The Adjunctive Use of Ketamine in Severe Alcohol Withdrawal - September 14, 2018 Hope Randle, PharmD PGY1 Pharmacy Resident Seton Healthcare ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Adjunctive Use of Ketamine in
Severe Alcohol Withdrawal
September 14, 2018
Hope Randle, PharmD
PGY1 Pharmacy Resident
Seton Healthcare Family
Christina.randle@ascension.org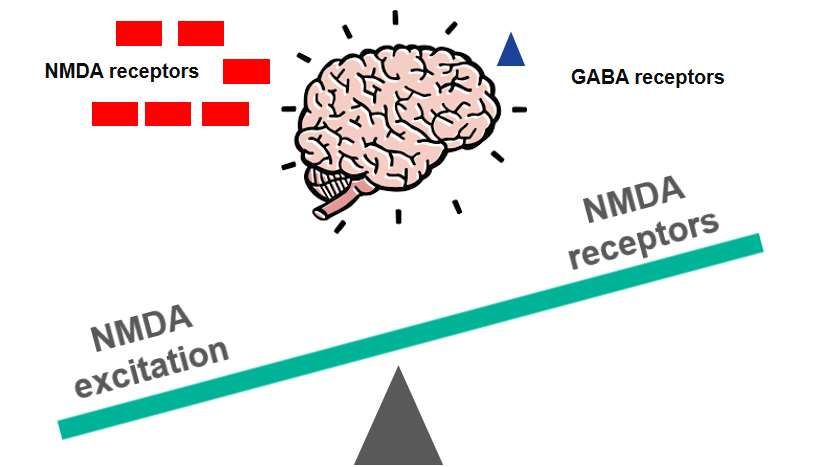
Conflict of Interest
ASCENSION TEXAS
The author of this presentation has no conflicts of interest to
The Adjunctive Use of Ketamine in Severe disclose.
Alcohol Withdrawal
Hope Randle, PharmD
PGY1 Pharmacy Resident
Seton Healthcare Family
September 14, 2018
2
Objectives Patient Case
• Review the pathophysiology of and current treatment DD is a 28 yo caucasian male, presenting to
recommendations for Alcohol Withdrawal Syndrome
(AWS) the ED from home with increased agitation
and new onset hand tremor
• Discuss the pharmacologic properties of ketamine as an
adjunctive agent to current treatment therapies
• HPI: Patient drinks 12 Lone Stars per day and started a
cleanse 3 days ago. His wife brought him to the hospital
• Analyze current literature evaluating the use of ketamine because he was shaking and seeing things.
in severe AWS
• He is diagnosed with alcohol withdrawal in the ED and
started on a symptom-triggered benzodiazepine therapy
• Evaluate the potential role of ketamine in the treatment of
severe AWS
3 4
Alcohol Withdrawal
• Alcohol related disorders affect 7% of the US population
• 25% of adults had at least one heavy drinking day in the
past year
Alcohol Withdrawal Syndrome
(AWS) • 500,000 episodes of alcohol withdrawal requiring
treatment each year
• Estimated cost per year: $223.5 billion
CDC 2015 National Health Interview Summary
Stehman et al. Am J Emerg Med. 2013;31:734-42 .
5 6
Mayo-Smith et al. Arch Intern Med. 2004;164:1405-11.
Walker et al. J Trauma Acute Care Surg. 2013;74(3):926-31.
Alcohol Pathophysiology of Alcohol Withdrawal
• CNS depressant
NMDA receptors GABA receptors
• Gamma-amino-butyric acid (GABA)
proliferation
- Increased inhibitory effects
GABA GABA
• N-methyl-D-aspartate (NMDA) inhibition inhibition receptors
- Decreased excitatory action
• Manifestations: sedation, impaired
decision making, loss of balance,
dizziness, nausea, vomiting
7 Valenzuela, Fernando, MD. Alcohol Health and Research 8 Littleton, J, MD. Alc Health and Research World; 1998, 22(1).
World; 21 (2), 1997.
Pathophysiology of Alcohol Withdrawal Alcohol Withdrawal
NMDA receptors GABA receptors
Symptom Intensity
NMDA NMDA
excitation receptors
9 Biology of the NMDA Receptor Chapter 4: The NMDA 10
Receptor and Alcohol Addiction Jose R Maldonado, MD. Crit Care Clin, 2017, Jul; 33(3); 559-599.
Assessment of Alcohol Withdrawal Severity Management of Alcohol Withdrawal
• Clinical Institute Withdrawal Assessment (CIWA-Ar)
- Scored 0 – 67 based on symptoms • Supportive care: electrolytes, IV fluids, folic acid, thiamine
- Agitation, anxiety, visual/auditory disturbances
- < 8 (mild), 8 – 15 (moderate), > 16 (severe)
- Also used to monitor withdrawal progression • Benzodiazepines (BZD)
- Symptom-triggered (based on CIWA score)
• Withdrawal Assessment Scale (WAS) - Fixed tapered dosing regimen
- Scored 0 – 96 based on symptoms
- Temperature, heart rate, respiratory rate, blood pressure
- Protocol attaches directions to scores • Adverse effects of BZDs
• < 10 no action needed
• 10 – 14: prn BZD - Respiratory depression
• > 14: prn BZD, call physician for reassessment - Sedation
- Delirium
• Motor Activity Assessment Scale (MAAS)
- Scored 0 (unresponsive) to 6 (agitated, uncooperative)
- Based on patient responsiveness and activity
11 See Appendix C, D, and E 12 Jose R Maldonado, MD. Crit Care Clin, 2017 July; 33(3): 559-599
British Journal of Addiction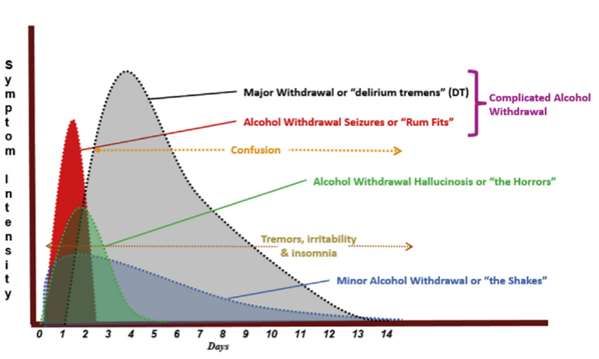
Management of Alcohol Withdrawal DD
Refractory Alcohol Withdrawal (RAW) • Hospital Course:
• Requirement of > 40 mg of diazepam (or diazepam - HPI: alcohol abuse
equivalents) within 1 hour - Admitted to ICU with diagnosis of AWS with delirium tremens (DTs)
- Tremor significantly worsened
• Treatment options
- CIWA Score: 25
Agent Mechanism of Concerns - 50mg diazepam in the last 60 minutes
action
- Symptoms largely unimproved at this time
Phenobarbital GABA agonist Respiratory depression,
bradycardia, hypotension
Dexmedetomidine α2 agonist Hypotension, bradycardia, -What's next?
lacks seizure protection
Propofol GABA agonist Hypotension, respiratory
NMDA antagonist depression
13 See Appendix B 14
Gold et al. Crit Care Med. 2007; 35: 724 – 730
What's wrong with the current
treatment of alcohol withdrawal?
BZD over-usage
→ Risk of over-sedation
→ Mechanical ventilation
→ Longer ICU/hospital stay
→ Increased cost of treatment
→ Increased risk of infection
15 September 7, 2018 16
Ketamine
Mechanism of action: NMDA receptor antagonist
Can adjunctive use of ketamine in
severe AWS improve outcomes?
ketamine
17 18 Abdallah et al. Depression Anxiety, 2016 Aug; 33(8); 689-97
Ketamine Clinical Concerns
Onset: IV effect within 30 seconds
Duration: 5 – 10 minutes
Could the dissociative effects of ketamine
Metabolism: hepatic via N-dealkylation
worsen symptoms?
Elimination: urine (91%)
Side effects: hypertension, tachycardia, dissociative reactions Could ketamine’s activating side effects be
Contraindications: known or suspected schizophrenia offset by BZD use?
Pros:
• Novel, disease state specific mechanism of action
• Short half life
How would ketamine use affect CIWA scoring?
• No respiratory depression
19 Per the American College of Emergency Physicians 20
Ketamine Package Insert. Par Pharmaceuticals. 2012.
Literature Summary
Wong et. al. (n=23) Shah et. al. (n=30) Pizon et. al. (n=63)
Population
Initiation
Duration
Evidence for adjunctive ketamine Dose
use
Adjunctive
agents
Outcomes
Side
Effects
21 22 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9
Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236..
Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771.
Wong et. al. Wong et. al.
• Single center retrospective cohort study (n=23) • RAW: 40mg diazepam / 1 hour
• Purpose: Evaluate the safety and efficacy of ketamine for • Symptom-triggered BZD dosing for WAS score > 10
the management of AWS
• Baseline characteristics: Procedure
- Primarily caucasian, middle aged, males • Ketamine initiation
- 75% experienced DTs - 34hr after first treatment of AWS
- 12hr after RAW designation
- 26% intubated
- Continued for ~ 56 hrs
- 100% required ICU admission for management of AWS
• Dose: optional LD 0.3 mg/kg, continuous IV infusion (CIVI)
• Assessment scales 0.2 mg/kg/hr
- Withdrawal assessment scale (WAS)
• Additional agents:
- Simplified acute psychology score (SAPS) - Dexmedetomidine, phenobarbital, haloperidol, propofol
23 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9 24 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9
Wong et. al. Wong et. al.
• Strengths:
Outcome Ketamine - 83% of patients qualified with BZD resistance
Change in diazepam equivalent at 12 hrs, mg - 40 (-106.7 – 21.7) - Specialized team to handle ketamine initiation/administration
- First study assessing ketamine use in AWS
Change in diazepam equivalent at 24 hrs, mg -13.3 (-86.7 - 50)
Change in WAS score + 1 (-4.5 – 2) • Weaknesses:
- Retrospective cohort study
Length of stay, mean days (SD)
ICU 6.3 (3) - No control group for comparison
Hospital 12.4 (6.6) - Lack of protocol
- Use of other adjunctive agents
Adverse events, n 1 (over-sedation)
Values reported as median (interquartile range), unless otherwise specified
ICU: intensive care unit; SD: standard deviation; WAS: withdrawal assessment scale • Take home points:
- No change in WAS score or sedation level from baseline
- No AWS side effects observed after ketamine initiation
25 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9 26 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9
Literature Summary Shah et. al.
Wong et. al. (n=23) Shah et. al. (n=30) Pizon et. al. (n=63)
Population • 26% intubated
• 100% admitted to • Single center retrospective review (n=30)
ICU
• Purpose: Evaluate the effect of adjunctive ketamine CIVI
Initiation • 34h from diagnosis
Duration • 56h on symptom control and lorazepam infusion requirements
Dose • LD: 0.3 mg/kg (n=8) for BZD-resistant AWS patients in the ICU
• Initial MD: 0.2
•
mg/kg/hr
Median: 0.2 mg/kg/hr
• Baseline characteristics:
Adjunctive • Dexmedetomidine - Male, average age ~ 45 years,
agents • Phenobarbital - Median CIWA score 23 (non-intubated), MAAS 4.6 (intubated)
• Haloperidol
• Propofol - 72% intubated
Outcomes No change in
sedation level • Scales used:
Side • Over-sedation (n=1) - CIWA
effects
- MAAS
27 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9 28 See Appendix B and D
Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236.. Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236..
Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771.
Shah et. al. Shah et. al.
• Severe AWS: CIWA > 20 Outcome Ketamine
• ICU severe AWS protocol:
Average lorazepam infusion rate, mg/hr
- 8mg lorazepam IV q15min x 3 doses
Initiation of ketamine 14
- Phenobarbital 260 mg IV, then 130 mg q15min x8
Post initiation of ketamine 10
- Lorazepam CIVI
Time to initial symptom control, hours
Shah et. al. Literature Summary
Wong et. al. (n=23) Shah et. al. (n=30) Pizon et. al. (n=63)
• Strengths:
Population • 26% Intubated • 72% intubated
- Inclusion of intubated and non-intubated patients • 100% admitted to • 100% admitted to ICU
- Utilized higher doses of ketamine ICU for AWS for AWS
Initiation • 34hr from diagnosis • 41hr from diagnosis
- Assessed length of intubation and ICU stay after ketamine infusion Duration • 56hr • 54hr
Dose • LD: 0.3 mg/kg (n=8) • Bolus: None
• Weaknesses: • Initial MD: 0.2
mg/kg/hr
•
•
Initial MD: 0.5 mg/kg/hr
Average max dose: 1.6
- Retrospective study • Median: 0.2 mg/kg/hr mg/kg/hr
- Other adjunctive agents used Adjunctive • Dexmedetomidine • Diazepam
agents • Phenobarbital
- No control group to assess resulting data • Haloperidol
• Propofol
Outcomes No change in
• Take home points: sedation level BZD requirements
- Ketamine reduced lorazepam requirements Withdrawal
- All patients achieved symptom control within 1 hour of ketamine symptoms
- All CIVI off within 48 hrs Side • Over-sedation (n=1) • Hypertension (n=2)
effectcs
31 Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236.. 32 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9
Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236..
Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771.
Pizon et. al. Pizon et. al.
Control group
• Prospective observational cohort study (n=63)
• Symptom-triggered BZD
• Intubation
• Purpose: Determine if treatment guidelines using - Propofol
adjunctive ketamine infusion improves patient suffering - Dexmedetomidine
from severe AWS
Ketamine group
• Symptom-triggered BZD
• Severe AWS: presence DTs • IV ketamine initiated immediately upon diagnosis of DTs
• Dosing
- LD: 0.3 mg/kg (optional)
- CIVI: 0.15 – 0.3 mg/kg/hr
- Average dose: 0.19 mg/kg/hr
• Additional agents:
- Propofol, phenobarbital, dexmedetomidine
33 Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771. 34 Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771.
Pizon et. al. Pizon et. al.
Outcome Control Ketamine p value • Strengths:
(n=29) (n=34) - Control group that did not receive ketamine
Mean ICU (days) 11.2 5.7 < 0.01 - Assessed length of stay, BZD use, and intubation requirements
- Addressed confounding elements
Mean hospital length 16.6 12.5 0.03
of stay (days)
• Weaknesses:
Mean diazepam 2,500 1,500 0.02 - No standardized ketamine protocol
equivalent (mg) - Variation of admission diagnoses
Intubations (number) 22 10
Literature Comparison
Population
Wong et. al. (n=23)
• 26% Intubated
Shah et. al. (n=30)
• 72% intubated
Pizon et. al. (n=63)
• 100% admitted to ICU for
Can adjunctive use of ketamine in
• 100% admitted to
ICU for AWS
• 100% admitted to ICU
for AWS
treatment of DTs
severe AWS improve outcomes?
Initiation • 34hr from diagnosis • 41hr from diagnosis • Immediately on diagnosis
Duration • 56hr • 54hr • 47hr
Dose • LD: 0.3 mg/kg (n=8) • Bolus: None • LD: 0.3 mg/kg (n=19/34)
• Initial MD: 0.2 • Initial MD: 0.5 mg/kg/hr • Initial MD: 0.15 mg/kg/hr
mg/kg/hr • Average max dose: 1.6 • Average dose: 0.19
• Median: 0.2 mg/kg/hr mg/kg/hr mg/kg/hr
Adjunctive • Dexmedetomidine • Diazepam • Dexmedetomidine
agents • Phenobarbital • Propofol
• Haloperidol • Phenobarbital
• Propofol
Outcomes
No change in BZD requirements Risk of intubation
sedation level
Withdrawal symptoms ICU length of stay
BZD requirements
Side effects • Over sedation (n=1) • Hypertension (n=2) • Over sedation (n=1)
37 Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9 38
Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236..
Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771.
Ketamine Advantages / Disadvantages Application: What dose to give?
Study Doses:
Advantages Disadvantages
Wong et. al. Shah et. al. Pizon et. al.
• NMDA antagonistic properties • Hypertension Bolus: 0.3 mg/kg N/A 0.3 mg/kg
Initial dose: 0.2 mg/kg/h 0.5 mg/kg/h 0.15 mg/kg/h
• Short duration of action • No consistent protocol
Difficult to assess existing Average dose: 0.2 mg/kg/h 1.6 mg/kg/h (max) 0.19 mg/kg/h
• Use does not require data
intubation
• Optimal dosing unknown Recommended dosing in critically ill patients:
• May decrease BZD usage
Source Bolus Dosing
• May decreased risk of PAD Guidelines (2013) 0.1 - 0.5 mg/kg 0.05 - 0.4 mg/kg/hr
respiratory failure PADIS Guidelines (2018) 0.5 mg/kg 0.06 – 0.12 mg/kg/hr
PAD: Pain, Agitation, Delirium
PADIS: Pain, Agitation/Sedation, Delirium, Immobility, Sleep Disruption
39 40 Barr et al. Crit Care Med, 2013 Jan; 41(1); 263-306
Devlin et al. Crit Care Med, 2018 sep; 46(9); e825-73
DD
• Received 50 mg lorazepam over last 60 minutes
• Symptoms largely unimproved at this time
What therapy to recommend next?
41 42 September 7, 2018Recommendation Conclusion: Ketamine in Severe AWS
Symptom-triggered
AWS Diagnosis
BZD • Ketamine offers logical mechanistic benefit for adjunctive
treatment of severe AWS
Does patient • Limited studies investigating clinical outcomes
require > 40mg
diazepam in 1 hr? • Available data suggest a benefit of adjunctive ketamine
treatment
No Yes
- Decrease BZD requirements
- Decrease ICU length of stay
- Decrease risk of intubation
Continue Increased risk of
- Few adverse effects
symptom- respiratory depression
triggered BZD / hypotension
dosing
Consider ketamine
43 44
Acknowledgements
ASCENSION TEXAS
• Evaluator: Merry Daniel, PharmD, BCCCP
The Adjunctive Use of Ketamine in Severe
• Molly Curran, PharmD, BCPS, BCCCP Alcohol Withdrawal
• Emily Hodge, PharmD, BCCCP
Hope Randle, PharmD
PGY1 Pharmacy Resident
Seton Healthcare Family
September 14, 2018
45Appendices Appendix A. Abbreviations Appendix B. Benzodiazepine dosing equivalents Appendix C. Clinical Institute Withdrawal Assessment Score Appendix D. Withdrawal Assessment Scale Appendix E. Motor Activity Assessment Scale Appendix F. Wong et. al. Outcomes Appendix G. Shah et. al. Outcomes Appendix H. Pizon et. al. Outcomes Appendix I. Literature Comparison
Appendix A. Abbreviations Abbreviation Meaning AWS Alcohol Withdrawal Syndrome BZD Benzodiazepine CIVI Continuous IV Infusion CIWA-Ar Clinical Institute Withdrawal Assessment in Alcohol - Revised DTs Delirium Tremens ED Emergency Department GABA Gamma-amino-butyric acid ICU Intensive Care Unit MAAS Motor Activity Assessment Scale NMDA N-methyl-D-aspartate PAD Pain, Agitation, Delirium PADIS Pain, Agitation, Delirium, Immobility, Sleep Disruption RAW Resistant Alcohol Withdrawal SAPS Simplified Acute Psychology Score WAS Withdrawal Assessment Scale
Appendix B. Benzodiazepine Dosing Equivalents Benzodiazepine Equivalent dose Alprazolam 0.5 mg Diazepam 5 mg Lorazepam 1 mg Clinical Handbook of Psychotropic Drugs, 4th revised edition, Bezchlibnyk-Butler et al. editors Hogrefe & Huber.
Appendix C. Clinical Institute Withdrawal Assessment (CIWA-Ar) Score Procedure:
1. Assess and rate each of the 10 criteria of the CIWA scale. Each criterion is rated on a
scale from 0 to 7, except for “Orientation and clouding of sensorium” which is rated on
scale 0 to 4.
2. Add up the scores for all ten criteria. This is the total CIWA-Ar score for the patient at
that time. Early intervention for CIWA-Ar score of 8 or greater provides the best means
to prevent the progression of withdrawal.
Total Score Interpretation
Score Severity
16 Severe
Sullivan et al. Brit J Addict, 1989 Nov; 84(11):1353-7.Appendix D. Withdrawal Assessment Scale (WAS)
WITHDRAWAL ASSESSMENT SCALE
Name __________________________________ Hospital number ______________________________________
Temperature (per axilla)
1 37.0-37.50 C 2 37.5-38.ooc 3 Greater than 38.00C
Pulse (beats per minute)
3 100-105 5 110-120
2 95-100 4 105-110 6 Greater than 120
Respiration rate (inspirations per minute)
1 20-24 2 Greater than 24
Blood pressure (diastolic)
1 95-100 mmHg 3 103-106 mmHg 5 109-112 mmHg
2 100-103 mmHg 4 106-109 mmHg 6 Greater than 112 mmH
Nausea and vomiting (Do you feel sick? Have you vomited?)
O None 4 Intermittent nausea with dry heaves
2 Nausea with no vomiting 6 Nausea, dry heaves, vomiting
Tremor (arms extended, fingers spread) O
No tremor 4 Moderate with arms extended
2 Not visible — can be felt fingertip to fingertip 6 Severe even with arms not extended
Sweating (observation) O
No sweat visible 4 Beads of sweat visible
2 Barely perceptible, palms moist 6 Drenching sweats
Tactile disturbances
O None
2 Mild itching or pins and needles or numbness
4 Intermittent tactile hallucinations (for example, bug crawling)
6 Continuous tactile hallucinations s
Auditory disturbances (loud noises, hearing voices)
O Not present
2 Mild harshness or ability to frighten (increased sensitivity)
4 Intermittent auditory hallucinations (appears to hear things you cannot)
6 Continuous auditory hallucinations (shouting, talking to unseen persons)
Visual disturbances (photophobia, seeing things)
O Not present
2 Mild sensitivity (bothered by the lights)
4 Intermittent visual hallucinations (occasionally sees things you cannot) 6
Continuous visual hallucinations (seeing things constantly)
Hallucinations
O None 2 Non-fused auditory or visual
1 Auditory, tactile or visual only 3 Fused auditory and visual
Clouding of sensorium (What day is this? What is this place?)
O Orientated
2 Disorientated for date by no more than two days
3 Disorientated for date
4 Disorientated for place (re-orientate if necessary)
Quality of contact
O In contact with examiner
2 Seems in contact, but is oblivious to environment
4 Periodically becomes detached6 Makes no contact with examiner
Anxiety (Do you feel nervous?) (observation)
O No anxiety; at ease 4 Moderately anxious, or guarded
2 Appears anxious 6 Overt anxiety (equal to panic)
Agitation (observation)
O Normal activity 4 Moderately fidgety and restless
2 Somewhat more than normal activity 6 Pacing, or thrashing about constantly
Thought disturbances (flight of ideas)
0 No disturbance
2 Does not have much control over nature of thoughts
4 Plagued by unpleasant thoughts constantly
6 Thoughts come quickly and in a disconnected fashion
Convulsions (seizures or fits of any kind) O
No 6 Yes
Headache (Does it feel like a band around your head?) O
Not present 4 Moderately severe
2 Mild 6 Severe
Flushing of face
O None 2 Severe
Total
Date
Time
FIGURE: The alcohol withdrawal assessment scale (adapted from Shaw et al).
Shaw et al. J Clin Psychopharmacol, 1984; 1: 382-389Appendix E. Motor Activity Assessment Scale
Score Description Definition
0 Unresponsive Does not move with noxious stimuli
1 Responsive only to Opens eyes or raises eyebrows or turns head toward
noxious stimuli stimulus or moves limb with noxious stimuli
2 Responsive to touch or Opens eyes or raises eyebrows or turns head toward
name stimulus or moves limb when touches or name loudly
spoken
3 Calm and cooperative No external stimulus is required to elicit movement
and patient is adjusting sheets or clothing
purposefully and follows commands
4 Reckless and cooperative No external stimulus is required to elicit movement
and patient is picking at sheets or tubes or uncovering
self and following commands
5 Agitated No external stimulus is required to elicit movement
and attempting to sit up or moves limb out of bed and
does not follow commands
6 Dangerously agitated, No external stimulus is required to elicit movement
uncooperative and patient is pulling at tubes or catheters or
thrashing side to side or striking at staff or trying to
climb out of bed and does not calm down when asked
Devlin et al. Crit Care Med. 1999, Jul; 27(7): 1271-5
Appendix F. Wong et. al. Outcomes
Outcome Ketamine
Change in diazepam equivalent at 12 hrs, mg - 40 (-106.7 – 21.7)
Change in diazepam equivalent at 24 hrs, mg -13.3 (-86.7 - 50)
Change in WAS score + 1 (-4.5 – 2)Length of stay, mean days (SD) 6.3 (3)
ICU 12.4 (6.6)
Hospital
Adverse events, n 1 (over-sedation)
Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9Appendix G. Shah et. al. Outcomes
Outcome
Average lorazepam infusion rate, mg/hr Prior
to initiation of ketamine 14
Upon discontinuation of ketamine 10
Time to initial symptom control, hoursMean diazepam 2,500 1,500 0.02 equivalent (mg) Intubations (number) 22 10
Appendix I. Literature Review
Wong et. al. (n=23) Shah et. al. (n=30) Pizon et. al. (n=63)
Population • 26% Intubated • 72% intubated • 100% admitted to ICU for
• 100% admitted to • 100% admitted to ICU treatment of DTs
ICU for AWS for AWS
Initiation • 34hr from diagnosis • 41hr from diagnosis • Immediately on diagnosis
Duration • 56hr • 54hr • 47hr
Dose • LD: 0.3 mg/kg (n=8) • Bolus: None • LD: 0.3 mg/kg (n=19/34)
• Initial MD: 0.2 • Initial MD: 0.5 • Initial MD: 0.15 mg/kg/hr
mg/kg/hr mg/kg/hr • Average dose: 0.19
• Median: 0.2 • Average max dose: 1.6 mg/kg/hr
mg/kg/hr mg/kg/hr
Adjunctive • Dexmedetomidine • Diazepam • Dexmedetomidine
agents • Phenobarbital • Propofol
• Haloperidol • Phenobarbital
• Propofol
Outcomes No change in sedation BZD requirements Risk of intubation
level ICU length of stay
Withdrawal symptoms BZD requirements
Side • Over sedation (n=1) • Hypertension (n=2) • Over sedation (n=1)
effects
Wong et al. Ann Pharmacother, Jan 2015; 49(1):14-9
Shah et al. Journ of Med Tox. Sept 2018; 14(3), 229 – 236
Pizon et al. Crit Care Med, aug 2018. 46(8); e768-e771You can also read