THE RUS-AUDIT VALIDATION STUDY PROTOCOL - Adapting and validating the Alcohol Use Disorders Identification Test (AUDIT) in the Russian Federation ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

THE RUS-AUDIT VALIDATION STUDY
PROTOCOL
Adapting and validating the Alcohol Use Disorders Identification Test (AUDIT)
in the Russian Federation
THE RUS-AUDIT VALIDATION STUDY PROTOCOL Adapting and validating the Alcohol Use Disorders Identification Test (AUDIT) in the Russian Federation
ABSTRACT The Alcohol Use Disorders Identification Test (AUDIT) is internationally recognized as one of the most successful instruments in screening for problematic alcohol use, including possible alcohol use disorders. However, inconsistent use of different existing Russian-language translations of the AUDIT has been observed in the Russian Federation as well as other countries, and none of the existing versions appears to have been formally validated using an established study protocol. Inconsistency in the way the various AUDIT versions that currently exist are applied in different settings creates problems both in their application and in the interpretation of results. Furthermore, it presents a significant barrier to the implementation of a screening and brief intervention strategy at primary health-care (PHC) level in the Russian Federation for early detection of individuals who consume alcohol in a way that puts them at risk. The present study protocol describes the steps that were required to validate the AUDIT in the Russian Federation. It documents several pre-studies that were conducted as part of an extended problem analysis and provides guidance on the specific steps that need to be taken to translate and adapt the AUDIT for use in the Russian language. It also gives an overview of study procedures aimed at determining the best AUDIT thresholds for different risk levels and thus implementing interventions at PHC level in the Russian Federation. The study protocol can inform validation efforts in other countries, while the study result has potential to be used in other countries that have drinking patterns and health-care systems similar to those in the Russian Federation. KEYWORDS ALCOHOL USE DISORDERS PRIMARY HEALTH CARE RUSSIAN FEDERATION SCREENING AND BRIEF INTERVENTION TEST TRANSLATION AND ADAPTATION ISBN 978-92-890-5572-7 © World Health Organization 2021 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition: The RUS-AUDIT validation study protocol: adapting and validating the Alcohol Use Disorders Identification Test (AUDIT) in the Russian Federation. Copenhagen: WHO Regional Office for Europe; 2021”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/rules/). Suggested citation: The RUS-AUDIT validation study protocol: adapting and validating the Alcohol Use Disorders Identification Test (AUDIT) in the Russian Federation. Copenhagen: WHO Regional Office for Europe; 2021. Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris. Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing. Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user. General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use. Photos: pp. v, 6 ©WHO/Anna Bunova, p. 13 ©WHO, p. 19 ©WHO/Maria Neufeld, p. 21 ©WHO/Evgeny Zhvania.

CONTENTS
Acknowledgements v
Abbreviations v
Executive summary vi
1. Background: the AUDIT as a screening instrument 1
2. Purpose and objective of the Russian validation 4
3. Preliminary studies and problem analysis 7 iviv
3.1 Systematic review of Russian AUDIT translations and validation studies 7
3.2 Qualitative expert interviews on the perception of the AUDIT 8
3.3 Main outcomes and recommendations of the pre-studies 10
4. Translation and adaptation procedures of the AUDIT 11
4.1. Adaptation procedure of the AUDIT to assess alcohol use in the Russian Federation 11
4.2 Translation and back-translation of the AUDIT and expert panel 11
4.3 Piloting the revised version with the target audience and cognitive interviewing 12
4.4 Panel discussion, revision and broader piloting of final forms 13
5. Main validation study 14
5.1 Objectives 14
5.2 Study design and sample 15
5.3 Data collection 16
5.4 Data processing and quality control 19
6. Ethical considerations 21
7. Implications for SBI in the Russian Federation 22
References 24
Annex 1. Advisory Board for the RUS-AUDIT validation project in the Russian Federation 30
Annex 2. Interview guide for the qualitative expert interview study (qualitative pilot) 31
Annex 3. Protocol for the pilot study (quantitative pilot), including questionnaire 33
Annex 4. Power calculations for the validation study 36
Annex 5. The constructed and adapted RUS-AUDIT as used in the questionnaire form
in the main validation study (back-translated from Russian) 38
Annex 6. THE RUS-AUDIT show card and conversion table as used in the questionnaire
form in the main validation study (back-translated from Russian) 40
Annex 7. Overview of training modules and activities of interviewer training 41
ACKNOWLEDGEMENTS
The WHO Regional Office for Europe expresses its gratitude to the Ministry of Health of the Russian Federation for its support
for the WHO European Office for the Prevention and Control of Noncommunicable Diseases. The study protocol was developed
as a collaborative project by the RUS-AUDIT Project Advisory Board under the guidance of the Ministry of Health of the Russian
Federation, the WHO Country Office in the Russian Federation and the WHO European Office for the Prevention and Control of
Noncommunicable Diseases. The Regional Office for Europe would like to thank all the members of the Project Advisory Board
of the RUS-AUDIT project for their overall contributions to developing the technical concept of the protocol, providing technical
support in conducting the pre-studies and discussing the results that have informed the final version of the protocol.
Development of the study protocol – including development of the technical concept, the study design, data collection and data
analysis for the various pre-studies – and the writing and review of this publication were carried out Maria Neufeld, consultant,
WHO European Office for the Prevention and Control of Noncommunicable Diseases; Jürgen Rehm, WHO Collaborating Centre
vv
and Institute for Mental Health Policy Research, Centre for Addiction and Mental Health, Toronto, Canada, Institute of Clinical
Psychology and Psychotherapy, Technische Universität Dresden, Germany, Agència de Salut Pública de Catalunya, Barcelona,
Spain, and Department of International Health Projects, Institute for Leadership and Health Management, I.M. Sechenov First
Moscow State Medical University, Moscow, Russian Federation; and Carina Ferreira-Borges, Acting Head, WHO European Office
for the Prevention and Control of Noncommunicable Diseases, and Programme Manager, Alcohol and Illicit Drugs, WHO European
Office for the Prevention and Control of Noncommunicable Diseases.
The WHO Regional Office for Europe would also like to extend its gratitude to the following experts for their contributions in
carrying out several pre-studies and discussing their results in the context of the study protocol: Anna Bunova, junior researcher,
National Medical Research Center for Therapy and Preventive Medicine, Moscow, Russian Federation; Artyom Gil, associate
professor, Institute for Leadership and Health Management, I.M. Sechenov First Moscow State Medical University, Moscow,
Russian Federation; Boris Gornyi, leading researcher, National Medical Research Center for Therapy and Preventive Medicine,
Moscow, Russian Federation; Eugenia Fadeeva, Head of the Department of Organization of Preventive Care in Narcology, National
Research Centre on Addictions – branch, V.P. Serbsky National Medical Research Center for Psychiatry and Narcology, Moscow,
Russian Federation; Anna Kalinina, Head of the Department of Primary Prevention of Chronic Noncommunicable Diseases,
National Medical Research Center for Therapy and Preventive Medicine, Moscow, Russian Federation; Anna Kontsevaya, Deputy
Director, National Medical Research Center for Therapy and Preventive Medicine, Moscow, Russian Federation; Evgenia Koshkina,
Aleksey Nadezhdin and Elena Tetenova, leading researchers, Moscow Research and Practical Center for Narcology of the
Department of Public Health, Moscow, Russian Federation; and Konstantin Vyshinsky, National Research Centre on Addictions
– branch, V.P. Serbsky National Medical Research Center for Psychiatry and Narcology, Moscow, Russian Federation.
The WHO European Office for the Prevention and Control of Noncommunicable Diseases is also grateful to Melita Vujnovic,
WHO country representative in the Russian Federation, and Elena Yurasova, NCD Technical Officer, WHO Office in the Russian
Federation, for leading technical consultations and contributing critical ideas to the content development of the protocol and
the overall RUS-AUDIT validation project.
The activities associated with the validation of the RUS-AUDIT protocol were fully or partially funded through a grant of
the Government of the Russian Federation in the context of the WHO European Office for the Prevention and Control of
Noncommunicable Diseases.
ABBREVIATIONS
AUC area under [the ROC] curve
AUD alcohol use disorder
AUDIT Alcohol Use Disorders Identification Test
AUDIT-C Alcohol Use Disorders Identification Test – Consumption
CIDI Composite International Diagnostic Interview
DSM-5 Diagnostic and Statistical Manual of Mental Disorders, 5th revision
ICD-10 International Statistical Classification of Diseases and Related Health Problems, 10th revision
ICD-11 International Statistical Classification of Diseases and Related Health Problems, 11th revision
NCD noncommunicable disease
PHC primary health care
ROC receiver operating characteristic
RUS-AUDIT Russian (Russian Federation-specific) Alcohol Use Disorders Identification Test
SBI screening and brief intervention
WMH World Mental HealthEXECUTIVE SUMMARY The Russian Federation has successfully implemented several alcohol control measures, such as WHO’s “best buys”, to reduce the burden of disease attributable to alcohol use and to increase life expectancy. In 2016 the Ministry of Health of the Russian Federation launched an initiative to implement screening and brief intervention (SBI) for alcohol problems in the primary health-care (PHC) setting; SBI is an evidence- based practice used to identify, reduce and prevent problematic use and abuse of alcohol and illicit drugs, as well as substance use disorders. As is recognized in the WHO Global Strategy to Reduce the Harmful Use of Alcohol and in the WHO European vivi Action Plan to Reduce the Harmful Use of Alcohol 2012–2020, delivering SBI for alcohol-related problems in PHC settings can be an effective and efficient way to reduce alcohol consumption by hazardous and risky drinkers and to raise general awareness of alcohol-related problems. The Alcohol Use Disorders Identification Test (AUDIT) was developed by WHO as the main instrument for delivering SBI and was validated in PHC facilities in six different countries across four continents. However, a systematic translation, adaptation and validation of the instrument in the Russian Federation are all still missing, which poses a significant barrier to the implementation of SBI at country level. Thus, by validating the AUDIT to conduct screening for alcohol consumption among patients in primary care, the present study will lay the groundwork for implementing the SBI strategy in the Russian Federation. The present protocol describes the background and history of the AUDIT, the specific scope and purpose of the validation in the Russian Federation, and the preliminary studies that systematically analysed existing problems in application of the AUDIT in various settings in the Russian Federation. The steps that were required to carry out the main validation study are also described and explained. The availability of a quick, effective and reliable screening tool as part of the SBI strategy is a crucial cornerstone of its success. Delivering SBI will contribute to increasing opportunities to educate patients about lower-risk alcohol consumption levels and the risks of excessive alcohol use; it will also be a starting point for discussions with them about the implications of their drinking for current symptoms and future health. The SBI strategy may alert clinicians to the need to advise patients whose alcohol consumption might adversely affect their use of medications and other aspects of their treatment and may also improve referral pathways. Finally, it will be a step towards making alcohol SBI part of health-care systems more widely and contribute to further reductions in alcohol-attributable mortality and morbidity at population level.
1 BACKGROUND: THE AUDIT AS
A SCREENING INSTRUMENT
The Alcohol Use Disorders Identification Test (AUDIT) has been one of the most
successful and frequently used screening instruments for hazardous and harmful
alcohol use and potential alcohol dependence (Babor et al., 2001; Saunders et al., 1
1993b). The instrument was developed by WHO in 1989 as a simple method of
screening for excessive drinking and to assist in brief assessment. It was primarily
intended for screening in the health-care system and to initiate interventions, but
suggestions were also made for its use in many other settings, such as in workplace
and employee assistance programmes, the military services, the courts, and jail
and prison settings (Babor et al., 2001). Since then, the AUDIT has been used not
only in many of these settings but also as a part of monitoring systems of the
general population and for research purposes (Lange et al., 2019; Lundin et al., 2015).
The original AUDIT was validated by research centres in Australia, Bulgaria, Kenya,
Mexico, Norway and the United States, using primary health-care (PHC) facilities
to gather empirical data from study participants on alcohol intake and drinking
practices, general medical history, and any physical or psychosocial problems
related to alcohol (Saunders et al., 1993a and 1993b). The goal was to develop an
international instrument to screen for hazardous and harmful alcohol consumption.
These two key terms have been defined by WHO as follows (WHO, 1994):
⋅⋅ Hazardous use • A pattern of alcohol use that increases the risk of harmful
consequences for the user, including consequences that affect
physical and mental health (as in harmful use) and social consequences.
In contrast to harmful use, hazardous use refers to patterns of use
that are of public health significance despite the absence of any current
disorder in the individual user.
The term “hazardous use” was not included in the 10th revision of the
International Statistical Classification of Diseases and Related Health
Problems (ICD-10) (WHO, 2019b), but was nevertheless used by WHO to denote
a drinking pattern carrying a risk of harmful consequences to the
drinker (Babor & Higgins-Biddle, 2001). However, it was introduced in the
11th revision (ICD-11), where it is defined as a pattern of psychoactive
substance use that increases the risk of harmful physical or mental health
consequences to the user or to others to an extent that it warrants
attention and advice from health-care professionals; the increased risk may
be from the frequency of substance use, from the amount used on a
given occasion, from risky behaviours associated with substance use or
the context of use, from a harmful route of administration, or from a
combination of these (WHO, 2020a).⋅⋅ Harmful use • A pattern of alcohol use that is causing damage to health.
The damage may be physical (such as liver damage following chronic drinking)
or mental (such as depressive episodes following heavy alcohol intake).
At the time of its development, the AUDIT did not allow social consequences
alone to justify a diagnosis of harmful use.
The term was introduced in ICD-10 and revised in ICD-11 under the heading
“Harmful pattern of use of alcohol”, where a distinction between continuous
and episodic patterns of use was also made (WHO, 2020b).
Importantly, harm to the health of others was included in the definition of
harmful use in ICD-11. Harm to the health of others may be intentional,
as in the case of homicides or interpersonal violence during intoxication with
alcohol (or drugs), or it may result from the substance user’s difficulty in 2
performing social, professional or family roles, as in the case of negligence
towards minors. Accordingly, in ICD-11, a harmful pattern of use is defined
Background: the AUDIT as a screening instrument
as one that has caused clinically significant harm to a person’s physical or
mental health, or in which substance-induced behaviour has caused clinically
significant harm to the health of other people. Again, harm may be caused by
the intoxicating effects of a substance, the direct or secondary toxic effects on
body organs and systems, or a harmful route of administration (WHO, 2020b).
For further discussion of hazardous and harmful use, see Higgins-Biddle & Babor,
2018; Poznyak, Reed & Medina-Mora, 2018; and Saunders, Peacock & Degenhardt, 2018.
The AUDIT contains 10 items which are classified in three domains: alcohol use,
dependence symptoms and harmful use (Table 1); the responses to each item are
scored between 0 and 4, and then summed to yield a potential score between 0
and 40 (Babor et al., 2001). AUDIT results can be used in a brief intervention to help
patients who drink too much to stop drinking or to cut down on their drinking to
avoid the harmful consequences of their alcohol use. They can also serve as a
basis for a referral for further assessment and treatment in patients with a more
severe alcohol use disorder (AUD).
Table 1. The AUDIT’s three domains and 10 items
Domain Item number Item content
1 Frequency of drinking
Hazardous alcohol use 2 Typical quantity
3 Frequency of heavy drinking
4 Impaired control over drinking
Dependence symptoms 5 Increased salience of drinking
6 Morning drinking
7 Guilt after drinking
8 Blackouts
Harmful alcohol use
9 Alcohol-related injuries
10 Others concerned about drinkingThe original intention was to create a screening instrument that did not include
consumption items (akin to the ICD definition), but this proved to be impossible as
much of the variation in screening for alcohol is determined by levels and patterns
of consumption. Accordingly, the final AUDIT included three consumption items
(questions 1–3 in Table 1), which are responsible for the vast majority of the variance
seen in most populations (see, for example, Bush et al., 1998). For a description of the
close relationship between drinking level and AUDs, see Rehm et al., 2013 and 2014.
The three consumption items have also been used as a shorter version of the AUDIT
under the name AUDIT-C (Alcohol Use Disorders Identification Test – Consumption)
(Bradley et al., 2003 and 2007; Bush et al., 1998; CIHS, 2018).
From the outset, the aims of the AUDIT were twofold:
⋅⋅ To develop a screening tool to be used in clinical settings to identify hazardous 3
drinkers requiring brief advice or more formalized brief interventions,
in addition to identifying people with potential AUDs who might require treatment
Background: the AUDIT as a screening instrument
at PHC level or referral for more specialized treatment (Babor et al., 2001).
To achieve this, three thresholds were needed: (1) one for simple advice on
reduction of hazardous drinking (AUDIT scores 8–15); (2) another for brief
counselling and continued monitoring (AUDIT scores 16–19); and (3) a third for
further diagnostic evaluation for alcohol dependence, often in specialized
settings (AUDIT scores ≥ 20).
⋅⋅ To allow for cross-cultural comparability and standardization.
Two major obstacles in the AUDIT’s development needed to be overcome: first, health-
care systems differ in how and where they treat AUDs (Klingemann, Takala & Hunt,
1992); and second, measurement of consumption was conceptualized by the concept
of a standard drink, often operationalized as 10–14 g of pure alcohol (in the original
version it was 10 g). However, the definition of a standard drink differs between
cultures (Kalinowski & Humphreys, 2016), and some cultures do not have such a
concept at all.
To surmount these problems for implementation, validation studies have been con-
ducted for different countries and health-care systems. Cultural adaptations for
other concepts used in the AUDIT may also be necessary, and additional test items
may be needed in order to improve the test’s characteristics. For examples of local
adaptation and validation studies of the AUDIT, see Gache et al., 2005; Higgins-Biddle
& Babor, 2018; Leung & Arthur, 2000; and Tsai et al., 2005.
The need for such a local adaptation for the Russian Federation became apparent
when, in 2016, the WHO Regional Office for Europe and the Ministry of Health of
the Russian Federation tried to introduce screening and brief intervention at PHC
level by developing appropriate training materials and modules (WHO, 2016). Many
experts involved in the initiative expressed their concern that the AUDIT might not
give an adequate assessment of specific drinking patterns common in the Russian
Federation as well as in neighbouring countries. As a consequence, a new study was
initiated to empirically lay the basis for an AUDIT, adapted to these drinking patterns
and the needs of the Russian health-care system.
The following study protocol proposes a methodology to conduct a new validation
study of the AUDIT, taking into account current drinking patterns and health-service
needs in the Russian Federation. It describes the results of various preliminary
studies that were carried out to inform the validation procedures and a step-by-step
approach towards a screening instrument validated at country level (Bunova et al.,
2021; Neufeld et al., 2021a–d; Rehm et al., 2020).2 PURPOSE AND OBJECTIVE OF
THE RUSSIAN VALIDATION
As outlined above, the AUDIT is one of the most commonly used screening in-
struments and an efficient tool to identify persons with harmful and hazardous
alcohol consumption before health and social consequences become pronounced. 4
Screening for excessive alcohol consumption assesses whether a person is at risk
of experiencing problems from alcohol use, including possible AUDs. As part of
the screening and brief intervention (SBI) approach, screening is followed by brief
intervention, which targets at-risk drinkers rather than those who already have a
pronounced AUD and would therefore require more intensive care. However, brief
interventions might serve as an initial step in the treatment process of patients
seeking extended treatment as they can be referred to specialists as part of the
brief intervention, if they wish to.
International research has shown that brief interventions at PHC level are low in
cost compared to specialized treatment and have proven to be effective (Angus et
al., 2014; Babor et al., 2004; Wutzke et al., 2001). By adopting the SBI model, several
countries have committed to fill the gap between preventive and PHC settings
and the more intensive specialized treatment required for persons with AUDs.
Facilitating access to screening, brief interventions and treatment has been included
in the WHO-led SAFER initiative as one of the five most cost-effective interventions
to reduce alcohol consumption and harm and has become a standard element of
any comprehensive alcohol policy approach (WHO, 2021b).
In 2016 the Russian Federation launched a new initiative to implement the SBI
programme within PHC settings. Leading Russian experts in the field of narcology,
addiction and prevention, practising physicians from hospitals in the Moscow
Oblast, and international consultants and representatives from the WHO Regional
Office for Europe set up a working group to develop training modules and materials
for SBI that could meet the needs of the Russian Federation. In the course of the
joint undertaking made by the WHO Regional Office for Europe and the Ministry of
Health of the Russian Federation to tailor the resources to the Russian context and
translate the WHO “training for trainers” SBI toolkit (WHO, 2017), it became evident
that there were a number of problems affecting the available Russian translations of
the training manual and, specifically, the AUDIT, the toolkit’s screening instrument.
As well as identifying inconsistencies in the various translations of the instrument
and in the way it was applied in different settings, the experts involved in the
Russian SBI initiative were concerned that the AUDIT might not give an accurate
assessment of specific drinking patterns that were common in the Russian Federation
and neighbouring countries, and thus fail to correctly classify individuals with
hazardous and harmful drinking. The principal area of concern was prolonged heavy
episodic drinking, which involves maximal alcohol intake on a single drinking occasion
followed by prolonged periods of abstinence. It was also noted that consumption
of unrecorded alcohol was not adequately captured by the AUDIT. This comprises
alcohol that is consumed as a beverage but is not recorded and taxed as such, and
includes homemade alcohol, smuggled or illegally produced alcohol, and alcohol
surrogates. According to recent WHO estimates, consumption of unrecorded
alcohol accounts for one third of total alcohol consumption in the Russian
Federation, and it poses specific challenges to the existing surveillance systems
and to the screening initiatives and treatments associated with them (Neufeld
et al., 2019; WHO, 2019a). Finally, a major concern affecting the application of theAUDIT in the context of the Russian Federation was that the concept of a “standard
drink” as defined in the instrument was not understood in the Russian Federation
(or in many other countries) – a problem that had previously been noted by several
research groups (Balachova et al., 2012; Cook et al., 2011).
For these reasons, it was concluded that a validation of the AUDIT was required
as the basis for a successful implementation of the SBI programme in the Russian
Federation. As a follow-up to this recommendation, the Alcohol and Illicit Drugs
Programme of the WHO Regional Office for Europe and the WHO Country Office in
the Russian Federation initiated the RUS-AUDIT (Russian AUDIT) review process,
dedicated to supporting the Ministry of Health of the Russian Federation in the
revision, adaptation and validation of the AUDIT. WHO invited key stakeholders
involved in the prevention and control of health risks, diseases and injuries due to
alcohol consumption to form an advisory board. Experts from the fields of public
5
health, preventive medicine, health administration, epidemiology and specialized
addiction medicine (a discipline known as “narcology” in the Russian Federation)
Purpose and objective of the Russian validation
were invited to join forces in creating a reliable and valid alcohol screening instrument
to meet the specific needs of the local context.
The RUS-AUDIT Project Advisory Board was constituted in 2018 to provide advice to
WHO and the Ministry of Health of the Russian Federation on the adaptation and
validation of the AUDIT (Annex 1). Based on the initial discussions, the advisory board
agreed to the following objectives of the RUS-AUDIT validation project:
1. to operationalize alcohol use in order to allow optimal identification of
hazardous use patterns in the Russian context;
2. to determine the best cutoff values for brief advice/interventions in PHC
settings for the Russian Federation;
3. to determine the best cutoff values for AUDs and for treatment interventions
that are needed in PHC settings or for referral to specialized treatment.
Currently, there are no lower-risk drinking guidelines for the Russian Federation,
which are commonly used in some other countries to determine minimum thresholds
for hazardous use (Rehm, Bondy & Room, 1996). Determining such thresholds
from the literature alone, rather than on the basis of local empirical evidence, is
problematic. Research has clearly shown that harmful use (in terms of its impact
on mortality rates) starts at fairly low levels of alcohol consumption (GBD 2016
Alcohol Collaborators, 2018; Shield et al., 2017; Wood et al., 2018), in some cases at
less than 12 g of pure alcohol per day (depending on methodology). However, it is
neither effective nor cost-effective to start brief interventions for patients in PHC at
such low levels of alcohol use (Rehm et al., 2016). Moreover, it has been shown that,
in general, interventions for lower levels of alcohol use seem to be less effective
than interventions for higher levels (Kaner et al., 2007 and 2018). Finally, the Russian
Federation and surrounding countries are known for their distinct heavy episodic
drinking patterns, which translate into detrimental health outcomes with a higher
level of harm per litre of alcohol consumed than is found elsewhere in the WHO
European Region (Popova et al., 2007; Shield & Rehm, 2015; Shield, Rylett & Rehm,
2016). Consumption of spirits and highly concentrated alcoholic products, including
unrecorded alcoholic products such as non-beverage alcohol and antiseptic lotions
with an alcohol content of up to 95%, is also frequently discussed in the literature
as one of the main drivers of alcohol-attributable harm in the Russian Federation
and neighbouring countries (Korotayev et al., 2018; Lachenmeier, Neufeld & Rehm,
2021; Leon et al., 2007; Neufeld & Rehm, 2018). This relationship between drinking
patterns and harm outcomes should also be taken into account when discussing
the scoring scheme and the thresholds for intervention of a screening instrument
for hazardous and harmful use.To determine the optimal intervention threshold for daily use or thresholds for other
patterns of use (such as frequency or level of heavy drinking occasions), a protocol
for a large-scale validation study at PHC level was developed and subsequently
carried out in several regions of the Russian Federation (Neufeld et al., 2021d; Rehm
et al., 2020; WHO, 2021a).
The present protocol proposes a methodology for conducting the RUS-AUDIT validation
study that takes account of local drinking patterns and health-service needs in
the Russian Federation. However, there are many other countries that face similar
challenges in the translation and implementation of screening tools for excessive
alcohol use. Inconsistencies in translation and diagnostic thresholds and lack of the
concept of a standard drink are issues common to various locations. This protocol
aims to detail the methodology of validating the AUDIT for the Russian Federation
in a format that can be transposed into other settings – most importantly, other
6
countries with similar drinking patterns. This would allow the knowledge and
experience of practitioners who consistently identify excessive drinking and provide
Purpose and objective of the Russian validation
appropriate interventions to be shared more widely among WHO Member States.
The RUS-AUDIT validation study was a multistage process involving stakeholders
from different health-care settings. To achieve the objective and purpose of the study
outlined above, the following steps were required:
1. Pre-studies and extended problem analysis to inform the validation study,
including:
⋅⋅ a systematic review of validation studies of the AUDIT in the Russian
Federation and all Russian translations of the instrument;
⋅⋅ qualitative expert interviews on the perception of the AUDIT instrument
by health-care workers and patients (in PHC and narcology settings); and
⋅⋅ a pilot study on the feasibility of using a revised version of the AUDIT
to assess alcohol use in PHC settings.
2. The main validation study to determine the optimal thresholds for using
the AUDIT in PHC settings.
The protocols for each step in the validation process are detailed below.3 PRELIMINARY STUDIES AND
PROBLEM ANALYSIS
In order to address the concerns raised by members of the advisory board, the RUS-
AUDIT validation project took a stepwise approach to analysing the existing problems
in the application of the AUDIT in the Russian Federation. This was achieved by 7
developing two preliminary studies (pre-studies).
3.1 SYSTEMATIC REVIEW OF RUSSIAN AUDIT
TRANSLATIONS AND VALIDATION STUDIES
Two systematic searches in Russian-language electronic bibliographic databases
were conducted and search engines were used in order to document and analyse
all existing Russian translations of the AUDIT and their applicability in Russian-
language populations. These various searches served to document and systematize
any reported issues with the application of the AUDIT in the Russian Federation
specifically.
The objective of the first systematic search for validation studies of the AUDIT in the
Russian Federation was to document any kind of correspondence between the AUDIT
and other means of assessing alcohol consumption, such as the WHO Composite
International Diagnostic Interview (CIDI), drinking diaries, biomarkers or established
AUD diagnoses by a specialist (for more information on CIDI, see section 5.3.2.2
below). The objective of the second search was to identify all Russian-language
translations of the AUDIT anywhere in the world and to document any differences,
such as thresholds for hazardous and harmful use, and recommendations for inter-
vention and referral.
The objectives of the two searches can thus be summarized as follows:
1. What Russian-language versions of the AUDIT exist globally and what are their
main differences?
2. What are the documented problems and solutions in the application of the
AUDIT in Russian-language populations and specifically in the Russian Federation?
3. What validation studies of the AUDIT exist in the Russian Federation?
4. What are the documented AUDIT thresholds for intervention and referral in
the Russian Federation?
The systematic searches were conducted independently by two researchers and
thoroughly documented as part of a separate publication (Neufeld et al., 2019).
In the course of the review, only one validation study of the AUDIT was identified
in the context of the Russian Federation that reported specificity and sensitivity of
the thresholds in comparison to the CIDI as an assessment method for AUDs (Yanov
et al., 2009). However, the study was conducted with a small sample of 252 patients
(183 males and 69 females) treated in a tuberculosis hospital in the Tomsk Oblast,
Siberia. Given the scale of the study and the fact that the sample was drawn from
a specific population of patients, the reported parameters of the AUDIT – namely,
91.7% sensitivity and 44.6% specificity for 12 months AUD prevalence for AUDIT scores
of > 8, and a sensitivity of 45.8% and specificity of 60.0% for AUDIT scores of > 20 –
should be interpreted with caution.In total, 61 unique Russian-language translations of the AUDIT were identified, the
majority of which were from the Russian Federation. In addition, several distinct
AUDIT versions were identified in official WHO publications (including manuals and
guidelines), as well as in clinical guidelines and recommendations from preventive
medicine and narcology specialists.
More than half of these versions failed to provide a definition of a standard drink
size, or the definition was not apparent from the source material. Many incorpo-
rated the concept of a standard drink as containing 10 g of pure alcohol, while one
version from Ukraine suggested a standard drink of 13 g, even though there is no
official definition of a Ukrainian standard drink. Various methods were employed to
demonstrate the information conveyed by the term “standard drink”. The majority
of the sources that had a standard drink definition explained it in the accompanying
material but not within the test itself – for instance, the definition appeared not
8
in the main text of a publication but in an appendix. The remaining sources either
featured an in-text explanation/definition that was part of the AUDIT instructions or
Preliminary studies and problem analysis
defined standard drink in the test’s second and third consumption items (questions
2 and 3 in Table 1 above). Some versions included pictures, a formula for calculating
individual consumption levels, or even conversion tables. Considerable inconsis-
tencies between the different versions were found, both in the presented volumes
of alcoholic beverages and in their conversion into standard drinks, as well as in the
proposed method to translate the information into an AUDIT score.
In addition, there were some other difficulties encountered, including incompre-
hensible questions, response options that deviated considerably from the original
AUDIT, and alternative cutoff points for hazardous and harmful use and possible
dependence. For instance, two sources from the Russian Federation stated that
individuals scoring 15 or more were likely to meet the criteria for current alcohol
dependence (Medpsy.ru, 2019; Petrov, 2003). The same low threshold was found in
a Russian AUDIT version from Israel (Ashdod.muni.il, 2019) and in an official WHO
publication, which stated that scores of 15 or more for men and 13 or more for women
could point to possible alcohol dependence (Graham et al., 2013). None of these
versions were properly validated empirically, nor did they mention a predetermined
protocol for systematic translation and back-translation of the tool.
These inconsistencies in the concept of a standard drink, translations of the AUDIT
and diagnostic thresholds confirmed that a single validated version of the question-
naire was needed in order to make correct assessments.
3.2 QUALITATIVE EXPERT INTERVIEWS ON THE PERCEPTION
OF THE AUDIT
In addition to the two systematic reviews, qualitative semi-structured interviews
with experts on the perception of the AUDIT were carried out (for more details, see
Neufeld at al., 2021c). In this case, experts were defined to include both health-care
professionals and patients in primary and specialized health care. The latter were
considered to be experts in the sense that they understood their own consumption
patterns and could judge whether the different versions of the AUDIT were capable
of assessing these patterns (Bogner, Littig & Menz, 2009).
The expert interviews had the following aims:
⋅⋅ to explore problems in understanding the current AUDIT items
(patients and health-care providers);
⋅⋅ to improve the clarity of any AUDIT items that were difficult to understand
(patients and health-care providers);
⋅⋅ to explore possible solutions and existing practices of screening and
quantification (health-care providers only); and
⋅⋅ to integrate experiences of using the AUDIT from earlier studies
(both published and unpublished) and applications (health-care providers only).The interview guide for the study (Annex 2) probed the following areas:
⋅⋅ the perception of frequency–volume questions and their importance (AUDIT-C);
⋅⋅ the perception of different versions of the AUDIT – specifically, two distinct Russian
translations from the main AUDIT website (auditscreen.org) featuring either
the concept of a standard drink or a predefined frequency–volume table; and
⋅⋅ the specificity of Russian drinking patterns – most importantly,
single occasions of drinking where intoxication is reached and specific markers
for problematic alcohol consumption in the Russian Federation.
The interviews were audiotaped for later content analyses. The interview guide
(Annex 2) gives an example of the kind of exploratory work that was needed to inform
9
the study protocol at this stage.
A total of 25 patients and 12 health-care professionals from PHC and narcological care
Preliminary studies and problem analysis
from the city of Moscow were interviewed as part of a convenience sampling method.
Of the patient sample, nine were recruited from inpatient narcological facilities
(only those being treated for alcohol-related conditions were recruited); nine from
an inpatient internal medicine unit of a general hospital specializing in preventive
medicine; and eight from an outpatient general polyclinic, who had presented to a
general practitioner. Twenty-one of the patients were current drinkers – that is, they
had consumed alcohol in the past 12 months; these patients were given the AUDIT-C
as part of the interview and were asked to report on the feasibility of the method
of standard drink quantification employed (that is, either pictorial material or the
volume quantification table).
Of the health-care professionals interviewed, seven were narcologists and five were
cardiologists and/or preventive medicine doctors. All the interviewed doctors had
worked with the AUDIT as part of their clinical practice or research and were thus
familiar with the instrument.
The overall results of the content analysis carried out on the interview data corrob-
orated the results from the systematic review. The difficulties in using the AUDIT
encountered by both patients and health-care providers were mainly related to the
first three items of the test – the consumption items that constitute AUDIT-C – and
their measurement of drinking volumes and intensity. The most frequently raised
issues related to (1) the usual problems of self-reported drinking volumes due to
memory bias and difficulties in understanding container and glass sizes; (2) the
unfamiliar concept of a standard drink and its applicability to the Russian context
where it is not used; and (3) the difficulty in defining a “single occasion” of drinking
and a different understanding of heavy episodic drinking. Both patients and doctors
expressed their concerns about the applicability of the concept of a standard drink,
as alcohol volumes in the Russian Federation were generally communicated in grams
and millilitres, as well as in glasses and bottles, although a more in-depth discussion
and analysis of this revealed that these notions were subjective and interchange-
able. At the same time, some health professionals from the PHC setting suggested
that the standard drink concept (which sounded neutral to patients) might be used
at PHC level for educational purposes, when informing patients about alcohol-related
harm; and it might also serve as an entry point to motivational interviewing and
general non-stigmatizing discussion about alcohol and health.
Another outcome of the interview study was the strong association between (perceived)
alcohol dependence and certain markers of problematic alcohol use, as based on
previous large-scale epidemiological studies in the Russian Federation (Leon et al.,
2007). These behaviours were seen, by both patients and doctors, as strong indica-
tors for AUDs and, specifically, for severe forms of alcohol dependence. The three
following criteria are arranged according to the severity level of the associated AUD
– in other words, the specificity of the criteria is perceived as increasing with the
severity level of alcohol dependence:⋅⋅ two or more episodes per week of excessive alcohol consumption, hangover
or going to sleep at night clothed because of drunkenness;
⋅⋅ one or more days of continuous drunkenness when the person is withdrawn from
normal social life (the operational definition of zapoi given by Leon et al., 2007);
⋅⋅ consumption of surrogate alcohol – that is, alcoholic products not officially
intended for drinking, such as colognes, lotions and alcohol for technical/
industrial purposes.
Specifically, the last criterion of surrogate alcohol consumption was strongly associated
with severe forms of AUD and marginalization by all interviewed subgroups of the
sample, including self-reports of consumers of surrogate alcohol from the narcology
setting. 10
3.3 MAIN OUTCOMES AND RECOMMENDATIONS OF THE
Preliminary studies and problem analysis
PRE-STUDIES
Based on both the systematic review of all AUDIT translations and the qualitative
interview study, the following conclusions were made to further guide the adaptation
and validation process:
⋅⋅ The concept of a standard drink alone, without assistive devices such as pictorial
support or conversion tables, is not feasible in the Russian Federation,
as there is no accepted definition of a standard drink known to patients in the
PHC or narcology settings (or to the general population).
⋅⋅ The term “single occasion of drinking” was not understandable to at least one
group of patients (very heavy drinkers who consume without interruption
for more than one day); this may lead to follow-up questions posed by inter-
viewers who have different understandings of what “one occasion” means.
This would make the AUDIT more dependent on the interviewer and the level of
their training and experience – an uncertainty that should be avoided in
the case of a standardized tool. This issue can be resolved by defining “occasion”
as a time period of 24 hours – in other words, to formulate the third
consumption item of the AUDIT in the same way as the second consumption
item and ask about a day of drinking instead of an occasion of drinking.
⋅⋅ The use of conversion tables, conversion formulas and/or show cards puts the
cognitive load on respondents, as well as on interviewers/physicians,
which will lead to biases (Schwarz, 2007; Sudman, Bradburn & Schwarz, 1996).
However, when choosing between the two, putting the cognitive load on
patients should be avoided, as the interviewer’s level of training is likely to
lead to less bias in this respect.
⋅⋅ Alternatively, we suggest that a pictorial form of quantity consumed is presented,
supported by a conversion table, and that respondents are asked only to
enumerate the number of glasses/bottles consumed and to help interviewers
with conversion of drinking volumes into standard drinks and AUDIT scores.
The concept of a standard drink can be retained as part of this assessment
to facilitate preventive and educational work, as outlined by health-care
professionals.
⋅⋅ Another option is computer-assisted tools, including animated assessment
elements such as sliders to indicate how much of a typical bottle of a particular
beverage would still be left after a respondent had poured their usual quantity
into a glass. All the conversions would be done by the computer program
as part of the computer-assisted personal interview, so neither the respondent
nor the interviewer would have to do any computations.4 TRANSLATION AND ADAPTATION
PROCEDURES OF THE AUDIT
4.1 ADAPTATION PROCEDURE OF THE AUDIT TO ASSESS 11
ALCOHOL USE IN THE RUSSIAN FEDERATION
Although there are internationally well-established methodological approaches and
documented best practices for translating, adapting and validating instruments in
health-care research, the quality of the instruments actually produced is known
to vary greatly, either because the multistep process is not considered important
enough to justify the resources required or because the process is carried out
inconsistently (Sousa & Rojjanasrirat, 2011).
WHO has an established multistep process of translation and adaptation of instruments,
the aim of which is to achieve different language versions of instruments that are
conceptually equivalent in each of their target countries/cultures (WHO, 2009). Such
an instrument should be equally acceptable and perform practically in the same
way, providing objective, reliable and valid measurements of a concept. For this
reason, the focus is on cross-cultural and conceptual (rather than linguistic and
literal) equivalence, which makes translation of instruments a very specific task,
often involving many experts from different fields.
The existing WHO guidelines for translation of instruments are based on several studies
and include the following steps:
⋅⋅ forward translation
⋅⋅ expert panel
⋅⋅ back-translation
⋅⋅ pre-testing and cognitive interviewing
⋅⋅ construction of final version
⋅⋅ documentation of the process.
In the following, the process was followed step by step to construct a Russian
Federation-specific version of the AUDIT, the so-called RUS-AUDIT (for a more detailed
description, see Neufeld et al., 2021b).
4.2 TRANSLATION AND BACK-TRANSLATION OF THE AUDIT
AND EXPERT PANEL
In the first step, a forward translation from English into Russian was made by a
group of specialists as part of the Russian translation of the WHO “training for
trainers” SBI toolkit (WHO, 2017). This version was discussed in a group discussion
by the RUS-AUDIT Project Advisory Board, which constituted the first expert panel. A
second expert panel, made up of professional translators, communication specialists
and linguists, was consulted as a separate part of the process. Existing translations
that had been identified in the systematic review were circulated and discussed,and different versions of possible translations were considered and discussed by
a smaller group of experts, who had experience in instrument development, trans-
lation and validation.
As a result of this multistep consultation process and based on the systematic review
and expert interviews, an adapted Russian version of the AUDIT was constructed,
which used pictorial material as part of the second test item to represent drinking
volumes and to convert them into standard drinks (Annex 3). A back-translation of
this penultimate version was then made by an independent expert, whose mother
tongue was English and who had no previous knowledge of the questionnaire. Some
issues and discrepancies were discussed again in a smaller expert group and a version
was prepared for a quantitative pilot study with cognitive debriefing elements.
12
4.3 PILOTING THE REVISED VERSION WITH THE TARGET
AUDIENCE AND COGNITIVE INTERVIEWING
Translation and adaptation procedures of the AUDIT
In the next step, the adapted instrument was pre-tested on the target audience –
specifically, patients from PHC facilities. The main objective of this quantitative pilot
study was to empirically test if the constructed version of the AUDIT was under-
standable to respondents and whether it was comprehensive enough to detect
hazardous alcohol consumption and potential AUDs.
In the pilot study, 79 patients from a PHC facility in Moscow, all of whom had con-
sumed alcohol in the past 12 months, were interviewed. The sample included
patients from a preventive medicine health centre and from cardiology, surgery and
internal medicine inpatient units. Additionally, participants of an ongoing study in
preventive medicine were included in the sample as they had reached out to the
preventive services of the PHC facility, which is part of PHC services according to
Russian legislation. Patients were approached in the facility by two interviewers and
asked for informed verbal consent to participate in the study in accordance with
a standardized script. Interviews were conducted face to face, either in a separate
room or in the hall of the medical unit concerned, and audiotaped. The protocol and
the questionnaire form used in the pilot study can be found in Annex 3.
All patients were administered the first three test items of the adapted version of
the AUDIT and randomly assigned to one third of the remaining items (to save time,
as these items were not found to be problematic). Cognitive debriefing was carried
out after each test item by means of several questions, and general observations
were documented by the interviewers (Ryan, Gannon-Slater & Culbertson, 2012).
Simple linguistic changes were introduced during the pilot phase and thoroughly
documented. All such changes were made as part of an iterative process of adaptation,
testing, cognitive debriefing, data analysis and discussion in a small expert group
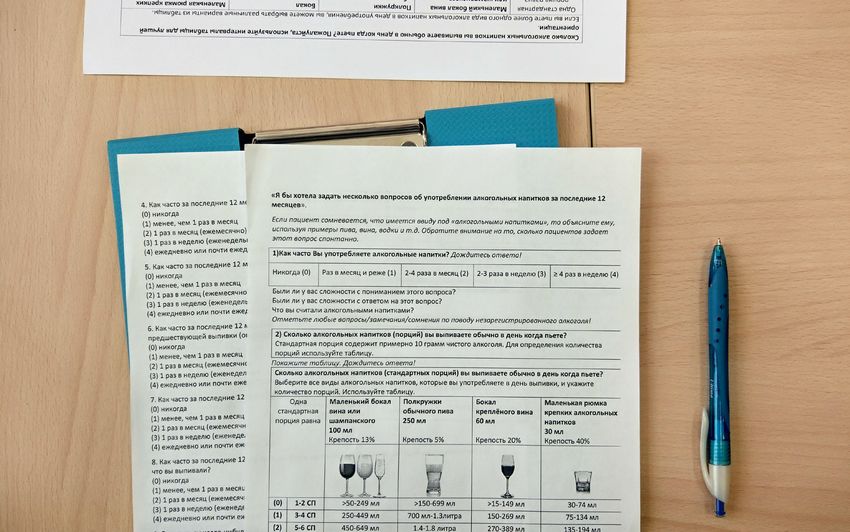
consisting of the interviewers and WHO and national experts. A show card with a
frequency–volume conversion table was developed to assist the interviewer with
standard drink quantification and score calculation as part of the second test item.
Different versions of the show card were tested, including more abstract pictograms
of alcoholic beverages and black-and-white pictures (shown in Annex 3). Overall,
it was found that a coloured show card with realistic (photographic) pictures of
alcoholic beverages worked better as part of the assessment and quantification
because it considerably reduced the reaction times of patients navigating the table
and attempting to recall typical drinking volumes.
A short report of the pilot phase documented all the changes and decisions made, as
well as the main outcomes of each interview, and was then presented to the Project
Advisory Board to inform further decisions.4.4 PANEL DISCUSSION, REVISION AND BROADER
PILOTING OF FINAL FORMS
The revised version of the RUS-AUDIT instrument, based on the results of the pilot
study, was then presented to the Project Advisory Board expert panel and thoroughly
discussed in the course of a one-day meeting (Fig. 1). The instrument was then changed
again, based on the recommendations and suggestions of the advisory board, and
a further round of pilot-testing was initiated, this time encompassing not only pre-
ventive facilities and hospital units but also narcology and polyclinic settings. In
addition to the joint Project Advisory Board expert group, two separate consulta-
tions, restricted to preventive medicine and narcology specialists, were carried out.
13
The revised version was then piloted in the relevant settings in full-study form,
incorporating the other instruments intended for the main validation study, to test
how well the questionnaire that had been developed worked with the target audi-
Translation and adaptation procedures of the AUDIT
ence. The additional phase was organized in a two-step process, using an interim
expert panel and following further adaptation. The first pilot phase was carried out
with 41 patients, 12 of whom were recruited from a general polyclinic in Moscow and
29 from two narcology clinics. It was found that, compared to PHC patients, narcology
patients had greater difficulty understanding the concepts of a “single occasion of
drinking” and a “typical drinking day”; they also struggled to find a suitable frame
in which to recall their drinking behaviours over the past 12 months because most
of their drinking patterns could be characterized as heavy episodic drinking, with
prolonged periods of heavy alcohol intake (the so-called Russian zapoi) followed by
abstention. These problems were not surprising, as the AUDIT was developed as a
screening (not a diagnostic) instrument and therefore behaves differently when used
in clinical populations. At the same time, the results of this pilot phase corroborated the
findings of the qualitative interviews and the systematic research, suggesting that
particular attention needed to be paid to heavy drinking occasions and the specific
nature of drinking patterns as such. Following the work of the interim expert panel,
some changes to the items on heavy episodic drinking were made and a second pilot
phase in the relevant facilities was initiated. This last pilot encompassed a total of
16 patients, 11 from a polyclinic and five from a narcology clinic.
Based on this iterative process, a final version of the RUS-AUDIT was constructed
(Annex 5), which was a paper-and-pencil interview version only, following requests
from the Project Advisory Board representatives. However, it was anticipated that
electronic and auto-administered versions of the tool could be developed and tested
in future pilot studies, based on the experience of the adaptation process described
here.
Fig. 1. The Project Advisory Board and collaborators meeting to discuss
the RUS-AUDIT following revision based on the pilot studyYou can also read