Trattamenti dell'ADHD nel bambino - EURAC research
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Psichiatria di Transizione
La complessità dell’ADHD
Bolzano , 5-6 dicembre 2016
Trattamenti dell’ADHD nel bambino
Alessandro Zuddas
Clinica di Neuropsichiatria dell’Infanzia e dell’Adolescenza
Sezione di Neuroscienze e Farmacologia Clinica
Dipartimento di Scienze Biomediche, Università di Cagliari
Ospedale Pediatrico “A. Cao”, AO “G.Brotzu”, Cagliari
AO Brotzu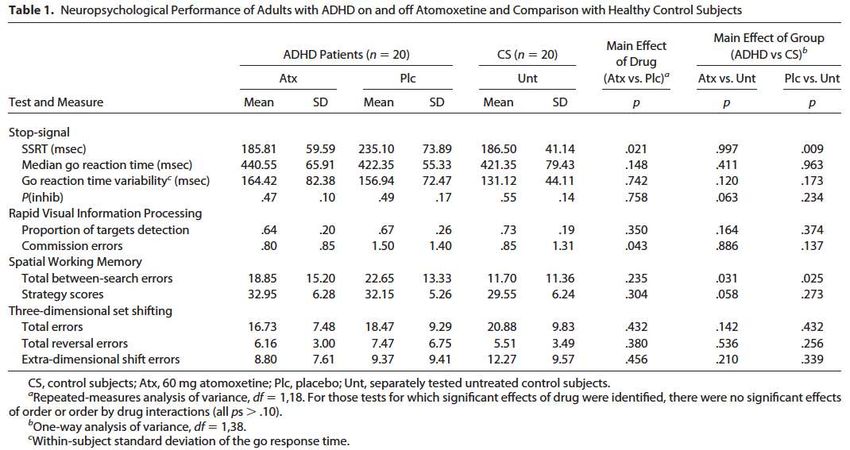
Financial Disclosure (2013-2016)
Research grants
• Shire
• Vifor
• Roche
• Lundbeck
• EU 7 Framework Program (PERS, STOP, ADDUCE, MATRICS)
• AIFA-Farmacovigilanza (Agenzia Italiana del Farmaco),
• Assessorato Sanità Regione Sardegna
Royalties
Giunti.OS, Oxford University Press
Speaker or advisory relationship with:
Angelini, Lilly, Otsuka, Shire, Takeda, Vifor.
Member of Data Safety Monitory Boards
Otsuka, Lundbeck,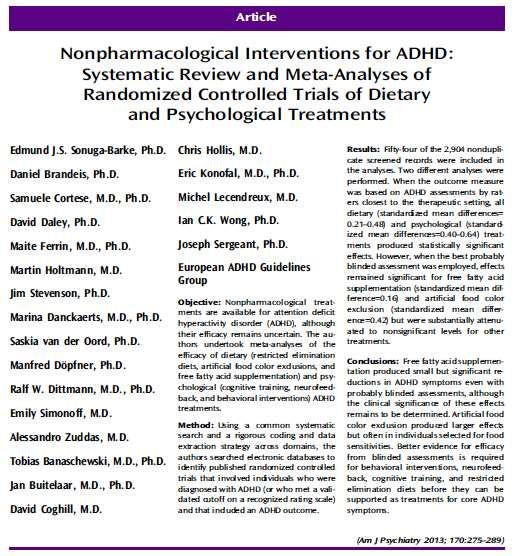
Traditional view
of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) Impairment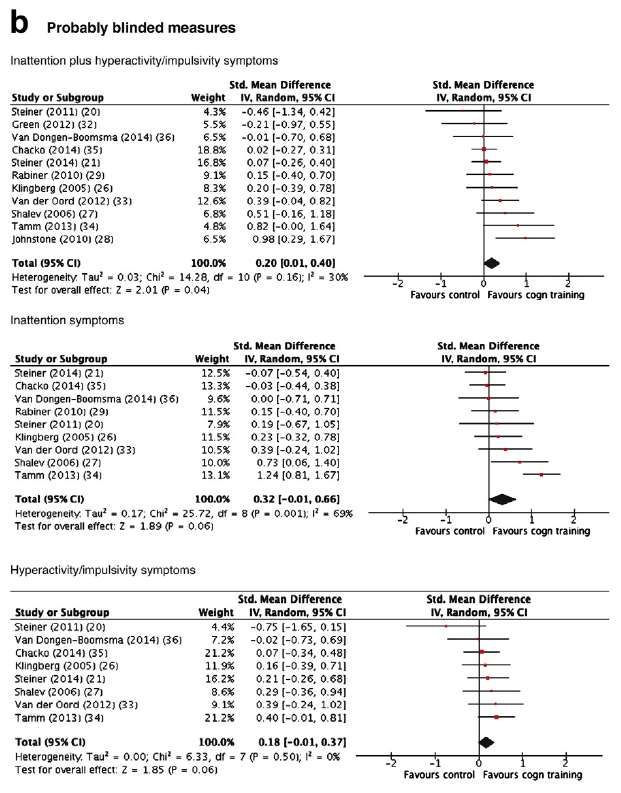
Alternative view
of causal pathway to ADHD
Symptoms
Impairment
Brain Structure
Genes
and Function
Cognition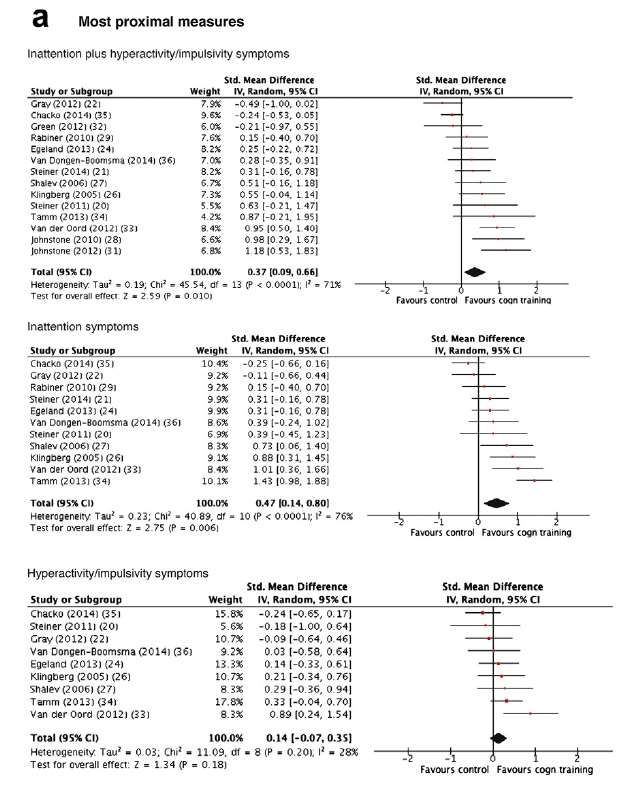
Trattamenti dell’ADHD nel bambino ADHD, executive functions & Neuro-economic models Psychological intervention Effect of Medications Clinical implications
Decision Making: a neuro-economic model
JCPP Sonuga-Barke et al. 2016
ADHD Neuroeconomic Model:
Inefficiency, inconsistency, impulsiveness
Evaluation Decision & Appraisal &
Managemnent Accomodation
Self referential Reducte integrity of DMN interference linked
(Default Mode DMN: impaired to attentional laspes
Network-DMN) prospection
Executive Dorsal fronto-striatal /
fronto-parietal deficits
reduce decision speed &
efficiency
Reinforcement Ventral fronto-striatal Disconnectivity in
deficits impair utility Orbito-frontal Ctx
estimate and with affects computation
Delay adversion in predicting errors ,
produce preference impairing learning
for immediacy
Sonuga-Barke et al. JCPP 2016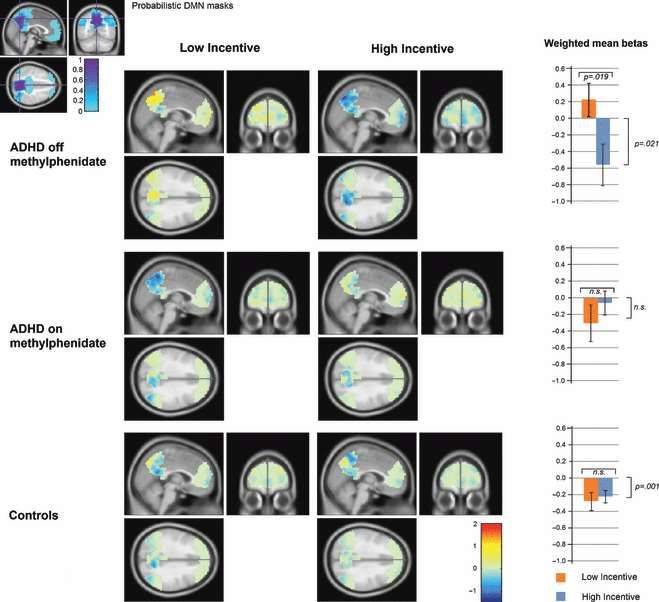
Deficit delle funzione esecutive
nei bambini con disturbo da deficit di attenzione e iperattività
ADHD is an heterogeneous disorder
ADHD & executive functions
Neuro-economic models
Psychological intervention
Effect of Medications
Clinical implications
Inclusion criteria
Age 3-18
Diagnosis ADHD ( any subtype)
Symptom measured by validated rating Scale
Appropriate control group
Stable medication allowed (sensitivity analysis)
Rare comorbidity (i.e. Fragile X) excluded
Outcome measure : ADHD symptoms scale
Most proximal assessment
Probably blinding assessment
Study quality independently assessed
(Jadad et al. criteria for randomization,
blinding and missing data)
Misure di efficacia delle terapie
Effect Size
Differenza nei cambiamenti dal baseline tra due trattamenti (es. farmaco
e placebo), diviso la media delle dev. standard (es. placebo e farmaco ad
end point).
L’effect size standardizza le unità di misura nei diversi studi.
Basaline EndPoint
Farmaco 38.5 + 5.8 25.5 + 4.2
Placebo 40.4 + 6.1 32.7 + 5.0
d= (38.5-25.5) - (40.4-32.7) = 13.0 -7.7 = ES 1.1
(4.2+5.0)/2 4,6
Secondo la definizione di Cohen, ES > 0.2 è considerato basso,
ES > di 0.5 è considerato medio; oltre 0.8 è considerato altoES in General Medicine
Aspirine for prevention cardiovascular disease 0.06
Antypertensive on long term mortality 0.11
ADHD
Corticosteroids for asthma 0.54
Antypertensive for high blood pressure 0.55
Interferone for Chronic Hepatitis C 2.27
ES in General (Adult) Psychiatry
SGA for schizophrenia (PANS) 0.51
SSRI for depression (HAMD) 0.32
SSRI/ Bdz for Panic 0.41
SSRI for OCD 0.44
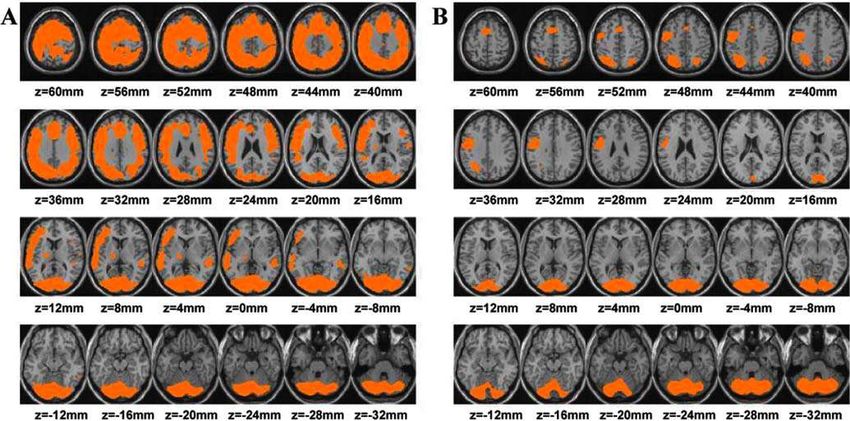
Leucht et al.2012Intervention Most proximal Probably blinding
assessment assessment (SMD)
(SMD)
Restricted Elimination 1.48 0.51
Diet
Artificial food color 0.32 0.42
exclusion
Free fatty acid 0.21 0.16
supplementation
Cognitive training 0.64 0.24
Neurofeedback 0.59 0.29
Behavioral intervention 0.40 0.02
Sonuga-Barke et al. AJP 2013Sonuga-Barke et al. AJP 2013 MPROX PBLIND
Behavioral interventions in attention-deficit/hyperactivity
disorder: a meta-analysis of randomized controlled trials
across multiple outcome domains. Daley et al. JAACAP 2014
Dimension MPROX PBLIND
ADHD 0.35 0.02
Conduct problem 0.26 0.31
Social skills 0.47
Academic Achievement 0.28
Dimension MPROX PBLIND
Positive parenting 0.68 0.63
Negative parenting 0.57 0.43
Parental self-concept 0.37
Parental Mental Health 0.09JAACAP 2015
JAACAP 2015
JAACAP 2015
JAACAP 2015
Deficit delle funzione esecutive
nei bambini con disturbo da deficit di attenzione e iperattività
ADHD is an heterogeneous disorder
ADHD & executive functions
RDoC & neuro-economic models
Psychological intervention
Effects of Medications
Clinical implicationsBiological Psychiatry 2007
Biological Psychiatry 2007
Biological Psychiatry 2009
Trattamenti dell’ADHD nel bambino ADHD, executive functions & Neuro-economic models Psychological intervention Effect of Medications Clinical implications
Pharmacotherapy for ADHD
Antihypertensive
Clonidine
Stimulants
Methylphenidate Antidepressant
Amphetamine compounds Tricyclics
Bupropion
Atomoxetine
Guanfacine Investigational
AcethylCholine (Nicotine) (Chan NPF
2007)
Glutamate: Ampakine
Histamine: H3 antagonists
(Esbenshade BJF 2008)
Serotonine: 5HT 7 Agonists
Omega 3/6More pharmacological treatment options are
available in North America than in Europe
Brands available Ritalin SR
in North America Desoxyn
Adderall Brands available
Adderall XR in Europe
Ritalin LA
Dexedrine spansules
Concerta XL
Dexedrine Intuniv Medikinet
Daytrana Vyvanse/Elvanse
Dextrostat Metadate CD
Methylin ER /Equasym XL Medikinet
Kapvay Strattera XL
Focalin XR Ritalin
Quillivant XR Amphetamine
Focalin Methylphenidate
Methylin
Non-stimulants
Generic dexamphetamine is available in EuropeMore pharmacological treatment options are
available in North America than in Europe
Brands available Ritalin SR
in North America Desoxyn
Adderall Brands available
Adderall XR in Europe
Ritalin LA
Dexedrine spansules
Concerta XL
Dexedrine Intuniv Medikinet
Daytrana Vyvanse/Elvanse
Dextrostat Metadate CD
Methylin ER /Equasym XL Medikinet
Kapvay Strattera XL In Italia
Focalin XR Ritalin
Quillivant XR Amphetamine
Focalin Methylphenidate
Methylin
Non-stimulants
Generic dexamphetamine is available in EuropeStimulants mechanism of action
Methylphenidate Decreased the Amount of Glucose Needed by the Brain to Perform a Cognitive Task Volkow et al., 2008
What is the action of dopamine on
prefrontal cortex ?
Suboptimal D1-receptor activity state Optimal D1-receptor activity state
Optimal signal-to-noise ratio
in interaction with other neurotransmitter systems Nach Seamans et al. J Neurosci 2001Effect of MPH on cognitive tasks
Volkow et al. 2004Volkow & Swanson AJP 2003
Task‐related default mode network modulation
and inhibitory control in ADHD:
effects of motivation and methylphenidate
Liddle et al. 2011Volkow & Swanson AJP 2003
Formulation for extended release:
Osmotic Pump (Concerta XL®) o coated beads (Equasym XL® CD)
Extended Release (ER) MPH
Two ER MPH ER MPH coated beads
Laser-Drilled
reservoirs
Hole
MPH
Compartment
#1
Tablet
MPH Shell
Compartme
nt
#2
Push
Compartme IR MPH overcoat IR MPH uncoated beads
nt
Immediate Release (IR) MPHEfficacia degli interventi per l‘ADHD
Lo studio MTA
Arnold et al. AJP 1997 MTA Cooperative Group
Arch. Gen. Psychiatry 1999EFFICACIA DEGLI INTERVENTI
Normalizzazione sintomatica nello studio MTA
80
68
70
60 56
Percentuale
50
40 34
30 25
20
10
0
Trattamento CBT MED MED + CBT
standardADHD (DSM-IV) vs HKD (ICD-10)
DIAGNOSI SECONDO DSM-IV (ADHD)
Inattenzione + Iperattività/impulsivita ADHD: tipo combinato
ADHD: tipo prevalentemente
Solo inattenzione
inattentivo
ADHD: tipo prevalentemente
Solo iperattività/impulsività
iperattivo/impulsivo
DIAGNOSI SECONDO ICD-10 (HKD)
Inattenzione+ Iperattività + Impulsività Disturbo ipercinetico
+ Disturbo ipercinetico
Disturbo della condotta
della condottaICD-10 DIAGNOSIS
579 ADHD - Combined
Without Anxiety/Depression Anxiety/Depression
432 147
3 Symptom domains Borderline
361 ADHD 71
Pervasive Home -P School -P
161 134 66
Impairment
HKD 145ADHD vs HKD SNAP Hyperactivity-Impulsivity (Parent)
Farmaci non stimolanti:
Atomoxetina
• Inibitore altamente selectivo del
reuptake della Noradrenalina
(Ki=4 nM)
HCl
• Basa affinità per altri siti di CH3
O N
reuptake per altri H
neurotransmettitori. CH3
Kratochvil CJ, et al. J Child Adolesc Psychopharmacol 2001;11:167-70; Michelson D, et al. Pediatrics 2001;108:E83;
Spencer T, et al. J Child Adolesc Psychopharmacol 2001;11:251-65.Atomoxetine mechanism of action
NORADRENERGIC NA
Neuron NA
DOPA DA NA NA
DOPA Dopamina-b R NA R Receptors
decarbossilase idrossilase MAO
NA
Transporter
NA Noradrenaline
DA Dopamine MHPG
DOPA 3,4-diidrossifenilalanine
MAO Monoaminoossidase Presynapsis Post-synapsis
MHP 3-metossi-4-idrossifenilglicole
GDAT DA
Dopamine transporter
HVA
HVA Homovanillic Acid
DA
DOPA DA DA
DOPA R DA R
decarbossilase
MAO
DOPAMINERGIC DAT
Neuron HVAAtomoxetine and Methylphenidate:
Effects on Extracellular Dopamine in
Rat Prefrontal Cortex, Nucleus Accumbens, and Striatum
Methylphenidate Atomoxetine
Prefrontal cortex Prefrontal cortex (3 mg/kg)
Striatum Striatal dopamine (10 mg/kg)
Nucleus accumbens Nucleus accumbens (3 mg/kg)
% Dopamine Baseline
% Dopamine Baseline
350 350
300 300
250 250
200 200
150 150
100 100
50 Methylphenidate 3 mg/kg ip 50
Atomoxetine 1 mg/kg ip
0 0
-1 0 1 2 3 4 -1 0 1 2 3 4
Time (Hours) Time (Hours)
Bymaster FP, et al. Neuropsychopharmacology 2002; 27( 5): 699–711.Dissociable effects of methylphenidate, atomoxetine and placebo on
regional cerebral blood flow in healthy volunteers at rest: A multi-
class pattern recognition approach
Marquand et al. NeuroImage 2012Atomoxetine Relapse Prevention study
Period I Period II Period III
Screening Acute Treatment Double-Blind Relapse Prevention
& Evaluation ATX (n=81)
ATX (n= 292)
atomoxetine placebo (n=82)
(n=604) 40 Wks
placebo (n=124)
1 Wk 10 Wks 2 Wks 58 Wks
J. Buitelaar, M. Danckaerts, C. Gillberg, A. Zuddas, et al.
A prospective, multicenter, open-label assessment of atomoxetine in non-Northern American
children and adolescent with ADHD. Eur. Child Adolesc. Psychiatry, 13: 249-257; 2004
D. Michelson, J. Buitelaar, M. Danckaerts, C. Gillberg,TJ. Spencer, A. Zuddas, D. Faries, S. Zhang, J. Biederman,
Relapse Prevention in Pediatric Patient with ADHD Treated with Atomoxerine: Randomized Double-blind,
Placebo-Controlled Study J. American Acad. Child Adolesc.Psychiatry, 43: 896-904; 2004
J. Buitelaar, D. Michelson, M. Danckaerts, C. Gillberg, T Spences, A. Zuddas, DE Faries, S. Zhang, J.Biederman
A Randomized, Double-Blind Study of Continuation Treatment
for ADHD After One Year Biological Psychiatry, 61: 694-699; 2007Atomoxetine Relapse Prevention study
ATX (n=81)
ATX (n= 292)
atomoxetine
40 Wks placebo (n=82)
(n=604)
placebo (n=124)
1 Wk 10 Wks 2 Wks 58 Wks
50
p < .001
1.0
41,3
40 0.9
0.8
ADHD RS Mean Total Score
30
0.7
0.6
0.5
20
18
0.4
0.3
10
0.2
Proportion Not Relapsing
0.1 Placebo
Atomoxetine
0
Baseline Endpoint 0.0
0 25 50 75 100 125 150 175 200 225 250 275
Buitelaar ECAP 2004 Days to Relapse
Buitelaar Biol.Psych. 2006
Michelson JAACAP 2004MPH-ER vs. ATX
Comparazione diretta
80 P=.423
70 P=.016
P=.026 64%
Percent Responders
60 56% 57% *
51%
50 45% * * ATMX
* OROS® MPH
40 * 37%
Placebo
30 24% 23%
25%
* Significantly
20
different from
10 placebo
0
All Patients Prior Stimulant Users Stimulant Naïve
(N=492) (N=301) (N=191)
Responder: 40% Reduction From Baseline in ADHD RS Total Symptom Score
Michelson, 2004
Based on direct comparisons, reviews by NICE concluded that there is little
difference in efficacy between IR-MPH, ER-MPH, ATXEfficacia: Effect Size
Differenza tra i cambiamenti dal baseline tra farmaco e placebo,
diviso la media delle dev. standard (placebo e farmaco ad end point).
L’effect size standardizza le unità di misura nei diversi studi.
Basaline EndPoint
Farmaco 38.5 + 5.8 25.5 + 4.2
Placebo 40.4 + 6.1 32.7 + 5.0
d= (38.5-25.5) - (40.4-32.7) = 13.0 -7.7 = ES 1.1
(4.2+5.0)/2 4,6
Secondo la definizione di Cohen, ES > 0.2 è considerato basso,
ES > di 0.5 è considerato medio; oltre 0.8 è considerato altoEfficacia
Effect Sizes sui sintomi di ADHD
Parent Teacher Clinician
No. of studies No. of studies No. of studies
SMD (rating scales SMD (rating scales SMD (rating scales References
used) used) used)
Adderall XR 0.9 1 1.1 1 1.2 1 Data on file Shire
Concerta XL 1.0 1 1.0 1 Wolraich et al.
Equasym XL 0.6 2 0.9 1 1.8 1 Greenhill et al.
Swanson et al.
Findling et al.
Medikinet 1.0 1 1.0 1 0.9 1 Döpfner et al.
retard
Ritalin LA 1.0 1 Biederman et al.
ATX 0.7 6 0.7 11 Data on file Eli
Lilly
Modafinil 0.6 3 0.7 3 Data on file
Cephalon
• Effect size = difference in outcome scores between drug and placebo groups divided by the pooled standard deviation
• Caveat: Effect size might be influenced by design features (e.g., different types of rater, durations of studies, dosing regimens)
Effect Size: MPH-IR = MPH-ER (approx 1) > ATX, Modafinil (approx 0.7)Efficacia
Effect Sizes sui sintomi di ADHD
Parent Teacher Clinician
No. of studies No. of studies No. of studies
SMD (rating scales SMD (rating scales SMD (rating scales References
used) used) used)
Adderall XR 0.9 1 1.1 1 1.2 1 Data on file Shire
Concerta XL 1.0 1 1.0 1 Wolraich et al.
Equasym XL 0.6 2 0.9 1 1.8 1 Greenhill et al.
Swanson et al.
Findling et al.
Medikinet 1.0 1 1.0 1 0.9 1 Döpfner et al.
retard
Ritalin LA 1.0 1 Biederman et al.
ATX 0.7 6 0.7 11 Data on file Eli
Lilly
Modafinil 0.6 3 0.7 3 Data on file
Cephalon
• Effect size = difference in outcome scores between drug and placebo groups divided by the pooled standard deviation
• Caveat: Effect size might be influenced by design features (e.g., different types of rater, durations of studies, dosing regimens)
Effect Size: MPH-IR = MPH-ER (approx 1) > ATX, Modafinil (approx 0.7)Efficacia: Number Needed to Treat (NNT)
Percentuale di patienti normalizzati
100 100 Numbers needed to treat =
100% / (% migliorato col
farmaco – % i migliorato
75 con Placebo)
Esempio:
50 Numbers Needed to Treat
= 100 / (75 – 25)
= 100 / 50
=2
25
Maggiore la differenza,
0 0 minore il numero
Active Placebo
treatmentEfficacia (Numbers Needed to Treat)
% normalised % normalised Number needed to
Medication
active med placebo treat (95% CI)
MPH IR 41 20 4.8 (±0.15)
Adderall XR 51 25 3.8 (±0.14)
Concerta XL * 66 14 1.9 (±0.20)
Equasym XL 39 20 5.3 (±0.15)
Medikinet
49 12 2.7 (±0.18)
retard
Atomoxetine 42.3 18.5 4.2 (±0.07)
NNT: MPH-IR = MPH-ER = ATX (c. 3–5)
*Caveat: Normalisation data may be influenced by an inadequate study design (e.g. Concerta
data)JAACAP 2014
JAACAP 2014
Teacher rating of ADHD symptoms
Symptoms ES: 0.77
QoL ES: 0.87
No risk for
serious adverse events
RR: 0.98
Minor risk for
non-serious adverse events
RR: 1.29ES in General Medicine
Aspirine for prevention cardiovascular disease 0.06
Antypertensive on long term mortality 0.11
Corticosteroids for asthma 0.54
Antypertensive for high blood pressure 0.55
Interferone for Chronic Hepatitis C 2.27
ES in General Psychiatry
SGA for schizophrenia (PANS) 0.51
SSRI for depression (HAMD) 0.32
SSRI/ Bdz for Panic 0.41
SSRI for OCD 0.44
Leucht et al.2012Efficacia a lungo termine delle terapie
Normalizzazione sintomatica nello studio MTA
80
68
70
60 56
Percentuale
50
40 34
30 25
20
10
0
Trattamento CBT MED MED + CBT
standardEfficacia a lungo termine delle terapie (studio MTA)
Sintomi di ADHD
2,5
2
Comb
1,5
Med
Beh
1
CC
0,5
0
0 1 2 3
Years Jensen et al. JAACAP 2007EFFICACIA DEGLI INTERVENTI
Diagnostic Status
ADHD ODD
120 120
100 100
80 80 Comb
Med
60 60
Beh
40 40 CC
20 20
0 0
0 1 2 3 0 1 2 3
Jensen et al. JAACAP 2007Percentuale di bambini che assumevano farmaci
nelle diverse fasi dello studio MTA
Years
Treatment 0 1 2 3
Comb 20 90 70 71
Med 22 90 70 71
Beh 19 14 35 43
CC 20 60 62 62
Jensen et al. JAACAP 2007MTA study follow up Jensen et al. JAACAP 2007
ADHD ODD
Symtoms
1,6
2,5
1,4
2 1,2
Comb 1 Comb
1,5 Med
Med 0,8
Beh Beh
1 0,6 CC
CC
0,4
0,5
0,2
0 0
0 1 2 3 0 1 2 3
Diagnostic status
120 120
100 100
80 80 Comb
60 Med
60
Beh
40 CC
40
20
20
0
0 1 2 3 0
0 1 2 3Secondary evaluation of MTA 36-month outcome:
propensity score and growth mixed model analysis
ADHD: SNAP score
2,5
2
Class 1
1,5
Class 2
Class 3
1
LNCG
0,5
0
0 1 2 3
Years
Swanson et al. JACAAP 2007Secondary evaluation of MTA 36-month outcome: propensity
score and growth mixed model analysis
Swanson et al. JACAAP 2007Secondary evaluation of MTA 36-month outcome: propensity
score and growth mixed model analysis
Swanson et al. JACAAP 2007Secondary evaluation of MTA 36-month outcome: propensity
score and growth mixed model analysis
Swanson et al. JACAAP 2007The MTA at 8 Years: Prospective Follow-up of Children
Treated for Combined-Type ADHD in a Multisite Study
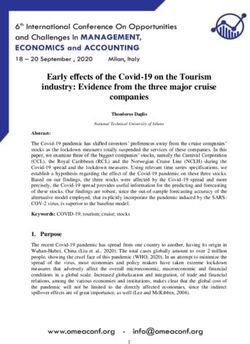
Molina et al. JACAAP 2009Nakao et al. AJP 2011
November 22, 2012 Vol. 367 No. 21
Change in executive functioning (planning and
set shifting) over a four year period
E.S.
7
Planning ADHD
9,5
* 1.4
(Stockings of
Cambridge) 6,9
Controls * 1.1
8,9
6,9
ADHD * 1.7
8,1
Set Shifting
(ID/ED) 7,8
Controls * 1.0
8,9
0 2 4 6 8 10
ADHD Time 1 ADHD Time 2
Controls Time 1 Controls Time 2
Coghill et al 2013 Psychological MedicineChange in executive functioning (spatial working
memory) over a four year period E.S.
56,6
Spatial ADHD * 1.1
33,5
Working
Memory
(Between 47,9
Search Errors) Controls 29
* 1.0
37,2
ADHD * 0.7
33,8
Spatial
Working
34,9
Memory Controls * 0.4
(Strategy 32,6
Score)
0 10 20 30 40 50 60
ADHD Time 1 ADHD Time 2
Controls Time 1 Controls Time 2
Coghill et al 2013 Psychological MedicineChange in non executive functioning
(recognition memory) over a four year period
E.S.
Delayed 60
ADHD 75,7 * 0.9
Matching to
Sample 0.8
(% correct)
Controls 71
*
84,1
80,4
Pattern ADHD 92,4 * 0.9
Recognition
(% correct) Controls 88,5
90,4
66,5
Spatial ADHD 68,2
Recognition
72,9
(% correct) Controls 79,7 * 0.6
0 20 40 60 80 100
ADHD Time 1 ADHD Time 2
Controls Time 1 Controls Time 2
Coghill et al 2013 Psychological MedicineLisdexamfetamina (LDX)
O CH3 O
H2 N H 2N
N OH CH 3
H
+ H2 N
Site of Cleavage
NH2 NH 2
NRP104 l-lysine d-amphetamineLysdexamfetamine: change in ADHD-RS-IV total score
LDX Placebo OROS-MPH
(n = 104) (n = 106) (n = 107)
50
Full analysis set
40 N = 317
ADHD-RS-IV total score
30
20
10
40.7 16.0 41.0 34.8 40.5 21.7
0 −24.3 −5.7 −18.7
−10
−20
−30
p < 0.001 p < 0.001
Baseline (mean ± SD) Effect size: 1.80 Effect size: 1.26
Endpoint (mean ± SD)
LS mean change (± SE)
p-values and effect sizes are from an ANCOVA model of the change in ADHD-RS-IV total score from baseline
to endpoint. ANCOVA, analysis of covariance; SD, standard deviation
Coghill et al. ENP 2013JAACAP 2014
Maintenance of efficacy of lisdexamfetamine dimesylate in
children and adolescents with attention-deficit/hyperactivity
disorder: randomized-withdrawal design Coghill et al. JAACAP 2014
Primary Outcome
relapses during the randomized withdrawn
100 Randomized full
Cumulative proportion of
treatment failures (%)
analysis set
80
60
40
20 ***
0 V4R V5R V6R V7R V8R V9R Endpoint
W27 W28 W29 W30 W31 W32
***p < 0.001 active drug versus placebo
≥ 50% increase in ADHD-RS-IV total score and a ≥ 2 point increase in Clinical Global
Impressions-Severity rating relative to visit 3R. Endpoint was the last on-treatment,
post-baseline visit of the randomized-withdrawal period (V4R–V9R) with a non-
missing assessmentQuality of Life in the LDX relapse prevention study
mean T-scores at baseline and endpoint of both periods
50 Open label (≤ 26 weeks) Randomized withdrawal (6 weeks)
40 LDX (n = 262) LDX (n = 76) Placebo (n = 77)
30
Baseline Endpoint Baseline Endpoint Baseline Endpoint
Achievement 30.2 38.9 39.6 40.1 41.2 35.3
Risk Avoidance 32.3 44.1 45.8 47.5 46.8 41.3
Resilience 36.8 40.5 42.0 43.3 42.6 40.2
Satisfaction 35.5 40.3 41.9 44.9 43.3 39.3
Comfort 44.5 49.4 51.0 51.1 51.1 48.5The cognitive function of children and adolescents with ADHD
in a two-year open-label study of lisdexamfetamine dimesylate
N= 314 (6-17y); LDX 51.1 mg/day (+14.3)
Delayed Matching to Sample (Stop Signal Task [SST]& Reaction Time[RTI])
Spacial working memory
Coghill, Banschewski, Bliss, Robertsone , Zuddas (in preparation)Trattamenti dell’ADHD nel bambino ADHD, executive functions & Neuro-economic models Psychological intervention Effect of Medications Clinical implications
Traditional view
of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) ImpairmentAlternative view
of causal pathway to ADHD
Symptoms
Impairment
Brain Structure
Genes
and Function
CognitionPredictions arising
from the traditional view of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) Impairment
If cognition and symptoms are causally linked in a linear manner it
would expect that:Predictions arising
from the traditional view of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) Impairment
If cognition and symptoms are causally linked in a linear manner we
would expect that:
When a treatment improves cognition it will also reduce symptomsPredictions arising
from the traditional view of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) Impairment
If cognition and symptoms are causally linked in a linear manner we
would expect that:
When a treatment improves cognition it will also reduce symptoms
When a treatment reduces symptoms it will also improve cognitionPredictions arising
from the traditional view of causal pathway to ADHD
Genes & Brain Structure Cognition Symptoms and
Environment and Function (executive functions) Impairment
If cognition and symptoms are causally linked in a linear manner we
would expect that:
When a treatment improves cognition it will also reduce symptoms
When a treatment reduces symptoms it will also improve cognition
If symptoms decline over time, this would be associated with a
similar improvement in cognitionEnvironmental
Factors
Cognitive training
X
Brain Structure
Genes Cognition Symptoms
and Function
IMPROVES
(some aspects of)
X REDUCES
MedicationsClinical Implications Symptoms
Impairment
Brain Structure
Genes
and Function
Cognition
The core symptoms of ADHD – as defined in the diagnostic systems-
may not be a full description of what it means to have ADHDClinical Implications Symptoms
Impairment
Brain Structure
Genes
and Function
Cognition
Treatments that reduce core ADHD symptoms may not also improve
cognition and there may be residual ADHD related impairments.Clinical Implications Symptoms
Impairment
Brain Structure
Genes
and Function
Cognition
Treatments that reduce core ADHD symptoms may not also improve
cognition and there may be residual ADHD related impairments.
Treatments that improve cognitive aspects of ADHD may not also
improve core ADHD symptoms (but may reduce impairment).Clinical Implications Symptoms
Impairment
Brain Structure
Genes
and Function
Cognition
Treatments that reduce core ADHD symptoms may not also improve
cognition and there may be residual ADHD related impairments.
Treatments that improve cognitive aspects of ADHD may not also
improve core ADHD symptoms (but may reduce impairment).
As a consequence both treatments may be required.Take home message ADHD is an heterogeneous disorder Executive dysfunction do NOT always explain ADHD symptoms and impairment Neuro-economic models (dysfunction of executive, default, reward and time perception systems) may be more useful to explain ADHD psychopathology Treatments that specifically reduce core ADHD symptoms or only improve cognitive aspects of ADHD, may not be effective to completely normalize ADHD-related impairment Both symptoms and cognition treatment approaches may be required
Grazie per l’attenzione
azuddas@unica.itYou can also read