The POPPY Study: Developing a Model of Family-Centred Care for Neonatal Units
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
The POPPY Study: Developing a Model
of Family-Centred Care for Neonatal Units
Sophie Staniszewska, DPhil, BSc (Hons), Jo Brett, BSc, MSc, MA, Maggie Redshaw, BA, PhD, C Psychol, Karen Hamilton, PhD, MSc, RSCN,
RGN, Mary Newburn, BSc, Nicola Jones, BSc, Lesley Taylor, BSc
ABSTRACT
Background: The concept of family-centred care in neonatal practice has become increasingly recog-
nised internationally. The underlying philosophy puts parents and the family at the centre of health care
and promotes “individualised, flexible care.”
Aims: To develop the first international model of family-centred care based on strong parental collab-
oration in the synthesis of robust research evidence to generate the philosophy, principles, model, and
indicators for implementation.
Methods and Synthesis: Seven key steps were followed to develop the POPPY model of care collabora-
tively with parents. Step 1 drew on the POPPY systematic review to identify effective interventions. Step 2
drew on the POPPY qualitative study to identify good parent experiences. Step 3 identified the philosophy
and principles of the POPPY model of care. Step 4 identified the key stages of the POPPY model of care.
Step 5 populated the POPPY model of care with data from steps 1 and 2. Step 6 developed the indicators
of family-centred care; and Step 7 undertook some initial testing with parents and practitioners.
Results: Seven key stages of the parents’ journey through their neonatal unit experience were identified
and formed the architecture of the POPPY model of care. These include: before admission to the unit,
admission, early days, growing and developing, transfers between units and between levels of care,
preparing for discharge, and transition to home and at home. A philosophy, a set of principles to
underpin the model, and a set of indicators to guide implementation in neonatal units were developed.
Conclusion: The POPPY model of family-centred care provides the first robust, collaboratively devel-
oped, parent-centred model, which can be implemented to deliver high quality care to parents of preterm
infants.
Implications: Implementing the POPPY model could help neonatal units to develop parent-focused
services which better meet parents’ needs for information, communication and support, key elements of
family-centred care.
KEYWORDS family-centred care, neonatal, premature, infant, parents’ experiences, evidence-based practice
Sophie Staniszewska, Senior Research Fellow, Patient and Public Involvement and Patient Experiences, Royal College of Nursing Research Institute, School of Health and Social
Studies, University of Warwick; Jo Brett, Research Fellow, Royal College of Nursing Research Institute, School of Health and Social Studies, University of Warwick; Maggie Redshaw,
Senior Research Fellow, National Perinatal Epidemiology Unit, University of Oxford; Karen Hamilton, Senior Research Associate, National Perinatal Epidemiology Unit, University of
Oxford; Mary Newburn, Head of Policy Research, National Childbirth Trust; Nicola Jones, previously Coordinator of Warwickshire Pre-Term Support Group, former NCT National
Specialist Worker on Prematurity, member of BLISS; Lesley Taylor, Breastfeeding Counsellor Tutor and Specialist Coordinator for Premature Birth, National Childbirth Trust.
The Parents of Premature Babies (POPPY) project was supported by an advisory group whose membership consisted of the following people: Dr. C. Bennett, Neonatal
Consultant, John Radcliffe Hospital NHS Trust, Oxford; Professor P. Brocklehurst (Chair), Professor of Perinatal Epidemiology and Director of the National Perinatal
Epidemiology Unit (NPEU) at the University of Oxford; Professor D. Bick, Centre for Research in Midwifery and Childbirth, Thames Valley University; Dr. J. Hawthorne,
Pychologist, The Brazelton Centre, Cambridge University Hospitals NHS Trust; Professor N. Crichton, Professor of Medical Statistics, South Bank University; Mrs. P. Goodger,
Senior Health Visitor, Oxford; Dr. G. Gyte, Research Associate, Cochrane Pregnancy and Childbirth Group; Dr. M. Harvey, Senior Lecturer, Birmingham City University; Dr.
Y. Richens, Consultant Midwife, University College of London Hospital; and C. Pimm, BLISS—the premature baby charity representative. The searches for this review were
conducted by P. Miller, Senior Information Specialist, Royal College of Physicians, London. The POPPY Project was funded by the Big Lottery.
Address correspondence to Dr. Sophie Staniszewska, RCN Research Institute, School of Health & Social Studies, University of Warwick, Coventry CV4 7AL,
sophie.staniszewska@warwick.ac.uk
Accepted 9 February 2012
Copyright ©2012 Sigma Theta Tau International
doi: 10.1111/j.1741-6787.2012.00253.x
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 243POPPY Model for Neonatal Units
INTRODUCTION A range of models of family-centred care has devel-
oped in relation to neonatal and children’s care, many
T he concept of family-centred care has advanced in re-
cent years and become recognised internationally, al-
though its implementation in children’s care and in neona-
developed in the United States (Saunders et al. 2003;
Mikkelsen & Frederiksen 2011). A key study undertaken
by Dunn et al. (2006) developed the Family-Centred Care
tology has been variable. The underlying philosophy puts
map (FCC) which identified potentially better practices
parents and the family at the centre of health care and
within an American setting and describing key stages in a
promotes “individualised, flexible care,” underpinned by
parents experience—pre-admission, golden hours, acute,
appropriate information, support, and effective commu-
growing stronger, breathing/feeding/growing, transition to
nication. Parents and their families are placed “at the
home and post-discharge. The FCC map drew on a range
centre of woman-focused, family-centred services” (Scot-
of information and evidence, professional perspectives, re-
tish Executive 2001; Department of Health 2004; NHS
search literature, and some parental input. The developers
Scotland 2005; Welsh Assembly 2005; Department of
of the FCC map acknowledge that whereas family-centred
Health 2007). The focus of family-centred care resonates
care has been implemented and investigated in the past
with many policy initiatives that promote patient-led
several decades, investigators have only recently begun to
health care and encourage health professionals to “step into
research systematically for the evidence base for practices
the parents’ shoes” and consider how parents feel when
(Dunn et al. 2006). In addition, although the FCC map
a preterm or sick infant is born. Implementing family-
included parents, the extent of their collaborative involve-
centred care includes introducing facilities and practices
ment, as defined by INVOLVE (2007) in the synthesis and
that support parents all the way through their experience in
development of the model is not entirely clear.
the neonatal unit and after discharge. Although these pol-
Despite some of the challenges in defining, conceptual-
icy initiatives provide a useful context for the implementa-
ising, and implementing family-centred care, studies have
tion of the family-centred care, and nurses seem to support
identified a range of benefits, including lower infant be-
the philosophy more generally, there is evidence to sug-
havioural stress cues, shorter lengths of stay, fewer read-
gest that health professionals can have difficulty integrat-
missions, enhanced breastfeeding (Forsythe 1998; Tessier
ing it into their own practice (Bruce et al. 2002; Petersen et
et al. 1998; Galvin et al. 2000; Van Riper et al. 2001;
al. 2004; Palladelis et al. 2005; Mikkelsen & Frederiksen
Furman et al. 2002; Feldman et al. 2003; Preyde & Ardal
2011).
2003; Byers et al. 2006; Johnson et al. 2006; Melnyk
Family-centred care has been identified as a complex
et al. 2004; Melnyk et al. 2006; Cooper et al. 2007), and
concept, which has only reached partial maturity in its de-
greater staff satisfaction, as well as a positive impact on
velopment. Family-centred care can be viewed in a num-
the stress experienced, comfort level, and parenting confi-
ber of ways (Mikkelsen & Frederiksen 2011) including as
dence among NICU parents and families (Van Riper 2001;
a paradigm (Hall 2007), a philosophy (Malinsky 2005), a
Copper et al. 2007). In addition, there is evidence that fam-
model of care (Shields et al. 2007), or as a practice theory
ily participation in infant care can lead to a better family
(Hutchfield 1999). Although family-centred care is based
experience with health care (Galvin et al. 2000; Feldman
in western culture, other studies have identified key ele-
et al. 2003). Ultimately, family-centred care may help to
ments of the concept in less developed country contexts
develop the relationship between an infant and the fam-
(Shields & Nixon 2004). There are a number of key princi-
ily and result in improved long-term outcomes for both
ples to family-centred care: including parents and families
(Feldman et al. 2003).
being treated with dignity and respect; parents having a
right to know about their infant’s care and condition and ORIGINS OF POPPY
updated information should be available to them, health-
The POPPY project (Parents of Premature Babies Project)
care providers prioritising open communication and shar-
emerged from a group of parents who felt that, while their
ing information with parents and families in ways that are
babies had received good quality clinical care, they them-
affirming and useful; information-giving being tailored ac-
selves had poor experiences of the neonatal unit. In many
cording to parents’ individual preferences for detail and
respects they felt they had received “non-family–centred
their changing needs; parents and family members being
care,” resonating with studies that have identified diffi-
encouraged to participate in their infant’s care with the
culties with properly implementing family-centred care in
aim of them developing a sense of confidence, control,
practice (Bruce et al. 2002; Petersen et al. 2004; Palladelis
and growing independence; and practical and emotional
et al. 2005; Mikkelsen & Frederiksen 2011).
support being provided continuously, throughout the care
These challenges suggested that it was important to re-
pathway (Johnson 2000).
examine family-centred care from the parent perspective.
244 Fourth Quarter 2012 r Worldviews on Evidence-Based NursingPOPPY Model for Neonatal Units
With the collaborative involvement of parents from the DATA COLLECTION AND ANALYSIS
start of POPPY, the key areas of family-centred care were
Full methods and results for the POPPY systematic re-
identified as communication, information, and support
view and the POPPY qualitative study are reported else-
(Staniszewska et al. 2007). From this base a research pro-
where (Staniszewska et al. 2007; Redshaw et al. 2010; Brett
posal emerged which focused on these three core aspects
et al. 2011). Brief methods and limitations of these stud-
of parents’ experiences. The POPPY project conceptualised
ies are described below to contextualise the POPPY model
family-centred care as a philosophy of care, with key prin-
development.
ciples and as a model of care with core components, which
can be implemented. Parents also recognised the impor-
tance of synthesising data about parental experiences with POPPY Systematic Review
research evidence from a systematic review that identified Systematic searches were undertaken for the period of Jan-
effective interventions. uary 1980–October 2009 in the following databases: Med-
line, Embase, PsychINFO, the Cochrane library, CINHAL,
Aims MIDIRS, HMIC, and HELMIS. Grey literature was sought
First, to develop the POPPY model of family-centred care, and the Neonatal Network Journal, Journal of Neonatal Nurs-
including the POPPY philosophy, principles, and indica- ing and Journal of Obstetric, Gynecologic, and Neonatal Nurs-
tors for implementation, from the synthesis of data from ing were hand searched. A non-quantitative synthesis was
the POPPY systematic review and POPPY qualitative study. conducted based on the extracted data. Seventy-two papers
Second, to work collaboratively with parents at all stages were included. The scope of this review was very broad,
to ensure the relevance, appropriateness, and acceptability and the searches were therefore developed to be inclu-
of the POPPY model of family-centred care. sive. This resulted in the search being sensitive, but not
specific. Furthermore, this systematic review included in-
tervention studies and non-intervention studies. Although
DESIGN this review identified a range of interventions that can
The study used a collaborative approach with parents in- help parents, certain groups were under-represented in
volved in developing the POPPY model of family-centred the study samples: these included minority ethnic, disad-
care at each stage. Evidence from different phases of the vantaged groups, and young parents.
study was synthesised to identify the philosophy and prin-
ciples of family-centred care and identify the key stages and POPPY Qualitative Study
components of care. The design of the study is summarised Ethical approval was sought and granted for the qualitative
in Figure 1. study through the UK National Research Ethics Service.
This study reports on data from 42 semi-structured in-
terviews with mothers and four focus groups with fathers
were conducted with mothers who have had a preterm in-
fant at 1–3 months after the infant was discharged from
the neonatal unit. Interviews and focus groups were care-
fully set up to ensure parents were appropriately supported
and could stop the discussion at any time, if they became
upset. Purposeful sampling was used to maximise variabil-
ity in the sample of mothers from seven neonatal units in
the England and Scotland. The “framework” analysis was
conducted to identify and group themes and coding, classi-
fying, and developing categories (Ritchie & Spencer 1994).
Emerging themes (or categories) were developed by draw-
ing out key themes and reviewing the inter-relationships
between these emerging themes, to build a “story” (Brett
et al. 2011). A key limitation was the difficulty experienced
in recruiting individuals from minority ethnic communi-
ties and harder to reach groups such as teenagers. The
third component of POPPY reported current policy, fa-
cilities, and practice in UK neonatal units that related to
Figure 1. Development of the POPPY model of care. parents and family-centred care (Redshaw et al. 2010).
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 245POPPY Model for Neonatal Units
SYNTHESIS AND RESULTS
The POPPY model of family-centred care was developed in
a number of key steps with collaborative parental involve-
ment embedded throughout. Although development of the
model is presented in steps, its development was iterative
and not always a linear process. Each step is described
below (see Figure 1).
Step 1: POPPY Systematic Review
Interventions that are effective in enhancing the parent ex-
perience in relation to communication, information, and
support for which there was evidence were identified, as
described above (Brett et al. 2011). The importance of a
strong evidence base for the POPPY model of care was
particularly important in light of Dunn et al.’s (2006)
recognition of the need to enhance the evidence base of
family-centred care models and practices. Parents read the
POPPY systematic review and were involved in discussions Figure 2. POPPY philosophy.
about the acceptability, relevance, and appropriateness of
the identified interventions.
Step 4: Identifying Key Stages of the POPPY Model of
Step 2: POPPY Qualitative Study Care
Interviews and focus groups with parents, as described The findings from steps 1 and 2, underpinned by the phi-
above, produced a rich and complex data set of experi- losophy and principles developed in step 3, were drawn
ences. POPPY parents read anonymised transcripts and together in discussion with parents. In this discussion it
participated in research team discussions. Where parent became apparent that there were seven key stages from the
experiences further supported interventions identified in parent perspective, which reflected their journey through
step 1 these data were added to the same themes within the the neonatal unit, underpinned by communication, infor-
emerging model. Parent experiences data that identified mation, and support (see Figure 3).
good practice, but which had not always been identified as
a tested intervention in the systematic review, were con- Step 5: Populating the POPPY Model of Care
sidered as an important form of evidence and included in Data from steps 1 and 2 were then used to populate the
the developing model (Staniszewska et al. 2010). model of care once the seven key stages were agreed. Each
of the stages of the POPPY model of care is presented below
alongside extracts of the POPPY qualitative data. Evidence
Step 3: Identifying the Philosophy and Principles of from the systematic review is included and referenced from
the POPPY Model of Care the original papers. A summary model is presented at the
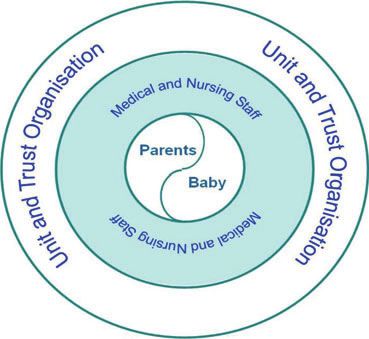
The role and identify of parents intrinsically involves pro- end of this section.
tecting and nurturing the infant, but many POPPY data Stage 1. Before admission to the neonatal unit. The
identified parent experiences were often associated with time before admission to the neonatal unit can be an im-
separation, marginalisation, lack of responsibility, and loss portant period of preparation for parents and for starting
of nurturing and protective role. The POPPY parents were to build knowledge, confidence, and understanding which
important in identifying the core philosophy: that the baby enable realistic expectations. For example, a tour of the
and parents should be at the core of family-centred care, neonatal unit, including virtual tours sometimes available
surrounded by medical and nursing staff, and then an outer on Web sites or a consultation with the neonatal team be-
layer of unit and trust organisation, expressed in Figure 2. fore admission is effective in preparing parents (Huckaby
To complement the POPPY philosophy, the principles 1999; Auckland District Health Board 2009).
underpinning the POPPY model of care were drawn from The consultant, she was absolutely brilliant in hospital, you know,
the evidence, advisory group discussion with researchers, sat down and explained what was going on, why I was going to
healthcare professionals, and parents (see Table 1). have the infant early. So everything was explained that way. . ..
246 Fourth Quarter 2012 r Worldviews on Evidence-Based NursingPOPPY Model for Neonatal Units
TABLE 1
POPPY principles
r Treat parents with dignity and respect and develop a relationship based on trust.
r Involve parents in all aspects of their infant’s care.
r Be aware of parents’ needs, the emotional impact of preterm birth and individual differences in parental responses and needs.
r Recognise critical steps for parents on the care pathway.
r Recognise and value the roles of parents, siblings and other family members.
r Provide sensitive and compassionate interaction.
r Provide practical help with infant care and parent interaction, including identification of behavioural cues.
r Provide psychosocial support for parents.
r Promote parenting skills in caring for an interacting with their infant.
r Maximise opportunities for communication with parents and parent groups.
r Support mothers’ ability to nurture their baby by expressing breast milk and breastfeeding.
r Provide appropriate family-friendly facilities.
Figure 3. POPPY model of family-centred care.
Parents suggested that this was a good time for neona- and machines bleeping, it’s a scary time and it’s good to know
tal units to record information, such as parent and family exactly what each tube was for and why.
details and telephone numbers and preferences for exam-
ple, in feeding and kangaroo care. They also proposed that Emotional support was also important for parents who
this was a good time for parents to receive practical de- did not see their infant immediately after the birth:
tails about the neonatal unit, such as contact and access That was something that could maybe have been done better, in
information and the possibility of transfer to another more that somebody could have maybe stayed with me at that point,
specialist unit. because it was midnight, it was dark anyway. . .. I was just on my
own and I didn’t actually know what had happened to the boys,
Stage 2. Admission. The second phase of the POPPY apart from the fact they were in intensive care.
model of family-centred care focuses on admission to the
neonatal unit. It may be the parent’s first visit and intro- It was important for many parents to be able to be to-
ductions to staff and collection of key information from gether and enabling both to stay overnight was valuable:
parents are important. This can be a very difficult time for I only stayed one night, and it was just because I felt totally
parents, particularly in relation to seeing their infant for horrible. They said my partner wasn’t allowed to stay.
the first time:
It’s just peace of mind really, reassurance. You have not been in Stage 3. Early days in the neonatal unit. Provid-
that situation before and seeing the infant with tubes up his nose ing appropriate orientation to the neonatal unit enabled
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 247POPPY Model for Neonatal Units
parents to familiarise themselves with the environment 1995) to enable them to develop experience and knowl-
and feel comfortable: edge of their infant’s behavioural cues (Szajnberg et al.
In intensive care it was so, you know you had so much care, with 1987; Culp et al. 1989; Hawthorne 2005). A small number
the nurses all the time, but in special care they . . . left you to deal of units also have a webcam or video link available for par-
with it a bit more which was scary to begin with, but then you ents so they can feel close to their infant, are reassured and
know, as time went on you could see what was happening and the developing parent-infant relationship is supported:
what you had to do for him as well.
So when you’re at home and you’re worried, but you don’t have
As part of orientation process parents appreciated an the courage to pick up the phone, just going on and seeing her. It
introduction to staff and to parent-friendly information would probably help with breastfeeding as well, for expressing. I
think it is a thing that they need to look at.
about the neonatal unit and its policies.
As soon as you walked in the nurse that was working came straight Opportunities for parents to participate in ward round
over to you and introduced herself . . . for the first time . . . she discussions about the infant’s progress and access to med-
went “Hi, I’m so and so and I’m caring for [name] today, this is ical notes and charts have been found to be important
what’s been happening.” So that communication was excellent, (Penticuff & Arheart 2005), as have recorded consulta-
the initial first couple of weeks.
tions, which can improve parents’ knowledge (Koh &
Studies show that parents find it helpful to understand Jarvis 1998). Parents in the POPPY study reported mixed
standardised unit policies on, for example, the promotion experiences:
of breast feeding, kangaroo care, and infant massage (Meier Information in the ward round was good, the fact that you could
et al. 1993; Elliott & Reimer 1998; White et al. 2000). An stay in for that and get to hear what all the doctors said, that was
information folder for parents to collate the different types good as well I think.
of information they may be given can be useful (Costello Parents also mentioned BabyLink (Gray et al. 2000;
et al. 1996; Gannon 2000) and unit booklets or specific Freer et al. 2005), a Web site where their infant’s notes
information leaflets can help orientate parents to the unit or progress charts can be placed for parents to access when
and make their experience more manageable: they are at home. The use of notes and diaries shared
There was a pack given to us in the early days and I can remember by staff and parents facilitates communication and like
when I was in the hospital, you know, after I sort of got over the BabyLink, enables them to feel in touch with their infant’s
initial bit feeling a bit better, I was able to go through that in my care and progress. The option to be involved when their
own time, there’s quite a good, quite a thick booklet with just all
the information about the Unit and different things and I found
infant is undergoing medical procedures was important for
that quite good because it meant that I probably wasn’t sort of some parents:
being bombarded by people telling me things and I was able to Only I didn’t know all the time what was happening and I would
pick up on, you know, because I didn’t feel that actually, it sounds sometimes go up and he would have been for a scan and I didn’t
ridiculous now, but I didn’t feel able to face the whole thing at know he was going. I understand if it’s an emergency but if it’s a
once. routine thing I would have liked to have known beforehand and I
would have taken him over myself.
During the early days in the unit parents begin to get to
know their infant and this interaction is particularly impor- Infant feeding was very important for many parents and
tant in developing this fundamental relationship and their mothers needed support and help in expressing breastmilk
parenting role. Healthcare professionals have an important and breastfeeding their infant:
role in encouraging and supporting parents to participate The nursing staff, you know, took care that because it was, at first,
in providing care for their infant, and in understanding it was hard doing the breastfeeding, trying to get her comfortable,
and responding appropriately to their infant’s cues (Meyer but they were always there, they were supporting her, they were
et al. 1994; Ali et al. 2003; Browne & Talmi 2005; showing us.
Karesen et al. 2006; Melnyk et al. 2006). This did not Stage 4. Growing and developing. Parents are likely
always happen for parents in the POPPY study: to spend significant amounts of time in the neonatal unit
I kept thinking everywhere I was walking there was skin to skin as their infant grows and develops and direct involvement
posters and there was leaflets but these . . . they weren’t wanting in their infant’s care is increasingly important during this
me to take him out and I thought but I want to hold him and take phase. Parents need to be supported to continue the pro-
him out, that’s what he needs, he doesn’t . . . you know he’s just
lying in there and I want to hold him.
cess of building the relationship with their infant and de-
veloping skills of monitoring, understanding and respond-
Parents can also be supported by the use of infant be- ing to their infant’s cues, learning as these change over
havioural assessment instruments such as the Brazelton time, and about the ways in which their baby is devel-
Neurobehavioral Assessment Scale (Brazelton & Nugent oping. Staff members have a vital role in supporting this
248 Fourth Quarter 2012 r Worldviews on Evidence-Based NursingPOPPY Model for Neonatal Units
process and enabling parents to gradually increase their Stage 6. Preparing for discharge and the transition to
caring responsibilities: home. Preparation for discharge and a satisfactory tran-
It takes a lot to sort of figure out the routines of SCBU and I think sition to home, with which parents feel comfortable and
once you get to that point the nurses were quite good at explaining during which babies are cared for appropriately, is a vi-
[name’s] care to us, sort of initiating us to how to do it ourselves tal part of the parental experience (Costello & Chapman
and things like that. I think that was quite helpful, we could learn 1998; Ortenstrand et al. 2001; Bennett & Sheridan 2005;
to take a part in his care.
Broedsgaard & Wagner 2005). It is important for the
Support schemes for parents or peer group support can neonatal team to collaborate with parents is setting a target
be effective and have psychosocial and well-being benefits, date for discharge and to provide clear, consistent infor-
as well as information sharing (Roman et al. 1995; Hurst mation about the discharge process:
2006; Bracht et al. 1998; Pearson & Andersen 2001; Preyde My partner was constantly booking days off work to come and get
& Ardal 2003; Buarque et al. 2006). Parents in the POPPY us and the doctor would turn up and say “Oh no, he is not going
home today” . . . so his paternity leave was wasted, probably 7 or
study reported that they benefited from being able to talk 8 days was wasted.
to other parents in the same situation and valued these
interactions:
It is also important to develop detailed care plans with
A lot of the stuff we got from like talking through with parents, additional information for parents to refer to at home:
especially things like . . . like certain ways babies behave with them
being premature, like certain phases they did, certain . . . we’d be All of a sudden it was oh you are going home . . . we didn’t really
talking about them because I can remember the one time saying know what we were doing, where we were doing it or what we
the infant keeps crossing his eyes over and you’d mention that to should be doing, it was very strange.
a few nurses and nobody said anything and then it was talking to
other mums and dads that they’d say ‘Oh yeah he does that’ and Parents intimated that the option of overnight stays with
I’ve been told that such and such and then that puts your mind at
the infant for one or both parents was an important element
rest.
in the transition to home. Having complete responsibility
Peer support was particularly important for parents who for the care of their infant before leaving the unit boosts
did not have support from extended family or friends in parenting confidence:
the local area: Once I was transferred across to [transitional care] I was a lot
happier because as I say, the girls were with me and I could see
It’s awful going through having a premature infant and all the
you know, what was happening and I was caring for them so it was
rest of it anyway but the fact that you’ve got no family, friends,
more, it was easier for me to cope because that’s what I expected.
not even any of your clothes, all of that makes it a hundred times
worse.
Stage 7. At home. The transition home is often diffi-
Stage 5. Transfers between different levels and different cult for parents, most of who continue to need support and
units. Transfers between different levels of care within information during this new phase where responsibility for
one hospital or to another hospital can be a difficult time the care of their infant has become theirs entirely:
for parents, particularly when they have become familiar
Yeah you are a bit abandoned because you’ve asked that many
with a particular neonatal unit. Preparation of parents for questions in there every day and you’ve had people looking after
transfers to other units was critical to those in the POPPY him every day, doing his temperature.
study, principally in relation to unit introduction and ori-
entation, policies and practices and provision of continuing Studies have shown how home support programmes
emotional support: reduce maternal stress and improve mother–infant inter-
Nobody actually sat down and said well this is the difference in action (Barrera et al. 1986; Resnick et al. 1988; Spiker
special care, this is what will happen in here compared to there et al. 1993; Klebanov et al. 2001). The importance of conti-
. . . and basically you just felt you were left to get on with it. nuity of care means that parents value visits from outreach
He was born . . . went into special care here and that was fine so
or unit-home liaison neonatal nurses (Langley 1999) and
they took us round the special care here, we met everybody that POPPY parents appreciated any contact with the neona-
nursed him and that was fine, you know I was completely settled tal unit or with a nurse with specialist knowledge and
then that we were going there. So it was a bit of a shock then expertise:
on the Friday to be told you’re going on a plane and it’s going
to be today and then they came back and said . . . a few minutes I think the support on discharge is really good. I do. I think having
later they said “it’ll be lunch time” which this was about 10:15 by the community liaison nurse is invaluable.
this time, I was like. . . I’ve got to go home, pack a bag and go to
[place], it was . . . that was a bit of a shock. After care, I’d say for the first week you feel really alone.
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 249POPPY Model for Neonatal Units
Planned
Unplanned
Figure 4. POPPY model of family-centred care.
Peer parental support and access to neonatal unit sup- Step 6: Identifying Indicators of Family-Centred Care
port groups or community groups was also identified as Drawing on POPPY findings from the neonatal unit survey
extremely valuable: (Redshaw et al. 2010), it was possible to identify indica-
My health visitor found out there was a premature infant support tors for the implementation of family-centred care, which
group afterwards, you know, that met in [name of town] once a neonatal units could use to audit their activities or develop
month and I actually found that very helpful. a more family-centred care model and practice. These indi-
cators provide some insight into whether the philosophy,
principles, and components of the POPPY model are be-
So it’s really valuable to have people who have had the same ing implemented. The indicators require further testing to
experience because you miss out on so many things that people assess their utility in effectively measuring POPPY imple-
accept as normal.
mentation (see Table 2).
A summary of the seven stages of the POPPY model Step 7: Initial Testing
of care capturing key aspects for parents is presented in The components of the POPPY model of family-centred
Figure 4. care have undergone some informal initial testing to
250 Fourth Quarter 2012 r Worldviews on Evidence-Based NursingPOPPY Model for Neonatal Units
TABLE 2
POPPY indicators of family-centred care for neonatal units
Philosophy of care and vision
r Unit policies which emphasise "partnership working" with parents and families.
r Openness and involvement shown in engaging with fathers, partners, and families.
r Access to written information and opportunities for discussion.
r Supportive handover of responsibility for care.
Organisational features
r Open visiting, that is unrestricted access to the neonatal intensive care unit.
r The development of specialist roles funded and/or organised by the neonatal unit (such as breastfeeding and bereavement support,
and neonatal outreach).
Specific policies on:
r Introduction and orientation to the unit and levels of care for parents and families.
r Education for parents, that is infant care, developmental and behavioural cues.
r Supporting parental contact with infant including fathers and partners and the availability of skin-to-skin "kangaroo" care.
r Information exchange with parents. Examples of good practice include parent folders, parent update meetings, attendance at ward
rounds, shared infant-logs or diaries.
r Ensuring policy implementation and consistency.
r Preparation and planning for discharge.
r Availability and use of staff in specialist roles (such as counselling, breastfeeding support, developmental care).
r Continuity of care after going home (home support programme).
Facilities
r A transitional care facility.
r Care areas in which six or fewer infants are cared for.
r Some single/double cubicles in which one or two infants can be cared for.
r A parents’ sitting room on or adjacent to the neonatal unit.
r A facility for parents to make snacks and hot drinks.
r A play-area or room for other children in the family.
r Overnight rooms (with ensuite facilities) for parents, appropriate in number for the population served.
identify acceptable content and face validity with parents, issues, that includes staffing, priorities in commissioning,
professionals, and neonatal units who received summaries the culture of maternity services, including neonatal units,
of the study, which suggests POPPY has relevance and the availability of resources, and the need for long-term
utility for neonatal units. The next phase of POPPY will commitment throughout the services providing care for
involve a pilot implementation study to explore the effec- babies and their families. The parents who identified the
tiveness of POPPY indicators as providing a valid measure need for POPPY experienced the consequences of poor
of implementation and to better understand the most ap- implementation and their experiences demonstrated the
propriate context and method for facilitating the POPPY provision of non-family-centred care, which had a sig-
model of family-centred care into practice (Rycroft-Malone nificant negative impact on them and their families. The
et al. 2004). POPPY Project examined family-centred care afresh, with
the aim of understanding what parents want from this ap-
proach and identifying family-centred practices that are
DISCUSSION AND CONCLUSIONS
supported by robust research evidence. Parental involve-
Family-centred care has evolved as a key concept in chil- ment from the outset in the form of strong collaborative
dren’s care and in neonatal services over the last few parental involvement was critical in developing a new
decades, with its aim of placing parents and the family model of care, which was relevant, appropriate, and ac-
at the centre of health care and promoting individualised, ceptable for parents, as well as based on robust research
flexible care. Evidence suggests it enables a better par- evidence. Such collaborative involvement involves parents
ent experience, with better outcomes for parents and in- as research partners, rather than as individuals who might
fants. Despite the focus placed on family-centred care, its be consulted occasionally or as individuals who are sub-
implementation has proved to be challenging (Mikkelsen jects of research, providing data on experiences (INVOLVE
& Frederiksen 2011). Although the reasons for this are 2012). Although a range of models of family-centred care
not entirely clear explanations may include organisational have been developed, strong parental collaboration of this
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 251POPPY Model for Neonatal Units
type does not appear to have been a key feature. Com- tribute to neonatal services in any country becoming more
parison between POPPY and other models such as the family-centred through more effectively addressing the ex-
FCC map (Dunn et al. 2006) shows some similarities and pectations and needs of parents, although providing high
some differences. The clear evidence base underpinning quality clinical care for their infants. In this way, high qual-
POPPY is one such difference, drawing on extensive qual- ity parent-centred services for families, based on clinical,
itative data and systematic review evidence, thus meeting economic and patient-based evidence (Staniszewska et al.
Dunn et al.’s (2006) challenge of demonstrating a clear ev- 2010) will become accepted healthcare practice.
idence base for family-centred care practice, which has not
been common practice in this area. The components of the References
POPPY model also differ from the FCC map in that they Als H., Gilkerson L., Duffy F.H., McAnulty G.,
could be described as more parent-focused in that POPPY Buehler D., VandenBerg K., Sweet N., Sell E.,
has tried to capture and reflect all aspects of what makes Parad R., Ringer S., Butler S., Blickman J.G.
for a good parent experience and to express it in language & Jones, K.J. (2003). A three-center, random-
parents would recognise, developed through collaboration ized, controlled trial of individualized developmen-
with parents. As such, it represents a model parents would tal care for very low birth weight preterm infants:
recognise and expect from their care. Medical, neurodevelopmental, parenting, and caregiv-
The responsibility for delivering family-centred neona- ing effects. Journal of Developmental and Behavioral Pe-
tal care lies with all healthcare professionals working in diatrics, 24, 399–408.
neonatal care and those working with babies and their Auckland District Health Board. (2009). Virtual tour
families after discharge home. The successful implemen- of the neonatal unit. Resources for parents. Re-
tation of the POPPY model of family-centred care requires trieved July 1, 2009, from http://www.adhb.govt.nz/
organisational commitment and engagement by individual newborn/ParentSupport/Virt ualNICUTour.htm.
practitioners, with specific roles and duties that include Barrera M.E., Rosenbaum P.L. & Cunningham C.E.
breastfeeding support, developmental care, home visiting, (1986). Early home intervention with low-birth-weight
emotional support, and bereavement care. It also requires infants and their parents. Child Development, 57, 20–
that the organisation responsible for providing care has 33.
parent- and family-oriented policies, training, and edu- Bennett R. & Sheridan C. (2005). Mothers’ perceptions of
cation. Finally, it includes neonatal networks and other ‘rooming-in’ on a neonatal intensive care unit. Infant, 1,
organisations or groups involved in the commissioning, 171–174.
provision, and organisation of care. To ensure that services Bracht M., Ardal F., Bot A. & Cheng C.M. (1998). Initiation
provide family-centred care there needs to be a commit- and maintenance of a hospital-based parent group for
ment to this approach throughout the entire service. As parents of premature infants: Key factors for success.
well as considering how the service is experienced by in- Journal of Neonatal Nursing, 17, 33–37.
fants, their parents and wider families, it means becoming Brazelton T.B., & Nugent J.K. (1995). The neonatal be-
a learning organisation in which there is regular communi- havioural assessment scale, 3rd edn London: MacKeith
cation across multidisciplinary teams, to share ideas, policy Press.
guidance, research findings and feedback from local par- Brett J., Staniszewska S., Newburn M., Jones N. & Tay-
ents to facilitate learning and service development, perhaps lor L. (2011). A systematic mapping review of effective
using approaches such as appreciative inquiry (Cooperider interventions for communicating with, supporting and
& Srivastvas 1987). We are planning a follow-up study to providing information to parents of preterm infants. BMJ
examine effective implementation to understand how the Open, 1. doi: 10.1136/bmjopen-2010-000023.
POPPY model of care can be moved into practice. Broedsgaard A. & Wagner L. (2005). How to facilitate
Although POPPY has been developed within a UK con- parents and their premature infant for the transition
text, it has drawn on international research evidence for home. International Nursing Review, 52, 196–203.
the systematic review. However, POPPY parents were UK Browne J.V. & Talmi A. (2005). Family-based intervention
based and their experiences may not reflect those of par- to enhance infant-parent relationships in the neonatal
ents in other countries. We would encourage researchers intensive care unit. Journal of Pediatric Psychology, 30,
in other countries to utilise the same collaborative model 667–677.
of involvement, working with parent groups with experi- Bruce B., Letourneau N., Ritchie J., Larocque S., Dennis C.
ence of having a preterm infant, to test the utility of the & Elliot M.R. (2002). A multisite study of health pro-
POPPY model in relation to its conceptual equivalence fessionals’ perceptions and practices of family-centred
for implementation in other countries. This could con- care. Journal of Family Nursing, 8(4), 408–429.
252 Fourth Quarter 2012 r Worldviews on Evidence-Based NursingPOPPY Model for Neonatal Units
Buarque V., de Carvaiho Lima M., Parry Scott R., care) to family interaction, proximity, and touch. Jour-
Vasconcelos M.G.L. (2006). The influence of support nal of Family Psychology, 17(1), 94–107.
groups on the family of risk newborns and on neonatal Forsythe P. (1998). New practices in the transitional care
unit workers. Jornal de Pediatria, 82(4), 295–301. center improve outcomes for babies and their families.
Byers J.F., Lowman L.B., Francis J., Byers J.F., Lowman Journal of Perinatology, 18(6 Pt 2 Suppl.), S13–S17.
L.B., Francis J., Kaigle L., Lutz N.H., Waddell T. & Diaz Freer Y., Lyon A., Stenson B. & Coyle C. (2005).
A.L. (2006). A quasi-experimental trial on individual- BabyLink—improving communication among clini-
ized, developmentally supportive family-centered care. cians and with parents with babies in intensive care.
Journal of Obstetrics, Gynecolology and Neonatal Nursing, British Journal of Healthcare Computing and Information
35(1), 105–115. Management, 22(2), 34–36.
Centre for Dissemination and Reviews. (2009). System- Furman L., Minich N. & Hack M. (2002). Correlates of
atic reviews: CRD’s guidance for undertaking reviews in lactation in mothers of very low birth weight infants.
health care. NHS Centre for Reviews and Dissemination. Pediatrics, 109(4), e57.
University of York. Retrieved April 2009 from http:// Galvin E., Boyers L., Schwartz P.K., Jones M.W., Mooney
www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdf. P., Warwick J. & Davis J. (2000). Challenging the pre-
Cooper L.G., Gooding J.S., Gallagher J., Sternesry L., Led- cepts of family centered care: Testing a philosophy. Pe-
sky R. & Berns S.D. (2007). Impact of a family-centered diatric Nursing, 26(6), 625–632.
care initiative on NICU care, staff and families. Journal Gannon B.A. (2000). Caring one day at a time. Neonatal
of Perinatology, 27(Suppl. 2), S32–S37. Network: The Journal of Neonatal Nursing, 19, 25–32.
Cooperider D.L. & Srivastvas S. (1987). Appreciate inquiry Gray J.E., Safron R.B., Davis G., Pompilio-Weitzner J.E.,
in organisational life. Research in Organizational Change Zaccagnini L. & Pursley D. (2000). Baby care link: Using
and Development, 1, 129–169. the internet and telemedicine to improve care for high
Costello A., Bracht M., Van Camp K. & Carman L. (1996). risk infants in pediatrics, Pediatrics, 106, 1318–1324.
Parent information binder: Individualizing education Hall E. (2007). When a newborn of small child is critically
for parents of preterm infants. Neonatal Network— ill. Nurses’, parents’ and grandparents’ experiences and
Journal of Neonatal Nursing, 15, 43–46. dynamics in family-centred care. Doctoral thesis, Aarhus,
Costello A. & Chapman J. (1998). Mothers’ perceptions of Denmark: University of Aarhus.
the care-by-parent program prior to hospital discharge Hawthorne J. (2005). Using the Neonatal Behavioural As-
of their preterm infants. Neonatal Network—Journal of sessment Scale to support parent-infant relationships.
Neonatal Nursing, 17, 37–42. Infant, 1, 213–218.
Culp R.E., Culp A.M. & Harmon R.J. (1989). A tool for Huckabay L.M. (1999). The effect on bonding behavior of
educating parents about their premature infants. Birth, giving a mother her premature baby’s picture. Scholarly
16, 23–26. Inquiry for Nursing Practice, 13(4), 349–362.
Department of Health. (2007). Maternity matters: Choice, Hurst I. (2006). One size does not fit all: Parents eval-
access and continuity of care in a safe service, London: uation of a support program in the neonatal intensive
Author. care nursery. Journal of Perinatal and Neonatal Nursing,
Department of Health. (2004). National Service Framework 20(3), 252–261.
for Children, Young People and Maternity Services: Mater- Hutchfiefd K. (1999). Family-centred care: A concept anal-
nity services, London: Department of Health; Depart- ysis. Journal of Advanced Nursing, 29(5), 1178–1187.
ment for Education and Skills. INVOLVE 2012. Briefing notes for researchers: Involving
Dunn M.S., Reilly M.C., Johnston A.M., Hoopes R.D. & the public in NHS, public health and social care re-
Abraham M.R. (2006). Development and dissemination search. Eastleigh, UK: INVOLVE.
of potentially better practices for the provision of family- Johnson B.H. (2000). Family-centered care: Four decades
centred care in neonatology: The Family-Centered Care of progress. Family Systems and Health, 18, 137–156.
Map. Pediatrics, 118(Suppl. 2), S95-S107. Johnston A.M., Bullock C.E., Graham J.E., Reilly M.C.,
Elliott S. & Reimer C. (1998). Postdischarge telephone Rocha C., Hoopes R.D., Van Der Meid V., Guiterrez S.
follow-up program for breastfeeding preterm infants dis- & Abraham M.R. (2006). Implementation and case-
charged from a special care nursery. Neonatal Network— study results of potentially better practices for family-
Journal of Neonatal Nursing, 17, 41–45. centered care: The family-centered care map. Pediatrics,
Feldman R., Weller A., Sirota L. & Eidelman A.I. (2003). 118(Suppl. 2), S108–S114.
Testing a family intervention hypothesis: The contri- Kaaresen P.I., Rønning J.A. Ulvund S.E. & Dahl
bution of mother-infant skin-to-skin contact (Kangaroo L.B. (2006). A randomized, controlled trial of the
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 253POPPY Model for Neonatal Units effectiveness of an early-intervention program in re- Stevens H. (2005). Implementing family-centred care: ducing parenting stress after preterm birth. Pediatrics, An exploration of the beliefs and practices pf paediatric 118(1), 9–19. nurses. Australian Journal of Advanced Nursing, 23(1), Klebanov P.K., Brooks-Gunn J. & McCormick M.C. 31–36. (2001). Maternal coping strategies and emotional dis- Pearson J. & Andersen K. (2001). Evaluation of a program tress: Results of an early intervention program for low to promote positive parenting in the neonatal intensive birth weight young children. Developmental psychology, care unit. Neonatal Network—Journal of Neonatal Nurs- 37, 654–667. ing, 20, 43–48. Koh T.H. & Jarvis C. (1998). Promoting effective commu- Penticuff J.H. & Arheart K.L. (2005). Effectiveness of an nication in neonatal intensive care units by audiotap- intervention to improve parent-professional collabora- ing doctor-parent conversations. International Journal of tion in neonatal intensive care. Journal of Perinatal & Clinical Practice, 52, 27–29. Neonatal Nursing, 19, 187–202. Langley D., Hollis S. & MacGregor D. (1999). Parents’ Petersen M.F., Cohan J. & Parsons V. (2004). Family- perceptions of neonatal services within the community: centred care: Do we practice what we preach? Journal A postal survey. Journal of Neonatal Nursing, 5, 7–11. of Obstetric, Gynecologic, and Neonatal Nursing, 33(4), Malusky S.K. (2005). A concept analysis of family-centred 421–427. care in the NICU. Neonatal Network, 24(6), 25–32. Preyde M. & Ardal F. (2003). Effectiveness of a parent Melnyk, B.M., Alpert-Gillis, L., Feinstein, N., Crean, H., “buddy” program for mothers of very preterm infants in Johnson, J.E., Fairbanks, E., Small L., Rubenstein J., a neonatal intensive care unit. Canadian Medical Associ- Slota M. & Corbo-Rickert B. (2004). Creating Opportu- ation Journal, 168, 969–973. nities for Parent Empowerment: Program effects on the Redshaw, M.E. & Hamilton K.E. on behalf of POPPY Team. mental health/coping outcomes of critically ill young (2010). Family centred care? Facilities, information and children and their mothers. Pediatrics, 113, e597–e607. support for parents in UK neonatal units. Archives of Melnyk B.M., Feinstein N.F., Alpert-Gillis L., Fairbanks E., Disease in Childhood. Fetal and Neonatal Edition, 95(5), Crean H.F., Sinkin R.A., Stone P.W., Small L., Tu X. & F365–368. Gross S.J. (2006). Reducing premature infants’ length Resnick M.B., Armstrong S. & Carter R.L. (1988). Devel- of stay and improving parents’ mental health outcomes opmental intervention program for high-risk premature with the Creating Opportunities for Parent Empower- infants: Effects on development and parent-infant in- ment (COPE) Neonatal Intensive Care Unit Program. teractions. Journal of Developmental & Behavioral Pedi- A randomised controlled trial. Pediatrics, 118, e1414– atrics, 9, 73–78. e1437. Ritchie J., Spencer I. (1994). Qualitative data analysis for Meier P.P., Engstrom J.L., Mangurten H.H., Estrada E., applied policy research. In Bryman A. & Burges R.G. Zimmerman B. & Kopparthi R. (1993). Breastfeeding (Eds.). Analysing Qualitative Data (173–194). London, support services in the neonatal intensive-care unit. UK: Routledge. Journal of Obstetric Gynecologic and Neonatal Nursing, Roman L.A., Lindsay J.K., Boger R.P., Dewys M., Beaumont 22, 338–347. E.J., Jones A.S. & Haas B. (1995). Parent-to-parent sup- Meyer E.C., Coll C.T., Lester B.M., Boukydis C.F., Mc- port initated in the neonatal intensive care unit. Research Donough S.M. & Oh W. (1994). Family-based interven- in Nursing and Health, 18(5), 385–394. tion improves maternal psychological well-being and Rycroft-Malone J., Harvey G., Seers K., Kitson A., McCor- feeding interaction of preterm infants. Pediatrics, 93, mack B. & Titchen A. (2004). An exploration of the 241–246. factors that influence the implementation of evidence Mikkelsen G. & Frederiksen K. (2011). Family-centred into practice. Journal of Clinical Nursing, 13, 913–924. care of children in hospital—A concept analysis. Journal Saunders R.P., Abraham M.R., Crosby A.M., Thomas K., of Advanced Nursing, 67(5), 1152–1162. Williams B.C. & Edwards W.H. (2003). Evaluation of NHS Quality Improvement Scotland. (2005). Clinical stan- potentially better practices for improving family-centred dards: Maternity services. Edinburgh. care in neonatal intensive care units. Pediatrics, 111, Ortenstrand A., Winbladh B., Nordstrom G. & Walden- e437. strom U. (2001). Early discharge of preterm infants Scottish Executive. (2001). A framework for maternity ser- followed by domiciliary nursing care: Parents’ anxiety, vices in Scotland. Edinburgh: Author. assessment of infant health and breastfeeding. Acta Pae- Shields L. & Nixon J. (2004). Hospital care of children diatrica, 90, 1190–1195. in four countries. Journal of Advanced Nursing, 45(5), Palladelis P., Cruickshank M., Wainohu D., Winskill R. & 475–486. 254 Fourth Quarter 2012 r Worldviews on Evidence-Based Nursing
POPPY Model for Neonatal Units
Shields L., Pratt J. & Davis L.M. (2007). Family-centred Low birth-weight prematures: Preventive intervention
care for children in hospital. Cochrane Database of and maternal attitude. Child Psychiatry & Human Devel-
systematic Reviews, Issue 1, Art. no. CD004811. doi: opment, 17, 152–165.
10.1002/14651858. Tessier R., Cristo M., Velez S., Giron M., de Calume Z.F.,
Spiker D., Ferguson J. & Brooks G. (1993). Enhancing ma- Ruiz-Palaez J.G. et al. (1998). Kangaroo mother care
ternal interactive behavior and child social competence and the bonding hypothesis. Pediatrics, 102(2), e17.
in low birth weight, premature infants. Child Develop- Van Riper M. (2001). Family-provider relationships and
ment, 64, 754–768. well-being in families with preterm infants in the NICU.
Staniszewska S., Crowe S., Badenoch D., Edwards C., Sav- Heart and Lung, 30(1), 74–84.
age J. & Norman W. (2010). The PRIME project: Devel- Welsh Assembly Government. (2005). National service
oping a patient evidence-base. Health Expectations, 13, framework for children, young people & maternity ser-
312–322. vices in Wales. Cardiff: Author.
Staniszewska S., Jones N., Newburn M. & Marshall S. White J.C., Smith M.M., Lowman D.K., Reidy T.G., Mur-
(2007). User involvement in the development of a re- phy S.M. & Lane S.J. (2000). Parent support of feeding
search bid: Barriers, enablers and impacts. Health Expec- in the neonatal intensive care unit: Perspectives of par-
tations, 10, 173–183. ents and occupational therapists. Physical and Occupa-
Szajnberg N., Ward M.J., Krauss A. & Kessler D.B. (1987). tional Therapy in Pediatrics, 19, 111–126.
Worldviews on Evidence-Based Nursing r Fourth Quarter 2012 255You can also read

















































