The planning and delivery of support for adults with complex needs; lessons learnt from the Emergency Response to rough sleepers housed as part of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
February 2021
The planning and delivery of support for adults with complex needs; lessons
learnt from the Emergency Response to rough sleepers housed as part of the
‘Everyone In’ COVID-19 Government initiative;
Evaluation Report
Key Messages
The emergency response to providing support for people presenting as homeless with complex needs (MDT model) demonstrated that this
approach is an effective and feasible model for creating greater efficiencies and reducing the burden on statutory services in
Hertfordshire; providing timely and appropriate support for service users and improved system efficiencies in line with the Hertfordshire
Supporting Adults with Complex Needs Strategy (HCC 2020 - Referred to as the Strategy).
A number of factors cemented this outcome;
• Effective partnership working between Hertfordshire County Council statutory services, and District Homelessness Teams
• A joint commitment to housing and supporting service users with complex needs
• Robust data collection and analysis to enable process and outcome evaluation
• Implementation of effective feedback mechanisms to enable continuous improvement
The potential benefits for statutory services of adopting this model include;
• Reduce needs escalation thus reducing the burden and cost on statutory services
• Improved communication between agencies leading to a reduction in inappropriate referrals/increase in appropriate referrals
• Improved understanding of remit, roles and responsibilities between agencies.
• Reduced workload and time spent chasing individual agencies
• Reduced hospital (re)admissions and ambulance callouts
• Reduced offending/police time
hertshealthevidence.org
1
PH.Evaluation@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Thorough planning and scoping activities involving all stakeholders will enable a further Countywide Pilot which will aim to increase the
capacity for statutory services to conduct preventative interventions and develop a common assessment framework, while effectively
demonstrating impact.
Author: Nichola Lee, Senior Public Health Evaluation Officer
Table of Contents
Key Messages.......................................................................................................................................................................................................................... 1
1. Introduction ............................................................................................................................................................................................................................ 4
1.1 Objectives ............................................................................................................................................................................................................................................................................................. 4
1.2 Definitions ............................................................................................................................................................................................................................................................................................ 5
1.3 Background.......................................................................................................................................................................................................................................................................................... 5
1.4 Local and National Picture ............................................................................................................................................................................................................................................................. 6
1.5 Commissioning and Procurement .............................................................................................................................................................................................................................................. 6
1.6 ‘Everyone In’ ........................................................................................................................................................................................................................................................................................ 6
2. Description of the Intervention ............................................................................................................................................................................................ 7
2.1 RS MDT Meeting Protocol ............................................................................................................................................................................................................................................................. 7
2.2 Identification of Cases ..................................................................................................................................................................................................................................................................... 7
2.3 Consent/Data Protection ................................................................................................................................................................................................................................................................ 8
3. Evaluation ............................................................................................................................................................................................................................... 8
3.1 Qualitative Data Collection ............................................................................................................................................................................................................................................................ 8
3.2 Quantitative Data Collection ......................................................................................................................................................................................................................................................... 9
hertshealthevidence.org
2
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
4. Results ..................................................................................................................................................................................................................................... 9
4.1 RS MDT Output Statistics ............................................................................................................................................................................................................................................................ 9
4.2 RS MDT Meeting Observations ................................................................................................................................................................................................................................................. 9
4.3 Key Themes....................................................................................................................................................................................................................................................................................... 14
4.4 Limitations of the Evaluation Methodology......................................................................................................................................................................................................................... 21
5. Recommendations ............................................................................................................................................................................................................... 21
5.1 A Countywide Pilot ........................................................................................................................................................................................................................................................................ 21
5.2 Common Assessment Framework Creation ......................................................................................................................................................................................................................... 23
5.3 Importance of Data........................................................................................................................................................................................................................................................................ 24
5.4 Sharing of Good Practice ............................................................................................................................................................................................................................................................ 24
5.5 Development of the Rough Sleeper MDT Toolkit for Practitioners ............................................................................................................................................................................ 24
6. References ............................................................................................................................................................................................................................. 26
Appendix 1 – Questions for MDT Member Interviews
Appendix 2 – Template for MDT Observation Notes
Appendix 3 – Case Studies
hertshealthevidence.org
3
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
1. Introduction
Nationally and locally, homelessness has become a growing issue, and many homeless applicants self-report having additional support needs. Between April
and December 2018, over 3,000 homeless approaches were made in Hertfordshire, of whom a third had self-reported needs. The Strategy establishes priorities
and principles for collaborative working to address homelessness and the support needs presented by this group. These principles were tested in a pilot in the
Broxbourne District. Broxbourne had the highest percentage of homeless applicants with support needs (70%). The pilot was designed to provide fair
access to people with multiple needs through a single point of access; enabling long-term housing and support solutions for all clients
presenting as homeless. Through increasing capacity to enable co-location of support services, and by designing and implementing a
Common Needs Assessment, the pilot sought to;
• Prevent escalation of care, health and support needs
• Reduce burden on statutory services (NHS, criminal justice, housing, social care etc)
• Prevent people from falling out of the system
• Get people to the right services quickly
• Reduce repeat homelessness
Due to Covid-19, and the immediate need to provide accommodation to homeless people under the Government’s ‘Everyone in’ initiative, the Broxbourne
pilot was stalled. However, a multi-agency model of support was developed locally, known as the Rough Sleeper Multi-Disciplinary Team (RS MDT). The
RS MDT held regular case conference meetings (attended by statutory services and Change, Grow, Live (CGL)) to focus on the priority cases identified by an
initial rough sleeper tracker. This ensured priority individuals were offered an assessment of need and/or the necessary referral into the appropriate agency
for housing and support.
The following report explores the benefits and challenges arising from the RS MDT model and considers its value as tried and tested way of working. The
report and the arising recommendations will help support the continued development of existing RS MDTs and will inform the future commissioning model
for Housing Related Support (HRS) provision.
1.1 Objectives of the evaluation
• To explore whether multi-agency working has saved time and resource (or might in the future) compared to pre-COVID models of working.
• To explore whether multi-agency working has provided more timely and personalised outcomes for individuals compared to pre-COVID models of
working.
• To explore why some but not all agencies/partners/services have bought into the multi-agency model.
hertshealthevidence.org
4
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• To explore why the multi-agency model has been successfully implemented in some but not all districts.
• To explore what went well during set up and implementation of the new support model and what could be improved going forward.
1.2 Definitions
Complex needs: An individual with two or more needs affecting their physical, mental, social or financial wellbeing. This could include, but is not limited to;
mental health issues, substance misuse, domestic abuse, homelessness, physical ill health, learning or physical disability.
Multi-Disciplinary Team (MDT): A group of people bound by a common purpose who meet regularly to communicate, collaborate and consolidate
knowledge from which plans are made, actions determined, and future decisions influenced. Each team member has an area of expertise and should be
capable of making autonomous decisions. In this case, the RS MDT common purpose was to discuss the unmet support needs of priority homeless individuals
and decide how these needs will be met and coordinated through existing service provision.
HCC Complex Needs Team: Partnership between Pubic Health and Adult Care Services.
1.3 Background
Housing related support services were originally established under the Supporting People Programme, which disbanded in 2009. See Strategy for further
information. Over the last decade, Housing Related Support (HRS) services have since developed organically across Hertfordshire. The service provision
accommodates and supports a homelessness cohort with a range of needs such as mental and physical health problems, drug and alcohol dependencies, and
domestic abuse experience. Referrals and assessments can originate from hospitals, police, prisons, local District/Borough housing departments or community
mental health services. However, the pathways into HRS services can be disjointed, with little multi-agency working. While there are several community services
in place to meet specific support needs, we know that such issues often combine and exacerbate each other, and there is a cohort of people with complex needs
who do not necessarily fit into one specific service. These individuals can find themselves failing to meet requirements of statutory services and falling through
the support net as a result. Evidence indicates that for these individuals, appropriate long-term accommodation alone will not achieve positive outcomes (Public
Health England, 2018), and that professional support is vital in enabling them to sustain the accommodation.
In an effort to begin addressing this, in 2019, Hertfordshire Adult Care Services produced a high-level Complex Needs Strategy (HCC, 2020), The strategy
focused on the following strategic priorities;
• Preventing and reducing care and support needs (Adult Care Services 15 Year Plan)
• Preventing Homelessness and reducing Rough Sleeping (including families)
hertshealthevidence.org
5
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• Connected Lives – helping to support people to remain in their homes and connected to communities
• Improving health and wellbeing and preventing ill health (due to homelessness)
1.4 Local and National Picture
The rate (crude per 1,000 households) of statutory homelessness in Hertfordshire saw an increase from 1.8 in 2013/14 to 2.7 in 2017/18. The England average
saw a similar statistically significant increase over the same time period.
The Ministry of Housing and Communities and Local Government (MHCLG) report that between April and December 2018, in Hertfordshire over 3,000
homelessness approaches were made, and of these, over one third had self-reported support needs.
1.5 Commissioning and Procurement
A comprehensive procurement programme is timetabled for 2021 with the aim of launching new housing related support services in April 2022 (subject to
COVID)
A review of current housing related support services is underway to gain a clear understanding of current provision. It will be the County Council’s role to:
• Provide a strategic overview of homelessness and HRS needs
• Commission HRS services for adults with complex needs, adopting an evidence-based approach
• Work in partnership with agencies to re-design service models
• Influence partners to work with us on the Complex Needs agenda
• Pilot and evaluate new ways of working.
1.6 ‘Everyone In’
In March 2020 Dame Louise Casey spearheaded the Government’s response to homelessness during the COVID -19 Pandemic. The ‘Everyone In’ initiative was
developed with the aim of getting all rough sleepers and those with shared air space a safe harbour to live in order to protect and prevent the spread of the
virus. This paved the way for Hertfordshire to test out the principles of the Strategy, as well as the principles of the original Broxbourne pilot. A tracker for
reporting on all rough sleepers who were placed in temporary accommodation across the 10 Districts was developed, alongside an MDT approach for addressing
the needs of priority cases. Rough Sleeper MDT’s (RS MDTs) were formalised across each of the 10 Districts with statutory mental health, drug and alcohol
hertshealthevidence.org
6
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
providers and probation in order to discuss priority rough sleepers identifying as having unmet support needs The use of the tracker along with observations
and outcomes from the MDT’s and interviews with MDT members form the basis of this evaluation.
2. Description of the Intervention
2.1 Identification of priority cases
In May/June 2020, each District Housing Options Team was asked to complete an initial RS Tracker, supplying detailed support needs information for all clients
housed as part of the Everyone In Programme. The HCC Complex Needs Team used this data to identify priority cases based on:
• Being recorded as having support needs (mental health, substance misuse, offending, safeguarding, no recourse to public funds (NRPF)) and not
currently receiving support from the relevant agency.
• Clinically Extremely Vulnerable (COVID Definition) and not currently receiving support from the relevant agency.
• Those who have been evicted and not currently receiving support from the relevant agency.
• At risk of rough sleeping due to eviction or are on a final warning from temporary accommodation and not currently receiving support from the
relevant agency.
• Those who have been assessed for move-on who have ongoing unmet support needs.
After the initial RS Tracker, further cases who would benefit from collaborative conversations and joint planning were brought to the RS MDT meetings by the
Housing Options Manager. All Care Leaver cases identified by the tracker were addressed outside of the MDT.
2.2 RS MDT meeting protocol
RS MDT meetings were organised by the Housing Options Managers in each District. Initially these were a one-off meeting to address the support needs of
the priority cases identified as part of ‘Everyone in’. However, 8(?) of the ten districts chose to continue with RS MDT meetings.
The following agencies were invited to attend:
• District Housing Options Managers
hertshealthevidence.org
7
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• Probation
• Hertfordshire Partnership Foundation University Trust (HPFT) (Community Mental Health Service)
• CGL (Change Grow Live) Spectrum (HCC Commissioned Drug and Alcohol service)
• Primary Health Care
A Hertfordshire Directory of Community Mental Health, Housing Related Support and Domestic Abuse services was provided to assist the RS MDT
representatives.
During MDTs, each case was discussed, and agencies pooled their knowledge to identify what further support could be of benefit, potential referral pathways,
and who should lead on each referral. The lead referrer, usually the Housing Options Team, would discuss all options with the client prior to referral.
All agencies were responsible for agreeing what a housing and support plan could look like for each case (including timeframes). For this process to be
effective, members were asked to attend RS MDT meetings prepared with information about their agency’s remit, their available capacity and how they could
co-operate with other agencies.
2.3 Consent/Data Protection
For the purposes of the tracker, a privacy statement was developed by Public Health with input and approval of the HCC Data Protection team. The notice
aligned to ‘COVID 19 Notice Under Regulation 3(4) of the Health Service (Control of Patient Information)’ which has been extended until 31st March 2021. The
privacy notice was used both for the purposes of gathering the data for the tracker and for the RS MDT meetings. Some Districts have also developed their
own privacy statements.
3. Evaluation method
3.1 Qualitative Data Collection
Fourteen semi-structured interviews were conducted by Nichola Lee, Senior Public Health Evaluation Officer (see Appendix 1 for interview questions). These
comprised the following:
hertshealthevidence.org
8
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• 8 members of District housing teams involved in the set up and chairing of the MDT meetings
• 2 HPFT colleagues who attended MDT meetings across a number of districts
• 1 probation colleague who attended MDT meetings across a number of districts
• 1 Change Grow Live (CGL) colleague who attended MDT meetings across a number of districts
• 2 Supported Housing providers (Haven and New Hope) who attended MDT meetings in the Districts in which they operate.
Seven initial RS MDT meetings and five subsequent MDT meetings were observed by members of the HCC Complex Needs Team. Detailed notes were taken
using a pre-agreed template (see Appendix 2). A focus group with members of the HCC Complex Needs Team allowed these different experiences to be
discussed, and the transcript included in the qualitative analysis. All transcripts were analysed using an inductive thematic approach. Analysis was carried out
by Nichola Lee using NVIVO 12 software.
3.2 Quantitative Data Collection
The design of the initial tracker meant that client outcome data was not captured in a reliable or valid way, making it unsuitable for use in this evaluation.
Instead, individual case studies, qualitative data and professional judgement were used to infer where the benefits might lie and the impacts of the RS MDT
model to date.
4. Results
4.1 RS MDT Output Statistics
Eight out of ten districts held an initial MDT meeting in July 2020. Of the 536 clients housed as part of Everyone in (Countywide), 81 were discussed at initial
MDT meetings (15%). The average number of cases discussed per initial MDT was ten.
Six out of the eight districts have subsequently held regular RS MDT meetings; differing in cadence between fortnightly and six-weekly.
4.2 RS MDT Meeting Observations
Table 1 describes the features of successful MDT meetings, along with the challenges experienced by the various agencies involved.
hertshealthevidence.org
9
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Table 1: Features of successful Rough Sleeper MDT meetings, challenges encountered and recommendations to overcome them.
Features of successful RS MDT meetings Challenges Recommendations Toolkit content
Good representation: The following agencies in • Maintaining engagement in the long • Develop a Rough Sleeper Tracker Tracker (excel)
attendance (as a minimum): term. to record service user outcomes development
• Hertfordshire Partnership Foundation Trust • Capacity to attend MDT meetings over time
(HPFT) • Some agencies having to leave • Circulate service user outcome Terms of
• Change, Grow, Live (CGL) and Emerging Futures before the end of meeting (meetings data to ensure continued buy-in Reference
• Housing (District team) not prioritised in diaries) from agencies template
• Probation • Frequency of MDT (for those areas • Well organised meetings mean
• Primary Health Care that have continued) is different attendance is more likely
• Adult Care Services (ACS) Social Workers from from one District to the next, • Develop toolkit; including Terms of
the following teams: older people, physical monthly, bi-monthly etc. Reference with clearly defined
disability, learning disability • No mandate to attend roles and responsibilities of all
• Children’s Services (engagement via • Statutory services sometimes do not agencies involved
Hertfordshire Protocol) perceive cases within their scope (do • Recommissioning opportunity:
• Supported Housing Providers not meet threshold for engagement) Build capacity into contracts to
• Consistent representation from each enable consistent representation
Consistent person representing each agency. agency – hand over needed if not at MDTs.
Well-planned and executed meetings. • Some agencies need to leave before • Standardise the way in which Create document
Include the following features: the end of meetings so miss meetings are run; Create ‘How to run an
• Run by District Housing Teams with one person inputting into new case discussions document ‘How to run an effective Housing
chairing and one person making notes/action (if new cases are held until the end). effective Housing MDT Meeting’ MDT Meeting’
tracking. • Discussions can be less fluid via • Dedicated admin resource (to be
• Dates for future meetings circulated well in remote platform (vs face to face). found within existing capacity).
advance (as a regular diary slot). • Admin support is needed. • Single point of contact for each
• Details of new cases circulated at least 3 days • Large initial workload for District agency.
prior to meetings (including Date of Birth) to housing Teams (reduces over time,
allow all agencies to look up cases and and time saved in chasing agencies
effectively contribute to discussions. for input into cases).
hertshealthevidence.org
10
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• Agencies who cannot attend in person to
provide a written update/summary on each
case (existing and new).
• Each agency asked to update on each client
before a general discussion about how best to
help them takes place.
• New cases discussed first (before existing
cases).
• Well run meetings; keep to time.
• Conducted via online video-calling facility
enables better attendance.
• Optimal meeting length 1.5 hours.
Action Tracking: • Time commitment needed to chase • Dedicated admin resource (to be Tracker (excel)
• Detailed notes on actions required after each actions from multiple agencies. found within existing capacity). development
meeting. • Updates needing to be chased when • Agreement that representative is
• Dedicated resource in District Housing team to agencies can’t attend the next the single point of contact for Terms of
follow up on actions. meeting. actions. Reference
• Realistic time frames for actions are discussed. • Admin support needed. • Agree ownership of actions. template
• Agencies carry out actions before next meeting.
Recording of SU Outcomes: • Data capture (to demonstrate Creation of Data Task Force (to include Set up Data Task
• Allow the effectiveness of MDTs to be impact) is not standardised across membership from five Districts, Public Force.
monitored. districts. Health and Adult Care Services) to
• Provides a morale boost for members. • No clear picture of what, how and examine; Tracker (Excel)
• Ensures continuing buy-in if outcomes are where data around support needs a) What data is needed to inform development.
positive and encourages innovation if not. for this cohort is collected. commissioning and evaluation (for
• Need to identify issues/gaps within short and long-term outcomes)
the current system. b) What data is currently collected
• Low sensitivity of current data that could meet these outcomes
collected e.g. housed/not housed. c) Any duplication that exists
• No standardised data collected on d) Design of any additional data
the level to which individual support collection methods as required.
needs are being met in this cohort. (E.g. capture a more
hertshealthevidence.org
11
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
comprehensive understanding of
the level of support need of
complex cases/all Rough sleepers).
To include gaining a greater understanding
of H:Clic, District case management system
capabilities, and MHCLG mandatory data
requirements.
Data Sharing: • Info sharing/data protection issues • Voluntary sector/non-statutory Data Sharing
• Agreement in place so non-statutory agencies service involvement to prevent Agreement
(e.g. MIND) can join meetings. escalation of care and support template
needs.
Case identification and throughput: • ‘Everyone in’ meant that all rough • Capture the support needs (and Tracker (excel)
• Cases identified by defined criteria e.g. Those sleeper cases were known to the engagement with services) of all development.
who identified as having support needs but Districts. The top 10 (as per criteria rough sleepers in the tracker (to be
were not receiving any support and/or clinically outlined to the left) were prioritised developed as part of the Data Task Develop criteria
vulnerable and/or had left their for the first discussion but many Force – see above). (and decision-
accommodation and/or had received final cases are still outstanding and won’t tree diagram) for
eviction warning and/or required additional be presented to MDTs. presenting and
support to maintain temporary • Unclear ‘threshold’ for cases being pausing cases
accommodation. presented at MDTs. discussed at
• Cases are presented/identified by all agencies. • Data on the support needs for these MDTs
• At each MDT meeting; cases aren’t currently captured or
o Information is updated for existing may be being captured elsewhere
cases/further discussion on barriers but this is unknown, as well as the
o Approx. 5 new cases are discussed. level of consistency of the data
• Cases where a positive outcome is achieved, or capture across all Districts.
natural pause occurs are removed from ‘open’ • Constant changing nature of support
case list to ensure a good throughput of cases. needs as people progress/or
• Defined criteria for pausing/removing a case disengage from support services.
from MDT discussions.
hertshealthevidence.org
12
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Attitude and Engagement: • New way of working. • Case studies and examples of good Top tips sheet:
• Problem-solving attitude of all members. • No consistency re. attendees practice to be shared with senior Ideas for
• An atmosphere where creativity is encouraged, updating their service’s own case managers. engaging
and members are resolved to find new management systems on newly • Set up a community of practice entrenched
solutions. identified risks (if service user is where members of MDTs across Rough Sleepers
• Discussion around overcoming barriers that are known to service). the County can meet and share with support
individual to each client. good practice and ideas for services.
engaging entrenched rough
sleepers. Set up a
Community of
• Recommissioning opportunity: practice; owned
New contracts to state need to and developed
update case management systems by members of
accordingly from any info gathered MDTs.
from MDTs.
Pointers around
updating case
management
systems for
agencies (good
practice)
Case Study
Template
New referral opportunities identified and acted upon: • Too early to tell whether service • Ensure provision available to take Updated
• All agencies able to identify when and where to users will engage or whether up new referrals – investment Directory of
appropriately refer each service user after referrals will have positive required in mental health and Services.
gaining a greater understanding of service user outcomes. drug & alcohol services to meet
history and current situation. • Pathways for referral are often need across the County (including
unclear. dual diagnosis workers).
• Practitioner present must be able to • Undertake a pathway mapping
correctly identify links between and identification exercise to
support needs – individual must be highlight gaps in provision.
viewed in a holistic way.
hertshealthevidence.org
13
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
• Low level mental health needs are • Develop and embed a common
identified as a support need in all assessment framework for adults
cases. with complex needs facing
homelessness. To be used at the
first point of contact with any
service, regardless of discipline.
• Recommend use of service
directory that was sent to
accompany the MDT’s.
4.3 Key Themes
For each benefit (defined through qualitative data analysis), a summary of the mechanisms and contexts (how the MDT model is expected to work and in what
circumstances) are detailed below.
The Impact of the Pandemic on the MDT approach
The biggest challenge overcome by statutory services was the amount of staff in isolation throughout the pandemic. This meant that attending the MDT
meetings could not be prioritised in some Districts and coverage was patchy. For this reason, the move to remote working and virtual meetings meant better
attendance:
‘My attendance at these kind of meetings has gone up because of it being remote. I would never have thought of having my face on the screen 24/7, but now its
common practice and means you can multi task in a way you couldn’t before.’ HPFT Practitioner 1.
Agencies felt that the pandemic improved cohesive working practices (‘The forum was always there but there was less impetus from other members to come
together cohesively.’ HPFT Practitioner 2. ‘There has been more of an appetite to have a discussion about supporting people post-COVID.’ Probation rep 1) and
stripped back bureaucracy (‘One thing that’s refreshing is that our services have stripped back levels of bureaucracy in order to deliver a service during the
pandemic; we have been able to react to the need when we went into crisis delivery. We developed services that would usually take 12-18 months to develop.’
HPFT Practitioner 1).
There was a sense of increased creativity during discussions about hard to reach service users:
hertshealthevidence.org
14
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
‘People been given funding and have been creative with that. Where they would have had a strict stance on how they manage rough sleepers before, they have
broken down barriers, got them into hotels. There has been a lot more creativity about how we support people, we can’t lose this creativity now it’s been there and
we can’t and unlearn things.’ HPFT Practitioner 2.
‘The creativity side is where we’ve really shone. Not just the organisation of it, but the group itself and having the forum to be able to discuss this freely without
prejudice.’ HPFT Practitioner 1.
Due to Everyone In, all rough sleeper cases were known to the District at the same time, meaning the true level of need in the local population could be
assessed.
‘Previously these people would have been street homeless, but because of COVID they’re placed in hotels and other resources in the community, so the platform
was different to how it was. So an outcome of COVID, was that homeless people were given somewhere to live during that period. Because of that now, housing
and services are able to work jointly to get them housing but previously we didn’t know where they were.’ Housing Options Manager 6.
‘Now they (rough sleepers) are a captive audience, everyone is stripped off the streets, they’re not going about their business as per usual, we know these people
much more, there is more ability to be creative in the way we’re implementing things.’ HPFT Practitioner 1.
‘They moved from one place to the next and it was difficult to maintain contact with them. It’s easier to wrap the services around the people because they are
already in some kind of temporary accommodation.’ Housing Options Manager 4.
‘High need people came together, and because of that it featured more significantly on people’s radar than it would have when it was diluted over months and
months.’ Strategic Lead, District Housing Team.
hertshealthevidence.org
15
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
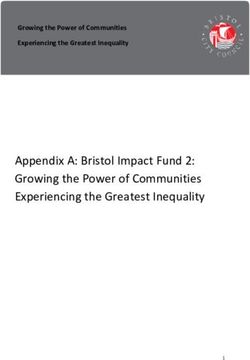
Benefits of the MDT model for Clients
Figure 1: Potential Benefits of the RS MDT Model for Clients.
District Housing Options Managers felt it was ‘easier to achieve positive outcomes for the clients’ through having a group of professionals focussed on the client
need. This enables early intervention so that the service user can engage with the ‘right’ service at the ‘right’ time.
‘There is an acknowledgement of the bigger picture. Everyone was there and everyone contributed with information. I would suggest that there is a more
coordinated response around individuals now.’ Housing Options Manager 1.
Improved information sharing and collaborative working enabled bespoke packages to be created around clients to enable them to maintain tenancies.
Dedicated support will strengthen trust between the worker and the service user to make a more meaningful intervention; supporting personal choice and
empowerment. Agencies stated that being placed in a suitable supported accommodation will prevent the service user ‘falling out’ of the system and facing a
‘revolving’ door scenario. See Appendix 3 for five summary case studies of clients whose outcomes were improved through discussion at the RS MDT
meetings. One of these included a case which was granted discretionary access to housing register using information from partners.
hertshealthevidence.org
16
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
‘We are making huge progress with some people that we've really struggled with over a long period of time so definitely it is working and the MDT is having a
positive impact even on those cases. Two cases in particular had been long-time chaotic, difficult to engage not sustaining accommodation and they are both
doing really well.’ Housing Options Manager 2.
RS MDT members felt that early intervention had helped prevent needs escalation in a number of cases. However as client outcome data (and engagement
with support services) was not collected as standard before the MDT model was introduced, the benefits outlined in this report are based on professional
judgement. See Recommendations section for details of how outcome data is being collected going forward.
‘Prevention is always better than cure; being able to start in start in early stages before they become a chronic problem is always better. People on the streets in
need of support and advice on meds, will always do better if they’re in an environment where we can reach them to deliver.’ HPFT Practitioner 1.
‘You’ve got nothing to compare it to because nothing was gathered before (in terms of collecting outcome data).’ HPFT Practitioner 2.
One limitation of the original method of case identification was that despite working initially as a way of finding out who the priority cases were, by the time
the initial MDT meetings occurred, some clients had moved on, been lost or were no longer a priority. This feedback enabled the development of the new
Rough Sleeper Tracker, which is a live document, updated at each MDT meeting (See section 5.3 The Importance of Data).
hertshealthevidence.org
17
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
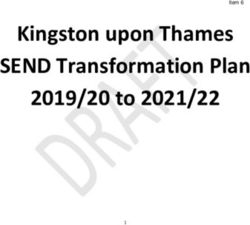
Benefits of the RS MDT model for Agencies
Figure 2: Benefits of the RS MDT model for Agencies.
The most commonly cited benefit for agencies was the time saved from chasing information for individual clients by attending these meetings. Previously, the
individual worker (from each agency) assigned to each client would need to be tracked down and then chased/followed up. Using this new model allowed all
known information to be shared about high priority/complex cases in one meeting, thus freeing up time previously spent chasing information. Contacts made
at these meetings were then used between meetings to quickly gain updates on cases or discuss other cases not meeting the threshold for discussion at an
MDT. It was universally felt that creating this multi-agency framework is necessary for supporting service users with multifaceted support needs.
‘To be able to do a piece of work and chase up, I haven’t got the time to care coordinate people who are chronically ill in the community. I haven’t got enough
time to ring 15 agencies to get that info that I would get in this 10-minute conversation about someone. That’s why it works.’ HPFT Practitioner 2.
hertshealthevidence.org
18
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
‘Pre-COVID it was done on an individual basis; you would have individual housing homeless officers dealing with this. I might have six people who were homeless
in my service and the staff could have been dealing with 6 different members of the housing team. There was no real oversight on the six. If you wanted feedback
of info on those homeless people, you would be phoning everyone to get the info’. HPFT Practitioner 1.
‘The key now is whether that can progress forward, time will tell. I do think as the homeless lead, I’m making links with people who I didn’t know existed. I have
networked and had conversations and I think it is really good. Even though sometimes I sit there and listen, I’m still getting involved, attending, I’m hoping to build
links that will help us’. Probation rep 1.
‘We’re got more time, we’re not chasing housing and likewise for housing, they’re not chasing us for info as well. We’ve got info readily available following the
meeting so staff (meaning individual social workers, nurses, consultants) have more time to do other things rather than chasing a housing officer in relation to a
housing application, so its time and also obviously communication is 100% better’. HPFT practitioner 2.
All agencies reported improvements in communication regarding clients. Agencies are now aware of each other’s remit and thresholds for referrals are
understood. Appropriate pathways were discussed based on a client’s history and information gleaned from the multi-agency discussions.
‘It’s opened our eyes to the more services that are out there to get them involved with clients. It made options officers aware of referrals they should be making’.
Housing Options Manager 2.
‘I'd say it's been really helpful for the staff on the ground who are dealing with the clients on a one to one daily basis in order to understand what is out there for
them, what they need to do in order to access that service and to support them in the right way to access that service’. Housing Options Manager 3.
‘I think one positive is that I’ve learnt more about what’s out there in terms of services than I knew pre-COVID. I’ve never spoken to anyone from CGL or Emerging
Futures before’. Strategic Lead, District Housing Team.
‘It’s gone very well in terms of communications. Comms have improved. I’m regularly getting calls from the housing teams about individual cases. Likewise, I’m
able to contact them directly with concerns about cases. Quick responses and problem solving together has improved dramatically’. HPFT practitioner 1.
‘I think there's certain services that are involved in the MDT that we perhaps really struggled to get communication open between ourselves and them that's been
really helpful’. Housing Options Manager 3.
hertshealthevidence.org
19
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Some housing options managers stated that setting up and running these meetings was time consuming, but felt it was a worthwhile investment of their time.
It was felt that admin support was a valuable resource to enable the smooth implementation of the MDT meetings (see MDT observations section). Other
agencies discussed the pressures on their time to attend regular meetings but felt that the attendance at these meetings was a good use of their time.
‘You could argue that this is an investment of the Housing Options Manager’s time. It is worthwhile as she has all the right people in the room at the same time.
She gets the facts and the situation in a more efficient way than in dribs and drabs’. Strategic Lead, District Housing Team.
‘The only consequence is we’re all slightly busier but busy doing meaningful things. I’d rather go to these meetings than other meetings where not a lot has been
achieved. I think it’s a positive thing’. Probation rep 1.
Agencies reported an improvement in the management of expectations for whom their service can help. Signposting played a big role in some MDT meetings
with referrals being triaged at this early stage. This enabled only relevant referrals to be received by the statutory services. A greater understanding of each
agency’s role in supporting service users managed expectations of what could be achieved by each agency and which referrals were relevant.
‘It gives me the ability to give information if we’ve seen the client and they’re not for us and be clear what our expectations are. It manages expectations of us’.
HPFT practitioner 1.
‘Triaging at the beginning, ensures we get relevant referrals further down the line’. HPFT practitioner 2.
Agencies felt that decisions about appropriate referrals and actions could be made quickly, as a person at the right level of management was present at the
meetings.
‘My role is very busy, I need to give it priority because the people who are there are the people who can make decisions’. Probation rep 1.
‘The point in sending someone of that level is that decisions can be made. It’s not someone on the frontline who then has to get plans agreed. If I say it will happen
it will happen. It’s pitched at right level of attendance. For me it means if I attend and I say the team will do something, I’ve made that decision and it won’t be
overridden. If you’re asking us to be creative, it’s about being creative and not following normal rules’. HPFT practitioner 1.
Agencies felt that there would be savings to the system from using this model. This would be achieved through the joint commitment to housing shown by all
agencies involved.
hertshealthevidence.org
20
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
‘17 of 85 names on the original tracker (20%) have said they have got repeated homelessness. Even if we can resettle half of those, they won’t be coming back in
2-3 years and that’s got to benefit the state and the publicly funded services who pick up the pieces.’ Housing Options Manager 5.
‘The MDT brings joint commitment to find a solution. Other agencies don’t have accommodation duties, but they benefit if accommodation is found, in a settled
nature. Probation will benefit, there will be less offending. CGL can help on their journey once they are accommodated. There is a real shared commitment to the
housing side even though they don’t have strict housing responsibilities. They are helpful in getting these people settled’. Housing Options Officer 4.
Data from the original MDT tracker allowed gaps in current housing related support service provision to be identified. This data fed into each District’s bid for
Next Steps Accommodation Programme (NSAP) funding. Ongoing Rough Sleeper Tracker data will enable evidence-based commissioning decisions to be
made and ensure resource is effectively targeted where the need is identified.
‘It’s identified the gap we have in our local services accommodation wise.’ Strategic Lead, District Housing Team.
4.4 Limitations of the Evaluation Methodology
The benefits outlined above were described from qualitative data analysis only due to the lack of time and resource available to design and implement the
required data quantitative capture mechanisms. This has led to the parallel development of the RS tracker (see recommendations) allowing the outcomes for
service users housed during lockdowns two and three to be assessed.
Due to scope of the evaluation and COVID pressures, as well as the resource and time available, service user interviews and case audits were not possible.
These valuable data collection methods will be within the scope of the proposed Countywide pilot evaluation (see Recommendations section).
5. Recommendations
5.1 A Countywide pilot
This evaluation has highlighted four areas for further development within the current model;
a) HPFT and CGL Practitioners are unable to support the preventative element due to the high level of demand for their services
b) Lack of a standardised approach to capturing client need at the first point of contact (with any service)
hertshealthevidence.org
21
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
c) Lack of robust data collection and analysis to support needs assessment, evaluation and commissioning decisions across all homeless groups (not only
rough sleepers)
d) Housing related support services monitoring framework provides limited understanding of service user outcomes
Therefore, a Countywide Pilot has been designed to address the need for investment in these areas. See Figure 3 for the pilot Theory of Change model.
In addition, a Strength-Based Practice model (working in a psychologically informed environment) will also be piloted in selected areas to enable the
development of innovative ways to commission and monitor service user outcomes as well as contract manage going forward. Strength-based models will be
used in conjunction with fully functioning MDT’s (in selected areas) enabling a comparison of this model and standard practice.
A further aim of the pilot is to address whether the extra investment outlined in Figure 3 could mitigate the risks of short-term MHCLG Rough Sleeper funding
coming to an end and therefore creating sustainable pathways.
The pilot will provide the opportunity to commission future services based on current need (identified through effective data collection and analysis) and
evidence of how service-user outcomes are influenced under different circumstances.
hertshealthevidence.org
22
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Figure 3: Anticipated benefits of the Countywide pilot (Theory of Change Model).
5.2 Common Needs Assessment Framework Creation (part of the Countywide pilot)
The results of this evaluation indicate that agencies believe a whole systems approach is broadly beneficial when addressing the complex needs of rough
sleepers. One part of achieving a holistic approach is through the development of the ‘No Wrong Door’ philosophy. This would involve co-creating a common
needs assessment framework as part of the Countywide Pilot. The assessment form will be completed by the first point of contact a resident has with any
service, regardless of discipline. It will cover all potential aspects of support required; ensuring residents get on the right pathway for help much earlier which
will facilitate early intervention and preventing needs escalation.
‘Developing a common assessment tool, where agencies trust the housing officers to gather appropriate information, is the Gold Standard in this field’. I feel we
have the buy-in and foundations to make this approach work in Hertfordshire.’ Housing Options Manager 3.
hertshealthevidence.org
23
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
5.3 The Importance of Data
A major finding from this evaluation is the importance of data to:
• Capture the level of unmet support needs in this population
• Capture outcomes over time
• Monitor outcomes and needs for those with protected characteristics
• Ensure effective targeting of resources
• Inform commissioning and MHCLG funding decisions.
• Enable effective running of MDT Case Conferences (including the prioritisation of cases for discussion)
Therefore, a Complex Needs Data Focus Group will examine the source, purpose and the value of data collected by the 10 Districts, Adult Care and Public
Health. It aims to standardise data collection where possible and avoid duplication. The group’s objective is to create an evidence base for housing related
support needs across the County, which will inform future commissioning decisions. This includes defining the role and scope of the RS Tracker developed as
part of the RS MDT Toolkit for Practitioners (see Toolkit section below).
Group membership will include membership from five District Housing Teams, Public Health and Adult Social Care – all acting as Complex needs data
champions.
5.4 Sharing of Good Practice
Members of the RS MDTs expressed a desire to set up a RS MDT Community of Practice (CoP). This will provide a forum for members to come together to
discuss challenges they’re facing, to problem-solve and to share best practice. The CoP will be developed and owned by members of the RS MDTs and will
become a valuable feedback mechanism for further development of the Countywide model.
5.5 Development of the Rough Sleeper MDT Toolkit for Practitioners
The main recommendation from the MDT Observations was the need to develop a toolkit for practitioners. This will be created using a combination of
observations from successful MDT Case Conferences, solutions from MDT practitioners to overcome challenges, and from conversations/interviews with
Housing Options Managers. The toolkit will describe how to set up and run effective MDT Case Conferences now (Phase 1), and as Phase 2 begins to roll out
this toolkit will continue to be updated. Please see Figure 4 for an overview of what Phases 1 and 2 will entail.
hertshealthevidence.org
24
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
Figure 4: Phased approach to the
delivery of the Evaluation
recommendations.
hertshealthevidence.org
25
PH.Intelligence@hertfordshire.gov.ukRough Sleeper Multi-Disciplinary Team Model – Evaluation Report February 2021
6. References
Public Health England, 2018. Evidence review: Adults with complex needs (with a particular focus on street begging and street sleeping).
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/680010/evidence_review_adults_with_complex_needs.pdf
Hertfordshire County Council, 2019. Supporting Adults with Complex Needs Strategy.
https://www.hertfordshire.gov.uk/media-library/documents/about-the-council/data-and-information/hertfordshire-supporting-adults-with-complex-needs-
strategy.pdf
hertshealthevidence.org
26
PH.Intelligence@hertfordshire.gov.ukYou can also read