Toronto Central Local Health Integration Network Annual Business Plan: 2018-2019 - Toronto Central LHIN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Toronto Central Local Health Integration Network Annual Business Plan: 2018-2019

Table of Contents
Table of Contents .................................................................................................................................................... 2
1. Context ............................................................................................................................................................. 4
A. Transmittal Letter from the LHIN Board Chair................................................................................................. 4
B. Mandate (confirmation of the LHIN’s mandate) and Strategic Directions ....................................................... 5
C. Alignment with the Priorities of the Minister’s Mandate Letter ........................................................................ 7
D. Overview of the LHIN’s current and forthcoming programs/activities ........................................................... 10
E. Environmental Scan ...................................................................................................................................... 18
2. Health System Oversight and Management ..................................................................................................... 21
2.1 Transparency and Public Accountability...................................................................................................... 21
2.2 Improve the Patient Experience .................................................................................................................. 22
2.3 Build Healthy Communities Informed by Population Health Planning ......................................................... 23
2.4 Equity, Quality Improvement, Consistency and Outcomes-Based Delivery................................................ 26
2.5 Primary Care ................................................................................................................................................ 28
2.6 Hospital and Partners .................................................................................................................................. 29
2.7 Specialist Care ............................................................................................................................................. 32
2.8 Long-Term Care .......................................................................................................................................... 33
2.9 Dementia Care ............................................................................................................................................. 35
2.10 Mental Health and Addictions .................................................................................................................... 37
2.11 Innovation, Health Technologies and Digital Health .................................................................................. 39
3. LHIN-Delivered Home and Community Care .................................................................................................... 41
3.1 Home and Community Care ........................................................................................................................ 41
4. French Language Services (FLS) ..................................................................................................................... 45
5. Indigenous Peoples .......................................................................................................................................... 47
6. Performance Measures .................................................................................................................................... 49
7. Risks and Mitigation Plans ................................................................................................................................ 59
8. LHIN Operations and Staffing Tables ............................................................................................................... 62
Table A: LHIN Spending Plan. .......................................................................................................................... 62
Table B: LHIN Staffing Plan (Full-Time Equivalents or FTE1) ............................................................................. 64
9. Integrated Communications Strategy ................................................................................................................ 66
Business Objectives .......................................................................................................................................... 66
Communications Objectives .............................................................................................................................. 66
Context............................................................................................................................................................... 66
Target Audiences ............................................................................................................................................... 66
Key Messages ................................................................................................................................................... 67
2
Strategic Approach ............................................................................................................................................ 69
Tactics................................................................................................................................................................ 69
Evaluation .......................................................................................................................................................... 70
10. Community Engagement ................................................................................................................................ 72
Appendix A ............................................................................................................................................................ 77
Corporate Snapshot Indicators: ......................................................................................................................... 77
3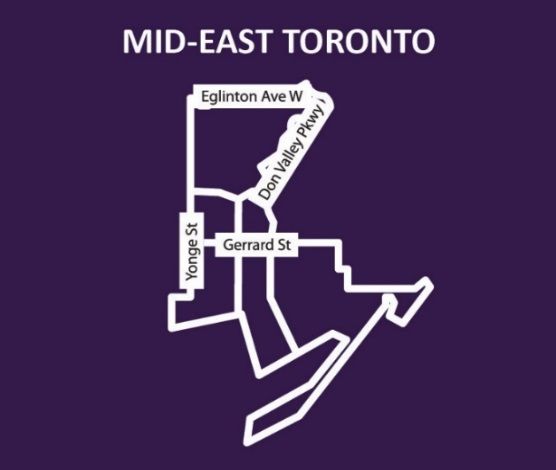
A. Transmittal Letter from the LHIN Board Chair
425 Bloor Street East, Suite 201
Toronto, ON M4W 3R4
Tel: 416 921-7453 • Fax: 416 921-0117
Toll Free: 1 866 383-5446
www.torontocentrallhin.on.ca
March 13, 2018
Dr. Helena Jaczek
Minister of Health and Long-Term Care
10th Floor, Hepburn Block,
80 Grosvenor St,
Toronto, Ontario, M7A 2C4
Dear Dr. Jaczek,
Please find attached the Toronto Central Local Health Integrated Network (LHIN) Annual Business Plan
(ABP) for 2018/19. The ABP sets out how Toronto Central LHIN will operationalize and deliver on the
priorities in the 2018-2019 Integrated Health Service Plan (IHSP- 4) for next fiscal year.
The ABP is an exciting opportunity to plan for the year ahead and outlines the Toronto Central LHIN’s plans
to progress against all strategic priority areas reflected in the 2018/19 Ministers Mandate letter.
Incorporating the planning and delivery of Home and Community Care, the ABP outlines our approach to
engaging and partnering with our citizens, stakeholders and partners to realize our collective goals to
advance the health of our population.
The Toronto Central LHIN remains committed to deliver on our Ministry-LHIN Accountability Agreement
(MLAA) indicators and will continue to progress on achievement of targets and implement opportunities for
improvement.
In 2018/19 the Toronto Central LHIN will continue with our sub-regional planning and sustain our
commitment to building health equity using a population health approach to proactively plan and design a
robust health system. Service provision across the health system will, as always, remain a key priority for
the Toronto Central LHIN and we will continue to evolve the model of care and improve quality outcomes
for our clients and citizens.
Our executive leadership team, along with the LHIN Board of Directors, will provide the leadership and
governance required to deliver our new mandate including the planning, funding and integration of health
services as well as the coordination and delivery of home care services.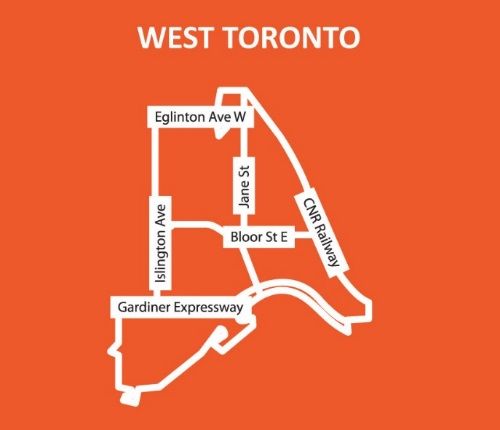
We look forward to the MOHLTC feedback on the plan and to continuing to collaborate with the MOHLTC, other LHINs, and health service providers and communities in Toronto Central LHIN to deliver on the ABP for the people we serve. Sincerely, Dr. Vivek Goel C: Mr. Tim Hadwen, Assistant Deputy Minister, Health System Accountability and Performance Division, MOHLTC 2
B. Mandate (confirmation of the LHIN’s mandate) and Strategic Directions
Toronto Central Local Health Integration Network (LHIN) is one of fourteen (14) local health-planning
organizations that serve Ontario. Toronto Central LHIN is responsible for providing excellent health care for the
1.3 million citizens in our region, as well as care and support for thousands of people who live outside of our
catchment area but access services within the City of Toronto.
Specifically, Toronto Central LHIN manages a system of service-based sectors and individual providers within
the City of Toronto including:
• More than 1,300 Independent Health Facilities, Specialists, Family Practice / General Physicians, and
Diagnostic Imaging Services
• 21 Service Provider Organizations
• 17 Community Health Centres
• 17 Hospitals
• 59 Community Support Service Agencies
• 75 Community Mental Health and Addictions Agencies
• 36 Long-term Care Homes
The passage of the Patients First Act, on December 7th, 2016, was intended to change the experience of the
patient/client/resident/caregiver by strengthening the relationship between primary care/community care and the
health care system, thereby improving access, coordination of care and their ability to navigate the health care
system. Beginning in May 2017, the responsibilities of the Community Care Access Centres were transferred to
the LHINs. And with that transfer, the mandate of Toronto Central LHIN was expanded beyond funding,
planning, implementing and evaluating local health services, to include coordination and delivery of publicly
funded home and community care services.
With a rapidly aging population and an increase in clients with complex medical issues, the scope and role of
home care and community care must evolve. Over the last five years, Toronto Central LHIN has seen a 73%
increase in the proportion of higher needs clients with complex health and chronic conditions. This is a critical
time for the LHIN to consider how home care can be better supported and integrated within the health care
system.
Following the successful transition to one organization in June 2017, Toronto Central LHIN is now directed by
the November 2017 Mandate Letter from the Minister of Health and Long-Term Care, to transform the health
care system and improve the health of citizens in the Toronto Central region. In addition, Toronto Central LHIN
is presently undertaking a strategic planning exercise to focus the direction and goals of the organization over
the coming years to improve patient care and the overall health of the population, in a fiscally responsible
manner.
As outlined in the letter from the minister, the mandate of Toronto Central LHIN is to create an Integrated Health
Service Delivery Network (IHSDN), which includes:
• Primary Care Providers
• Inter-professional Health Care Teams
• Hospitals
• Public Health
• Mental Health and Addictions
• Home and Community Care
Our engagements with patients, health service providers, caregivers, and residents have given us substantial
insights into what is required of us to improve the care experience with a focus on:
• Access
• Navigation / Coordination, and
• Communication
The current Toronto Central LHIN strategic plan expires in 2018. Given Toronto Central LHIN’s change in
6mandate, the strategic plan was modified in 2017/2018 to reflect both legacy organizations in an interim
strategy aligned with Five Strategic Priorities:
• Designing Health Care with Citizens
• Taking a Population Health Approach
• Transforming Primary Health and Community Care
• Achieving Excellence in Operations
• Leading and Supporting Our People
The Annual Business Plan for 2018-2019 is based on our existing strategic priorities and the Minister’s mandate
letter. As we are presently developing our new strategic plan, which will guide Toronto Central LHIN into the
future, our business goals will evolve to align with our new strategy.
C. Alignment with the Priorities of the Minister’s Mandate Letter
In developing this year’s Annual Business Plan, Toronto Central LHIN aligned all activities to the Mandate Letter
received from the Ministry of Health and Long-Term Care on November 24, 2017. The following is a summary of
those activities planned for 2018/19:
Minister’s Mandate Letter Key commitments, goals, actions and/or
Priorities outcomes from the LHIN’s ABP
Transparency and Public Toronto Central LHIN is committed to deliver on our Ministry-
Accountability LHIN Accountability Agreement (M-LAA) indicators for
2018/19. We have developed and continue to evolve our
internal performance management frameworks and
dashboards, which are key tools in providing our leadership
up-to-date information to direct our performance improvement
plans.
Improve the Patient Experience In 2018/19 Toronto Central LHIN’s Citizens’ Panel will
continue to focus on target initiatives defined by the Panel
including integration of the patient/client voice in local
planning, community engagement with a focus on
vulnerable/marginalized populations and implementation of our
LHIN’s Strategic Plan.
The LHIN has also implemented a Patient and Family Advisory
Committee (PFAC) for Home and Community Care to ensure
that our clients’, family members’, and caregivers’ point of
view, perspective, and experience are heard and integrated
into our service and quality improvements.
Build Healthy Communities Toronto Central LHIN believes that good health is more than
Informed by Population Health the absence of disease. In 2018/19, the LHIN will continue our
Planning sub-region planning collaboration, which includes non-health
providers in areas of identified high-need. As well, the LHIN
will continue to improve population health outcomes built on a
foundation of integrated and optimized planning for health and
social service programming and infrastructure. This work will
be enabled by a strategic and operational partnership between
the City and Toronto Central LHIN.
7Minister’s Mandate Letter Key commitments, goals, actions and/or
Priorities outcomes from the LHIN’s ABP
Equity, Quality Improvement, Toronto Central LHIN is taking a population health approach
Consistency and Outcomes-Based to planning at the local level and is committed to health
Delivery equity. This means that the LHIN is using data informed by
community consultation to understand the greatest gaps in
health, and to target efforts and investment. The LHIN
recognizes that many populations require the combined effort
of health and social sectors to develop joined prevention
initiatives, early intervention and targeted interventions in
order to significantly improve their health outcomes.
Primary Care Toronto Central LHIN has established a core network and
mechanisms to engage primary care providers on an ongoing
basis in planning and designing a health system that
incorporates and integrates the primary care sector as
envisioned in the Patients First mandate.
In 2018/19 the LHIN will continue implementation of our
Integrated Primary Care Strategy to strengthen connections
across the system and improve outcomes for patients.
Hospitals and Partners Toronto Central LHIN has a strong hospital network who are
instrumental in our system improvement work. The hospitals
collaboratively work through our LHIN committee structures to
address quality, access and patient experience.
In 2018/19 there will be specific system improvement work
targeting reducing avoidable hospital readmissions in
collaboration with community and primary care.
The LHIN will continue to work with our hospital network to
implement current integrated funding models for bundled care,
and support the identification of new, and innovative models to
support quality, efficiency and effective care.
Specialist Care Access to specialized services is a key strategy to complement
our sub-regional/population health strategy.
Through our primary care, community and hospital partnerships,
Toronto Central LHIN will model a consistent approach and
method to access specialized services for appropriate patients
from Toronto Central LHIN, Greater Toronto Area (GTA) and
across the province.
In partnership with our primary care network we will advance
access to specialized services for providers through the
expansion of Seamless Care Optimizing the Patient Experience
(SCOPE).
8Minister’s Mandate Letter Key commitments, goals, actions and/or
Priorities outcomes from the LHIN’s ABP
Long-Term Care Toronto Central LHIN supports empowering seniors to make
the choices that are right for them when it comes to their care,
their independence, and how they access government
services - whether that's finding ways to keep up an active
lifestyle or getting the support needed to live at home longer.
In 2018/19 the LHIN will continue to prioritize assessing and
building capacity in Long-Term Care to meet the evolving needs
and demands of the system. This includes identifying new,
innovative models of care, leveraging enhanced community
supports and redeveloping existing, and building new beds. This
multi-pronged approach to mitigating capacity limitations is only
possible through partnership with health service providers, the
City of Toronto, and other system leaders.
Dementia Care Toronto Central LHIN will continue efforts which commenced
in 2017/18 aimed at strengthening care delivery and
coordination in long-term care homes, the broader community,
and inpatient settings.
In 2018/19, with the release of the Dementia Strategy, the
LHIN will work to further coordinate and align existing services
to create an integrated, effective client and caregiver-centered
system that addresses a broad range of client needs, across
multiple service delivery settings.
Mental Health and Addictions In 2018/19, the LHIN will continue to focus on community-based
mental health and addictions through the development of
integrated health service delivery networks, targeted initiatives
as part of the Opioid strategy, and coordinated access to
structured psychotherapy and supportive housing.
Innovation, Health Technologies Toronto Central LHIN has developed a Digital Health Strategy
and Digital Health that positions the LHIN and its health service providers to
continue to move forward priority projects from the province in
digital health.
In 2018/19 Toronto Central LHIN will begin the implementation
of a Digital Delivery Centre of Excellence that leverages our
regional and system assets to ensure the capacity and
capabilities to meet the implementation goals and continuous
improvement outlined in the Digital Health Plan.
As well, the work that will continue as part of our Digital Health
Strategy will establish Toronto Central LHIN as leaders and
key influencers in digital health to further accelerate
achievement of our local goals and priorities.
9Minister’s Mandate Letter Key commitments, goals, actions and/or
Priorities outcomes from the LHIN’s ABP
Home and Community Care Shifting funding and support to strengthen community services
is a priority, and it was identified that measuring quality of care
is critical to assessing the impacts.
Toronto Central LHIN will continue to focus on reducing home
and community care wait times by implementing our Right
Place of Care strategy, and identifying opportunities to
improve coordination and consistency with input from patients,
caregivers and partners.
As well, Toronto Central LHIN will continue to work with the
Toronto Central Palliative Care Network to implement the
Ontario Palliative Care Network’s (OPCN) 3-year Action Plan.
D. Overview of the LHIN’s current and forthcoming programs/activities
New LHIN Organization:
Over the past year, Toronto Central LHIN’s role expanded from planning, funding and integrating to include the
delivery of home and community care. The LHIN is leveraging this new role as a service provider to strengthen
integrated and collaborative planning in order to improve outcomes for patients. Our vision for an integrated health
service delivery network includes a full system of care with clear and equitable access for all those who live or
receive services in Toronto Central LHIN. The LHIN’s role can be seen in three parts which are the keys to
unlocking system potential:
1. Creating a strong foundation: it is our role to create one common vision for Toronto Central LHIN, and to
plan a path forward that is based in evidence, aligns with government direction, and responds to what
citizens need
2. Bringing citizens and partners to the table: it is also our role to understand what our citizens need, and
to bring all of our partners together to plan with citizens and local communities
103. Enabling transformation: leveraging our legislative mandate to fund, integrate, performance manage,
and provide high quality home care services.
Primary Care:
Toronto Central LHIN launched a consultation with a broad range of physicians and partners in early 2016 to
inform the development of an integrated Primary Care Strategy. This strategy identified five (5) priorities:
1. Attachment, Access and Continuity;
2. Access to Interprofessional Teams;
3. Discharge Planning;
4. Access to Specialists; and
5. Secure Communications.
Primary Care Clinical Leads (PCCLs) have been recruited into leadership positions in each of our five sub-
regions within Toronto Central LHIN. Their focus is to lead planning and engagement at the system and local
level focused on these five priorities in order to improve patient access, service integration and system
efficiency.
Integrated Home and Community Care:
A move toward integrated community care requires collaboration across many providers, and must be guided by
a shared vision for health service delivery that responds to local needs. Toronto Central LHIN has launched an
integrated community care vision informed by our clients, caregivers, providers, and partners with the following
priorities:
1. Simplified and Coordinated Access to Home and Community-Based Services
2. Improving Capacity and Client Flow
3. Easy Navigation and Care Coordination
4. Common Service Standards
5. Common Assessment and Referral Tools
Strategic Partnerships:
There is a strong commitment to working together between the City of Toronto and Toronto Central LHIN, building
on current relationships and shared initiatives to address Torontonians’ health and well-being. As well, downtown
Toronto is growing four times faster than the City as a whole. There is a recognition of the impact of this urban
growth on the health system and a desire for more a more integrated approach to planning that incorporates joint
11impact assessments to align health services with the needs of the growing population.
Key data sources are available and will be leveraged for enhanced and innovative program planning and delivery.
There are opportunities to expand our effective partnerships to optimize services and outcomes for our shared
public. As well, there are significant opportunities for better, faster, and more coherent decision-making processes
between the City and Toronto Central LHIN. In order to do this, organizations need a better understanding of each
other’s role, mandate and assets.
Recognizing these opportunities, the City of Toronto and Toronto Central LHIN have committed to a sustained
and coordinated strategic partnership that will enable improved service delivery, deliver greater resource
efficiency to support a healthier Toronto. The Partnership Agreement outlines identified areas of joint action,
supported by data-sharing and a structure for joint decision-making.
Population Health and Equity Strategy:
Toronto Central LHIN is taking a population health approach to planning at the local level. This means that the
LHIN is using data, informed by community consultation to understand the greatest gaps in health, and to target
efforts and investment. The LHIN recognizes that many populations require the combined effort of health and
social sectors to develop joined prevention initiatives, early intervention and targeted interventions in order to
significantly improve their health outcomes. For this reason, the LHIN has developed an extensive partnership
table that will provide oversight three key streams of work:
1. Generating tools that will help us understand and stratify the population into smaller groups based on
need and risk.
2. Seeking to develop health equity solutions for particular populations whose health outcomes are
significantly poorer than the broader group.
3. Providing tools to clinicians to help them more effectively serve particular groups of patients and clients.
There are four core components to the Population Health and Equity Strategy that include: Health-Based
Assessment; Health Equity; Practice-Based Population Health; and Strengthening our Partnership with Toronto
Public Health.
Local Collaboratives:
The Toronto Central LHIN has established five sub-regions to serve as the focal point for population-based
planning, service alignment and integration, and performance improvement. Several sessions of Local
Collaborative meetings have brought together more than 280 Health Service Providers, partners and residents
throughout the year to develop a deeper understanding of the local neighbourhoods and populations within each
sub-region.
Over this past year the Local Collaboratives identified priority areas for improvement, informed the development
of a Collaborative Agreement, and delved deeper into data that captured the unique needs of each sub-region at
the neighbourhood level.
A profile of each sub-region has been included below (please note that the neighbourhoods that are split between
two sub-regions are represented in both sub-regions).
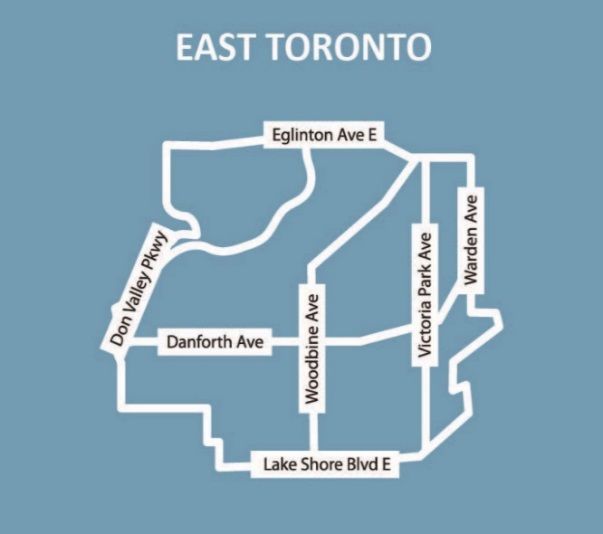
12275,385 residents
21 neighbourhoods
6389.4 people/km2
East Toronto sub-region overview:
• Highest percentage (23.1%) of children and youth (aged 0-19 years) in 2016 among the sub-regions and
compared to Toronto Central LHIN (17.9%).
• Highest percentage (6.7%) of recent immigrants (arrived between 2011 and 2016) compared to the other
sub-regions.
• In 2016, highest percentage of visible minorities (43.0%) compared to the other sub-regions; most heavily
represented visible minorities are South Asian, Chinese and Black.
• Highest marginalization scores compared to other sub-regions
(2011).
• In 2016, a relatively high percentage of the sub-region population
(3.9%) have no knowledge of English or French.
• In 2016, highest percentage (28.3%) of children younger than six
living below the low income measure compared to other sub-
regions. Second highest percentage of overall population
(22.7%) living below the low income measure.
• Four neighbourhoods are estimated to experience more than
20% growth in the next 10-15 years; Clairlea-Birchmount (27%),
Thorncliffe Park (24%), Birchcliffe-Cliffside (23%), and South
Riverdale (21%) while the remaining 17 neighbourhoods are
estimated to have growth less than 15%.
Health status:
• Highest rate of total hospital births for women aged 15-49: 47.7/1000 women (fiscal years 2012/13 to
2014/15).
• Highest number of deaths (1,712) and second highest crude death rate (634.6/100,000 population) among
sub-regions in 2011.
• Highest prevalence rate for all chronic diseases among the sub-regions for 20 years and older (for COPD
35+ years) (fiscal year 2014/215).
Primary care and other health service providers:
• As of March 31, 2017, there were 235 primary care physicians, with 19% practicing in Community Health
Centres or Family Health Teams. Some neighbourhoods have very few (one or two) primary care
physicians.
• Neighbourhoods with the lowest levels of primary care continuity include Thorncliffe Park (27.8%),
Flemingdon Park (24.3%) and Taylor-Massey (23.3%), in fiscal years 2011/12 and 2012/13.
• Michael Garron Hospital is the main hospital in the area. There are also nine Community Support Services,
five Community Mental Health and Addictions agencies and eight Long-term Care Homes.
Health service utilization:
• 27% (25,430) of a total 94,279 Emergency Department visits were of low urgency during fiscal year
2015/16.
• 13.5% of the total number of hospital inpatient days were designated as Alternate Level of Care (ALC).
13158,730 residents
9 neighbourhoods
7247.9 people/km2
Mid-East sub-region overview:
• In 2016, had the smallest land area of all the sub-regions, at 21.9 km2, the smallest sub-region population,
comprising 13% of Toronto Central LHIN and the second highest population density of the sub-regions.
• In 2016, almost 75% of the population were adults aged 20-64. Youth aged 0-19 and seniors aged 65 and
older each make up ~13% of the sub-region.
• In 2016, the most heavily represented visible minorities were Chinese, South Asian and Black.
• Compared to the other sub-regions, had the highest percentage
(3.3%) of those who report French as their mother tongue in 2016.
• Relatively high marginalization scores compared to other sub-
regions (2011).
• Second highest number of homeless shelters in Toronto Central
LHIN (21) (most in Moss Park, and Church-Yonge Corridor) with the
highest number of shelter beds (2,030 beds).
• In 2016, relatively high percentage (24.0%) of population, with the
highest percentages of children under the age of 18 (30.4%) and
seniors aged 65 and older (23.0%), living below the low income
measure compared to other sub-regions.
• Relatively high percentage (6.0%) of recent immigrants (2011-2016)
• In 2016, highest percentage (36.2%) of lone parent families
compared to other sub-regions.
• Four neighbourhoods are estimated to experience extremely high growth in the next 10-15 years: Waterfront
Communities-The Island (125%), Regent Park (117%), Church-Yonge Corridor (106%), and Moss Park
(71%).
Health status:
• Second lowest rate of total hospital births for women aged 15-49: 31.2/1000 (fiscal years 2012/13-14/15).
• Lowest number of deaths (770) and second lowest crude death rate (537.0/100,000 population) among sub-
regions in 2011.
• Particularly high rates for all chronic diseases among the sub-regions for adults 20 years and older.
Primary care and other health service providers:
• As of March 31, 2017, there were 215 primary care physicians, with 55% practicing in Community Health
Centres or Family Health Teams.
• Neighbourhoods with the lowest levels of primary care continuity include Waterfront Communities-The
Island (26.9%), Moss Park (25.4%), and Church-Yonge Corridor (24.9%), in fiscal years 2011/12 and
2012/13.
• Main hospital is St. Michael’s Hospital. Highest concentration of Community Mental Health and Addiction
agencies (23), high number of Community Support Services (15) and four Long-term Care Homes. High
number of health/community providers serving the Indigenous population.
Health service utilization:
• 25.7% (14,437) of total visits to Emergency Department (56,259) were of low urgency in fiscal year 2015/16.
14347,820 residents
19 neighbourhoods
9057.8 people/km2
Mid-West sub-region overview:
• In 2016, Mid-West sub-region had the largest population (28% of Toronto Central LHIN) and the highest
population density compared to other sub-regions.
• From 2011 to 2016, experienced the highest population growth (14%) compared to other sub-regions
• In 2016, nearly three-quarters (74%) of the population were adults aged 20-64. Children aged 0-19 and
seniors aged 65+ each represented 13% of the sub-region population
• Relatively low rate of recent immigrants (4.9%) in 2011-2016.
• In 2016, highest percentage (5.4%) of individuals with no knowledge of English or French compared to other
sub-regions. 2.4% of the population reported French as their mother tongue.
• In 2016, 18.8% of the population living below the low income measure.
• Mid-West had the highest number of homeless shelters in the LHIN (22) (most in Kensington-Chinatown,
followed by Niagara and Annex) with a total of 1,099 beds.
• In 2016, relatively high percentage (33.8%) of lone parent families compared to other sub-regions.
• Three neighbourhoods are estimated to experience high growth in the next 10-15 years: Waterfront
Communities-The Island (125%), Bay Street Corridor (74%), and Kensington-Chinatown (53%).
Health status:
• Lowest rate of total hospital births for women aged 15-49: 30.3/1000 (fiscal years 2012/13 to 2014/15).
• Second highest number of deaths (1,633), but lowest crude death
rate (534.2/100,000 population) among sub-regions in 2011.
• Low prevalence of chronic diseases compared to Toronto Central
LHIN in fiscal year 2014/15. Weston-Pellam Park and Keelesdale-
Eglinton West had remarkably high prevalence across the
neighbourhoods for all diseases.
Primary care and other health service providers:
• As of March 31, 2017, there were 493 primary care physicians, the
highest number per sub-region, with 26% practicing in Community
Health Centres or Family Health Teams.
• High percentage of people with low primary care continuity (21.3%),
with highest rates of low continuity seen in Niagara (29.2%) and
Waterfront Communities-The Island (26.9%) in fiscal years 2011/12
and 2012/13
• Has three academic hospitals (Sinai Health, University Health Network and Women’s College Hospital) and
two specialty hospitals (Centre for Addiction and Mental Health and The Hospital for Sick Children) leading
to high inflow of patients from outside the sub-region.
• High number of Community Mental Health and Addiction agencies (20), Community Support Services (13)
and 12 Long-term Care Homes located in the sub-region. Highest number of hospitals (five) located within
the sub-region
Health service utilization:
25.7% (30,799) of total visits to the Emergency Department (120,034) were of low urgency in fiscal year
2015/16.
15203,700 residents
13 neighbourhoods
5250.0 people/km2
North sub-region overview:
• Highest percentage (16.0%) of seniors older than 65 years in 2016 amongst the sub-regions
• Relatively high percentage (22.0%) of youth (aged 0-19) in 2016 compared to other sub-regions and
Toronto Central LHIN overall (17.9%).
• Low growth rate (2%) between 2011 and 2016.
• Lowest percentage (24.5%) of lone parent families in 2016 compared to other sub-regions.
• 5.7% of the population were recent immigrants (arriving between 2011 and 2016).
• Lowest marginalization scores (2011) compared to other sub-regions.
• In 2016, highest percentage (71.5%) of those who report English as their mother tongue and lowest
percentage (1.2%) of those with no knowledge of English or French.
• In 2016, lowest percentage of population living below the low income measure for all ages (13.0%), for
children younger than six (11.4%), youth younger than 18 (12.0%), and seniors 65 years and older (13.8%).
• 12 (of 13) neighbourhoods are estimated to have growth of 20%
or less in the next 10-15 years while Mount Pleasant West is
estimated to experience growth of 90%.
Health status:
• Rate of total hospital births for women aged 15-49: 36.5/1000
(fiscal years 2012/13 to 2014/15).
• 1,212 deaths with a crude death rate of 608.9 per 100,000
population in 2011.
• Lowest prevalence rates for Diabetes, Mental Health Visits and
chronic obstructive pulmonary disease (COPD) of all sub-regions.
Primary care and other health service providers:
• As of March 31, 2017, there were 215 primary care physicians,
with the lowest percentage (13%) practicing in Community Health
Centres or Family Health Teams.
• Better primary care continuity for enrolled and non-enrolled residents compared to other sub-regions.
Neighbourhoods with the lowest levels of continuity include Humewood-Cedarvale (22.9%), Forest Hill North
(22.4%) and Englemount-Lawrence (22.2%) in fiscal years 2011/12 and 2012/13.
• Three academic hospitals (Sunnybrook, Baycrest and Holland Bloorview), nine Community Support
Services, three Community Mental Health and Addictions agencies and three Long-term Care Homes.
Health service utilization:
• 23.8% (13,373) of total visits to Emergency Departments (56,148) were of low urgency in fiscal year
2015/16.
• 15.6% of the total number of hospital inpatient days were designated as Alternate Level of Care.
16245,490 residents
15 neighbourhoods
4909.8 people/km2
West sub-region overview:
• In 2016, the second highest percentage of seniors aged 65 and older (14.9%) compared to the other sub-
regions.
• Slightly higher percentage of children and youth aged 0-19 in 2016 (18.9%) compared to Toronto Central
LHIN (17.9%).
• In 2016, lowest population density of all sub-regions and the highest land area (50km2)
• Had the lowest percentage (4.4%) of recent immigrants from 2011 to 2016 compared to the other sub-
regions.
• 17.2% of the population, with 19.0% of children under the age of six, 19.2% of youth under the age of 18
and 17.9% of seniors aged 65 and older, living under the low income measure in 2016
• Four neighbourhoods are estimated to have moderate growth in 10-15 years: Islington-City Centre West
(57%), Mimico (57%), High Park North (37%), and Junction Area (27%) while the remaining 11
neighbourhoods are estimated to experience growth of 20% or less.
Health status:
• Second highest rate of total hospital births for women aged 15-
49: 38.8/1000 (fiscal years 2012/213 to 2014/15).
• 1,518 deaths with the highest crude death rate
(652.6/100,000) among sub-regions.
• Slightly higher prevalence of chronic diseases compared to
Toronto Central LHIN. Mount Dennis, New Toronto and
Rockcliffe-Smythe are characterized by high prevalence rates.
New Toronto had remarkably higher rates across all conditions
apart from diabetes (fiscal year 2014/15).
Primary care and other health service providers:
• As of March 31, 2017, there were 187 primary care physicians,
the lowest of all the sub-regions, with 25% practicing in Community Health Centres or Family Health Teams.
• Slightly lower proportion of adults with low primary care continuity (25.9%) compared to Toronto Central
LHIN (26.1%). Neighbourhoods with the lowest levels of continuity include; Rockcliffe-Smythe (24.8%),
Mount Dennis (24.6%) and New Toronto (24.3%) in fiscal years 2011/12 and 2012/13
• Main hospital is St Joseph’s Health Centre, two rehabilitation/complex continuing care hospitals, nine Long-
term Care Homes, eight Community Mental Health and Addictions, and five Community Support Services
agencies.
Health service utilization:
• 28.8% (28,818) of total emergency department visits (100,172) were of low urgency in fiscal year 2015/16.
• 15.7% of the total hospital inpatient days were designated as Alternative Level of Care (ALC).
17E. Environmental Scan
After conducting an environmental scan, Toronto Central LHIN has identified several environmental factors that
impact our business planning for 2018/19.
Environmental Factor Description Implications for Toronto Central LHIN
Political Environment • Provincial politics and emerging • Priorities and direction from the
Ministry direction impact the ministry could change in 2018/19
LHIN’s ongoing business goals
• The LHIN will continue to monitor the
• Activities in the first half of the political landscape and develop plans
fiscal year 2018/19 may impact for any foreseeable changes in health
the LHINs sector priorities
Growing Importance of • In Summer 2017 the Ministry of • Toronto Central LHIN will continue to
Digital Health Health and Long-Term Care work with providers to embrace digital
released a Digital Health Strategy health technologies, monitor the
and Ten Point Action Plan to be impacts of digital health disruption and
aligned with the Patients First identify opportunities where we can be
mandate a leader in adoption to achieve our
business goals
• Toronto Central LHIN has
developed and is implementing a
local Digital Health Strategy that
will define how the organization
will improve the health of our
residents and communities by
ensuring information and tools
are available to support better
care and patient experience
Expanded Mandate and • The Patients First Act was • As the LHIN is impacted by provincial
Responsibilities Related to passed in late 2016 and direction, it is critical that the business
Patients First Act empowers the LHIN with new goals of the organization over the next
responsibilities and a broader year are aligned with the expanded
mandate within the health system mandate from the Patients First Act
and any further direction from the
ministry related to the expanded
powers and responsibility, including
integrating targeted improvements in
home and community care within our
broader strategic planning process
Patient Advocacy • Patients and caregivers are • Toronto Central LHIN will place patient
becoming ever more involved in experience and outcomes at the
their own care and as advocates; centre of our planning and we will
they are asking for the right care, continue to use and expand our
at the right time, in the right place mechanisms to include the patient
voice in all that we do
• While patients may receive
excellent care from individual
care organizations, coordination
and communication across the
system can be improved
18Environmental Factor Description Implications for Toronto Central LHIN
Cross-LHIN Collaboration • Toronto Central LHIN provides • Planning for provision of health care
more services to people living services must be done with a keen
outside of its catchment area than eye to those patients who will return
any other LHIN home outside of this LHIN to receive
their care upon discharge; this
• As many of the large academic requires close collaboration with our
hospitals and regional treatment neighbouring LHINs
centres are located in downtown
Toronto, residents who live • We must recognize the important work
outside of Toronto Central LHIN our regional and provincial resources
will often seek treatment here, play, where these providers are relied
and then return to their own upon to be not only local resources
community for primary and follow- but also care for patients outside of
up care their immediate geography
• Many individuals who live outside
of Toronto Central LHIN, but work
downtown will continue to seek
primary health care services
during the day within the LHIN
Population Health and • Planning across different sectors • Through our sub-region collaborative
Equity is critical to improving the health partners, Toronto Central LHIN has
of the broader population. This identified subsets of the population
means continuing our planning in that have the poorest health outcomes
conjunction with housing, social relative to the rest of the population,
services, justice, emergency and is implementing targeted
responders and many other approaches to improve the health of
partners in the community those specific groups
Community Care • Shifting funding and support to • Toronto Central LHIN is using our
strengthen community services is Regional Quality Table to advance
a priority, and it was identified cross-sectoral priorities for measuring
that measuring quality of care is and improving quality of care
critical to assessing the impacts
• With the LHIN’s expanded mandate,
we must work with our partners to take
full advantage of our position as a
funder, system planner, and now a
service provider to continually find and
execute on opportunities to improve
patient outcome and experience
Voluntary Integration of • Health service providers across • Toronto Central LHIN will continue to
Health Service Providers the LHIN have collaborated with support our health service providers to
one another, and Toronto Central make decisions regarding integration
LHIN, and found opportunities to which support providing excellent
integrate and work more closely patient care and value for the health
together system
• There are examples of these
voluntary, LHIN-supported
integrations across the health
care system within community
and acute care
19Environmental Factor Description Implications for Toronto Central LHIN
Convergence in Health • Moving towards a system of care • As a system funder, integrator,
Care Sector which puts the patient at the performance manager, and service
centre will require leveraging provider, Toronto Central LHIN is well
technologies and capacities from positioned to work with our health
across the health ecosystem service providers and the broader
system to identify opportunities to
continue to evolve value for patients
Population Growth in GTA • The population of the GTA is • The Toronto Central LHIN’s Home and
rapidly growing and Community Care delivery may
simultaneously the proportion continue to see increased demand for
over the age of 70 is increasing services which will need to be
managed through close partnership
with Community Support Services
Increasing Complexity of • There is an ever-increasing • As the complexity of clients served by
Clients in Home and number of patients and citizens Toronto Central LHIN Home and
Community Care who have multiple co-morbidities Community Care increases, we must
and complex health issues have strategies in place to manage
these complex patients and partner
with our service provider organizations
and health service providers to
optimize the use of system resources
Shortage of Personal • There have been reported • We must work with our Service
Support Workers shortages of key healthcare Provider Organizations and
professionals, notably Personal Community Support Service Health
Support Workers, which may Service Providers to understand
impact the delivery of community where there may be limitations to the
services in the LHIN services they can provide due to
staffing shortages and develop
solutions to mitigate and solve these
challenges
We have considered all of this external factors and their implications as we developed our business goals for the
2018/19 fiscal year.
202. Health System Oversight and Management
2.1 Transparency and Public Accountability
Toronto Central LHIN is committed to deliver on our Ministry-LHIN Accountability Agreement (MLAA) indicators
for 2018/19. Throughout the ABP, initiatives have been identified to target specific MLAA indicators which are
listed in Section 6. The LHIN has developed and continues to evolve our internal performance management
frameworks and dashboards, which are key tools in providing our leadership up-to-date information to direct our
performance improvement plans. As well, the LHIN continues to share health system achievements and
performance publicly through our website and through ongoing engagement with our health service providers
(HSP), service provider organizations (SPO) and the community.
Goals:
• Expand public reporting of performance metrics to drive provider excellence in care delivery
• Complete an enterprise review in partnership with Health Shared Services Ontario (HSSOntario) and
develop a work plan to implement recommendations
Government Priorities:
• Continue to be accountable for outcomes and report on your progress towards achieving health system
performance targets
• Collaborate with the ministry to develop performance targets to measure the success of transformational
activities and publicly report on progress and outcomes
• Effectively manage all operational, strategic and financial risks encountered by the LHIN while ensuring
alignment with government priorities and achievement of business objectives
• Work with HSSOntario to complete an enterprise-wide review of the LHINs that identifies opportunities
for improving efficiency and effectiveness, and opportunities for savings that can be reinvested into
patient care.
Action Plan:
Action Plan Expected Status Expected Measurement of Success
by March 2019 Completion Date:
Improve performance of MLAA Ongoing March 31, 2019 Improve performance on MLAA
indicators indicators towards provincial
targets
Operationalize a performance Complete March 31, 2019 Dashboard completed, data
measurement framework for analyzed and reported to the
strategic goals, priorities and Board
organizational performance
Collaborate with LHINs to In progress March 31, 2020 Pan-LHIN performance
develop a pan-LHIN management framework in place
performance management
framework
Participate in Enterprise-Wide Ongoing March 31, 2019 Action plan initiated
review with HSSOntario and
initiate implementation of action
plan
21Risks / Mitigations:
Risk/Barrier Mitigation
Ensuring providers understand and are able to meet Work closely with health service providers to set a
MLAA indicator targets clear strategy for improvement with incremental goals
to improve outcomes over time.
Data may not be available for measurement of (non- Continue to establish databases and data collection
MLAA) indicators methods, increasing the comprehensiveness of data
sources while considering timeliness and quality.
Some programs may deliver additional improvements Work with hospitals, health service, and community
that currently do not fit within our current measurements providers to determine feasible assessment of new
and metrics ventures. Different sources of data will be identified
through partnerships.
2.2 Improve the Patient Experience
Toronto Central LHIN strives to improve the patient, client, and caregiver experience for those who live in, and
receive care, within our catchment area. Through initiatives targeted at ensuring the patient voice and citizen
needs are captured in our planning and delivery of health services, we endeavor to design and support the
implementation of a care system that is informed by patients/clients and caregivers. Our goal is to achieve a
patient experience that is:
• seamless, where transitions are barrier-free across sectors and facilities;
• supported by open and effective communication between patient and provider as well as, across
providers;
• culturally appropriate and culturally competent, and
• inclusive of family and caregivers – across all generations.
In 2017/18 Toronto Central LHIN refreshed our Citizens’ Panel with new membership that reflects our diverse
population and the LHIN’s expanded mandate. Toronto Central LHIN has implemented a Patient and Family
Advisory Committee (PFAC) for Home and Community Care to ensure that our clients’, family members’, and
caregivers’ point of view, perspective, and experience are not only heard, but also integrated into our service
delivery and quality improvements.
In 2018/19 the Citizens’ Panel will continue to focus on target initiatives defined by the Panel including
integration of the patient/client voice in local planning, implementation of our LHIN’s community engagement
strategy with a focus on hearing the voice of our vulnerable or marginalized populations, and implementation of
our LHIN Strategic Plan.
Goals:
• Improve patient experience for clients of Toronto Central LHIN and the citizens of the region through
implementation of the LHINs community engagement strategy
• Include the citizen voice in all appropriate aspects of LHIN’s mandate including planning, funding,
integration and service delivery
Government Priorities:
• Continue to engage the LHIN’s Citizens’ Panel and Home and Community Care PFAC to ensure
patients and families are involved in health care priority setting and decision-making
• Work towards improving transitions for patients between different health sectors and providers so that
patients receive seamless, coordinated care and only tell their story once
• Support patients and families by implementing initiatives that reduce caregiver distress
22Action Plan:
Action Plan Expected Status Expected Measurement of Success
by March 2019 Completion Date:
Continue to strengthen the Complete March 31, 2019 Increase percentage of Citizens’
Citizens’ Panel and Home and Panel members who report
Community Care PFAC satisfaction regarding
engagement by the LHIN
(satisfied or above)
Continue to implement plan for Complete March 31, 2019 Participation of at least one (1)
Community Engagement in Citizen Advisor or Panel Member
Sub-Regions at local sub-region sessions
Embed the client voice in LHIN In progress March 31, 2020 Assignment of at least one (1)
planning and operations Citizen Advisor to identified LHIN
planning and operational
committees
Risks / Mitigations:
Risk/Barrier Mitigation
For patient/client engagement to be effective the Build the capacity for effective patient engagement
LHIN will need to ensure that it is embedded within Toronto Central LHIN, so that the patient/client
throughout the organization. voice is key in shaping our programs, services and
initiatives designed to improve care in the LHIN.
Knowledge of how the health care system works and The LHIN will focus on removing barriers to full
understanding of specific areas of focus such as care engagement through a variety of knowledge building
coordination, hospital readmissions etc. are critical and exchange initiatives.
success factors in enabling citizens to provide input
at all levels of engagement, including up to co-
creation.
2.3 Build Healthy Communities Informed by Population Health Planning
Planning across the health care system has generally been focused on meeting the needs of those actively
receiving health care. Evidence suggests that by adopting a population health approach and by proactively
planning for the health needs of all people, both patients and the system will benefit. In taking this approach, we
are reorienting the work of Toronto Central LHIN towards activities that aim to improve the health status of the
population as a whole, as well as its many sub-populations.
In 2017/18, Toronto Central LHIN hosted Governance-to-Governance (G2G) sessions, which were identified as
part of our work plan in Implementing the Integration Program. This feedback was incorporated into an updated
Integration Strategy to guide engagement, planning, and integration approvals aligned with the LHIN’s
expanded mandate outlined in the Patients First Act 2016.
This updated strategy reflects four key areas of action:
1. Create Integrated Service Delivery Networks (to respond to local needs)
2. Support back-office integration (to build shared capacity)
3. Set standards for services (ensuring positive client/patient experiences and outcomes)
4. Harmonize funding for services (to create equitable funding and strengthen accountability)
23We believe that good health is more than the absence of disease. Reorienting the health care system to take
into consideration the broader social determinants of health that go beyond clinical and curative services is a
major shift, which can only be achieved through long-term strategic partnerships. This includes non-traditional
partnerships with organizations outside the health care system, such as shelters, police, housing, and
employment centres, to work toward addressing the full range of factors that impact health.
In 2017/18, Toronto Central LHIN launched our Population Health and Equity Table with representatives from
across health services, clinicians, Toronto Public Health, academia, research, social services, and Citizens’
Panel members. The Table provided guidance to the LHIN on their work plan focusing on four key areas: Needs
Assessment; Health Equity; Practice-Based Population Health; and Partnership with Toronto Public Health.
This work has resulted in a coordinated response to opioid overdoses in Toronto Central LHIN in partnership
with Toronto Public Health. As well, the LHIN has refreshed our Health Equity Data collection project with Sinai
Health Systems, and developed detailed sub-region demographic and utilization data.
Planning in smaller geographies fosters the ability to focus on specific populations where the data and
community engagement point to the need for tailored strategies and efforts. The local collaborative concept
brings a network of providers together with primary care providers and other partners (e.g. City of Toronto or
Toronto Community Housing) to offer seamless, accessible and integrated services.
The City of Toronto and Toronto Central LHIN have partnered with the collective aim to improve the quality of
life for similar population groups - the City from a social service and delivery view and Toronto Central LHIN
from a health care view. The City of Toronto and Toronto Central LHIN built on our current accomplishments
and close working relationship by establishing an agreement in 2017/18 to support a much closer strategic and
working relationship between both partners well into the future. A joint Steering Committee between the City,
Toronto Public Health and the LHIN has been established to provide oversight and guidance on key priorities
that will improve outcomes for Torontonians.
Goals:
• Strengthen our partnership with the City of Toronto and Toronto Public Health to achieve sustained,
coordinated planning and decision making between the LHIN and the City
• Continue to assess local population health needs, identifying vulnerable populations and high needs
areas for targeted improvements
• Leverage the five sub-region planning areas as the focal point for population-based planning, service
alignment and integration, quality improvement, and partnership building to improve patient experience
and outcomes
Government Priorities:
• With input from patients, providers and partners, assess local population health needs, patient access to
the services they need, wait times and the capacity of health providers to serve the community
• Through sub-region (community level) planning, identify how providers will collaborate to address health
gaps, and improve patient experience and outcomes
• Work with public health and other health care providers to incorporate health promotion strategies in
integrated planning, with a special focus on chronic disease prevention
Action Plan:
Action Plan Expected Status Expected Measurement of Success
by March 2019 Completion Date:
Advance a population-based In progress March 31, 2020 Population-based funding
funding approach at the LHIN framework is defined for sub-
sub-region level regions
24You can also read