Trauma-Informed Care - Pediatrics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
Trauma-Informed Care
Heather Forkey, MD, FAAP,a Moira Szilagyi, MD, PhD, FAAP,b Erin T. Kelly, MD, FAAP, FACP,c James Duffee, MD, MPH, FAAP,d
THE COUNCIL ON FOSTER CARE, ADOPTION, AND KINSHIP CARE, COUNCIL ON COMMUNITY PEDIATRICS, COUNCIL ON CHILD ABUSE
AND NEGLECT, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH
Most children will experience some type of trauma during childhood, abstract
and many children suffer from significant adversities. Research in a
Department of Pediatrics, University of Massachusetts, Worcester,
genetics, neuroscience, and epidemiology all provide evidence that Massachusetts; bDivisions of General and Developmental-Behavioral
these experiences have effects at the molecular, cellular, and organ Pediatrics, Department of Pediatrics, University of California, Los
Angeles, Los Angeles, California; cAmbulatory Health Services,
level, with consequences on physical, emotional, developmental, and Philadelphia Department of Public Health, Philadelphia, Pennsylvania;
behavioral health across the life span. Trauma-informed care translates and dDepartments of Pediatrics and Psychiatry, Boonshoft School of
that science to inform and improve pediatric care and outcomes. To Medicine, Wright State University, Dayton, Ohio
practically address trauma and promote resilience, pediatric clinicians Drs Forkey, Szilagyi, Kelly, and Duffee were equally responsible for
conceptualizing, writing, and revising the manuscript and
need tools to assess childhood trauma and adversity experiences as considering input from all reviewers and the Board of Directors;
well as practical guidance, resources, and interventions. In this clinical and all authors approved the final manuscript as submitted.
report, we summarize current, practical advice for rendering trauma- This document is copyrighted and is property of the American
Academy of Pediatrics and its Board of Directors. All authors have
informed care across varied medical settings. filed conflict of interest statements with the American Academy of
Pediatrics. Any conflicts have been resolved through a process
approved by the Board of Directors. The American Academy of
Pediatrics has neither solicited nor accepted any commercial
involvement in the development of the content of this publication.
INTRODUCTION
Clinical reports from the American Academy of Pediatrics benefit
Experiences in childhood, both positive and negative, have a significant from expertise and resources of liaisons and internal (AAP) and
external reviewers. However, clinical reports from the American
effect on subsequent health, mental health, and developmental Academy of Pediatrics may not reflect the views of the liaisons or
trajectories. For many children and adolescents, traumatic experiences the organizations or government agencies that they represent.
are all too common. Almost one-half of American children, or 34 million The guidance in this report does not indicate an exclusive course
younger than 18 years, have faced at least 1 potentially traumatic early of treatment or serve as a standard of medical care. Variations,
taking into account individual circumstances, may be appropriate.
childhood experience.1–7 Such traumas may include those originating
All clinical reports from the American Academy of Pediatrics
outside the home, such as community violence, natural disasters, automatically expire 5 years after publication unless reaffirmed,
unintentional injuries, terrorism, immigrant or refugee traumas revised, or retired at or before that time.
(including detention, discrimination,6,8,9 or racism), and/or those DOI: https://doi.org/10.1542/peds.2021-052580
involving the caregiving relationship, such as intimate partner violence, Address correspondence to Heather Forkey, MD. E-mail:
parental substance use, parental mental illness, caregiver death, heather.forkey@umassmemorial.org
separation from a caregiver, neglect, or abuse, originally defined as PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
adverse childhood experiences (ACEs).10 For many children, medical
events, such as injury, medical procedures, and/or invasive medical
treatments, can be traumatic. Given the robust science explaining the To cite: Forkey H, Szilagyi M, Kelly ET, et al. AAP COUNCIL ON
FOSTER CARE, ADOPTION, AND KINSHIP CARE, COUNCIL ON
physiologic consequences of accumulated trauma experiences on the COMMUNITY PEDIATRICS, COUNCIL ON CHILD ABUSE AND
brain and body,11–14 there have been calls for pediatric clinicians to NEGLECT, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND
address childhood trauma and child traumatic stress.10,14–16 However, FAMILY HEALTH. Trauma-Informed Care. Pediatrics.
2021;148(2):e2021052580
Downloaded from www.aappublications.org/news by guest on October 11, 2021
PEDIATRICS Volume 148, number 2, August 2021:e2021052580 FROM THE AMERICAN ACADEMY OF PEDIATRICSpractical guidance about how to services. TIC can be conceptualized in processes for referral to counsel-
consider, address, and operationalize a public health stratification, as ing with evidence-based thera-
this care, although necessary, has summarized in Table 1: pies when indicated; and
been insufficient. attention to the prevention and
primary prevention of trauma
treatment of STS and associated
Pediatric clinicians are on the front and promotion of resilience;
sequelae.
lines of caring for children and secondary prevention and interven-
adolescents and, thus, have the tion for those exposed to potentially Pediatricians have a powerful voice
greatest potential for early traumatic experiences, including and reach that could promote the
identification of and response to caregivers, siblings, guardians, and policies and procedures necessary to
childhood trauma. Data indicate health care workers; and transform pediatric health care into
that, although pediatric providers tertiary care for children who
a TIC system. This guidance for
intuitively understand the negative display symptoms related to
pediatric clinicians is organized
effects of trauma, they report a lack traumatic experiences.
around 5 strategies for
of knowledge, time, and resources as implementation to become trauma
major barriers to providing trauma- This clinical report and the
informed: awareness, readiness,
informed care (TIC).5,6 Yet, experts accompanying policy statement19
detection and assessment,
believe that the complete address secondary prevention and
management, and integration. The
assessment of child and adolescent intervention: practical strategies for
companion policy statement19
behavioral, developmental, identifying children at risk for
outlines broad recommendations for
emotional, and physical health trauma and/or experiencing trauma
implementing TIC in child health
requires consideration of trauma as symptoms. “Children,” unless
systems.
part of the differential diagnosis to otherwise specified, refers to youth
improve diagnostic accuracy and from birth to 21 years of age. These
appropriateness of care.17,18 clinical strategies and skills include
the following16,20:
AWARENESS
TIC is defined by the National Child
Traumatic Stress Network as medical knowledge about trauma and its Pediatric clinicians can promote
care in which all parties involved potential lifelong effects; resilience, identify adversity and
assess, recognize, and respond to the support for the caregiver-child trauma, and ameliorate the effects of
effects of traumatic stress on children, relationship to build resilience adversity in their work with
caregivers, and health care providers. and prevent traumatic stress children and families. Although the
This includes attention to secondary reactions; epidemiology and physiology of
traumatic stress (STS), the emotional screening for trauma history and trauma have been explored in the
strain that results when an individual symptoms; literature,9,12,13,21,22 few concepts
hears about the first-hand trauma recognition of cultural context of have been translated into the
experiences of another. In the clinical trauma experiences, response, provision of practical TIC in
setting, TIC includes the prevention, and recovery; pediatric settings.6,16,23 Awareness
identification, and assessment of anticipatory guidance for families of the science and epidemiology of
trauma, response to trauma, and and health care workers; trauma provides the scientific
recovery from trauma as a focus of all avoidance of retraumatization; grounding for the practices of TIC.
TABLE 1 Range of Trauma Experiences, Symptoms, and Response
Potentially Traumatic Experiences Trauma Symptoms (Table 5) Office Response
None None to some Primary prevention: anticipatory guidance; resilience promotion
Single-incident or minor trauma None or latent or mild Secondary prevention: anticipatory guidance; resilience promotion; trauma-
informed guidance; close monitoring: screen for trauma history and symptoms
Major event or cumulative Mild to moderate Secondary and tertiary prevention: anticipatory guidance; resilience
promotion; psychoeducation; trauma-informed guidance, close monitoring,
and follow-up; possible referrals to community services, mental health
Major event or cumulative Moderate to severe Tertiary prevention and treatment: anticipatory guidance; resilience promotion;
psychoeducation; trauma-informed guidance, close monitoring, and follow-up;
avoidance of retraumatization; referrals to community services; referral to
evidence-based and evidence-informed trauma mental health services
Adapted from Forkey H, Griffin J, Szilagyi M. Childhood Trauma and Resilience: A Practical Guide. Itasca, IL: American Academy of Pediatrics; 2021.
Downloaded from www.aappublications.org/news by guest on October 11, 2021
2 FROM THE AMERICAN ACADEMY OF PEDIATRICSFROM THE AMERICAN ACADEMY OF PEDIATRICS
Safe, Stable, and Nurturing manage stressful experiences. events that may be long lasting,
Relationships Physiology, in addition to severe in intensity, or frequent in
The most fundamental adaptational psychology, is affected by protective occurrence. The available caregiver
mechanism for any child is a secure relationships.14,25–27 support is insufficient to turn off the
relationship with a safe, stable, body’s stress response. It is critical
Toxic Stress and Trauma
nurturing adult who is continuous to note that the toxic stress
over time in the child’s life.24 This is All children experience some stress response has 2 components: the
usually the child’s parent or and adversity at some point in life, significant stressors and the relative
caregiver but can involve extended but when it is managed within the insufficiency of protective
family and biological or fictive kin. It context of these nurturing relationships. In sum, there is a
is in the protective context of this relationships, such events can be marked imbalance between
secure relationship that the child weathered and even used for stressors and protective factors.28
develops the varied resilience skills growth. Adverse events that lead to
that will prevent or ameliorate the the frequent or prolonged activation Toxic stress responses can result in
effects of cumulative adversities. of the stress response (see Fig 1) in potentially long-lasting or lifelong
The nurturing caregiver protects the the relative absence of protective impairments in physical and mental
child from harm, mediates the world relationships has been termed “toxic health through biological processes
for the child, and helps the child to stress” in the pediatric literature.14 that embed developmental, neurologic,
develop the adaptive skills to Toxic stress responses result from epigenetic, and immunologic
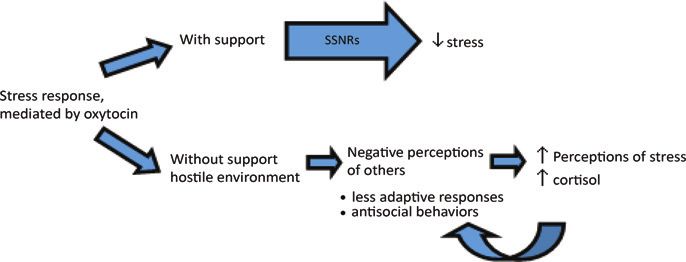
Stress Responses
Freeze • Originates in central nucleus of the amygdala and mediated by
hypothalamus and superior colliculus222
• Typically brief response, forces the organism to alert to danger
• Can be followed by the fight-or-flight responses
• Parasympathetic and vagal response can lead to dissociation or faint
Fight or flight • Results from adrenal release of epinephrine and cortisol that allow the
threat to be addressed
• Short term: physiological changes, including increased heart rate and
blood pressure
• Excess or frequent activation in childhood can result in long-term
changes in HPA axis function, which leads to dysregulation of the
neuroendocrine stress response and consequent physiologic changes
(see Table 2)12,223
Affiliate (gather • Higher brain response mediated by oxytocin,224,225 appears to mediate
social support, stress within the social context by promoting the ability to look to
“tend and others in the environment for support in managing a threat (social
befriend”) salience)70,226
• With the provision of support, stress response declines 70,227
• Having no support or a hostile environment leads to negative perceptions
of others, induces less adaptive responses and antisocial behaviors, and
70,228-230
leads to increased perception of stress and increased cortisol
• Emerging science underlying the affiliative response elucidates how
safe, stable, nurturing relationships can buffer adversity and promote
resilience
Without support or in a
C
Less
A
FIGURE 1 Stress responses. HPA, hypothalamic-pituitary-adrenal.
PEDIATRICS Volume 148, number 2, Downloaded
August 2021 from www.aappublications.org/news by guest on October 11, 2021 3TABLE 2 Physiologic Effects of Trauma in Children
Area Impact Specifics Implications and Associations
93
Brain connectivity Cortisol acts on rapidly Amygdala overactive; hippocampus Preliminary association with more
developing brain underactive; prefrontal cortex not severe clinical course in major
structures accessible depressive disorder
Epigenetic changes21 Methylation patterns Methyl groups attach to promoter region or Adult stress and reactivity behavior231,232
impacted by threat, come off promotor regions of genes,
mediated by cortisol leading to the transcription or lack of
transcription of genes
Immune function80 Alteration of immune Inflammatory system up-regulated; humoral Symptoms including the following:
system in response to immunity diminished; cytokine-induced decreased appetite, fatigue, mood
constant threat “sickness behavior”81 (feeling sick) changes including depression and
irritability, poor cognitive function
changes.12,14 The lifelong effects of derived from this literature is more likely to be exposed to
toxic stress are statistically related to important in appreciating the scope, discrimination.45,46 The
many adult illnesses, particularly those variety, and nuances of TIC and how psychological, interpersonal, and
related to chronic inflammation, and to actualize them. These are perhaps physiologic effects of
causes for early mortality.29 The summarized in Table 3. trauma inflicted on a community
robust literature on the physiologic (particularly because of race,
High-risk Populations identity, or ethnicity) may be passed
effects of toxic stress is beyond the
scope of this clinical report yet briefly It is important to be aware that the to succeeding generations and is
summarized in Table 2. exposures of some child populations referred to as historical trauma.47,48
and their families put them at Community violence and bullying,
Trauma is a broader term used to particular risk of experiencing along with cyberbullying, are
describe both a precipitant and a trauma but also that the experienced by many children and
human response. The Substance components of TIC can benefit these recognized as traumatic exposures
Abuse and Mental Health Services children and families.31–34 More included in expanded definitions of
Administration defines trauma as an than 7.4 million children, or nearly 1 ACEs.49–51 Lesbian, gay, bisexual,
event, series of events, or in 10 children, are reported as transgender, and queer children and
circumstances experienced by a potential victims of child abuse and adolescents, children of color,
person as physically or emotionally neglect annually.35 In 2019, more American Indian and Alaskan native
harmful that have long-lasting than 670 000 children spent time in children, immigrant children,
adverse effects on the person’s foster care.36 Children who remain neurodiverse children and
functioning and well-being at home after child protective adolescents, and children and
(emotional, physical, or spiritual).16 services investigation or are moved adolescents with overweight
This definition accounts for the fact to kinship care resemble their peers and obesity are all more likely to
that people may respond differently in foster care in having an extremely experience discrimination, both
to potentially traumatic events and high prevalence of significant overt and as a series of
informs TIC with appreciation that childhood trauma.37–39 Immigrant microaggressions (small slights,
the traumas people experience can and refugee children may have left insults, or indignities either
result in behavioral changes that poverty, war, and violence, may intentional or unintentional) that
may allow them to manage the have encountered abuse or accumulate over time.52–54
trauma in the short-term but can separation from family members, Additionally, children of military
have lasting negative effects on and can be at risk for deportation, families have a higher prevalence of
conduct. These difficulties should detention, and separation and trauma, abuse, grief, and loss.55
not be viewed as malicious actions discrimination.6,40,41 Poverty, or Populations at higher risk for
or even intentional but as near poverty, affects approximately pediatric medical traumatic stress
consequences of adversity.30 43% of US children, and both urban include preterm infants, children
and rural poverty have been linked with complex and/or chronic
Because these epidemiological and with multiple stressors and medical conditions, and those
physiologic studies provide the increased risk of trauma.42–44 suffering from serious injury or
background and impetus for TIC, Children of underrepresented racial, illness.56 Up to 80% of children and
understanding the terminology ethnic, and religious groups are family members experience trauma
Downloaded from www.aappublications.org/news by guest on October 11, 2021
4 FROM THE AMERICAN ACADEMY OF PEDIATRICSFROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 3 Definitions of Terminology in TIC
Terminology of Traumas Definitions
Acute stress disorder and Psychiatric diagnoses that include having experienced or witnessed a traumatic event and then having persistent
Post-traumatic stress symptoms that include the following: reexperiencing (intrusive thoughts, nightmares, or flashbacks); avoidance
disorder (PTSD) (feeling numb, refusing to talk about the event); hyperarousal (irritability, exaggerated startle response, always
expecting danger); acute stress disorder: symptoms occur 3 d to 1 mo after traumatic exposure81; PTSD:
symptoms must occur $3 mo after the trauma233
ACEs Stressful or traumatic events, including child abuse and neglect, that occur within the primary caregiving
relationship; often breach the parent-child relationship, which is fundamental to nurturing healthy development;
linked in population studies to physiologic and behavioral changes impacting the health and well-being of
patients over their life course with a wide array of health problems, including associations with substance
misuse.10,21,24,80 The original ACEs (from initial study published in 1998) are the following: physical abuse, sexual
abuse, emotional abuse, physical neglect, emotional neglect, intimate partner violence, mother treated violently,
substance misuse within household, household mental illness, parental separation or divorce, and incarcerated
household member. Subsequent studies have expanded the original ACE panel to include other adversities,9,234
including the following: experiencing racism, experiencing bullying, separation from caregiver (resulting from
immigration, foster care, incarceration, death, or any other reason), witnessing violence, community violence,49
adverse neighborhood experience,235 and financial insecurity236
Complex childhood trauma Encompasses both a child’s exposure to multiple interpersonal traumatic events, including maltreatment and
(as defined by the household dysfunction, and the broad, pervasive, and predictable impact this exposure has on the individual
National Child Traumatic child83,237; can disrupt a child’s attachment with caregivers, development, and sense of self
Stress Network)
Developmental trauma A proposed diagnosis based on evidence that children exposed to complex trauma are at risk for severe pervasive
disorder (DTD) disruptions in their development in the domains of emotional health, physical health, attention, cognition, learning,
behavior, interpersonal relationships, and sense of self; sometimes used interchangeably with complex childhood
trauma; describes problems in affect dysregulation, negative self-concept, and difficulty with relationships that occur
as a result of trauma-related developmental impairments; symptoms overlap or co-occur with several PTSD
symptoms, but DTD includes a fuller spectrum of dysregulation resulting from the insults to multiple pathways in the
developing brain when nurturing and is seen as a result of complex childhood trauma; more accurately describes
the outcomes of such trauma in children than does the diagnosis PTSD158,238
Pediatric medical The distress that children and family members experience during hospitalization for a perceived life-threatening
traumatic stress diagnosis or while living with or caring for someone with life-altering chronic conditions239–241; often related to
(PMTS) the person’s subjective experience of the medical event rather than its objective severity and is mitigated by
SSNRs that promote resilience
Secondary traumatic A response that may occur in parents, other family members, and health care workers such as physicians, nurses,
stress (STS) other hospital staff (including nonclinical staff), first responders, and therapists who are exposed to the
suffering of others, particularly children242; may have many of the same long-term effects on health that affect
children exposed to trauma; individual trauma histories can contribute to the reaction
Social determinants of Conditions of the greater ecology or environment, occurring where people live, learn, work and play, which affect
health (SDoHs) the neuroendocrine stress response and affect a wide range of health risks and outcomes8,22; can be mitigated
by an SSNR and other protective factors and exacerbated by ACEs and intrafamilial and interpersonal traumas;
examples include: poverty, food insecurity, homelessness, and lack of access to health care; examples that also
overlap with the expanded ACEs include racism, discrimination, and community violence
Trauma An event, series of events, or set of circumstances an individual experiences as physically or emotionally harmful
that can have lasting adverse effects on the person’s functioning and mental, physical, emotional, or spiritual
well-being14; can occur outside caregiving relationships (eg, dog bites, natural disasters), within the context of
the caregiving relationship (eg, exposure to domestic violence, various forms of abuse or disordered caregiving
because of parental mental illness or substance use disorder), or in the context of relationships outside the
family (racism, bias, discrimination, bullying)
symptoms after a life-threatening informed approach acknowledges and challenges?” “What are the
illness, injury, or painful medical the biological effects of adversity child’s strengths and challenges?”
procedure.57 without suggesting that childhood and “Who supports you?” This
adversity is destiny. It requires a changes the pediatric role from
compassionate approach that does “I must fix you” to “I must
READINESS not suggest blame. It requires understand you (and the
TIC transforms the fundamental pediatric health care workers at relationships that created you and
questions in medical care from every level to understand the can help you heal).”25,58 Thus,
“What is wrong with you?” to “What context of a child’s relationships, readiness includes an understanding
happened to you?” and, finally, to especially within the family, and ask, of what provides resilience and how
“What’s strong with you?” A trauma- “What are the caregiver’s strengths to promote it.
PEDIATRICS Volume 148, number 2, Downloaded
August 2021 from www.aappublications.org/news by guest on October 11, 2021 5Relational Health Care regulation. Secure attachment happens before and while raising concerns
TIC is fundamentally relational health as a child predictably receives this supports the caregiver. The empathy
care, the ability to form and maintain sympathetic support from the caregiver provided to the caregiver thus
safe, stable, and nurturing when the child is distressed and the allows the opportunity for them to
relationships (SSNRs). Pediatricians child comes to confidently anticipate reattune to the child.62
are able to support the caregiver-child that support. This relationship becomes
a reliable source of safety, and the Resilience
relationship, the context in which there
can be recovery from trauma and the caregiver is a secure base from which Resilience is defined as a dynamic
restoration of resilience. Fundamental the child can explore their process of positive adaptation to or
to these concepts is an understanding environment.62 Multiple studies have despite significant adversities.71 This
of attachment. shown that a secure attachment is not a static or innate quality but
relationship is the best means for includes skills children can learn
Attachment building or rebuilding resilience in over time with reliable support from
Attachment describes the children; it is also the context for attachment figures. The
emotionally attuned give-and-take promoting healthy brain growth and development of resilience includes
between caregiver and child and the development.62,65,68,69 With these aptitudes that are attained through
trust, safety, and security provided positive affiliative experiences, play, exploration, and exposure to a
to the child59 that promotes healthy modulation of the stress response variety of normal activities and
brain growth, development of begins and includes the release of resources. Studies have shown that
accurate mental maps of self and oxytocin, a potent hormone regulator of development can be robust, even in
others, development of resilience, the sense of safety and well-being.68,70 the face of severe adversity, if
and protection from trauma.60 certain basic adaptational
Fundamentally, the predictable Thus, the first step of TIC is to mechanisms of human development
compassionate availability of the assess this aspect of the (resilience factors) are protected
caregiver promotes the secure relationship, observing the and in good working order. These
attachment of the child.61,62 Recent child-caregiver interaction, including mechanisms include attachment to a
studies show attachment remains the caregiver’s attention to the child, competent caregiver, cognitive
malleable beyond infancy, even into the caregiver’s ability to read and development with opportunity for
adolescence and adulthood, to some respond to the child in continued growth, mastery of age-
extent.63,64 developmentally appropriate ways, salient developmental tasks, self-
and the child’s ease, comfort, and control or self-regulation, belief that
Effective Parenting response to the caregiver. life has meaning, hope for the
Effective parenting encompasses the Discussion can begin by focusing on future, a sense of self-efficacy, and a
skills that caregivers bring to the task the caregiver’s and child’s strengths network of supportive
of parenting and is the context in and noting the constructive aspects relationships.71 On the other hand, if
which secure attachment develops of the relationship while providing those basic adaptational
and is relied on during and after the caregiver with empathy. When mechanisms or protective factors
traumatic experiences. Although attachment is strained, caregivers are absent or impaired before,
caregivers approach parenting with a have often lost empathy for the during, or after the adversity, then
range of skills, attitudes, and beliefs child. The positive regard and the outcomes for children tend to be
rooted in their cultural and family attuned attentive listening provided poorer71 (see Table 4).
contexts, studies have shown that
effective or positive parenting has TABLE 4 Adaptational Mechanisms of Resilience
some universal features.65–67
It is through secure attachment with T Thinking and learning brain, with opportunity for continued growth; cognitive development
H Hope, optimism, faith, belief in a future for oneself
a predictably empathic caregiver
R Regulation (self-regulation, self-control of emotions, behaviors, attention, and impulses)
that children learn to regulate their E Efficacy (self-efficacy) or sense that one can impact their environment or outcomes
emotions. Children start by turning A Attachment, secure attachment relationship with safe, stable, and nurturing caregiver or
to a caregiver when upset. The competent caregiver
caregiver comforts the child by D Development, mastery of age-salient developmental tasks
S Social context, or the larger network of healthy relationships in which one lives and learns
touch, words, and compassion,
Adapted from Masten AS. Ordinary magic. Resilience processes in development. Am Psychol. 2001;56(3)227–238;
which shuts down the stress Forkey H, Griffin J, Szilagyi M. Childhood Trauma and Resilience: A Practical Guide. Itasca, IL: American Academy of
response and restores emotional Pediatrics; 2021.
Downloaded from www.aappublications.org/news by guest on October 11, 2021
6 FROM THE AMERICAN ACADEMY OF PEDIATRICSFROM THE AMERICAN ACADEMY OF PEDIATRICS
Robust implementation of TIC is triage, engagement, history-taking, caregivers to increase their ability to
strength-based, building on family surveillance and screening, provide effective support for their
protective factors rather than examination, differential diagnosis, child. The Healthcare Toolbox
emphasizing deficits. At almost sharing of the diagnosis, and includes a number of specific
every encounter, from early management, which may include suggestions, including assessing
childhood through adolescence, office-based anticipatory guidance, distress (D), providing emotional
pediatric care can include resilience referral, psychopharmacology, and/ support (E), and addressing the
promotion, building on identified or follow-up or recommendations. family needs (F)—a D, E, F protocol
strengths. Because resilience is a to follow the A, B, Cs of
dynamic process of positive Surveillance for maladaptation after resuscitation.74
adaptation, routine anticipatory experiencing trauma includes
guidance about development or consideration of all those who may Another comprehensive strategy
safety can be used to promote be affected by exposure to the direct used by schools and community
relational health and positive suffering of the child. Health care agencies when a mass trauma or
childhood experiences, including workers, such as first responders, disaster occurs is Psychological First
achievements at home, at school, nurses, social workers, trainees, Aid (PFA).75 Developed by the
and in neighborhoods, which physicians, and nonclinical hospital National Child Traumatic Stress
enhance resilience.72 When or clinic employees, may be deeply Network, PFA is an evidence-
addressing adversities or concerns affected by witnessing or hearing informed program that is designed
about development, surmounting about the traumatic experiences of to help children, families, adults, and
the challenges can be framed with children. Parents (biological, foster, other witnesses in the immediate
resilience and positive experiences kinship, or adoptive) are particularly aftermath of a disaster or terror
as the goal.73 For example, when at risk for prolonged trauma event. Core skills for implementation
speaking with a caregiver about a reactions that may impair their of PFA are identical to TIC: establish
child learning to fall asleep on their an emotionally safe environment,
ability to care for and comfort their
own, sleep skills can be framed as connect with primary support
children. Siblings may also be
building resilience by supporting persons (relational health), link to
affected, particularly when there is
self-regulation and self-efficacy. community resources, and provide
complex trauma or exposure to
Alternatively, when a caregiver psychoeducational materials to help
suffering, such as having a sibling
expresses concern about a child or understand the potential responses
with cancer or another life-altering
teenager who had been sleeping of children to the exposure.
disease that involves chronic pain.
until experiencing a traumatic event, Triage
the discussion can be framed around Peri-trauma
what resilience factors are being The first step in medical care is to
Peri-trauma refers to situations in
challenged (developmental skill identify an emergency versus
which medical providers are caring
mastery, self-efficacy, self- nonemergency situation. When
for children as the traumatic events
regulation) and which ones can be dealing with trauma, its causes, or
are unfolding. One example is
used to support the child’s recovery its consequences, consideration of
pediatric medical traumatic stress.
(attachment and thinking). whether a child may be emergently
Pediatric medical traumatic stress is
at risk requires assessment and
a situation in which children response as a top priority. In
DETECTION AND ASSESSMENT experience medical procedures or practicing TIC, protocols and
Detection involves both surveillance other aspects of medical care as practices to identify and address
and formal screening to identify traumatic events. The effects of such child or family safety issues, both
children and families with the trauma can be mitigated by physical and psychological, are
history of exposure to potentially attending to the child’s and family’s integral to care.
traumatic experiences as well as experience of medical care and
those who exhibit signs and reducing (as much as possible) Trauma may result from children
symptoms of trauma. Although TIC frightening or painful aspects of being in unsafe settings because of
is common in social services and necessary care and procedures. This abuse, neglect, or impaired
other mental health settings, in a mitigation can include asking caregiving. When the practitioner
health care environment, TIC can be children (and caregivers) about suspects maltreatment or failure of
conceptualized by using a medical their fears and worries, optimizing the caregiver to protect a child at
model. Similar to other medical pain management and comfort any point in a health encounter,
conditions, TIC includes purposeful measures, and working with referral to child protective services
PEDIATRICS Volume 148, number 2, Downloaded
August 2021 from www.aappublications.org/news by guest on October 11, 2021 7is necessary and mandated. These curiosity, and empathy are conveyed collect symptoms of trauma that
issues need to be considered even to the patient or caregiver in the may not have been identified in the
before screening and addressed with process of attentive listening.61 chief complaint but that can offer
standard protocols to respond to Engagement also involves mutual valuable insight into the current
identified risks.76–78 regard between the provider and impact of trauma on the patient.80,81
family. Adolescents and capable Symptoms may be functional,
Other immediate safety issues may children bring their own neurodevelopmental, or related to
arise when a consequence of trauma perspective. Each brings expertise to immune function.
is self-harm or intent to injure the TIC of the child or adolescent.
others. Screening for suicidality, self- The provider has expertise in 1. Functional symptoms: Manifestation
injury, or intent to harm others is medicine, whereas the patient and of the symptoms of trauma may
included in TIC along with clear family have expertise about the evolve over time. Functional com-
protocols for how to address child, what happened, and their plaints can result after single-
positive endorsement of these situation, beliefs, strengths, and incident traumas (eg, automobile
issues. culture. crash, hurricane) or may be early
Engagement manifestations of complex
When working with families and trauma.82–84 Sleep difficulty, changes
TIC creates a respectful and patients who have experienced in appetite, toileting concerns (eg,
emotionally safe space in which to trauma, the provider’s body
constipation, abdominal pain or
engage children, adolescents, and language, affect, and tone of voice
enuresis), and challenges with
families around the discussion and can promote or inhibit care. Affect
school functioning (eg, poor atten-
management of these issues and to describes the facial and body
tion or attendance) may be the early
prevent retraumatization. Discussion expressions that reflect our
presentation of ongoing trauma.84,85
of trauma may raise stress levels, emotional state. Individuals who
Diagnostic criteria for attention-defi-
and appropriate engagement have experienced trauma are more
cit/hyperactivity disorder and
reassures the child and family that sensitive to body language, facial
adjustment disorder overlap with
the setting is safe. Culture can also expressions, and tone of voice.70
some of these functional symptoms.
affect how trauma is experienced Approaching children slowly and
When these signs and symptoms are
and understood by families, and calmly or letting them sit with a
cultural awareness can ease the noted, it can be useful to include
caregiver and using higher pitched,
conversation. Engaging children and trauma in the differential
more musical speech may ease a
families begins with greeting the diagnosis.17,86,87
child’s tension because these sounds
patient and family and being fully 2. Neurodevelopmental symptoms:
are associated with the release of
present in the moment while Some of the most recognizable
oxytocin in the amygdala, resulting
maintaining a balance between in calming of this threat-sensitive manifestations of early trauma
professionalism and friendliness. It brain area. A shift to low tones result from the effect on areas of
involves initially asking open-ended during a discussion may alert a child the rapidly developing brain of
questions, followed by more or caregiver to potential danger and young children. Developmental
specific and probing questions as stimulate defensive responses.61 skill acquisition (higher brain)
needed and that are elicited by can be hindered as recognition of
caregiver and child or adolescent History and response to threat is priori-
responses. It involves listening in an Much of the information needed to tized (lower brain).88,89 Specific
active, nonjudgmental, attuned way, integrate TIC into practice may be areas of the brain affected are the
reflecting back to the family what is obtained as part of the routine limbic system, hippocampus, and
heard for clarification and health evaluation. Social, prefrontal cortex.12,13,90–92 The
confirmation, seeking clarification developmental, and medical history prefrontal cortex is involved in
when necessary, paraphrasing, are all opportunities to identify cognition, emotional regulation,
attending to and reflecting on the risks, stressors, and strengths. The attention, impulse control, and
emotions that accompany the health history provides an executive function. Consequently,
information, and summarizing what opportunity to assess child and children may have developmental
is discussed. Implicit bias can affect family resilience factors, social delay and behave as if they are
the provider’s ability to be connectedness, parenting attitudes, younger than their actual age89,93
nonjudgmental in these and skills. The review of systems (see Table 5 for an easy way to
conversations.46,79 Acceptance, allows the medical provider to remember these effects). Other
Downloaded from www.aappublications.org/news by guest on October 11, 2021
8 FROM THE AMERICAN ACADEMY OF PEDIATRICSFROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 5 Most Common Symptoms of Trauma Exposure concerned that asking questions
about a family’s needs, a child’s
trauma history, or a child’s
F Frets (anxiety and worry) and fears
R Regulation difficulties (disorders of behaviors or emotions; hyperactive, impulsive, easily symptoms may distress the child or
becomes aggressive or emotional; inattentive) caregiver, but studies in which this
A Attachment challenges (insecure attachment relationships with caregivers); poor peer relationships topic has been explored indicate
Y Yawning (sleep problems) and yelling (aggression, impulsivity) that, when the topic is raised,
E Educational and developmental delays (especially cognitive, social-emotional, and communication)
D Defeated (hopeless), depressed, or dissociated (separated from reality of moment, lives in
families respond well to having the
own head) issues acknowledged and addressed
Adapted from Forkey H, Griffin J, Szilagyi M. Childhood Trauma and Resilience: A Practical Guide. Itasca, IL: American in a supportive setting.85,103,104
Academy of Pediatrics; 2021.
Children only heal from trauma in
the context of SSNRs, so it is also
observed symptoms may include perception of feeling unwell that can
necessary to ask about the strengths
the following: include headaches, stomachaches,
that are already present in the
rapid, reflexive response to and lethargy.80,81
family. Starting these conversations
stimuli, reminders, or
Surveillance with questions about child,
triggers93,94;
adolescent, or family strengths
inattention, poor focus, hyper- Surveillance or monitoring is the
activity, and difficulty com- process of recognizing children who frames the conversation in a
pleting tasks86,95; might be at risk for being affected positive and resilience-focused
difficulty tolerating negative by trauma and is modeled after way.105,106 For instance, a clinician
mood so the child seeks ways developmental surveillance. may ask how the child, adolescent,
to defuse the tension through Surveillance is less formal than or family copes with stress, what a
hyperactivity, impulsive behav- screening and can be conducted at teenager does well, whether they
iors, aggression, self-harm, every visit. Asking about caregivers’ have frequent family meetings to
such as cutting and suicidality, concerns, obtaining a trauma talk about solving problems, and
or engagement in health risk history, observing the child, and whether each member of the family
behaviors (substance use, sex- identifying risk and protective has someone to turn to for safety
ual activity)89,95,96; factors provides information about and comfort when they are upset.
reactions to stimuli, triggers, or resilience supports and trauma Trauma that occurs because of
reminders can be transient and exposure.100 Surveillance requires problems in the primary attachment
flip suddenly back to “normal”; attention to relationships and relationship represents the greatest
this appears to the observer as engagement. Questions such as “Has threat to the child or adolescent and
emotional lability88,92; and anything scary or concerning may be the most challenging for
negative world view and self- happened to you or your child since providers to explore. Caregivers may
narrative; flat affect; difficulty the last visit?” are a way to more have their own trauma histories or
engaging socially or viewing specifically explore the possibility of mental health struggles, substance
themselves as worthless.88,92,97 adverse experiences.85 Recognizing use issues, and/or multiple stressors
3. Immune function symptoms: When that certain symptoms may indicate related to social determinants of
a child is exposed to early, severe, or exposure to childhood adversities, health (SDoHs), including poverty,
prolonged trauma, the immune sys- we can ask, “What has happened to housing instability, and violence
tem is chronically pressed into you (or your family)?” For exposure that affect their parenting.
action, and, over time, changes can adolescents, these questions can be Exploring parenting stressors,
occur in the inflammatory system asked as part of the HEADSSS strengths, and attitudes in
and humoral immunity.80,89 A per- (questions about Home conversation can help the provider
sistent inflammatory response can environment, Education and to pinpoint specific leverage points
leave children vulnerable to dis- employment, Eating, peer-related to help children but may also create
eases, such as asthma and metabolic Activities, Drugs, Sexuality, Suicide/ an opportunity for the caregiver to
syndrome.80,98,99 Humoral immu- depression, and Safety) psychosocial reflect about the effects of their
nity may be impaired so that chil- interview.101,102 Questions that are parenting or stressors on the child.
dren are more susceptible to considered less threatening are TIC is compassionate and assumes
infection. Additionally, immune sys- asked first and followed with that all caregivers love their
tem stimulation may result in the questions that may be perceived as children and are doing the best they
“sick syndrome,” which is a more intrusive.101 Providers may be can. It also assumes that children
PEDIATRICS Volume 148, number 2, Downloaded
August 2021 from www.aappublications.org/news by guest on October 11, 2021 9are doing the best they can.107,108 traumas are known.118 These tools skills.107 Similar to ACE screening,
Adolescents should be included in effectively help identify the there are few available standardized
these conversations and have a role diagnostic criteria for PTSD, validated resilience screening tools,
in identifying strengths and although they are not designed to although the Connor-Davidson
challenges. Pediatricians who have identify the full spectrum of Resilience Scale126 and Brief
cared for a family over time may symptoms of complex trauma Resilience Scale127 assess
already have considerable insight (developmental trauma disorder caregiver resilience.128 (Readers are
into the family’s dynamics and be [DTD]). referred to the AAP Screening
able to engage the caregivers in an Technical Assistance Web site at
empathic yet open conversation. Screening, per American Academy of https://www.aap.org/en-us/
Furthermore, compassionate Pediatrics (AAP) guidelines, suggests advocacy-and-policy/
surveillance can be combined with using instruments that are aap-health-initiatives/Screening/
use of screeners or questionnaires standardized and validated and have Pages/About-Us.aspx for developmen-
to elicit more information. defined psychometric properties tal and SDoH screening tools.)
(sensitivity, specificity, positive
Screening predictive value). By that definition, A limitation of ACE and SDoH
Validated screeners used at there are currently no screening screening tools is their lack of
preventive health care visits can tools for ACEs and only a few nuance: they identify risk factors
provide valuable information about validated screening tools for SDoHs. that have been derived from
child development, mental health, However, standardized (but not epidemiological studies, not
and behavior.109 They can be validated) tools are being used in outcomes at the individual
some pediatric settings to assess level.129,130 Those outcomes are the
reassuring when normal or alert the
ACEs and SDoHs and are using result of the physiologic response to
pediatric provider to symptoms or
aggregate risk scoring to target adversities. Although currently only
risks when borderline or abnormal.
providing increased support.119–121 available in the research setting,
Commonly used tools, such as the
biomarkers of this physiologic
Ages and Stages Questionnaire,110 Many of the available screening
response have the potential to be
the Pediatric Symptom Checklist,111 tools expanded on the domains
more accurate measures of the
the Strengths and Difficulties included in the original Centers for
effects of adversity at the individual
Questionnaire,112 and the Patient Disease Control and Prevention/
level.131–133 Eventually, clinic-
Health Questionnaire-9113 may elicit Kaiser ACE study to include
friendly, noninvasive biomarkers
symptoms that are the possible additional items applicable to urban
could also be used to identify
result of trauma (developmental and minority populations, including
patient-specific response to both
delays, social-emotional problems, witnessing neighborhood violence
stressors and therapeutic
anxiety, etc). Perinatal depression and experiencing bullying or
interventions.134,135
screening may not only identify discrimination.9 Parental ACE
symptoms of this illness but provide screening may offer the opportunity Screening health care workers for
opportunities to explore maternal to align with caregivers and build a the effects of hearing about and
stressors and strengths.114 Those partnership to explore issues that addressing the trauma experiences
exposed to known traumas can be may be affecting their parenting. of others is most commonly
evaluated by using standardized Indeed, several recent studies achieved with informal self-
posttraumatic stress disorder suggest that parental ACEs can be assessment strategies to identify
(PTSD) screening tools such as the linked with concerning outcomes for symptoms or experiences that may
PTSD Reaction Index Brief Form,115 children.122–125 Concurrent be associated with burnout or
and those exposed to medical resilience screening offers the STS.136 Substance use disorder,
traumas can be evaluated by using a opportunity to identify protective depression, and suicidality may be
tool such as the Psychosocial factors that can buffer identified associated with exposure to
Assessment Tool.116,117 The stressors, thus providing more secondary trauma, and there
Pediatric Traumatic Stress Screening nuanced understanding of a child’s appears to be overlap between
Tool in the Intermountain Care risk. Screening also offers the burnout and STS.137–144 An example
Process Model has been recently opportunity to then frame the of a screening tool for health care
developed to screen for pediatric discussion around promoting workers is the Professional Quality
traumatic stress in the primary care strengths in the caregiver-child of Life Scale,145 which includes
setting, either as a universal screen relationship to protect a child from subscales for compassion
or with targeted screening when toxic stress and build adaptive satisfaction, burnout, and STS.
Downloaded from www.aappublications.org/news by guest on October 11, 2021
10 FROM THE AMERICAN ACADEMY OF PEDIATRICSFROM THE AMERICAN ACADEMY OF PEDIATRICS
Cultural considerations affect all incorrect or incomplete diagnosis MANAGEMENT
aspects of TIC, including screening. and treatment, enabling the effects
Sharing the Diagnosis With Children
Instruments that are not normed for of trauma to further embed.17,157,158
and Caregivers
the population or translated and Trauma may be mistaken for other
validated in the language of the conditions, such as attention-deficit/ Some parents and caregivers may
patient and family can result in hyperactivity disorder, and includes come to understand the role of
misleading results. Thus, it is symptoms that overlap with other adversities in their child’s symptoms
important to consider screening diagnostic categories, such as through discussion of the trauma
history and symptoms, and others
results cautiously with consideration anxiety and depression.86,87,159 It
of the family’s culture and ethnicity will require the provider to explain
has been proposed that trauma may
this connection before they can
in relation to the screening tool result in a different “ecophenotype”
being used.146 appreciate the provider’s advice and
of common conditions that have a
recommendations. Psychoeducation
different trajectory and different
Examination is the first step in management of
response to common treatments.93
Blood pressure measurement at childhood trauma and includes
Children may also have comorbid empathic, nonjudgmental sharing of
preventive health visits or when conditions, such as ADHD, anxiety,
stress is a potential etiologic factor diagnostic information and provider
depression, or developmental and concerns about the etiology of a
for concerns is indicated.147 learning issues, because they child’s symptoms The provider’s
Elevated blood pressure may be the frequently accompany childhood role is to integrate the child or
first symptom of childhood trauma. A more detailed description adolescent and caregiver’s concerns,
traumatic stress, especially as youth
of diagnoses that are commonly the child or adolescent’s symptoms,
age.148,149 Abnormalities in hearing,
confused with trauma or comorbid and elements of a thorough history
vision, and growth parameters can
with it are covered in the AAP and examination into an explanation
be clues to adversities.150,151
clinical report “Children Exposed to of why this raises a concern about
Overweight and obesity have been
Maltreatment: Assessment and the trauma exposure or why trauma
associated with ACEs.152–154
Role of Psychotropic Medication.”87 may be the underlying cause or one
Physical examination may reveal
of the causes of a child’s symptoms,
signs of neglect or abuse. The Diagnostic Continuum much as is done for any diagnosis. A
immunologic effect of trauma may
Pediatric providers may encounter simple explanation of the
result in inflammatory or infectious
children with a wide range of pathophysiology of trauma may help
consequences identifiable on the caregiver to move from
symptoms resulting from trauma. As
examination.1,80,99,155,156 Children frustration with the child or
noted, trauma can result in short-
who have sustained cumulative adolescent’s behaviors or symptoms
term changes in behavior or have a
ACEs and traumas may exhibit to empathy. In some situations, the
more lasting impact depending on
certain common behaviors the explanation may also provide the
the child, the trauma itself, and the
provider may witness during caregiver with insight into their own
supports or emotional buffers in a
physical and mental health history of trauma and its impact on
child’s life. When traumatic events
evaluation (refer to history and their parenting behaviors or
are more severe, prolonged, or less
symptoms described earlier). responses to their child’s behaviors,
buffered by a caregiver, effects on
or how an event that affected their
Differential Diagnosis various aspects of functioning can
child may have traumatized the
Considerations and Comorbidities be more severe.1,160–163 Children
caregiver as well.
The provider is encouraged to exposed to chaotic households,
consider trauma as a possible abuse, or neglect, especially in the Psychoeducation includes
etiology in the assessment of early years of life, may have more acknowledging that a trauma history
developmental, mental health, severe symptoms and symptoms can affect behavior and thoughts,
behavioral, and physical symptoms that evolve over time.94,159,164,165 with some discussion of how that
in all pediatric encounters because Diagnostically, this may result in happens. Table 6 has information on
of the following: (1) the experience children who have functional specific psychoeducation. The
of adversity is so common; (2) the symptoms (short-term problems variable responses of children to
symptoms of trauma overlap with with sleeping, eating, toileting), trauma can be frustrating or
the symptoms of other common adjustment disorder, PTSD, or confusing. Discussion of the
pediatric conditions87,95; and (3) complex trauma emerging data on the biological
failure to do so might lead to an symptoms.163,166,167 sensitivity to context may be useful
PEDIATRICS Volume 148, number 2, Downloaded
August 2021 from www.aappublications.org/news by guest on October 11, 2021 11TABLE 6 Responses to Trauma to Explain to Caregivers: Psychoeducation
Impacts of Trauma on Function and Behavior Clinical Presentation
Changes in auditory processing Children may lose the ability to hear sounds of safety (musical high-pitched voice) and be
preferentially attuned to low-pitched sounds that warn of caregiver depression and anger.247
Changes in how children interpret Children may misinterpret the affects and emotions of others, particularly confusing anger and
facial expressions fear.93
Limited vocabulary for emotions Children may also not accurately recognize or express their own emotions, leading them to act out
or respond in ways that seem “off.” What a child (or caregiver) identifies as “anger” may be
disappointment, frustration, fear, grief, or anxiety.88
Negativity Trauma results in children having overactive limbic systems with a focus on safety and a
presumption of danger. This can result in strong negative reactions as the first response to a
stimulus that might be benign or ambiguous.61
Triggers Triggers can be physical (smells or sounds that recall details of the trauma) or emotional (feeling
embarrassed or shamed, recalling how child felt during abuse). Prevention of exposures to reminders
or triggers is the best approach. Triggers may be subtle, so educating and assisting caregivers with
their identification is key. This helps caregivers understand a child’s response.167
Learned Behavior Behaviors that were adaptive for a child in a previous environment may be maladaptive in their
current environment. These behaviors can evoke some of the same reactions from caregivers
that the child experienced with other adults, reinforcing a familiar pattern of interactions that
may not be productive in the new setting.61
Adapted from the National Child Traumatic Stress Network. Families and caregivers. Available at: https://www.nctsn.org/audiences/families-and-caregivers. Accessed January 11,
2021;243 US Department of Health and Human Services, Administration for Children and Families. Resources on trauma for caregivers and families. Available at: https://www.
childwelfare.gov/topics/responding/trauma/caregivers/. Accessed January 11, 2021244; and American Academy of Pediatrics. Parenting After Trauma: Understanding Your Child's
Needs. Available at: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/healthy-foster-care-america/Documents/FamilyHandout.pdf. Accessed June 24, 2021245.
to caregivers.168,169 Genetic state Maternal Child Health Title V helping the children to learn words
variations in how a person responds programs, and Family to Family to describe a variety of emotions,
to stress may contribute to a child’s Health Information Centers ready and promoting self-reflection
sensitivity to adversity.170 Yet, those for distribution, directly contacting concerning the caregiver’s own
with high reactivity who are the referral provider with the trauma history, the pediatric
supported and learn to channel that patient present, or providing formal clinician can render primary
reactivity to positive activities and care coordination all facilitate family prevention against the development
passions may have the greatest engagement and help families of anxious and maladaptive
potential.168 This information, along connect to needed community attachment patterns and promote
with specific suggestions about how resources. For older children and regulation.82,174 Examples of
to support children, can address adolescents, trauma-informed relevant anticipatory guidance
some of the consternation of schools and teenager crisis centers include advice, resources, or
caregivers regarding children’s may be available in the community. referrals to community programs,
heterogeneous responses to both In trauma-informed schools, including Reach Out and
adversity and interventions. personnel at all levels have a basic
Read175–177; developmentally
realization about trauma and an
Office-Based Anticipatory Guidance appropriate play with others178–180;
understanding of how trauma affects
and Management promoting positive, authoritative (in
student learning and behavior in the
contrast to punitive or
Trauma-informed anticipatory school environment.171,172
guidance provided by pediatricians authoritarian) parenting
can help families promote resilience Every encounter in an office setting, styles181–183; and
and begin to address the effects of from those with young children to mindfulness.184–186 Table 7 includes
trauma. If screening for SDoHs is those with adolescents, is an specific advice to promote
being conducted and/or social needs opportunity to strengthen the regulation after trauma.
are identified, referral to applicable attachment between a child and
Referral for Treatment
community-based services is caregiver.173 Through techniques
indicated (eg, food bank, pro bono such as reinforcing positive back- The presence of complex symptoms,
legal aid, etc). Having a list of and-forth interactions between a mental health diagnoses, substance
community providers, such as Early parent and a child (serve and abuse, and/or a significant trauma
Head Start, Head Start, evidence- return), helping the caregiver to history are indications for referral to
based maternal, infant, and early understand the child’s experience evidence-based trauma-informed
childhood home visiting programs, (keeping the child’s mind in mind), mental health services.
Downloaded from www.aappublications.org/news by guest on October 11, 2021
12 FROM THE AMERICAN ACADEMY OF PEDIATRICSYou can also read

















































