Using a Composite Graft of Natural 15% Chitosan Gel in the Management of Intrabony Defects: A Case Series
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of the International Academy of Periodontology 2019 21/1: 4-10
Using a Composite Graft of Natural 15%
Chitosan Gel in the Management of Intrabony
Defects: A Case Series
Irfana Babrawala, Prabhuji MLV and Karthikeyan BV
Department of Periodontology, Krishnadevaraya College of
Dental Sciences and Hospital, Hunsmaranahalli, Near Interna-
tional Airport Road, Bangalore – 562157, India
Abstract
Introduction: Periodontitis is a chronic infection affecting the supporting tissues of the
teeth which, if left untreated, eventually leads to tooth loss. Various grafting materials
and barrier membranes have been used to repair periodontal intraosseous lesions. It has
been shown that chitosan, a natural polymer, has potential to be used for periodontal
tissue regeneration. Thus, it is possible that chitosan, in conjunction with bone grafting,
might have good potential to be used for periodontal regeneration. The purpose of this
case series was to evaluate the efficacy of chitosan, along with bovine porous bone
mineral, in periodontal regeneration of intrabony defects.
Materials and Methods: Ten patients aged between 30 and 55 years with intrabony
defects ≥3 mm and pocket probing depth (PPD) ≥5 mm were selected. All participants
received chitosan gel (15% w/v) plus bovine porous bone mineral as a composite bone
graft. Clinical and radiographic measurements were recorded at baseline, 3 months after
healing and at 6 and 9 months. Significance was set at 0.05.
Results: After nine months, all the defects treated with this combination showed PPD
reduction of 5.30 ± 0.822 mm, relative clinical attachment level (CAL) gain of 5.80 ±
0.499 mm, reduction in intrabony defect (IBD) depth of 3.00 ± 0.497 mm and defect
resolution of 78.32 ± 5.80 %, all of which were statistically significant.
Conclusion: Within the limits of this study, this case series study suggests that chitosan gel, along
with bovine porous bone mineral, has a promising role to play in periodontal regeneration.
Key words: Chitosan, Periodontal regeneration, Bovine porous bone mineral,
Wound healing
Introduction include the use of an array of regenerative materials (Garrett,
1996; Laurell et al., 1998), tissue regeneration methods using
Methods for the management of periodontal disease have barrier membranes and a combination of both bone grafts
progressed considerably over the last two decades. However, and membranes (Joly et al., 2002). Despite each regenerative
in some cases inability to control the progression of periodon- material possessing its own unique regenerative potency, there
tal disease results in osteolysis of the alveolar bone supporting are certain inherent biological and surgical limitations which
the teeth leading to intrabony defects (Gupta, 2010; Krebs restrain their widespread acceptance (Wagh, 2004; Suzuki et
and Clem, 2006). The long-term prognosis of teeth may be al., 1989).
adversely affected if the intrabony defects are not treated These concerns and limitations have stimulated consider-
appropriately. Several approaches to facilitate regeneration in able interest in the development of artificial materials, that are
these osseous defects have been reported in the literature and natural in origin, to be used as bone graft substitutes (Gian-
noudis et al., 2005). Recently, the discovery of chitosan (a novel
natural polymer), has been considered as a useful adjunct for
regenerative periodontics (Klokkevold et al., 1996) because of
its biological properties such as biocompatibility, non-toxicity,
Correspondence to: Prabhuji MLV, Department of Periodontology, anti-inflammatory, biodegradability and bio-adhesion (Senel
Krishnadevaraya College of Dental Sciences and Hospital, Hunsma-
ranahalli, Near International Airport Road, Bangalore – 562157, et al., 2000a; Senel et al., 2000b; Ikinci et al., 2002; Fakhry
India. Email: prabhujimlv@gmail.com; Mobile no +91-9448057407 et al., 2004; Aksungur et al., 2004; Akncbay et al., 2007).
© International Academy of Periodontology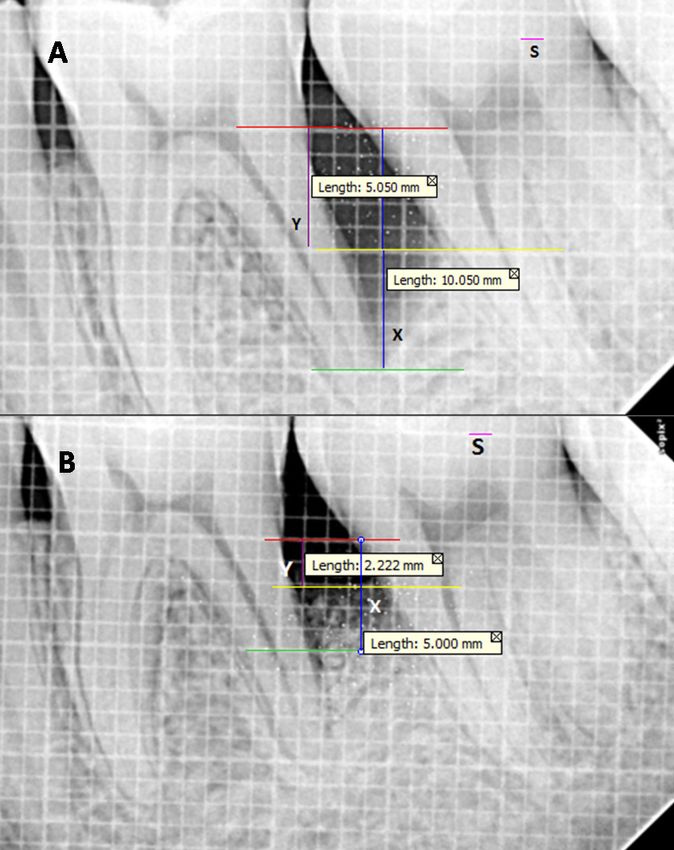
Babrawala et al.: Composite graft in intrabony defect 5
In dentistry, chitosan has been used in various forms Selection Criteria
such as mouthwashes and films (Vilasan et al., 2013). Our Systemically healthy patients aged 30-55 years with the
research team has recently reported that chitosan can presence of localized PPD ≥5 mm, CAL ≥5 mm, 3-wall
also be used as a local drug delivery system during non- intrabony defect ≥3 mm deep (assessed by transgingival
surgical periodontal therapy (Babrawala et al., 2016a). probing and to be confirmed after flap elevation) with
Chitosan possesses several bioactive properties the defect not extending to a root furcation area and
including antimicrobial properties, hemostatic activ- no invasive periodontal therapy carried out in the past
ity, tissue regenerative capacity, osteoconductivity and 6 months and associated tooth and neighboring teeth
induction of neovascularization that lead to accelerated with ≤1 mm of tooth mobility were included in the
bone growth (Park et al., 2000; Wang, 2003; Chevrier study. Patients with unacceptable levels of oral hygiene
et al., 2007; Jayasuriya and Kibbe, 2010). Chitosan has (PI > 1.5; Silness and Loe., 1964), pregnant and lactat-
also been evaluated for the treatment of bone lesions ing women, smokers, patients with suspected or known
by incorporating it with platelet-derived growth factor- allergy to chitosan or on medications known to interfere
BB (PDGF-BB) (Park et al., 2000), hydroxyapatite with periodontal wound healing and immunocompro-
(Mukherjee et al., 2003), GTR membranes (Shin et al., mised patients were excluded from the study.
2005) and has shown high tissue compatibility with Phase 1 therapy (scaling and root planning) was
no evidence of inflammatory reaction. Boynuegri et performed and re-evaluation was carried out 8 weeks
al., (2009) evaluated a combination of 1% chitosan after completion of the initial therapy.
gel with demineralized bone matrix (DBM) for the One examiner (IB) performed all the surgeries while
treatment of periodontal intraosseous defects and another examiner (MLVP) performed all the clinical and
reported favorable bone fill. Subsequently, an in radiographic measurements.
vitro study demonstrated that chitosan, when used in
combination with bone grafts, at a concentration of Inter-examiner and intra-examiner calibration
15% has a superior regenerative potential than other Prior to commencement of the study, inter-examiner
concentrations (Weir and Xu., 2010). Recently, we and intra examiner calibration was achieved by examin-
have reported that chitosan at a 15% concentration ing 20 patients two times (24 hours apart). The examin-
has the potential to induce regeneration of intraosse- ers were considered as calibrated if the measurements
ous defects (Babrawala et al., 2016b). However, to date recorded at baseline and 24 hours were analogous within
there have been no data published on the regenera- 1 mm at the 95% level.
tive potential of chitosan at 15% concentration when
combined with bone grafts. Hence, the present case Clinical and Radiographic Measurements
series aimed to evaluate the efficacy of 15% chitosan
Prior to surgery, pocket probing depth (PPD) and
gel when combined with bovine porous bone mineral
relative clinical attachment level (CAL) were recorded
for the treatment of intrabony defects.
using a UNC-15 (Hu-Friedy, Chicago, IL, USA) manual
probe from the apical extent of a customized acrylic
Materials and methods stent that was grooved to the base of the defect to
Source of data ensure reproducible placement of the probe for each
A total of 10 patients; 7 males and 3 females, aged successive measurement. All the radiographs were
between 30 and 55 years old attending the outpatient taken using a paralleling technique of radiovisiography
section of Department of Periodontology, Krishnade- pre-operatively at baseline and post-operatively at 3,
varaya College of Dental Sciences and Hospital, Banga- 6 and 9 months. A calibrated measurement software
lore were included in the study (study dates: September (Digimizer, MedCalc Software BVBA, Belgium, version
2015 to August 2016). The study protocol was reviewed 4.0) was used for the radiographic measurements. The
and approved by the institutional ethical committee and cementoenamel junction (CEJ), the crest of alveolar
review board. The design, nature of the clinical trial and bone (AC) and the base of the defect (BD) were
the potential risks if any were explained to the patients. marked on the image. A line was drawn from CEJ to
A signed informed written consent for their participa- BD. The software then displayed the distance between
tion was obtained from them. these two points. The same procedure was then re-
peated to obtain the distance between CEJ and AC.
Sample size determination Subtracting the two measurements; the depth of the
G power software was used for a priori computation of osseous defect was obtained. The total bone fill was
the sample size of our study by keeping effect size 0.4, measured subtracting the depth of the osseous defect
α error 0.05. Using this data we arrived at a sample size at 9 months from the baseline measurement (Mahajan
of 10 with 80% statistical power. and Kedige., 2015).6 Journal of the International Academy of Periodontology (2019) 21/1
Formulation of 15% chitosan gel were sutured to their original position with 4-0 silk su-
After purification, chitosan was further prepared by tures (Mersilk, Ethicon, Johnson & Johnson, Himachal
dissolution-precipitation and dialysis, and reacetylation Pradesh, India) with a 16 mm reverse cutting, 3/8 circle,
up to a degree of 50%. In order to produce gels at atraumatic swagged needle. Simple interrupted sutures
37°C, 15% chitosan solution (chitosan + sterile distilled were made to achieve primary closure (Figure 1D) fol-
water at pH 7.2) was prepared followed by neutralization lowed by placement of periodontal dressing (Coe Pack,
with sodium hydroxide. This process resulted in a small GC America Inc, IL, USA).
increase in viscosity and a very slow gelation capacity.
Post-operative wound management
Thermosetting properties were tested before and after
lyophilization to produce a stable formulation. Addition Following surgery, 500 mg of amoxicillin every 6 hours
of trehalose preserved the thermosetting properties. for 5 days, 400 mg of ibuprofen every 8 hours and
The 15% concentration of chitosan gel was prepared 0.2% chlorhexidine digluconate twice daily for 4 weeks
in as described by Weir and Xu (2010) at the Essence post surgically were prescribed to the patient. Patients
Biotech Research Laboratory (Kochi, Kerela, India). were reevaluated for pain, sensitivity and discomfort.
Patients were recalled after 7 days for suture removal.
Surgical procedure Hard and soft tissue measurements were taken at 3, 6,
After administration of local anesthesia with 2% ligno- and 9 months post-surgically (Figure 2).
caine hydrochloride and epinephrine concentration of
Statistical analysis
1:80,000 (Lignox 2%, Indoco Remedies Ltd, Goa, India),
full thickness mucoperiosteal flaps were raised on the The data collected were entered in Microsoft Excel and Sta-
buccal and lingual aspects of the involved sites. Thor- tistical analyses were performed using the Statistical Package
ough debridement was performed using area-specific for Social Science (SPSS ver 10.5) software. Shapiro-Wilks
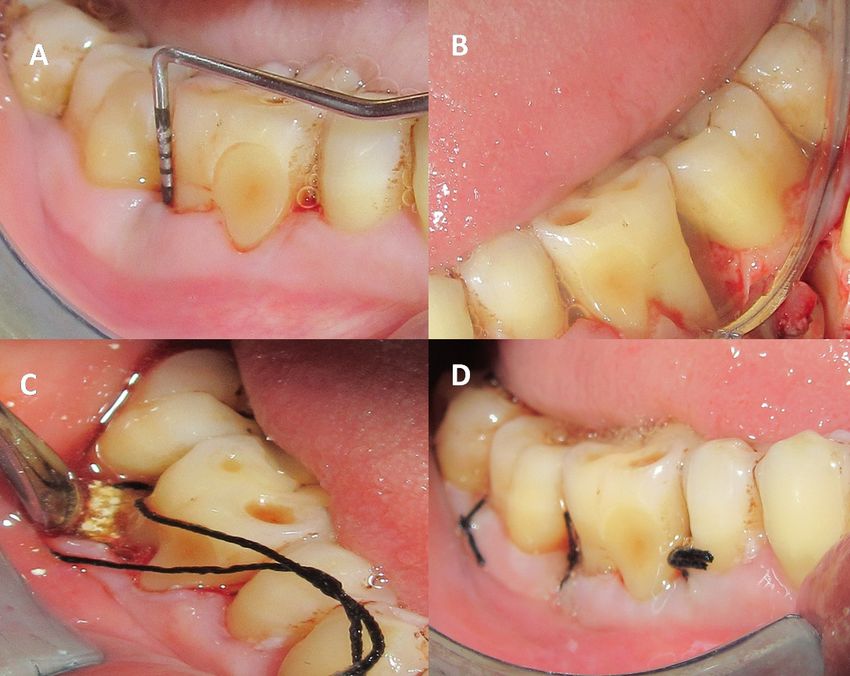
curettes and ultrasonic scalers (Figure 1A and 1B). Fifteen test was used to test the normalcy of the data and the data
percent chitosan gel, in combination with bovine porous were found to be normally distributed. Therefore, parametric
bone mineral (Bio-Oss™, Geistlich Biomaterials, Swit- statistical tests were used. To test differences in the defect
zerland), was used as the bone regenerative material to level over time, Analysis of Variance (ANOVA) test was
fill the intrabony defect (Figure 1C). Thereafter, the flaps performed with significance set at the level of 5%.
Figure 1. (A) Pre-operative measurement of pocket probing depth. (B) Raising full thickness
mucoperiosteal flap followed by debridement. (C) 15% chitosan gel + bovine porous
bone mineral packed in the defect. (D) Primary closure with simple interrupted sutures.Babrawala et al.: Composite graft in intrabony defect 7
Figure 2. Radiographic analysis to determine the depth of the intrabony defect with 3 reference lines, i.e. red
line represents the cementoenamel junction (CEJ) of the tooth; yellow line represents the level of alveolar crest
(AC) and green line represents the base of the alveolar defect (BD) using a software known as Digimizer (ver
4.0). Standardization of the radiograph (S). X is the distance from CEJ to BD and Y is the distance from CEJ to
AC. Depth of intrabony defect = X-Y. (A) Pre-operative radiograph. (B) 9 months post-operative radiograph.
Results Table 1. Intragroup comparative evaluation of pocket
probing depth (PPD), clinical attachment level (CAL)
A total of 10 defects in 10 patients were evaluated. The and radiographic depth of intrabony defect (IBD) in
treated sites were evaluated for clinical parameters at baseline, millimeters (mm) at different visits
3 months, 6 months and 9 months post-operatively using the
Mean ± Std
ANOVA test. No patient dropped out during the study and Parameter Visit p value
Deviation
uneventful healing was observed for all cases. Good oral hy-
giene was maintained by the patients during the study period. Baseline 8.20 ± 1.39
3 months 5.30 ± 0.67
Significant reduction in pocket probing depth (PPD) PPD 6 months 4.10 ± 0.73 0.001*
was observed from baseline (8.20 ± 1.39 mm) to 9 months 9 months 2.90 ± 0.56
(2.90 ± 0.56 mm). Similarly, significant gains in attachment
were noted from baseline (8.90 ± 1.17 mm) to 9 months Baseline 8.90 ± 1.17
3 months 5.70 ± 0.82 0.001*
(3.10 ± 0.67 mm; Table 1). CAL 6 months 4.20 ± 0.70
Significant reduction in intrabony defect depth was 9 months 3.10 ± 0.67
observed from baseline to 3 months i.e., 1.30±0.06 mm
Baseline 3.80 ± 0.91
(3.80 ± 0.91 mm - 2.50 ± 0.85 mm = 1.30±0.06 mm), 6
3 months 2.50 ± 0.85 0.001*
months i.e., 2.1±0.24 mm (3.80 ± 0.91 mm - 1.70 ± 0.67 IBD
6 months 1.70 ± 0.67
mm= 2.1±0.24 mm) and 9 months i.e., (3.80 ± 0.91 mm 9 months 0.80 ± 0.42
- 0.80 ± 0.42 mm = 3.00± 0.49 mm; Table 1). Percentage
*p value ≤ 0.05 is statistically significant. ANOVA test
of defect fill noted at 9 months was 78.32 ± 5.80 (Table
2). On an average, complete defect fill was noted in 50%
of patients after 9 months.8 Journal of the International Academy of Periodontology (2019) 21/1
Discussion osteoblastic differentiation may be enhanced by chi-
tosan which may interfere with the fibroblast function
This is the first study, to the best of our knowledge, to inhibit bone formation and indirectly facilitate
in which a combination of chitosan gel at a concen- osteogenesis (Klokkevold et al., 1996). The noteable
tration of 15% and bovine porous bone mineral has advantage of chitosan is that its degradation product
been evaluated for the treatment of periodontal bone is a neutral to weak base sugar, as opposed to some
defects. The outcome of the present study demon- graft materials that generate acidic degradation by
strated that chitosan has good regenerative potential products, evoking undesirable tissue reactions (Weir
as both clinical and radiographic parameters improved and Xu, 2010).
significantly. Despite the favorable results, the outcome of this
In the present study, no inflammatory reactions study should be interpreted with caution as there are
were noted, with total biological acceptance. Overall certain inherent limitations. Direct comparison be-
the post-operative healing was uneventful. To ensure tween studies including the present one might not be
standardization, all measurements were recorded by reasonable due to large variation among them regarding
calibrated examiners and only 3- wall intrabony defects patient and graft characteristics, defect morphology,
≥3 mm affecting molars were considered. All the se- surgical technique and wound management. The de-
lected patients had a thick gingival biotype. The biotype fects included in the present study were 3-wall defects
was evaluated by placing the periodontal probe in the which were deemed as having a reasonable potential for
facial aspect of the gingival sulcus. It was categorized regeneration. Furthermore, it should be noted that the
as thin if the outline of the underlying probe could be radiographs used in this study were not identical due
seen through the mucosa and thick if the probe could to minor errors in film placement. Nevertheless, this
not be seen. Intrabony defects, when repaired with this technique of combining chitosan with bovine porous
combination, exhibited significant PPD reduction of bone mineral should be explored further in defects
5.30 ± 0.822 mm, CAL gain of 5.80 ± 0.499 mm, re- with limited regenerative potential such as 1- and
duction in IBD depth of 3.00 ± 0.497 mm and defect 2-wall defects. The present case series did not include
resolution of 78.32 ± 5.80 % at 9 months. a control group. Therefore, it is not known if the use
A previous study where a combination of chitosan of bovine porous bone mineral alone could also have
gel at 1% concentration + demineralized bone matrix resulted in acceptable defect fill in this study. Apart
(DBM) (Boynuegri et al., 2009) was used for intraos- from small sample size and short follow-up, chitosan
seous defects, reported a reduction in PPD of 2.60 ± itself has some limitations despite the fact that it is a
0.17 mm, gain in attachment of 1.80 ± 0.12 mm and propitious material. This natural polysaccharide has
the mean amount of intrabony defect depth observed poor solubility (Chen et al., 2005) and lacks long-term
at 6 months was 1.40 ± 0.08 mm. In comparison, the stability. Since chitosan is a weak scaffold, the desired
results of the current study were superior in all param- mechanical strength can be attained by using additional
eters even at 6 months. In addition, our results showed hydroxyapatite (Malafaya and Reis, 2009) or gelatin
a similar trend with other studies where chitosan ws (Jiankang et al., 2009). With the analytical methods
used in combination with collagen membranes or available today, histologic evaluation is needed for
combined chitosan with hydroxyapatite and PDGF-BB, conclusive evidence of this therapeutic outcome.
suggesting that chitosan improves clinical parameters It may also be worthwhile to evaluate chitosan
and radiographic bone resolution (Park et al., 2000; with other regenerative materials. There is also a need
Mukherjee et al., 2003; Shin et al., 2005; Boynuegri et for multi-centered long-term randomized clinical tri-
al., 2009). als to be conducted in order to validate the outcome
The favorable results noted in our current study of this preliminary report. With the limited evidence
can be assumed to be due to the favorable regenera- available, it can be concluded that a combination of
tive properties of chitosan. Primarily, chitosan may 15% chitosan gel and Bio-Oss™ that acts as a biologi-
be considered as a very promising scaffold material in cal modifier might support and enhance periodontal
bone tissue engineering due to its ability to potentiate regeneration. The present data indicates that the
the differentiation of osteoprogenitor cells that may treatment of intrabony defects with 15% chitosan and
facilitate bone formation (Klokkevold et al., 1996). bovine porous bone mineral resulted in considerable
Secondly, chitosan demonstrates structural similari- clinical and radiographic improvements.
ties to the glycosaminoglycan hyaluronic acid which is
found in extracellular matrices of many tissues. Hya- Conflict of Interest
luronic acid is believed to facilitate the proliferation
The authors reported no conflict of interest.
and migration of progenitor cells facilitating tissue
regeneration (Adzick and Longaker, 1992). Thirdly,Babrawala et al.: Composite graft in intrabony defect 9
References Jiankang H, Dichen L, Yaxiong L et al. Preparation of
chitosan-gelatin hybrid scaffolds with well organized
Adzick NS and Longaker MT. Characteristics of fetal microstructures for hepatic tissue engineering. Acta
tissue repair. In: Adzick NS, Longaker MT, Fetal Biomaterialia 2009; 5:453-461.
Wound Healing. New York: Elsevier Science Pub- Joly JC, Palloto DB, Martorelli de Lima AF, Mota LF
lishing Co. Inc., 1992; 53-70. and Caffesse R. Clinical and radiographic evaluation
Akncbay H, Senel S and Ay ZY. Application of chitosan of periodontal intrabony defects treated with guided
gel in the treatment of chronic periodontitis. Journal tissue regeneration. A pilot study. Journal of Periodontol-
of Biomedical Materials Research, Part B, Applied Bioma- ogy 2002; 73:353-359.
terials 2007; 80:290–296. Klokkevold PR, Vandemark L, Kenney EB and Bernard
Aksungur P, Sungur A, Unal S, Iskit AB, Squier CA and GW. Osteogenesis enhanced by chitosan (Poly-N-
Senel S. Chitosan delivery systems for the treatment Acetyl Glucosaminoglycan) in vitro. Journal of Peri-
of oral mucositis: In vitro and in vivo studies. Journal odontology 1996; 67:1170-1175.
of Controlled Release 2004; 98:269–279. Krebs KA and Clem DS 3rd. Guidelines for the manage-
Babrawala IS, Prabhuji MLV, Karthikeyan BV and ment of patients with periodontal diseases. Journal of
Khanna D.. A novel approach using natural 1% Periodontology 2006; 77:1607-11.
(w/w) chitosan as a local drug delivery system in the Laurell L, Gottlow J, Zybutz M and Persson R. Treatment
management of non-surgical periodontal treatment: of intrabony defects by different surgical procedures.
a pilot study. Journal of the International Academy of A literature review. Journal of Periodontology 1998;
Periodontology 2016a; 18:129-133. 69:303–13.
Babrawala I, Munivenkatappa LVP and Bangalore VK. Mahajan A and Kedige S. Periodontal bone regeneration
A novel approach using 15% natural chitosan gel in in intrabony defects using osteoconductive bone graft
the management of intrabony defects: A pilot study. versus combination of osteoconductive and oste-
Chinese Journal of Dental Research 2016b; 19:231-237. ostimulative bone graft: A comparative study. Dental
Boynuegri D, Ozcan G, Senel S et al. Clinical and radio- Research Journal (Isfahan) 2015; 12:25–30.
graphic evaluations of chitosan gel in periodontal Malafaya PB and Reis RL. Bilayered chitosan-based scaf-
intraosseous defects: A pilot study. Journal of Bio- folds for osteochondral tissue engineering: influence
medical Materials Research, Part B, Applied Biomaterials of hydroxyapatite on in vitro cytotoxicity and dynamic
2009; 90:461-466. bioactivity studies in a specific double-chamber bio-
Chen J, Li Q, Xu J et al. Study on biocompatibility of reactor. Acta Biomaterialia 2009; 5:644-660.
complexes of collagen-chitosan-sodium hyaluronate Mukherjee DP, Tunkle AS, Roberts RA, Clavenna A, Rog-
and cornea. Artificial Organs 2005; 29:104-113. ers S and Smith D. An animal evaluation of a paste of
Chevrier A, Hoemann CD, Sun J and Buschmann MD. chitosan glutamate and hydroxyapatite as a synthetic
Chitosan glycerol phosphate/ blood implants in- bone graft material. Journal of Biomedical Materials Re-
crease cell recruitment, transient vascularisation and search, Part B, Applied Biomaterials 2003; 67:603–609.
subchondral bone remodelling in drilled cartilage Park YJ, Lee YM, Park SN, Sheen SY, Chung CP and Lee
defects. Osteoarthritis Cartilage 2007; 15:316-327. SJ. Platelet derived growth factor releasing chitosan
Fakhry A, Schneider GB, Zaharias R and Senel S. Chi- sponge for periodontal bone regeneration. Biomaterials
tosan supports the initial attachment and spreading 2000; 21:153–159.
of osteoblasts, preferentially over fibroblasts. Bioma- Senel S, Kas HS and Squier CA. Application of chitosan
terials 2004; 25:2075-2079. in dental drug delivery and therapy. In: Muzzarelli
Garrett S. Periodontal regeneration around natural teeth. RAA (Ed): From Dietary Supplement to Drug Carrier.
Annals of Periodontology 1996; 1:621–666. Italy: Atec, Grottammare; 2000a; 241-256
Giannoudis P, Dinopoulos H and Tsiridis E. Bone sub- Senel S, Ikinci G, Kas S, Yousefi-Rad A, Sargon MF and
stitutes: an update. Injury 2005; 36:20–27. Hıncal AA. Chitosan films and hydrogels of chlorhex-
Gupta SC. Local drug delivery in periodontics. Indian idine gluconate for oral mucosal delivery. International
Journal of Dental Sciences 2010; 2:32-34. Journal of Pharmaceutics 2000b; 193:197- 203.
Ikinci G, Senel S, Akncbay H et al. Effect of chitosan on Shin SY, Park HN, Kim KH et al. Biological evaluation of
a periodontal pathogen, Porphyromonas gingivalis. In- chitosan nanofiber membrane for guided bone regen-
ternational Journal of Pharmaceutics 2002; 235:121-127. eration. Journal of Periodontology 2005; 76:1778–1784.
Jayasuriya AC and Kibbe S. Rapid biomineralization of Silness J and Loe H. Periodontal disease in pregnancy.
chitosan microparticles to apply in bone regenera- II. Correlation between oral hygiene and periodon-
tion. Journal of Materials Science. Materials in Medicine. tal condition. Acta Odontologica Scandinavica 1964;
2010; 21:393-398. 22:121-135.10 Journal of the International Academy of Periodontology (2019) 21/1 Suzuki JB, Goodman SB and Phillips B. Compaision of Wagh A. Chemically Bonded Phosphate Ceramics: Twenty-first clinical healing of human periodontal defects with century materials with diverse applications; Elsevier Sci- HTR synthetic grafts. Journal of Dental Research 1989; ence: New York, NY, USA, 2004. 68:409 (Abstr. 1822). Wang M. Developing bioactive composite materials for Vilasan A, MLV Prabhuji, Karthikeyan BV and Selvan tissue replacement. Biomaterials 2003; 24:2133-2151. A. Control of streptococcus sanguinis oral biofilm by Weir MD and Xu HH. Osteoblastic induction on cal- novel chlorhexidine-chitosan mouthwash: An in vitro cium phosphate cement-chitosan constructs for study. Journal of Experimental and Integrative Medicine bone tissue engineering. Journal of Biomedical Materials 2013; 3:165-169. Research, Part A, 2010; 94:223–233.
You can also read

















































