THE MEDICAL TREATMENT OF OBESITY - Session # 1 January 9th, 2020 - ECHO OBN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THE MEDICAL TREATMENT OF OBESITY Session # 1 January 9th, 2020
DISCLOSURES Liviu Danescu MD, FACE January 9, 2020 Disclosures: Grants/Research Support: Novo Nordisk Canada, Valeant, Servier, Sanofi Speaker’s Bureau/Honoraria: Boehringer-Ingelheim, Eli Lilly, Novo Nordisk Canada, Sanofi, AstraZeneca, Jansen, Valeant, Bausch Health, Abbott, Sutherland Global Services Canada ULC Consulting Fees: Boehringer-Ingelheim, Eli Lilly, Novo Nordisk Canada, Sanofi, AstraZeneca, Jansen, Valeant, Bausch Health, Abbott
ACKNOWLEDGEMENTS These slides were prepared and originally presented by: Dr. Stephen A. Glazer MD FRCPC FCCP Humber River Regional Hospital *Slides have been modified for today’s session Special thanks to Jennifer Brown from the Ottawa BCOE
OBJECTIVES
1) How do we define obesity?
▪ Obesity as a chronic disease
▪ Assessment and management options
2) Patient engagement strategies
▪ Bariatric centres of excellence
3) Medications for obesity management
▪ Meal replacements: Optifast®
▪ Medications: Orlistat, Liraglutide, Buproprion/Naltrexone
4) Questions
HOW DO WE DEFINE OBESITY?
OBESITY: HISTORICAL APPROACHES
25 to
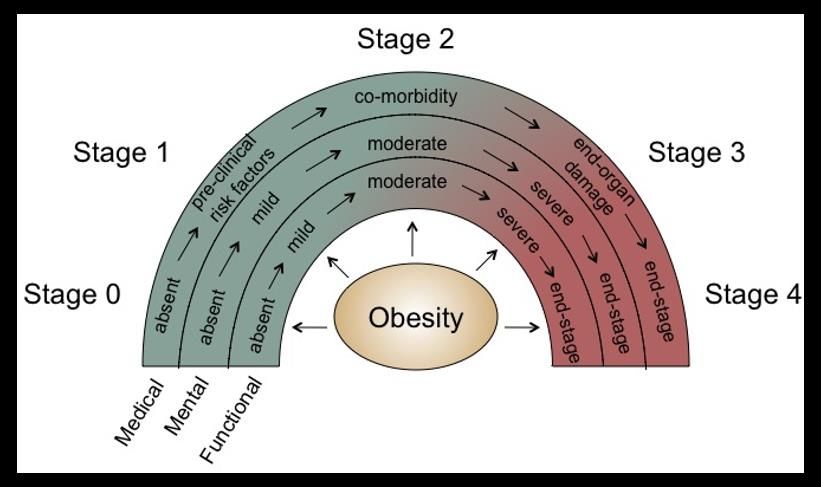
OBESITY: NEW APPROACHES
Edmonton Obesity
Staging System (EOSS)
or King’s Criteria
Looks at the health and
complication-based
conditions (medical,
mental and functional)
not size or weight alone
FACTORS AFFECTING WEIGHT
Social Influences
Individual Physiology
Food Food Individual Activity
Production Intake Activity Environment
Biology
http://kim.foresight.gov.uk/Obesity/Obesity.html
OBESITY IS A CHRONIC DISEASE
Canadian Medical Association (CMA)
declared obesity a chronic disease in 2015
▪ Multiple factors contributing to body weight
(genetics, physiology/metabolism, environmental,
psychosocial, etc)
▪ Excessive adipose tissue affecting health (medical, mental
and functional health)
▪ Other organizations have also declared obesity a chronic disease:
▪ American Medical Association (AMA)
▪ World Health Organization (WHO)
▪ World Obesity Foundation (WOF)
CMA. CMA recognizes obesity as a disease. 2015. https://www.cma.ca/En/Pages/cma-recognizes-obesity-as-a-disease.aspx.
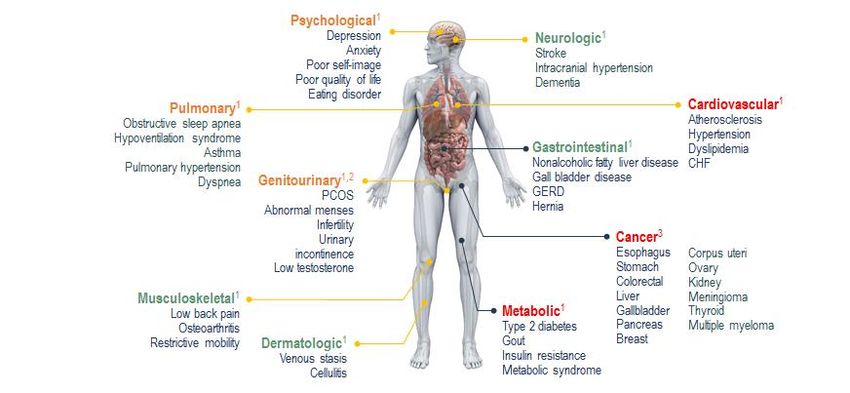
OBESITY IS A COMPLEX CHRONIC DISEASE CHF = congestive heart failure; GERD = gastroesophageal reflux disease; PCOS = polycystic ovarian syndrome. 1. Catenacci VA et al. Clin Chest Med. 2009;30:415-444. 2. Wang C et al. Diabetes Care. 2011;34:1669-1675. 3. Lauby-Secretan B et al. N Engl J Med. 2016;375:794-798.
HEALTH BENEFITS OF WEIGHT LOSS Cefalu et al. Diabetes Care. 2015; 38:1567-1582.
OBESITY: EXPECTATIONS Adapted from www.drsharma.ca & Ryan et al. Arch Intern Med. 2010 Jan 25;170(2):146-54.
MANAGING WEIGHT IS TRICKY
Body weight conservation (adipose tissue): evolutionary protective mechanism to
defend against weight loss
Hormonal Adaptation Thermogenic Adaptation
▪ Hunger hormones ↑ ▪ Energy expenditure ↓
▪ Satiety hormones ↓ after weight loss
▪ Desire to eat highly ▪ Homeostatic drivers in
palatable foods ↑ brain adapt to want to
▪ All to defend against conserve energy and
weight loss (adipose loss) increase body weight
Morton GJ, et al. Nature. 2006;443:289-295.
Leibel RL, et al. N Engl J Med. 1995;31:621-628.
Schwartz A & Doucet É. Obes Rev. 2010;11:531–547.
Sumithran P et al. N Engl J Med. 2011;365:1597–1604.PATIENT ENGAGEMENT STRATEGIES
MYTHS SURROUNDING OBESITY:
THE LIVED EXPERIENCE
“Food causes
obesity” “It’s just a lack of
will power”
“Obesity is
a choice”
“Who cares
about why?
“Calories in, Just eat less”
calories out”UNDERSTAND & LISTEN
Ask Ask for permission to discuss their weight and explore readiness
Assess health status, obesity-related risks (BMI + EOSS) and root causes to their
Assess weight gain (metabolic, functional, mental health, environment)
Advise on health risks and benefits of treatment options.
Advise Aim for focus on improving HEALTH rather than simply weight loss
Agree Agree on health outcomes and behaviour-related goals
Assist in accessing appropriate resources, providers, programs to support
Assist patients goals/behaviours
Refer to the 5A‘s of Obesity Management for research and resources on use in Primary Care: https://obesitycanada.ca/resources/5as/EXPECTATION MANAGEMENT:
ALIGNING HCP/PATIENT EXPECTATIONS
▪ Discuss patient goals prior to
treatment to identify unrealistic
expectations
▪ Discuss biological/physiological
Patient Expectations limitation HCP Expectations
▪ Shift goals beyond weight loss -5-10%
- 30% ▪ Improvement in metabolic and
cardiovascular measures
▪ Improvements in quality of life measures
HCP = healthcare professional.
Foster et al. Am J Clin Nutr. 2005;82(suppl):230S-235S.COUNSELLING WITHOUT PERCEIVED JUDGEMENT IMPROVES
PATIENT OUTCOMES
Patients who received
Patients who did not
weight-management
perceive judgment
counseling were
during counseling were
5x more likely to achieve
more likely to attempt
weight loss than those
≥10%
weight loss compared
who did not, and
with patients who did
achieve clinically
perceive judgment
significant weight loss
aA US cross-sectional, internet-based survey in 600 adults with overweight/obesity (BMI ≥25 kg/m2) to assess differences
in weight-loss attempts and clinically significant weight loss (≥10%) based on receipt of HCP counseling and perceived judgment.
BMI = body mass index; HCP = health care professional.
Gudzune KA et al. Prev Med. 2014;62:103-107.PUTTING THE PATIENT FIRST
DO SAY OR “Patients living with…”
~20% WRITE ▪ Obesity
▪ A higher weight
of patients who perceive
▪ Weight problems
weight stigma from their
health care provider
would avoid future
▪ Obese
appointments or seek out DON’T SAY OR ▪ Fat*
a new health care WRITE ▪ Extremely obese
provider ▪ Super or morbid obese
Obesity Action Coalition. http://www.obesityaction.org/wp-content/uploads/People-First.pdf. Accessed July 20, 2016; 2. Puhl R et al. Int J Obes (London). 2013;37:612-619.CANADIAN CENTRES OF EXCELLENCE IN
BARIATRIC MEDICINEHOSPITAL MEDICAL PROGRAMS
Case Management
• Patient assessment by physicians or nurse practitioner with expertise in bariatric medicine
Registered Dietitian
Social Worker, Psychologist or Behaviourist
Kinesiologist, Exercise Physiologist, Physiotherapist, Occupational Therapist
Access to pharmacotherapy counsellingMEDICATIONS FOR OBESITY MANAGEMENT
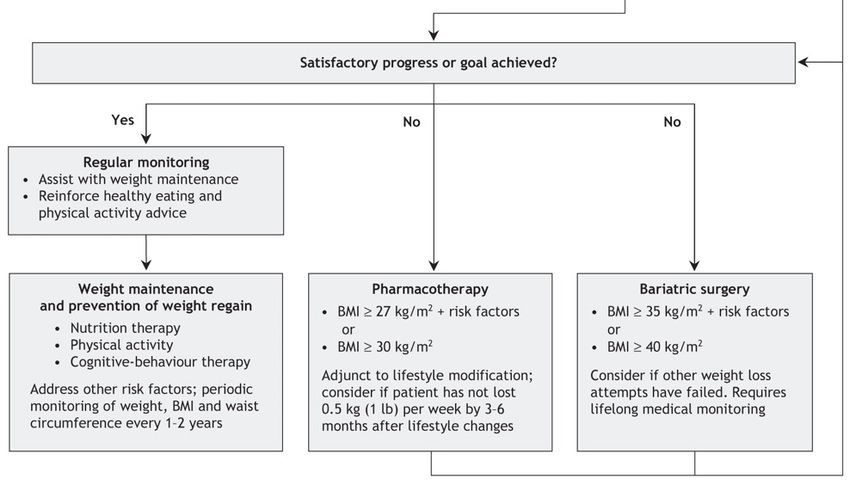
WHEN IS PHARMACOTHERAPY APPROPRIATE?
Pharmacotherapy (Based on 2006 CPG)
BMI ≥27 kg/m2 + risk factors or
BMI ≥30km/m2
Adjunct to lifestyle modifications consider if
patient has not lost 0.5kg (1lb) per week by 3 – 6
months after lifestyle changes
UPDATED Canadian CPG for
Obesity Management coming
early 2020ORLISTAT
▪ Pancreatic and gastric lipase inhibitor
▪ Naturally produced by Stephomyces toxytricini
▪ Mechanism of action:
▪ Forms covalent bond with active serine site of gastric and
pancreatic lipases in lumen of GI tract
▪ Prevents enzymes from hydrolyzing dietary fat (triglycerides)
into absorbable free fatty acids and monoglycerols
▪ Undigested triglycerides are eliminated in feces
▪ Lipase inhibition decreases dietary fat absorption
(contributing to lower caloric intake → weight
loss)
1.Heck et al. Pharmacotherapy. 2000; 20(3): 270-279. 2. Hadvary et al. Biochem J. 1988; 256:357-361. 3. Borgstrom et al. Biochim Biophys Acta. 1998; 962:308-316. 4. Hadvary et al. J
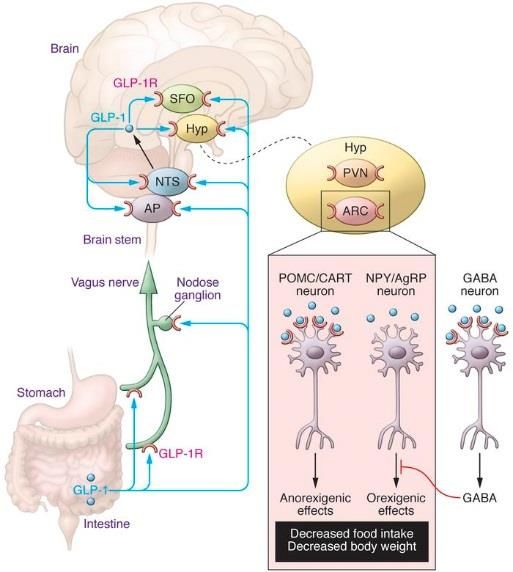
Biol Chem. 1991; 266(4):2021-2027. 5.Ransac et al. Eur J Biochem. 1991; 202:395-400.LIRAGLUTIDE
▪ Peripheral administration of GLP-1 receptor agonists
▪ Reduces short term oral intake
▪ Promotes satiety
▪ Decreases energy intake
▪ Net effect = decreases body weight
▪ Mechanisms of action:
▪ GLP-1 receptors are expressed in the stomach on gastric parietal
cells
▪ Interact with receptors localized to hypothalamic CNS centers that
regulate eating behaviors
▪ Activating neurons in the CNS coupled to gastrointestinal motility
and gastric emptying (ascending neural pathways; vagal afferent
fibers)
1. Shaefer et al. Postgrad Med. 2015; 127(8): 818-826; 2. Elrick et al. J Clin Endocrinol Metab. 1964; 24:1076-1082; 3.Baggio et al. Gastroenterology. 2007; 132: 2131-2157; 4.Nauck et al. J Clin
Endocrinol Metab. 1986;63:492-498; 5.Baggio et al. J Clin Invest. 2014;124(10):4223-4226.COMBINATION: NALTREXONE AND BUPROPION
The hypothalamus (hunger The mesolimbic reward
center) to reduce hunger system to help control cravings
1. Naltrexone product information; 2. Wellbutrin SR Product Information.REGULATION OF HUNGER:
ROLE OF HYPOTHALAMIC POMC NEURONS
POMC neurons
▪ Integrate multiple energy
Hypothalamus balance signals
α-MSH
▪ Released from POMC neuron
POMC stimulus ▪ Binds to MC4-R to decrease food
intake
α-MSH
POMC
neuron
↓ Appetite
↑ Energy Expenditure
MC4-R
µ-opioid receptor
POMC negative feedback loop
β-endorphin (endogenous opioid)
▪ Released from POMC neuron with α-MSH
▪ Binds to µ-opioid receptor to increase food intake and conserve energy (negative feedback
loop)
1. Billes SK et al. Pharmacol Res. 2014;84:1-11. 2. Modi, Renuca. Pharmacotherapy III: Contrave for Chronic Weight ManagementSYNERGISTIC ACTION OF NALTREXONE & BUPROPION TO
ACTIVATE POMC NEURONS TO SUPPRESS APPETITE
Hypothalamus
Directly ↑ POMC activity
POMC
neuron
↑ POMC activity
↓ Hunger
↓ Weight
Indirectly ↑ POMC activity
Figure adapted from Billes et al,1 © 2014, and Modi R2, 2018
1. Billes SK et al. Pharmacol Res. 2014;84:1-11. 2. Modi, Renuca. Pharmacotherapy III: Contrave for Chronic Weight ManagementCHOOSING A MEDICATION: CONTRAINDICATIONS Orlistat • Chronic Malabosprtion, Cholestasis, Cyclosporin Liraglutide • PHx/FHx medullary thyroid Ca, Multiple endocrine neoplasia syndrome type 2 (MEN2) • Females – actively trying to conceive Bupropion/Naltrexone • HTN, Seizures, Eating Disorder(s), Severe Hepatic Impairment, End-stage Renal Failure • Use of opiods or opioid agonists, Thioridazine, MAOIs, Tamoxifen • Abrupt d/c of etoh, sedative and/or antiepileptic drugs
CHOOSING A MEDICATION: CAUTIONS Orlistat ▪ Nephrolithisais (Ca oxalate) Liraglutide ▪ Pancreatitis, Gallstones, Arrhythmias Bupropion/Naltrexone ▪ CYP2B6 inhibitors: Clopidogrel, ticlopidine ▪ Inhibits CYP2D6: SSRI, SNRI, B-Blockers, Type 1 C Antiarrhythmic (proprafenone, flecainaide) ▪ Anxiety, Insomnia, Arrhythmia
CHOOSING A MEDICATION: PATIENT CONSIDERATIONS
Considerations Orlistat Liraglutide Bupropion/Naltrexone
Pre-diabetes Pre-diabetes Smoker
Comorbidities Constipation Type 2 Diabetes Desire to decrease ETOH
Dyslipidemia Depression
Hunger None Yes Yes
Cravings None None to Mild Mild to StrongSUMMARY ▪ Obesity is a complex, chronic disease defined by having excess or abnormal adipose tissue that impairs health ▪ Use comprehensive medical assessment of health factors (medical, mental and functional health) → EOSS instead of BMI alone ▪ Use 5As to obesity management ▪ Medications can be part of obesity management ▪ Lifelong management
QUESTIONS
&
DISCUSSIONREFERENCES
Jensen MD et al. J Am Coll Cardiol. 2014;63:2985-3023; Mathew B, et al. J Am Board Fam Med. 2008;21:562-568.
Lau DCW et al. CMAJ. 2007;176:1103-6; Mokdad AH, et al. JaMA. 2003;289:76-79.
CDA Guidelines. Can J Diabetes. 2013;37(suppl 1):S1-212 Billes SK et al. Pharmacol Res. 2014;84:1-11.
NCD Risk Factor Collaboration. Lancet. 2016;387:1377-96. Hollander P, et al. Diabetes Care. 2013;36:4022-4029.
NCD Risk Factor Collaboration. http://www.ncdrisc.org/d- Apovian CM, et al. Obesity..13;21:935-943
adiposity.html.
Luppino FS, et al. Arch Gen Psychiatry. 2010;67:220-229.
Twells et al. CMAJ OPEN. 2014; 2(1): 18-26.
Parkin DM, et al. Br J Cancer. 2011;105(suppl 2):S77-S81
Thomas CE et al. Obesity. 2016;24:1955-1961.
Calle, EE., et al. N Engl J Med. 1999;341:1097-1105.
Catenacci VA et al. Clin Chest Med. 2009;30:415-444.
CMA. CMA recognizes obesity as a disease. 2015.
Wang C et al. Diabetes Care. 2011;34:1669-1675. https://www.cma.ca/En/Pages/cma-recognizes-obesity-as-a-
disease.aspx.
Lauby-Secretan B et al. N Engl J Med. 2016;375:794-798.
Whitlock G, et al. Lancet. 2009;373:1083-1096REFERENCES
Garvey WT, et al. [published online May 24, 2016]. Endocr Pract. Morton GJ, et al. Nature. 2006;443:289-295. 2. Leibel RL, et al. N
Engl J Med. 1995;31:621-628.
Jensen, MD et al. Circulation 2014: 129;5102-38.
Schwartz A & Doucet É. Obes Rev. 2010;11:531–547.
National Heart, Lung, and Blood Institute. 2002.
https://www.nhlbi.nih.gov/files/docs/resources/heart/steps.pdf. Sumithran P et al. N Engl J Med. 2011;365:1597–1604.
Accessed July 26, 2016.
Rosenbaum M et al. Am J Physiol Regul Integr Comp Physiol.
Obesity Society. http://www.obesity.org/obesity/resources/facts- 2003;285:R183–R192.
about-obesity/infographics/potential-contributors-to-obesity.
Accessed April 4, 2017. Rosenbaum M & Leibel R. L. Int J Obes (Lond). 2010 October ; 34(0
1): S47–S55.
Foster et al. Am J Clin Nutr. 2005;82(suppl):230S-235S.
Ryan et al. Arch Intern Med. 2010 Jan 25;170(2):146-54
CONTRAVE [product monograph], February 12, 2018, Valeant
Canada LP; Laval, QC. Lau, et al. 2006 Canadian clinical practice guidelines on the
management and prevention of obesity in adults and children.
Obesity Action Coalition. http://www.obesityaction.org/wp- CMAJ. 2007;176(8 suppl):Online-1-117.
content/uploads/People-First.pdf. Accessed July 20, 2016; 2. Puhl
R et al. Int J Obes (London). 2013;37:612-619. Heck et al. Pharmacotherapy. 2000; 20(3): 270-279
Gudzune KA et al. Prev Med. 2014;62:103-107. 2
2REFERENCES
Hadvary et al. Biochem J. 1988; 256:357-361. Nauck et al. J Clin Endocrinol Metab. 1986;63:492-498
Borgstrom et al. Biochim Biophys Acta. 1998; 962:308-316. Baggio et al. J Clin Invest. 2014;124(10):4223-4226.
Hadvary et al. J Biol Chem. 1991; 266(4):2021-2027. Saxenda (product monograph), July 12, 2017, Novo Nordisk Canada
Inc, Mississauga, ON.
Ransac et al. Eur J Biochem. 1991; 202:395-400.
CONTRAVE [product monograph], February 12, 2018, Valeant
Xenical (product monograph), November 18, 2015, Hoffmann-La Canada LP; Laval, QC.
Roche Limited, Mississauga, ON.
Naltrexone product information; Wellbutrin SR Product Information.
Shaefer et al. Postgrad Med. 2015; 127(8): 818-826
Greenway FL, et al. Lancet. 2010;376:595-605;3. Wadden TA, et al.
Elrick et al. J Clin Endocrinol Metab. 1964; 24:1076-1082 Obesity. 2011;19:110-120
Baggio et al. Gastroenterology. 2007; 132: 2131-2157
2You can also read