (2021) 24:599–630
included FA ses- cost of service as acceptable, lower
sions) cost for telehealth
than in-person
Suess et al. (2014) Three children with Parents VC using Skype and Parents conducted Multi-element design, The children’s and Parents’ fidelity at
ASD (males, Debut software all FA and FCT with alterna- parent’s behaviors implementing inter-
2–3 years of age) sessions while being tions between were recorded and vention increased,
coached by a behav- (A-coached) and coded, IOA, parent parents rated high
ior consultant (B-independent) fidelity, TARF-R levels of satisfaction,
trials and the children’s
problem behaviors
were reduced
Ingersoll and Berger 28 parents of children Parents VC using Skype Parents completed Children were CEWFS, CES-D, There were high rates
(2015) with ASD (age a self-directed or matched on their ImPACT knowledge of parent engagement,
ranged from 27 to therapist-assisted expressive language quiz, intervention therapist-assisted
73 months) version of ImPACT using the Mullen fidelity, program group had greater
(6 months). The Scales of Early engagement, engagement than the
therapist-assisted Learning; then program evaluation, self-directed group,
group attended 24 randomly assigned TEI, BIRS and the therapist-
total (2–30 min) to the self-directed assisted group was
remote coaching or therapist-assisted more likely to finish
sessions per week group program
13
607Table 2 (continued)
608
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Wainer and Ingersoll Five parent–child Parents Online VC using RIT Parent training either Single-subject, BIRS, program 4 of 5 parents achieved
(2015) dyads (age website self-directed or multiple-baseline engagement, parent overall fidelity of
ranged from 29 to taught through design knowledge of RIT implementation, 4 of
59 months) coaching sessions quiz, RIT fidelity 5 children maintained
form, child imita- higher than baseline
tions, IOA spontaneous imita-
tion, remote coaching
was rated high
Ingersoll et al. (2016) 28 parents of children Parents VC using Skype Parents either Children were Parent intervention Both groups increased
with ASD (age completed a matched on their fidelity, PSOC, FIQ, parent fidelity to
ranged from 27 to self-directed or expressive language language targets treatment, parent’s
73 months) therapist-assisted using the Mullen during the parent– rates of self-efficacy,
version of ImPACT Scales of Early child interaction and reduced parent
(6 months). The Learning; then pre-, post-, and stress, the therapist-
therapist-assisted randomly assigned follow-up interven- assisted group made
group attended 24 to the self-directed tion. MacArthur- greater gains in parent
total (2–30 min) or therapist-assisted CDI, Vineland-2 fidelity, marginally
remote coaching group greater gains in lan-
sessions per week guage targets during
the parent–child inter-
action and was the
only group to improve
in social skills on the
Vineland-2
Lindgren et al. (2016) 107 children with Parents Only Group 2 and All three groups con- FA: Mult-ielement FA sessions were There were no sig-
ASD or other DD 3 received remote ducted FAs and FCT single case design coded, reduction of nificant differences on
(age 21–84 months) coaching from a with their children. Random group problem behaviors, reduction of behavior
and their parents telehealth center, Group 1: treated assignment, Single- treatment costs for between groups, and
Group 2 used exist- in-home by trained subject designs, each group, parent-rated accept-
ing VC software, consultants, Group comparisons ability was high for
and Group 3 used 2: parents were between treatment all three groups, par-
VC on Skype coached on FAs delivery models ents can successfully
and FCT via VC (group differences) be taught to reduce
at a training clinic their child’s behavior
Group 3: coached problems through FA
via VC at home and FCT
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Machalicek et al. Three parent–child Parents VC through IChat on Study 1: 60-min FBA Study 1: Brief multi- Data on the occur- Intervention strategies
(2016) dyads (two females, laptop with webcam interview, and 4 tel- element treatment rence of challenging derived from FA
8–16 years of age, ehealth sessions for comparison. Study behaviors, IOA, decreased challenging
one male, 9 years of FA, provided feed- 2: Individual multi- procedural fidelity, behaviors, each parent
age; all with ASD) back and coaching. element design, A-B social validity ques- chose to continue the
Study 2: coached non-experimental tionaries strategies they liked
to implement brief design implementing the best
multi-element treat-
ment comparison,
had video clips
modeling strategies
Meadan et al. (2016) Three mother–child Parents VC through Skype on Phase 1: 45-min train- Multiple-baseline Parent quality and rate General increase of
dyads (children with an iPad (recorded ing session, iPics single case design with which parents rate and quality of
ASD, 2–4 years of sessions) coaches taught par- implemented the strategy use, main-
age) ents on 3 naturalistic three strategies, tained above baseline,
Clinical Child and Family Psychology Review (2021) 24:599–630
teaching strategies children’s social Parents reported high
(i.e., modeling, communication satisfaction with
mand-model, time initiations and goals, procedures,
delay) and envi- responses, IOA, and outcomes
ronmental arrange- social validity
ment. Phase 2:
Ongoing coaching
combined environ-
mental arrangement
and 3 naturalistic
strategies. Phase 3:
Maintenance
Pickard et al. (2016) 28 parents of children Parents VC using Skype Self-directed: Children were Sociodemographic Both groups found
with ASD (age ImPACT online 12 matched on their questionnaire, ImPACT to be favora-
ranged from 27 to sessions, Therapist- expressive language ImPACT ratings, ble and easy to learn,
73 months) assisted: ImPACT using the Mullen qualitative inter- positive perceptions
online 12 sessions Scales of Early views (Analyzed by about acceptability of
in addition to two Learning; then REAM) program, Therapist-
30-min remote randomly assigned assisted group was
coaching sessions to the self-directed 50% more likely to
per week or therapist-assisted spontaneously report
group child made social
communication gains
13
609Table 2 (continued)
610
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Suess et al. (2016) Five parent–child Parents VC using Skype Before FA, 1-h group FA: Multi-element IOA, task comple- Reduction in children’s
dyads (three males remote meet- design. FCT: Non- tion, mands (either problematic behavior
and two females ing FA sessions: concurrent multiple- prompted or not by average of 65.1%,
with ASD, ranged Parent conducted baseline design prompted), fre- suggest evidence sup-
from 2–7 years in during 1-h session across children quency of problem porting that parents
age) at autism center behavior and other can be coached to
FCT sessions: with variables implement FA and
coaching during 3, FCT via telehealth
15-min remote visits
over 3 consecutive
weeks
Simacek et al. (2017) Three children (two Parents VC using Debut soft- FA sessions: 5 min FAI, followed by Idiosyncratic AAC responses were
females with ASD ware with Logitech with no more SDA using a multi- responses for each strengthened when
and one female with HD Pro Webcam than 10 sessions element design. FA child included reinforcement
Rett syndrome; chil- C920 (sessions (50 min), live was then conducted, frequency, AAC was delivered for
dren between 3 and recorded) coaching and feed- followed by FCT responses, IOA, AAC response and
4 years of age) back; FCT: coached used an adapted TARF-R denied for idiosyn-
with verbal feedback multiple-probe cratic responses in
and instruction to design, in addition intervention phases,
use most to least to ABAB design parents rated overall
prompting for treatment as highly
AAC requests, up acceptable
to 7 sessions were
conducted per day,
with either 3 trial
blocks or lasting
5 min each
Subramaniam et al. Four parent–child Parents VC using Cisco In vivo initial visit Nonconcurrent Global parent treat- Parents were accurately
(2017) dyads (children WebEx program and training with multiple-baseline ment integrity, able to implement
with ASD, ranged confederates, parent design component parent DTI skills with VC,
from 18 months to training/teaching treatment integ- generalized skills and
12 years of age) DTI skills. VC ses- rity, child mastery, maintained accurate
sions, feedback was trainer procedural implementation over
immediate (twice a fidelity, problem 26 weeks post-train-
week), with fading behavior, TARF ing, VC deemed as
of VC sessions effective
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Bearss et al. (2018) 14 children with ASD Parents VC 6-month open trial of Open Trial Subject categoriza- High treatment
(ranged from 3 to RUBI-PT program tions, fidelity, significant
7 years of age) via telehealth (11 Feasibility measures improvements on
core sessions, 2 (i.e., TFC, PTAS, ABC, 78.6% of
supplemental, 3 parent satisfac- children were “much
telephone boosters) tion questionnaire, improved” on CGI-I,
telehealth caregiver parent-reported
satisfaction survey, greater confidence in
telehealth provider handling behaviors,
satisfaction survey, telehealth services
Efficacy measures deemed acceptable by
(ABC, HSQ-ASD, parents
PTP, CGI-I, Vine-
land-2)
Benson et al. (2018) Two children (one Parents VC using Google Coaches delivered FA: Multi-element SDA, IOA, reduction High levels of parent
Clinical Child and Family Psychology Review (2021) 24:599–630
male with ASD, Hangouts commu- remote instruction design. FCT: ABAB in children’s self- satisfaction with
5 years of age and nication platform, and support to par- single case experi- injurious behavior, procedures and use
one male with cer- Dell computer and ents for FA and FCT mental design implementation of technology, high
ebral palsy, 8 years Logitech camera sessions fidelity implementation fidel-
of age) ity across, reduction
in child’s problematic
behaviors
Kuravackel et al. 33 children with ASD Parent VC Parents were assigned Iterative pretest–post- M-CHAT, SCQ, Reduction in child
(2018) (age 3–12 years of either the waitlist test control group ADOS-2, PSI, problem behaviors,
age) control group, face- design ECBI, BPS, Vine- an increase in parent
to-face C-HOPE land-2, CSQ, GSRS, competency, and a
intervention or Parent fidelity decrease in parent
C-HOPE delivered questionnaire stress, no differ-
by telehealth over an ences in parent stress
18-month period or competency by
treatment modality,
parents were highly
satisfied with both
face-to face and tel-
ehealth modalities
Schieltz et al. (2018) Two children Parents VC using Skype on Mothers provided FA: Multi-element Behavioral defi- High treatment fidelity
(2–6 years of age Windows-based PC FA and FCT while design, FCT: non- nitions, IOA, reported by parents,
with ASD) being coached from concurrent multiple- (assessed using children’s problem
behavior consultants baseline design exact interval-by- behaviors decreased
through telehealth across participants interval com-
sessions parisons), treatment
fidelity
13
611Table 2 (continued)
612
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Vismara et al. (2018) Eight parent–child Parents VC using Citrix pro- Intervention: 12 Randomized group P-ESDM fidelity tool, Parents reported
dyads (children gram GoToMeeting weekly, 1.5-h parent assignment program website increased satisfaction
were 18–48 months coaching sessions usage, program in P-ESDM group
old and with ASD) of P-ESDM topics, satisfaction ratings, than community
access to learning social communica- group, children in
modules, Compari- tion behaviors P-ESDM group pro-
son: monthly 1.5-h duced more imitation,
coaching sessions, increase in fidel-
access to website ity at follow up for
without P-ESDM P-ESDM group
content
Guðmundsdóttir et al. Three parent–child Parents VC using Skype Training on naturalis- Multiple-baseline Parents’ behaviors, Teaching parents
(2019) dyads (3–4 years of through Microsoft tic behavioral inter- design children’s behaviors via brief in-person
age with ASD) LifeCam Cinema ventions (Sunny (social attending, situation training, and
Starts Program, requesting, number on-going telehealth
DANCE) given to of words, unintelli- training increased
parents (almost 2 h gent verbalizations), their skills and had a
per session, 7–14 IOA positive effect on the
sessions depending) child’s skills, parents
reported that social
attending increased in
children
Davis et al. (2020) Two parent–child Parents VC through What- Token economy sys- Nonconcurrent Token economy pro- Increase in implemen-
dyads (one male, sapp and video data tem implementation, multiple-baseline cedural fidelity (e.g., tation accuracy for
6 years of age, and collected through 3-week baseline, design frequency of token both participants
one female, 15 years SendSafely training interven- adherence, redirec- after baseline, both
of age, with ASD) tion phases (fixed tion, appropriate averaged over 84%
interval 30 s), and prompting through accuracy through fad-
faded intervention transitions to activ- ing phase; decreased
phase (fixed interval ity and break using perception of disrup-
60 s) tokens) based on tion and confidence in
observational data, using token economy
IOA, social validity system; parents
survey reported convenience
and ease of telehealth
platform
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Fisher et al. (2020) 36 parent–child Parents VC through VPN Intervention Group: RCT, pre-post test BISWA and BISPA, Percentage of oppor-
dyads (30 with Logitech web- Coached scripted comparisons social validity ques- tunities for BISWA
females, 6 males, cam and Bluetooth role-plays with tionnaire, IOA and BISPA increased
26–46 months, with headset one parent of dyad pre-to post treatment
ASD) and confederates in intervention group;
to implement EIBI intervention was rated
skills, Parent com- as socially acceptable
pleted 9 E-learning
modules Waitlist
Control: second par-
ent of dyad
Lindgren, (2020) 51 children (between Parents VC using Skype Competed FA with RCT FA: Multiple- The percent of reduc- All children showed
21 and 84 months coaching before element design tion of problem improved behavior in
with ASD) randomization, FCT FCT: nonconcurrent behavior in children, FCT group compared
Intervention Group: multiple-baseline TARF-R to two in Delayed
Clinical Child and Family Psychology Review (2021) 24:599–630
Parents conducted across participants, group, improved in
FCT with real-time plus reversal design social communication
coaching (60-min and task completion
weekly session for in FCT group, and the
at least 12 weeks). parent implemented
Delayed FCT FCT using telehealth
Group: 12 weeks of reduced children’s
treatment as usual problem behavior
Marino et al. (2020) 74 parents of 36 Parents Web platform within Phase 1: Both groups RCT—group com- HSQ-ASD, PSI/SF Decrease on PSI/SF of
children with Google-suite 12, 2-h informative parisons tele-assisted group
ASD, (average age: sessions Phase 2: but not control group,
69.6 months) 12 weeks of 2-h increased ability of
group behavioral tele-assisted group to
therapy, 1-h per face stress
week one–one ABA
for child Phase 3:
12 weeks Telehealth
Group: 2-h per
week tele-assisted
one-on-one parent
training and coach-
ing Control Group:
same intervention
protocol without
tele-assistance
13
613Table 2 (continued)
614
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Rooks-Ellis et al. Ten parent–child Parents VC using Zoom 12-week interven- Concurrent multiple- P-ESDM Parent Parent fidelity
(2020) dyads (six males, tionists trained and baseline design Fidelity Rating increased during
four females with coached parents to across participants System; P-ESDM generalization and
ASD, mean age implement P-ESDM Coaching Fidel- maintenance phases;
29.3 months) ity Rating System; Positive change in
Autism Impact autism symptoms;
Measure; social parents were satisfied,
validity question- and majority found it
naire effective
Suess et al. (2020) Four parent–child Parents VC using Skype Behavioral consultant Four Phases: (a) FA, Individualized Target Problem behavior
dyads (males coached caregivers (b) Extinction base- Mands and Target reduced an average of
with ASD; ages to complete FA, line in treatment Tasks were recorded 97.8% following
3–6 years) Extinction baseline, context, (c) FCT and coded, IOA initial alternative
FCT (3 contexts) in three alternative contexts FCT; miti-
and FCT in treat- contexts, (d) FCT in gated resurgence of
ment context (1 h treatment context problem behaviors;
weekly) generalized appro-
priate behaviors
across participants/
significant reductions
in resurgence were
found
Gerow et al., (2021a, Seven parent–child Parents VC using VSee Therapist coached Brief FA: 4 or 5 rand- Response per minute Reduction in challeng-
b) dyads (six males, parent during prefer- omized conditions; of target challenge ing behavior during
one female, with ence assessment; treatment evalua- behavior; TARF-R FCT; Assessment
ASD, 3–11 years Provided written tion was based on strategy was found
of age) and verbal instruc- reversal design to be feasible and
tions, prompting, acceptable
and feedback
(during all phases:
Brief FA and FCT
sessions)
Gerow et al., (2021a, Four parent–child Parents VC using VSee Goal develop- Concurrent multiple- Percentage of com- Accurate implementa-
b) dyads (males with ment (daily living baseline design pleted steps of task tion led to increase
ASD, 5–9 years of skills) therapist analysis in daily living skills
age) provided instruc- across participants
tions, prompting,
and feedback for all
phases (preference
assessment, teaching
trials, intervention)
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Hao et al. (2021) 30 parent–child Parents VC using Zoom In-person and Tel- Group differences Initiations, responses, No significant dif-
dyads (matched on ehealth group; Two and NDW per ferences between
gender ratio Female: group sessions and 6 minute, MLU; Reli- intervention groups;
Male, 3:12, range weekly 1 h individ- ability for dependent significant gains
of 23–86 months of ual sessions—feed- variables based on NDW
age with ASD) back was provided and MLU; parents’
on implementation increase fidelity of
accuracy of SKILLS implementation of
intervention
O’Brien et al. (2021) One parent and child Parents Vidyo teleconferenc- 10 min of 60 min Single-subject design Data collected on FA indicated behaviors
(3 years of age) with ing software session was used for target problem maintained by escape
ASD “check in,” 40 min behaviors, inde- and access functions,
used for FA or pendent requests FCT lead to reduction
FCT sessions were for preferred items, in problem behavior,
conducted, 10 min Reliability data, by 7th session, 100%
Clinical Child and Family Psychology Review (2021) 24:599–630
feedback was pro- IOA, TARF-R independent request-
vided to parent ing; 100% independ-
ent requesting at
6-month follow-up;
highly acceptable
Pierson et al. (2021) Four children, Parents WebEx, Google Drive Anticipatory set (pre- Multiple-probe- Parent implementa- No changes in child
three with ASD view elements of across-participants tion of modified DR responses were
(5–7 years of age), storybooks); Train- design intervention; Child found for major-
one with Down ing consisted of answers to compre- ity of participants;
Syndrome (6 years didactic teaching of hension questions; Parent-reported some
of age) storybook DR inter- IOA; social validity difficulty with child
vention (following questionnaire behavior and inter-
PEER); Coaching vention procedures
was synchronous
1 time per week,
feedback provided
Sivaraman et al. Six total dyads four Parents Video-calling Live coaching Nonconcurrent Duration of seconds All children tolerated
(2021) parent–child dyads platform on laptop caregivers to teach multiple-baseline wearing mask; wearing a mask for
(three males, one (no specific VC pro- face mask wear- design Scored completed 10 min (target dura-
female 6–8 years gram was reported) ing; taught through steps of hierarchy; tion); Parents found
of age) and two graduated exposure, TARF-R, IOA the training to be use-
therapist-child behavior shaping, ful and practical
dyads (6–7 years of and contingent
age), all with ASD reinforcement
13
615Table 2 (continued)
616
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
13
Yi and Dixon (2021) 13 parent–child dyads Parents VS using software ACT group: 60-day RCT—group com- Percentage of online Parents in ACT group
(11 males, 2 females (i.e., Zoom, Skye, telehealth ABA parisons lessons parents finished more lessons;
with ASD, average GoToMeeting) parent training cur- completed, aver- no differences in
age: 8 years) riculum included age scores during scores on knowledge
onboarding with knowledge checks; checks; program was
brief ACT session, social validity ques- rated favorably by
5 self-paced les- tionnaires; IOA parents
sons, 5 individual
consultations with
follow-up coach-
ing. Control Group:
same program with
modifications of
onboarding and
progress monitoring
(no ACT session)
Gibson et al. (2010) One 4-year-old male Preschool staff VC using Skype on Initial face-to-face ABAB design to IOA, BIRS-R, Elope- Reduction in elope-
with ASD and two desktops. Verbal FA, video chat evaluate the effec- ment (defined by ment behavior from
preschool staff feedback was consultation with tiveness of FCT consultants) baseline to post-inter-
transmitted via teachers on how intervention on vention, consultation
microphone system to do FCT, and reducing the child’s procedures were
in the staff’s ear immediate feedback behavior (12 ses- found to be accept-
given to teachers on sions) able by teachers
their administration
of the FCT during
class using micro-
phone system
Neely et al. (2016) Three interventionists Interventionist VC using Vsee on Training package Concurrent multiple Interventionist All interventionists
and three children iPad or MacBook to teach novice baseline across behavior: Frequency achieved high fidelity
(all with ASD, (recorded sessions interventionists inci- participants of communication for 4 consecutive
4–8 years of age) at clinic) dental teaching for opportunity, Child sessions, increased
children (feedback behavior: number number of communi-
on videos) of child’s verbal cation opportunities
mands, duration following training,
of training, IOA, two of the three
treatment integrity, interventionists were
TEI-SF able to maintain high
fidelity long term,
each child increased
their mands above
levels at baseline
Clinical Child and Family Psychology Review (2021) 24:599–630Table 2 (continued)
Article Participant character- Telehealth participant Technology Service Design/method Measures Reported outcomes
istics
Barkaia et al. (2017) Three therapists, Therapist VC using Skype and Baseline: coach to Concurrent multiple- Therapist behaviors: Coaching helped
three children (three telephone audio implement interven- baseline design Correct command increase treatment
males, two 4 years connection using tion for language sequences, positive efficacy, therapists
of age, one 6 years Viber development, consequences, Child increased in levels
of age) coached watched behaviors: mands of higher order com-
15 min and provided and echoics, social ments and decreased
feedback Coaching: validity scale in levels of direct
15-min coach- commands, all chil-
ing session to the dren’s verbalization
therapist increased in respond-
ing from baseline, and
children demonstrated
increased echoic
Neely et al. (2018) Two first-tier coaches Coaches, interven- VC using Vsee on After target phase Multiple-baseline Interventionist Incidental teaching
six s-tier interven- tionist iPad (recorded ses- was set via VC, design for remote dependent variables and performance
Clinical Child and Family Psychology Review (2021) 24:599–630
tionists, paired with sions at clinic) coaches conducted incidental teaching, (incidental teaching, criteria were met with
one child with ASD 5-min sessions with multi-probe design communication high fidelity, child
(3–7 years of age) child, completed 1-h to evaluate the opportunities), participants increased
online module, set effects of coaches frequency of child their requests above
target phase via VC teaching interven- requests, IOA, baseline, communica-
with interventionist, tionists to imple- treatment integrity, tion opportunities
met target phase, ment incidental TEI-SF, researcher- were variable, high
and then taught teaching developed question- acceptability of inter-
interventionist via naire vention
VC on target steps
D’Agostino et al., Six preschool Preschool practition- VC using Zoom Telehealth training of Single case multiple Practitioner behavior: A functional relation-
(2020) practitioners and ers NDBI procedures probes across par- frequency of target ship between training
6 children (chil- with coaching ticipants design skill opportunity: and practitioner
dren between 3 sessions involving Child behavior: behavior, and
and 4 years of age, delayed feedback target communica- between training and
only one child with and video self- tion behavior, IOA, the frequency of child
ASD) evaluation treatment fidelity, target communication
TSP questionnaire, behavior, increase in
TEIYD scale, child communication
IRP-15, researcher- opportunities related
developed question- to increase in child
naire behavior, high accept-
ably of training
13
617You can also read