Vertebral COLUMNS - ISASS - The International ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vertebral
FALL 2020
COLUMNS
International Society for the Advancement of Spine Surgery
FLATTENING
THE MIS
LEARNING CURVE
ALSO
Update on the Impact of COVID-19 on Awake Robot-Assisted Single- Occupational
Use of Intrawound Finances and Growth Plans Lumbar Position Surgery: Health Hazards
Vancomycin of Orthopedic Practices in Fusion The Perfect Application in Spine
Powder the United States Surgery for Robotics? Surgery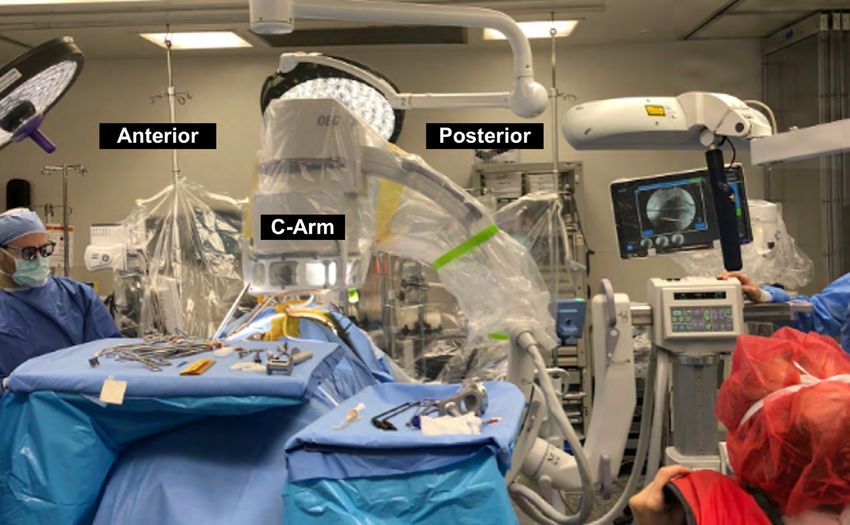
Editor in Chief
Kern Singh, MD
3 EDITORIAL
Flattening the MIS Learning Curve Editorial Board
Peter Derman, MD, MBA
Brandon Hirsch, MD
8 COVID-19
Sravisht Iyer, MD
Impact of COVID-19 on Finances and Growth Plans
Safdar Khan, MD
of Orthopedic Practices in the United States
Yu-Po Lee, MD
Sheeraz Qureshi, MD
14 ROBOTICS
Robot-Assisted Single-Position Surgery: The Perfect
Grant Shifflett, MD
Application for Robotics? Managing Editor
Audrey Lusher
18 ANESTHESIA
Awake Lumbar Fusion Surgery Designer
CavedwellerStudio.com
22 COMPLICATIONS
Update on the Use of Intrawound Vancomycin
Powder
25 PHYSICIAN HEALTH
Occupational Health Hazards in Spine Surgery
Vertebral Columns is published
quarterly by the International Society
for the Advancement of Spine
Become a Surgery.
member
©2020 ISASS. All rights reserved.
today
Opinions of authors and editors do
not necessarily reflect positions
taken by the Society.
This publication is available digitally
https://www.isass.org/about/membership/ at www.isass.org/news/vertebral-
columns-fall-2020
Fall 2020 Vertebral Columns isass.org
EDITORIAL 3
Flattening the MIS Learning Curve
Since the introduction of minimally inva- introduced into surgery by the
sive surgery (MIS), the way in which spine Bristol Royal Infirmary, which
surgeons perform procedures has changed aimed to reduce mortality in
drastically. As a growing body of evidence infants undergoing procedures
has demonstrated, use of MIS techniques for congenital heart disease. 8
and specialized technolog y can lead to Since its inception, surgeons
Conor P. Lynch, MS
shorter operative times and reduced soft have typically assessed prog-
tissue trauma, which in turn can result in ress along the learning curve in
fewer complications and improved postop- terms of reductions in operative
erative outcomes.1,2 Within the past decade, time, blood loss, and rates of
MIS has become more the rule rather than complications. While all sur-
the exception for many spine surgeons, geons aim to become proficient
and it is projected that nearly half of all early in their careers, studies Elliot D.K. Cha, MS
spine procedures in 2020 will involve these suggest the time to proficiency
techniques. 3 The appeal of MIS is rooted in may differ based on the type of
potential benefits not only to the patient, spine procedure.9-11 This raises
but also to the surgeon and team. Such ben- two questions: (1) What aspect(s)
efits include smaller incisions, avoidance of of MIS contribute to the curve?
crushing injury to soft tissue through the and (2) What are the best ways
Kern Singh, MD
use of tubular dilators, and preservation to shorten time to proficiency?
of spine stabilizing muscles.4 Additionally,
for spine surgeons, MIS techniques result Challenges of MIS
in increased operative efficiency, reduced While mastery of some surgical techniques
operative times, and decreased blood loss, can be acquired quite rapidly, significantly
all of which can translate to reduced cost more experience may be required to achieve
and improved outcomes for the patient. 5-7 optimal results for MIS procedures. A case
However, achiev ing prof iciency in MIS series of the senior author’s first 65 prima-
techniques requires a substantial leap in ry MIS transforaminal lumbar interbody
both surgical and team management skills, fusions (TLIF) illustrates this point nicely:
resulting in what some have described as a procedures in the latter half of this series
daunting learning curve. demonstrated significantly better outcomes
Characterized as the progression of re- in terms of surgical and anesthesia duration,
sults as a new skill improves over time, estimated blood loss, and administration
the concept of the learning curve was first of intraoperative fluids.12 Similar trends in
isass.org Vertebral Columns Fall 2020
4 EDITORIAL
As residents, fellows, and new attendings
navigate through their training, there are
While mastery of some surgical
several aspects of MIS to consider that
techniques can be acquired quite contribute to the learning curve. First, the
rapidly, significantly more experience challenge itself is multifactorial, and address-
ing one particular aspect does not result in
may be required to achieve optimal a cure-all effect. Second, exposure to MIS
results for MIS procedures. techniques during a surgeon’s training may
be minimal until he or she begins a spine
operative proficiency were also detailed over fellowship. Limited exposure diminishes
the course of our practice’s experience with familiarity with the challenges posed by MIS
MIS lumbar decompression11 and anterior and limits opportunities to learn from those
cervical discectomy and fusion, where a who have mastered these techniques. Third,
90% proficiency was reached by case 57.13 a surgeon’s training is predicated on visual
The steep initial curve associated with MIS and tactile training in the operating room;
TLIF reflects a period of substantial learning however, MIS drastically reduces not only
and acquisition of pertinent techniques and the visibility window but also the ability to
“tricks” that facilitate a more efficient proce- identify key anatomical landmarks vital to
dure. However, during this time, patients may accurate placement of implants, screws, and
be exposed to a greater risk of complications. use of specific surgical instruments. Finally,
A systematic review of early complications one aspect that adds to the challenge of MIS
associated with the learning curve in MIS that may not be inherently obvious is the
spine surgery detailed that specific types concept of teamwork. The largest benefit to
of procedures may be linked with lower or the technique is its ability to drastically re-
higher rates of complications, with lumbar duce operative time and the associated risks;
decompressions having the lowest rate and however, this benefit can only be realized
MIS TLIF having the highest, with an overall with team-wide efficiency. Given this reality,
rate of 20%.14 To further complicate the matter surgeons must not only navigate the duress
is the potential for a “second wave” of the involved with applying MIS techniques and
learning curve as attendings take on more avoiding lengthened procedures, but they
challenging cases once they have established must also coordinate the surgical team to
a level of comfort with the procedure. This maintain optimal efficiency. If this dynamic
presents an early challenge for surgeons is not appreciated, then the key benefit of
aiming to improve their technique as they MIS spine procedures may be lost. Although
strive to “do no harm” to their patients while some may suggest a steep learning curve is
simultaneously taking full advantage of unavoidable, we highlight several tactics, in
every opportunity to better themselves as the context of MIS TLIF, that may be used
MIS spine surgeons. to “flatten” the curve.
Fall 2020 Vertebral Columns isass.org
EDITORIAL 5 Flattening the Curve Perhaps the most straightforward way for junior surgeons to improve operative out- comes for their MIS TLIF procedures is to simply perform more of them, as it has been well established that outcomes are more fa- vorable after surgeons have a considerable number of TLIF procedures under their belt. Silva et al9 demonstrated a 50% improvement in surgeons’ proficiency by their 12th MIS TLIF procedure; by their 39th case, they had achieved a 90% “learning milestone.” They and the use of intraoperative instruments were also able to demonstrate a consider- and technology. Smaller approach windows able reduction in their rate of complications place increased reliance on a team’s ability over this series of procedures. The obvious to track the procedure’s stage without direct downside of learning through experience visualization and coordinate with the sur- is that it necessitates that some outcomes geon to effectively perform their roles. To will inherently be less than optimal for the this end, standardization of every possible earlier procedures toward the “left end” of part of the process is key. From instrument the learning curve. Although this has been trays to team positioning to the procedural the traditional model for learning surgery steps themselves, the more consistency and and most aspects of medical practice, it may predictability that is incorporated, the better not be agreeable to those patients who are the surgeon and team can be prepared for among a surgeon’s first few patients as an success. independent practitioner. With this in mind, As a newer surgeon seeks to begin his or it is important to consider ways to maximize her practice of MIS, the guidance and men- a surgeon’s proficiency with MIS procedures torship of a more senior surgeon who has from day one. mastered the MIS technique can be invaluable Before the proficiency of the surgeons for appreciating the subtleties of the craft themselves is addressed, one should consid- and avoiding crucial errors. The model of er that the surgical team is one of the most apprenticeship is quite standard to medical important factors for a successful procedure. practice, with residents and fellows learning For any procedure to be performed in a safe, under the guidance of experienced attending efficient manner, the performance of the physicians. However, for specialized spine surgical team must be optimized. For MIS procedures such as the MIS TLIF, residents procedures, it is especially important that and fellows may receive relatively little ex- the team is highly familiar with the steps of posure during their regular training. As the the operation, the necessary preparation, role of MIS TLIF continues to expand in spine isass.org Vertebral Columns Fall 2020

6 EDITORIAL
surgery, it will become important to increase and allow senior surgeons to provide more
the opportunities available to trainees to gain direct guidance and feedback. In one study,
experience in such techniques while under AR technology known as the VIPAR system
the mentorship of an expert. Since many MIS allowed surgeons in Birmingham, Alabama,
procedures are performed in the setting of to provide real-time input and guidance for
ambulatory surgical centers, exposure for neurosurgery procedures performed in Ho
residents and fellows who primarily rotate Chi Minh City, Vietnam.17 In addition to al-
in hospital settings may be further limited. lowing audio and visual correspondence with
Therefore, it will be important for training minimal (approximately a 237 millisecond)
programs to consider how to incorporate delay, this system allowed the surgeons in
procedures performed in ambulatory settings Vietnam to receive direct video overlay of
more thoroughly in their curriculum. hand movements and gestures made by their
While mentorship from those who have collaborators in Alabama. The applications of
mastered the technique is assuredly invalu- such technology for resident/fellow training
able, junior surgeons must be able to practice are numerous. Especially for procedures such
“hands on” in order to become proficient. as the MIS TLIF, where direct visualization
Augmented reality (AR) and virtual reality and operative space are extremely limited,
(VR) technologies can offer an excellent such a visual overlay and “virtual” gesturing
opportunity for trainees to obtain this ex- could be invaluable to allow senior surgeons
perience without compromising the safety to monitor and instruct their trainees while
of patients. Simulated surgical procedures still allowing the junior surgeons to get di-
using VR technology have allowed trainees rect, hands-on surgical experience.
to practice and receive feedback, resulting Implementation of robotic surgery in the
in signif icant improvements in perfor- operating room continues to expand as
mance of techniques such as lateral mass technology advances and its use becomes
screw placement.15 Additionally, a VR-based more accepted. For hig h ly dema nding
training model for pedicle screw placement spine procedures such as the MIS TLIF,
that utilized haptic feedback and realistic robotics can provide increased precision
visual tracking was tested with 51 fellows and facilitate more predictable, calculated
at the American Association of Neurological i nt raoperat ive movement s. For ex a m-
Surgeons annual meeting and demonstrat- ple, robotic surger y can remove human
ed substantial benefits in terms of learning error to a certain degree and use native
retention and accuracy improvement.16 image mapping to plan trajectories for
While VR has been helpful for “preop- demanding operat ions such as pedicle
erative” training, which is fully removed screw placement.18 However, use of robotic
from actual patient care, AR technolog y surger y may result in slower procedures
has implications for “real life” surgical set- and increased operative duration com-
tings to improve the safety of procedures pared to more traditional operations. 19
Fall 2020 Vertebral Columns isass.org
EDITORIAL 7
The precise role that robotic surger y will to facilitate early hands-on experience will
play in the reduction of the MIS curve is represent a substantial force to help flatten
currently unclear, and increased famil- the MIS learning curve. Although not every
iarity and development will be required physician will have access to cutting-edge
to fully appreciate the advantages it offers technology such as AR and VR, the use of
to spine surgeons. MIS techniques in spine surgery as well as
other surgical domains will continue to grow.
How to Improve? With increasing popularity and benefits
Many challenges young attendings w ill to the patient, surgical training programs
face during the refinement of their oper- may begin to expand the integration of
ative techniques are unavoidable; howev- MIS techniques in their curriculum to help
er, integration of both early exposure for trainees and young attendings flatten the
trainees and use of innovative technology MIS learning curve. n
References
1. Sayari AJ, Patel DV, Yoo JS, Singh K. 8. Subramonian K, Muir G. The “learning 15. Gottschalk MB, Yoon ST, Park DK, Rhee
Device solutions for a challenging spine curve” in surgery: what is it, how do JM, Mitchell PM. Surgical training
surgery: minimally invasive transforaminal we measure it and can we influence using three-dimensional simulation
lumbar interbody fusion (MIS TLIF). Expert it? BJU Int. 2004;93(9):1173-1174. in placement of cervical lateral mass
Rev Med Devices. 2019;16(4):299-305. screws: a blinded randomized control
9. Silva PS, Pereira P, Monteiro P, Silva
trial. Spine J. 2015;15(1):168-175.
2. Qin R, Liu B, Zhou P, et al. Minimally inva- PA, Vaz R. Learning curve and com-
sive versus traditional open transforaminal plications of minimally invasive trans- 16. Luciano CJ, Banerjee PP, Bellotte B, et
lumbar interbody fusion for the treatment foraminal lumbar interbody fusion. al. Learning retention of thoracic pedicle
of single-level spondylolisthesis grades 1 Neurosurg Focus. 2013;35(2):E7. screw placement using a high-resolution
and 2: a systematic review and meta-anal- augmented reality simulator with haptic
10. Lee KH, Yeo W, Soeharno H, Yue WM.
ysis. World Neurosurg. 2019;122:180-189. feedback. Neurosurgery. 2011;69(1 suppl
Learning curve of a complex surgical
operative):ons14-ons19; discussion ons19.
3. Phillips FM, Cheng I, Rampersaud YR, et technique: minimally invasive transforam-
al. Breaking through the “glass ceiling” of inal lumbar interbody fusion (MIS TLIF). J 17. Davis MC, Can DD, Pindrik J, Rocque BG,
minimally invasive spine surgery. Spine Spinal Disord Tech. 2014;27(7):E234-E240. Johnston JM. Virtual interactive presence
(Phila Pa 1976). 2016;41(suppl 8):S39-S43. in global surgical education: international
11. Ahn J, Iqbal A, Manning BT, et al.
collaboration through augmented reality.
4. Sharif S, Afsar A. Learning curve and Minimally invasive lumbar decom-
World Neurosurg. 2016;86:103-111.
minimally invasive spine surgery. pression—the surgical learning curve.
World Neurosurg. 2018;119:472-478. Spine J. 2016;16(8):909-916. 18. Lieberman IH, Kisinde S, Hesselbach-
er S. Robotic-assisted pedicle screw
5. Phan K, Hogan JA, Mobbs RJ. Cost-util- 12. Nandyala SV, Fineberg SJ, Pelton M, Singh
placement during spine surgery. JBJS
ity of minimally invasive versus open K. Minimally invasive transforaminal lum-
Essent Surg Tech. 2020;10(2):e0020.
transforaminal lumbar interbody fusion: bar interbody fusion: one surgeon’s learn-
systematic review and economic evalua- ing curve. Spine J. 2014;14(8):1460-1465. 19. Wang T, Hamouda F, Sankey EW, Goodwin
tion. Eur Spine J. 2015;24(11):2503-2513. CR, Karikari IO, Abd-El-Barr M. Operative
13. Mayo BC, Massel DH, Bohl DD, Long
time and learning curve between conven-
6. Al-Khouja LT, Baron EM, Johnson JP, Kim WW, Modi KD, Singh K. Anterior cer-
tional fluoroscopy, fluoroscopy-based
TT, Drazin D. Cost-effectiveness analy- vical discectomy and fusion: the
instrument navigation, and robot-as-
sis in minimally invasive spine surgery. surgical learning curve. Spine (Phila
sisted instrumentation in minimally
Neurosurg Focus. 2014;36(6):E4. Pa 1976). 2016;41(20):1580-1585.
invasive transforaminal lumbar inter-
7. Hammad A, Wirries A, Ardeshiri A, Nikifor- 14. Sclafani JA, Kim CW. Complications body fusion (MIS-TLIF) [abstract P36].
ov O, Geiger F. Open versus minimally inva- associated with the initial learning Spine J. 2020;20(9 suppl):S163-S164.
sive TLIF: literature review and meta-anal- curve of minimally invasive spine sur-
ysis. J Orthop Surg Res. 2019;14(1):229. gery: a systematic review. Clin Orthop
Relat Res. 2014;472(6):1711-1717.
isass.org Vertebral Columns Fall 2020
8 COVID-19
Impact of COVID-19 on Finances
and Growth Plans of Orthopedic
Practices in the United States
In December 2019, a novel coro- affected in the early stages of the pan-
navirus, severe acute respira- demic, the near-term projected healthcare
tor y syndrome coronavirus-2 outlook, and how this outlook may impact
(SARS-CoV-2) or coronavirus-19 the growth plans of orthopedic practices
(COVID-19), was discovered in in the United States.
the People’s Republic of China1
Ram Alluri, MD
and quickly evolved into a glob- Immediate Financial Impact of COVID-19
al pandemic. As of October 2, on Orthopedic Practices
2020, the virus has infected 188 In Februar y and March 2020, COVID-19
countries/regions, resulting in cases continued to increase throughout
34,353,480 confirmed infections the United States, raising concerns about
and 1,023,983 deaths.2 Estimates t he ava i labi l it y of protect ive persona l
project that COVID-19 will be equ ipment (PPE) a nd t he prospec t of
Ahilan Sivaganesan, MD one of the top three cause of healthcare rationing as hospitals reached
death in the United States in surge capacity. In response to this growing
2020. 3 Aside from the substan- concern, on March 18, 2020, the Centers
tial morbidity and mortality due for Medicare and Medicaid Services (CMS)
to the viral infection, attempts mandated that all elective surgeries be
to control the virus have result- delayed in an attempt to preser ve PPE,
ed in global economic instabil- inpatient hospital beds, and ventilators.
ity and significant changes to Additionally, healthcare providers were
Sheeraz Qureshi, MD
societal norms. Businesses have instructed to encourage patients to remain
been forced to rapidly adapt to at home, barring an emergency, to limit the
stay-at-home orders and social distancing populace’s exposure to the virus and best
precautions while attempting to remain comply with local stay-at-home orders.
financially solvent. Hospital systems and The moratorium on elective procedures,
medical pract ices are no except ion. In which lasted several months in some re-
this review, we discuss specifically how gions, and the concomitant reduction in
orthopedic practices have been financially clinic volume had a signif icant impact
Fall 2020 Vertebral Columns isass.org
COVID-19 9 on the revenue f low of many orthopedic ing expenditures, large healthcare systems prac t ices. Some st ud ies est i mate t hat throughout the country made substantial or t hopedic surg ica l volume decreased changes to their payroll structure by fur- by approximately 90% and clinic volume loughing employees, reducing salaries for decreased by approximately 70% during administrative staff, and withholding pay this period.4,5 This abrupt and substantial from orthopedic surgeons.4,8 As a case in decrease in patient care jeopardized the point, the Mayo Clinic has been projected f inancial integrit y of many ort hopedic to lose $900 million in 2020 revenue, despite practices, which rely on these sources of furloughing workers and decreasing physi- revenue to pay for office overhead, other cian pay.9 University Hospitals in Cleveland fixed costs, and ongoing capital expendi- is facing a similar financial problem and tures. 6 It was projected by some surveys has temporarily decreased physician pay that one third of multispecialty physician by 7% to 10%.10 Even well-regarded ortho- groups would run out of cash-on-hand pedic groups such as the Rothman Institute within weeks if clinical and surgical vol- face financial adversity, with a projected ume continued to remain low.7 $120 million revenue loss, and therefore In an attempt to combat the stark imbal- temporarily closed offices, reduced the ance between incoming revenue and outgo- effective number of full-time employees isass.org Vertebral Columns Fall 2020

10 COVID-19
healthcare providers, and patients. Some
practices invested in the infrastructure to
Approximate
-90%
support care via telemedicine, which can
decrease in orthopedic be costly.14 From a surgical standpoint,
surgical volume many practices began to test their patients
preoperatively for COVID-19 and provide
addit ional PPE to minimize t he risk of
nosocomial transmission of COV ID-19.
Wit h each subsequent challenge, costs
Approximate
-70%
increased while the efficiency of providing
decrease in orthopedic care decreased after the release
clinic volume of the moratorium on elective cases.
As practices adapted to providing care
in this new healthcare reality, predicting
by 50%, instituted structured salary reduc- the expected clinical volume remained
tions for management staff, and eliminated difficult. One study reported that nearly
salaries for full shareholders in the month 90% of pat ients planned to reschedu le
of April.4 Significant salary reductions and their orthopaedic care as soon as possible, 5
decreased clinical operations also took while other clinicians reported that, even
place at Midwest Orthopaedics at Rush, af ter an init ial rebound, clinic volume
OrthoCarolina, New England Orthopedic remained 40% lower than before the pan-
Surgeons, and other private orthopedic demic.15 Anecdotally, we noted an initial
groups throughout the United States.4,11,12 surge in scheduled surgeries throughout
In May 2020, CMS released guidelines July 2020, primarily stemming from pa-
for t he cont rol led resu mpt ion of elec- tients whose elective surgeries had been
tive procedures based on local and state deferred, as opposed to new patients. In
guidelines and hospital discretion.13 Many August 2020, clinic and operative volume
or t hopedic pract ices felt a substant ia l s l ig ht l y t apered a nd rem a i ned below
economic imperative to rapidly increase pre-pandemic numbers.
clinical and surgical volume to compen-
sate for months of revenue loss. However, Healthcare Outlook
ma ny of t hese prac t ic es encou ntered Before the COV ID-19 pandemic, the or-
sig nif icant log ist ical challenges in t he thopedic industry was experiencing strong
clinic and operating room. Practices had growth, with 3.5% and 3.8% year-over-year
to shift responsibilities to facilitate some expansion in 2018 and 2019, respectively.16
staf f to work f rom home. Addit iona lly, Some subspecialties within orthopedics
clinics had to be reorganized to allow for demonstrated even higher year-over-year
adequate social distancing of office staff, growth ranging from 5% to 6% in 2018 and
Fall 2020 Vertebral Columns isass.orgCOVID-19 11 2019.16 However, the onset of the pandem- and 2021. 21,22 ic abruptly reversed these steady growth Although it is difficult to predict when trends and brought about widespread un- surgical volume will return to pre-pan- certainty regarding the economic outlook demic numbers, 28% of orthopedic sur- for the healthcare industry. Although the geons believe this will not occur until the immediate short-term impact of the ongo- second half of 2021. 23 Optimistically, one ing pandemic is difficult to gauge, if one study estimated that orthopedic surgery uses medical dev ice sales as a possible volume may reach 90% of pre-pandemic surrogate, volume has decreased 30% to volume in early 2021, but, in a pessimistic 47% in the second quarter of 2020.17,18 scenario, others predict that volume may The recovery of the healthcare sector, and not normalize until late 2021, 24 while still in particular elective orthopedic surgery, others expect the effects of the pandemic is incredibly difficult to predict due to the to last beyond 2022.16 uncertainty regarding a possible second wave of v iral spread, potent ial an x iet y Impact on Growth Plans of t he general populace when entering In the setting of this uncertainty, health- healthcare facilities, decreased activit y ca re prov iders a nd orga n i zat ions w i l l due to social distancing (thereby possibly attempt to limit variable costs, decrease decreasing orthopedic injuries), and the fixed costs, consider consolidation, and uncertainty about the timing and efficacy of limit or suspend previously planned growth a future vaccine. Given the unprecedented and capital investments. Consolidation nature of this pandemic in the modern era, of healthcare practices may allow for the many have turned to the Great Recession sharing of fixed cost, thereby decreasing of 2008 for insight. During an economic overhead, but it may limit the autonomy of recession, t he volume of most elect ive orthopedic providers and decrease surgeon procedures is ex pected to decrease, in choice for patients. Additional strategies to part due to changes in insurance cover- control costs may involve the suspension age and increasing unemployment.19 In of ongoing construction, such as a $120 the first year after the Great Recession of million spine tower or a $10 million sports 2008, a survey conducted by the American medicine center. 25,26 Associat ion of Hip and K nee Surgeons Perhaps the greatest aspect of orthopedic (A A HKS) found t hat bot h surg ica l and growth to be impacted by the COVID-19 clinic volume decreased approx imately pandemic will be the hiring of new ortho- 30%. 20 Given that unemployment rates are pedic surgeons. The recruitment of new currently two to three times higher than orthopedic surgeons into existing practices they were during the Great Recession of will likely be tempered for the next few years 2008, it is not unreasonable to predict an until surgical volume increases and original even greater decrease in volume in 2020 workforces are restored to pre-pandemic isass.org Vertebral Columns Fall 2020
12 COVID-19
levels. In the current pandemic, one study and seeking first-time employment. Some
reported that 50% of orthopedic surgeons orthopedic groups have already withdrawn
sustained a decrease in compensation, 27 employ ment offers to residents/fellows
further prov iding impetus to limit new as a result of the COVID-19 pandemic. 27
hiring until revenue for currently employed Unfortunately, this unfavorable job envi-
orthopedic surgeons returns to normal. ronment for residents and fellows entering
Lastly, in prior recessions, some orthopedic the workforce in 2020 and 2021 may ne-
surgeons reported a 30% loss of retirement cessitate choosing a position in locations
savings, prompting surgeons to delay retire- that are sub-optimal for a given trainee
ment and in turn constricting opportunities but have a greater demand for orthopedic
for new hires to enter existing practices. 20 care. Additionally, trainees may consider
Limited recruitment of new orthopedic locums work, allowing for flexibility should
surgeons will have the greatest impact on the job market improve in a desired geo-
trainees finishing residency or fellowship graphic area. Those trainees who do find
References
1. Zhu N, Zhang D, Wang W, et al. A nov- 7. Stewart A. Washington state survey: 31% 11. Dyrda L. Massachusetts orthopedic group
el coronavirus from patients with of solo, multispecialty group physicians halts physician pay, furloughs employ-
pneumonia in China, 2019. N Engl will run out of cash within weeks. Beck- ees due to the coronavirus: 4 details.
J Med. 2020;382(8):727-733. er’s Healthcare. April 24, 2020. https:// Becker’s Healthcare. March 24, 2020.
www.beckersasc.com/asc-coding-bill- https://www.beckersspine.com/orthope-
2. Coronavirus resource center. Johns
ing-and-collections/washington-state-sur- dic-spine-practices-improving-profits/
Hopkins University and Medicine web-
vey-31-of-solo-multispecialty-group-phy- item/48640-massachusetts-ortho-
site. https://coronavirus.jhu.edu/map.
sicians-will-run-out-of-cash-within-weeks. pedic-group-halts-physician-pay-fur-
html. Accessed August 28, 2020.
html. Accessed August 28, 2020. loughs-employees-due-to-the-coro-
3. Bean M. COVID-19 is 3rd leading cause of navirus-4-details.html. Accessed
8. O’Connor CM, Anoushiravani AA, DiCap-
death, STAT analysis suggests. Beck- August 28, 2020.
rio MR, Healy WL, Iorio R. Economic
er’s Healthcare. May 1, 2020. https://
recovery after the COVID-19 pan- 12. Stewart A. Orthopedic group cut pay for
www.beckershospitalreview.com/
demic: resuming elective orthopedic 60 physicians, retained 93% of staff after
public-health/covid-19-is-3rd-lead-
surgery and total joint arthroplasty. J volumes vanished. Becker’s Healthcare.
ing-cause-of-death-stat-analysis-sug-
Arthroplasty. 2020;35(7S):S32-S36. July 17, 2020. https://www.beckersspine.
gests. Accessed August 28, 2020.
com/orthopedic/item/49584-orthope-
9. Haefner M. Mayo Clinic projects $900M
4. Vaccaro AR, Getz CL, Cohen BE, Cole BJ, dic-group-cut-pay-for-60-physicians-re-
shortfall, implements cost-cutting
Donnally CJ III. Practice management tained-93-of-staff-after-volumes-vanished.
measures. Becker’s Healthcare. April 10,
during the COVID-19 pandemic. J Am html. Accessed August 28, 2020.
2020. https://www.beckershospitalreview.
Acad Orthop Surg. 2020;28(11):464-470.
com/finance/mayo-clinic-projects-900m- 13. Center for Medicare & Medicaid Services.
5. Mo AZ, Mont MA, Grossman EL, et al. shortfall-implements-cost-cutting-mea- Opening Up America Again: Centers for
The effect of the COVID-19 pandem- sures.html. Accessed August 28, 2020. Medicare & Medicaid Services (CMS)
ic on orthopedic practices in New Recommendations. Re-opening Facilities
10. Paavola A. University Hospitals to cut
York. Orthopedics. 2020;43(4):245. to Provide Nonemergent Non-COVID-19
all physician pay. Becker’s Healthcare.
6. Sathiyakumar V, Jahangir AA, Mir HR, et Healthcare: Phase I. https://www.cms.gov/
June 4, 2020. https://www.beckersspine.
al. Patterns of costs and spending among files/document/covid-flexibility-reopen-es-
com/orthopedic-spine-practices-im-
orthopedic surgeons across the United sential-non-covid-services.pdf. Posted
proving-profits/item/49235-universi-
States: a national survey. Am J Orthop April 19, 2020. Accessed August 28, 2020.
ty-hospitals-to-cut-all-physician-pay.
(Belle Mead NJ). 2014;43(1):E7-E13. html. Accessed August 28, 2020.
Fall 2020 Vertebral Columns isass.orgCOVID-19 13
jobs may seek to sign contracts with more virus has resulted in a marked decrease in
guaranteed income in lieu of contracts with orthopedic clinical and surgical volume,
performance incentives, whereas those economically straining orthopedic practic-
groups hiring new trainees may seek to es and necessitating temporary decreases
offer contracts of the opposite structure, in staff and compensation. When clinical
thereby hedging their risk if a new hire’s volume will return to near pre-pandemic
practice does not generate significant rev- levels is unk now n. A rapid turnaround
enue in part due to the pandemic. may occur if an effective vaccine is de-
veloped with lasting immunity, but even
Conclusion in that scenario, it may take several years
Ultimately, much remains to be seen re- for orthopedic practices to fully recover
garding the impact of COV ID-19 on the financially and resume previous plans for
growth plans of orthopedic practices in the growth and expansion. n
United States. The immediate impact of the
References
14. PR Newswire. GlobalMed simplifies 18. Stewart A. Zimmer Biomet’s worldwide 23. Pedersen A. Is the bounce-back in
telehealth costs for clinicians with its new knee sales plummet 46.8% in Q2, hitting orthopedic surgery volumes sustainable
cost simplified solution [news release]. $374M. Becker’s Healthcare. August 4, as COVID-19 cases surge? MD+DI. July
April 30, 2018. https://www.prnewswire. 2020. https://www.beckersspine.com/or- 13, 2020. https://www.mddionline.com/
com/news-releases/globalmed-simplifies- thopedic-a-spine-device-a-implant-news/ orthopedic/bounce-back-orthopedic-
telehealth-costs-for-clinicians-with-its- item/49711-zimmer-biomet-s-worldwide- surgery-volumes-sustainable-covid-19-
new-cost-simplified-solution-300639161. knee-sales-plummet-46-8-in-q2-hitting- cases-surge. Accessed August 28, 2020.
html. Accessed August 28, 2020. 374m.html. Accessed August 28, 2020.
24. Jain A, Jain P, Aggarwal S. SARS-CoV-2
15. Oliver E. Despite rebound, outpatient 19. Fujihara N, Lark ME, Fujihara Y, Chung KC. impact on elective orthopaedic surgery:
visits still 40% lower than before. The effect of economic downturn on the implications for post-pandemic recovery.
Becker’s Healthcare. June 26, 2020. volume of surgical procedures: a system- J Bone Joint Surg Am. 2020;102(13):e68.
https://www.beckersspine.com/orthope- atic review. Int J Surg. 2017;44:56-63.
25. Condon A. $10M sports medicine center at
dic-spine-practices-improving-profits/
20. Iorio R, Davis CM 3rd, Healy WL, Fehring Texas hospital delayed until 2021. Becker’s
item/49437-despite-rebound-outpa-
TK, O’Connor MI, York S. Impact of the Healthcare. June 12, 2020. https://www.
tient-visits-still-40-lower-than-before.
economic downturn on adult reconstruc- beckersspine.com/sports-medicine/
html. Accessed August 28, 2020.
tion surgery: a survey of the American item/49301-10m-sports-medicine-cen-
16. Bonezone. Orthopedic outlook: COVID-19’s Association of Hip and Knee Surgeons. ter-at-texas-hospital-delayed-until-2021.
impact on industry growth and trends. J Arthroplasty. 2010;25(7):1005-1014. html. Accessed August 28, 2020.
June 9, 2020. https://www.bonezonepub.
21. Monthly labor review. U.S. Bureau of Labor 26. Condon A. Texas hospital suspends
com/2710-orthopedic-outlook-covid-
Statistics. https://www.bls.gov/opub/ construction of $120M spine tower due to
19-s-impact-on-industry-growth-and-
mlr/2008/. Accessed August 28, 2020. economic challenges. Becker’s Healthcare.
trends. Accessed August 28, 2020.
June 22, 2020. https://www.beckersspine.
22. Chaney S, Guilford G. Millions of
17. Condon A. NuVasive Q2 net sales down com/orthopedic-spine-practices-improv-
U.S. workers filed for unemployment
30%, unclear if growth will return by end ing-profits/item/49381-texas-hospital-
benefits last week. The Wall Street
of 2020: 6 insights from CEO Chris Barry. suspends-construction-of-120m-spine-
Journal. April 23, 2020. https://www.
Becker’s Healthcare. August 5, 2020. tower-due-to-economic-challenges.
wsj.com/articles/millions-of-u-s-work-
https://www.beckersspine.com/ortho- html. Accessed August 28, 2020.
ers-continue-to-seek-unemployment-
pedic-a-spine-device-a-implant-news/
help-amid-coronavirus-11587634201. 27. Culp BM, Frisch NB. COVID-19 impact on
item/49715-nuvasive-q2-net-sales-down-
Accessed August 28, 2020. young arthroplasty surgeons. J Arthro-
30-unclear-if-growth-will-return-by-end-
plasty. 2020;35(7 suppl):S42-S44.
of-2020-6-insights-from-ceo-chris-barry.
html. Accessed August 28, 2020.
isass.org Vertebral Columns Fall 202014 ROBOTICS
Robot-Assisted Single-Position
Surgery: The Perfect Application
for Robotics?
Over the past 5 years, it seems using less radiation per case in the robot group.
nearly every implant company has These findings demonstrate that robotic screw
introduced or plans to introduce placement is at least as accurate as freehand
a robotics-based platform for and fluoroscopically guided techniques and
spinal instrumentation. Someone are an important proof of concept for this
with a cynical perspective on this new technology.
new technology might argue that However, such findings are not without a
the growth in robotics is driven caveat, as fewer studies have been performed
Sravisht Iyer, MD
purely by a business model. Just comparing robotics to computer-based nav-
like iPhone users must rely on igation. This is an important comparison to
the App Store for apps, hospital make, as navigation is less expensive and
systems that have absorbed the serves as an “open” platform that is typically
substantial capital expense of a interoperable with multiple implant systems.
robot are tightly tied to the same Robotic-assisted spine surgery is, however,
company’s implants to maximize arriving at an opportune time given recent
efficiency and compatibility. developments in surgical technique. As spine
There is, however, a reasonably surgeons have adopted more minimally inva-
Lauren Barber, MD
strong clinical case to be made for sive surgery (MIS) techniques, we have moved
robotics. For instance, in a study toward more lateral- and anterior-based
comparing robotic-assisted placement to approaches to treat degenerative pathology
fluoroscopic-guided freehand placement of and spinal deformity. MIS approaches have
2,937 lumbar pedicle screws in 597 patients lower rates of intraoperative complications
and 12 cadavers, a significant increase in compared to open and hybrid approaches. Ad-
“perfect” and “clinically acceptable” place- ditionally, MIS may enable shorter constructs
ment was demonstrated using robotic-assisted in deformity surgery without compromising
technology.1 Similarly, Han et al2 conducted a outcomes. Furthermore, lateral and anterior
randomized controlled trial of 1,116 pedicles approaches to the spine allow for placement
in 234 patients and found no screw repositions of large interbody implants that limit sub-
were required in the robot cohort, whereas 2 sidence and maximize the available surface
were required in the freehand group despite area for fusion, alignment correction, and
Fall 2020 Vertebral Columns isass.orgROBOTICS 15
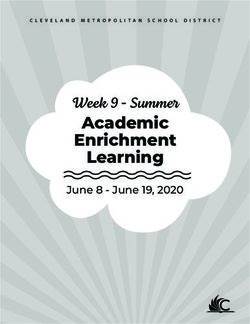
indirect decompression. These advantages Figure 1. Screw
placement using
have led several investigators to attempt lateral robotic-assisted
interbody fusion with percutaneous screws single-position
surgery.
placed in the lateral position (single-position
surgery).
Although experience with this technique
is limited, preliminary results have shown
that single-position surgery demonstrates
no difference in any outcome measure (in-
cluding alignment correction and indirect
decompression), but it saves 30 to 60 minutes
of operating room time when compared to tions and may represent an ideal platform
lateral-then-prone surgery.6,7 However, single to demonstrate the added value of robotics.
position surgery is technically challenging: it Our early experience with RASP has been
requires surgeons to place pedicle screws in largely positive. In our first 10 cases, more
an unfamiliar orientation, is not conducive to than 98% of screws were placed without the
most available navigation techniques, and (in need for repositioning (Figure 1), and the
its current state) requires significant amounts safety profile was acceptable, with no intra-
of fluoroscopy and radiation exposure. operative complications and no substantial
Robotic-assisted single-position (RASP) radiation. The use of robotics allows us to
surgery circumvents many of these limita- place the “down” sided pedicle screws with
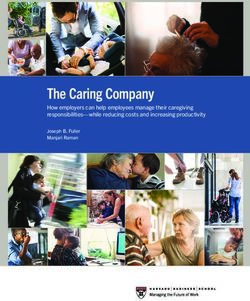
Figure 2.
Patient
positioning and
draping for ro-
botic-assisted
single-position
surgery.
isass.org Vertebral Columns Fall 202016 ROBOTICS
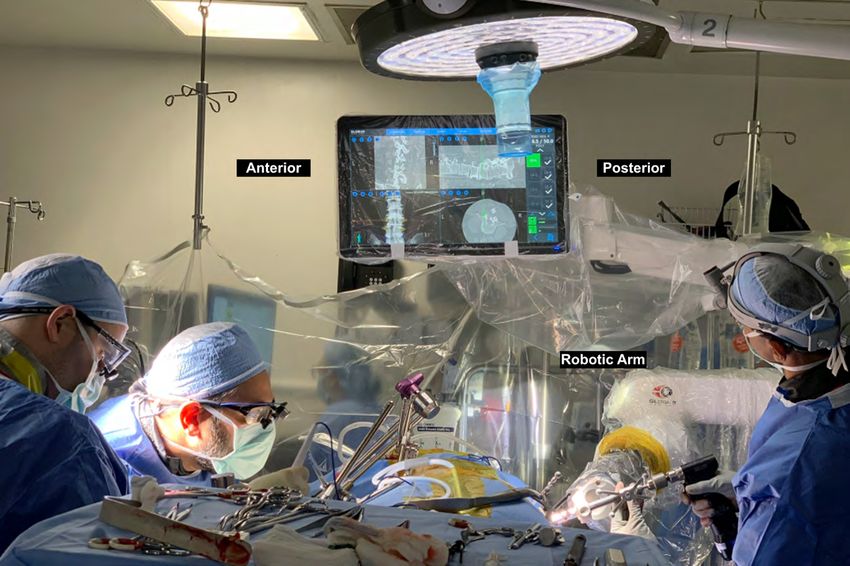
Figure 3.
C-arm posi-
tioning for ro-
botic-assisted
single-position
surgery.
Figure 4.
Robotic arm
positioning for
robotic-assist-
ed single-posi-
tion surgery.
Fall 2020 Vertebral Columns isass.orgROBOTICS 17
relatively little difficulty and minimizes the important to be completely below the vascular
need for fluoroscopy compared to free-hand bifurcation and beware of the “Mickey Mouse”
techniques. psoas, in which the vessels are more lateral
As with most new techniques, obstacles and the plexus more anterior. Additionally,
have been revealed during the early stages patients with a high pelvic incidence can
of use. Given current limitations in both pose difficulties for robot access and thus
navigation and robotics, registration and require freehand placement, which can be
positioning can be difficult for patients with technically difficult in the lateral position.
high body mass indexes. For RASP surgery, Similarly, a narrow pelvis can make placing
patients are positioned laterally on their side L5-S1 screws difficult, so pelvic orientation
while both the anterior or lateral, as well as is of particular importance when deciding
the posterior, exposures are draped into the if a patient is a candidate for RASP surgery.
sterile field (Figure 2). The C-arm comes in Overall, RASP surgery allows for safe treat-
posteriorly to the patient (Figure 3) with ment of many lumbar pathologies, significant
the monitor positioned within the eyeline time savings, less radiation, and likely im-
anteriorly. The robot is positioned posteriorly proved screw accuracy compared to freehand
as well (Figure 4). With the assistance of an or fluoroscopic techniques. The robotic arm
access surgeon, the anterior exposure can provides guidance in a position where many
happen simultaneously with the placement surgeons do not yet have muscle memory. As
of posterior percutaneous screws. such, the use of robotics in single position
As the indications for MIS approaches and lumbar surgery can assist in overcoming
RASP surgery continue to expand, a few pa- the learning curve of using navigation in an
tient-related relative contraindications have unfamiliar position and may be the perfect
become clear. To maintain a safe corridor, it is application of robotics. n
References
1. Fan Y, Du JP, Liu JJ, et al. Accuracy of pedicle screw place- ous robotic-guided, pedicle screw placement. Eur Spine J.
ment comparing robot-assisted technology and the free-hand 2011;20(6):860-868. hptts://doi.org/10.1007/s00586-011-1729-2
with fluoroscopy-guided method in spine surgery: an updat-
5. Moore LJ, Wilson MR, McGrath JS, Waine E, Masters RSW, Vine
ed meta-analysis. Medicine (Baltimore). 2018;97(22):e10970.
SJ. Surgeons’ display reduced mental effort and workload while
hptts://doi.org/10.1097/MD.0000000000010970
performing robotically assisted surgical tasks, when compared
2. Han X, Tian W, Liu Y, et al. Safety and accuracy of robot-assisted to conventional laparoscopy. Surg Endosc. 2015;29(9):2553-
versus fluoroscopy-assisted pedicle screw insertion in thoracolum- 2560. hptts://doi.org/10.1007/s00464-014-3967-y
bar spinal surgery: a prospective randomized controlled trial. J Neu-
6. Hiyama A, Katoh H, Sakai D, Sato M, Tanaka M, Watanabe
rosurg Spine. 2019;1-8. hptts://doi.org/10.3171/2018.10.SPINE18487
M. Comparison of radiological changes after single-po-
3. Hyun SJ, Kim KJ, Jahng TA, Kim HJ. Minimally invasive robotic sition versus dual-position for lateral interbody fusion
versus open fluoroscopic-guided spinal instrumented fusions: a and pedicle screw fixation. BMC Musculoskelet Disord.
randomized controlled trial. Spine (Phila Pa 1976). 2017;42(6):353- 2019;20(1):601. hptts://doi.org/10.1186/s12891-019-2992-3
358. hptts://doi.org/10.1097/BRS.0000000000001778
7. Ziino C, Konopka JA, Ajiboye RM, Ledesma JB, Koltsov JCB,
4. Kantelhardt SR, Martinez R, Baerwinkel S, Burger R, Giese A, Cheng I. Single position versus lateral-then-prone positioning for
Rohde V. Perioperative course and accuracy of screw posi- lateral interbody fusion and pedicle screw fixation. J Spine Surg.
tioning in conventional, open robotic-guided and percutane- 2018;4(4):717-724. hptts://doi.org/10.21037/jss.2018.12.03
isass.org Vertebral Columns Fall 202018 ANESTHESIA
Awake Lumbar Fusion Surgery
Advances in perioperative proto- degenerative pathology refractory to conser-
cols,1 regional anesthesia,2-4 and vative care. Patients with anxiety or mental
surgical techniques 5-8 have led health conditions may not tolerate awake
to a recent rise in awake spine surgery, and other relative contraindica-
surger y. Proponents of awake tions include poor respiratory reserve and
spine surgery cite improved pa- morbid obesity. Of note, spinal implants and
tient satisfaction, reduced costs, anesthetics are frequently used off-label in
Alexander Satin, MD improved outcomes, accelerated these techniques.
rehabilitation, and enhanced In this article, we detail modern surgi-
neuromonitoring capabilities cal and anesthetic techniques for awake
when spine surgery is performed lumbar fusion surgery, which builds upon
without general endotracheal a previous piece in the Spring 2020 issue
anesthesia (GETA).9-16 However, of Vertebral Columns that reviewed related
it is important to note that the regional anesthetic techniques for lumbar
absence of GETA does not always spine surgery.
equate to “awa ke” surger y—
Mohammed S. there is a continuum of seda- Awake Endoscopic Spine Fusion
Ahmed, MD tion and patient responsiveness. Endoscopic spine surgery is generally per-
Different anesthetic techniques formed using GETA or conscious sedation
and protocols uniquely impact (CS). CS coupled with local anesthetic allows
consciousness, responsiveness, the patient to remain awake and maintains
respiratory function, and neuro- protective reflexes. Endoscopic procedures
logical monitoring.15,17 Given the are uniquely suited for CS from a pain stand-
potential benefits over traditional point because they can be performed via
techniques, surgeon and patient sub-centimeter incisions with minimal soft
interest in awake spine surgery tissue disruption to generate intraoperative
Peter B. Derman, has increased in recent years, pain response. Awake patients can provide
MD, MBA
particularly in regard to lumbar immediate feedback if a neural structure
fusion surgery. is inadvertently contacted and can confirm
As with all elective spine sur- the relief of radicular symptoms.18 This is
gery, patient selection is critical to main- particularly useful for endoscopic trans-
taining patient safety and obtaining optimal foraminal procedures where the exiting
outcomes. Typically, awake spinal fusion is nerve root is often in close proximity to the
reserved for patients with one-and two-level working cannula. Additionally, traditional
Fall 2020 Vertebral Columns isass.orgANESTHESIA 19
intraoperative neuromonitoring is not nec- two-level (n=16) fusions. While they reported
essary when performing awake endoscopic significant patient improvement as well as
surgery in this fashion. favorable operative times, reported blood
Initial reports of awake endoscopic trans- loss, and length of stay, they also detailed
foraminal lumbar interbody fusion (TLIF) some of the challenges associated w ith
were published in 2016, where Wang and awake endoscopic TLIF surgery. In partic-
Grossma n 6 descr ibed t heir ex per ience ular, the authors reported that four cases
and 1-year outcomes for the first 10 con- required an intraoperative conversion to
secutive patients whom they treated. The GETA, albeit without complication. Reasons
authors utilized propofol and ketamine for conversion included emesis (n=2), epi-
to keep patients under light to moderate staxis, and extreme anxiety. Furthermore,
sedation and did not administer narcotics there were two cases of cage migration,
or spine-based regional anesthesia, but li- one case of osteomyelitis, and one case of
posomal bupivacaine was injected into the
percutaneous pedicle screw tracts. As such,
patients were able to provide live feedback
Awake patients can provide
to the surgeons throughout the procedure. immediate feedback if a neural
After preparing the disc space for fusion,
structure is inadvertently contacted
they inserted 2.1 mg of recombinant hu-
man bone morphogenetic protein-2 in the and can confirm the relief of
disc space followed by a 22-mm or 25-mm radicular symptoms.
expandable cage. All patients underwent
successful surgery without complication or
conversion to alternate techniques, and all endplate fracture. There were no reported
but one patient were discharged on postop- cases of pseudoarthrosis or hardware failure
erative day one (the longer length of stay for with an average radiographic follow-up of
that patient was a result of a lack of social 14.6 months. The authors also commented
support). At 1-year follow-up, patients had that their growing familiarity and improved
a significant improvement in dysfunction efficiency with the procedure eventually
from lower back pain, and there were no enabled multilevel cases to be performed.
reported cases of pseudoarthrosis. To avoid The authors concluded that in appropri-
respiratory compromise, the authors limited ately selected patients, awake endoscopic
these procedures to 120 minutes. TLIF is a safe and efficacious procedure
In an expansion of their 2016 report, Kol- for lumbar fusion without the morbidity
cun et al8 reported 1-year clinical outcomes of open surgery. Since this publication, the
for awake TLIFs performed on the first 100 authors continued to refine their surgical
patients who underwent awake endoscopic and anesthetic techniques,7,19 and increased
TLIFs, including both one-level (n=84) and efficiency now allows for the performance
isass.org Vertebral Columns Fall 202020 ANESTHESIA
of three-level fusions. In an effort to avoid airway in the prone position, and the poten-
intraoperative emesis and prevent epistaxis, tial impact on postoperative neurological
the addition of preoperative glycopyrrolate function. Contraindications to SBRA include
and ondansetron as well as oxymetazoline bleeding disorders and/or severe stenosis
spray were implemented, respectively. precluding proper anesthetic permeation.
Further investigation is needed to assess Chan et al20 described an awake minimally
the ability to maintain or restore sagittal pa- invasive TLIF technique in two patients
rameters with endoscopic fusion techniques, using tubular retractors, navigation, spinal
regardless of whether or not the patient is anesthesia, liposomal bupivacaine, and
awake. While concerns do presently exist, no intraoperative neuromonitoring. The
we are optimistic that techniques and de- authors highlighted their ability to perform
vice technology will continue to improve a direct decompression, unlike previously
with time. described endoscopic techniques, and
reported no intraoperative complications.
Minimally invasive spine surgery They concluded that their novel approach
was feasible for select patients; however,
is more suitable for local and larger cohorts and/or control cohorts are
regional anesthetic techniques than needed to better evaluate their techniques.
traditional open spine surgery. Sekera k et a l 2 completed a compa ra-
tive outcome analysis of SBRA for awake
minimally invasive TLIFs. The aut hors
Awake Minimally Invasive Spine Fusion retrospectively reviewed outcomes of 111
Minimally invasive spine surgery is more patients and compared outcomes of GETA
suitable for local and regional anesthetic to SBR A w it h a nd w it hout TLIP block.
techniques than traditional open spine Patients who underwent SBR A (+/- TLIP
surgery. Spine-based regional anesthesia block) had significantly reduced postop-
(SBRA) and ultrasound-guided fascial plane erative pain scores, required fewer opioids
blocks may be utilized in perioperative pro- in the postanesthesia care unit, and had
tocols for awake minimally invasive spine reduced time in the postanesthesia care
surgery. 2,15,20 Garg et al15 recently published unit after surgery compared to patients who
their perioperative protocol for awake lum- received GETA. Furthermore, the addition
bar fusions and recommended multimodal of a TLIP significantly reduced length of
analgesia, titrated propofol sedation, and stay compared w it h GETA and trended
lumbar spinal and thoracolumbar interfas- toward significance when compared with
cial plane (TLIP) block utilizing liposomal SBRA alone. The authors concluded that
bupivacaine. Common concerns with SBRA SBRA alone and SBRA with TLIP block are
include its finite duration of effectiveness, viable and beneficial options to perform
difficultly of establishing an emergency awake TLIFs.
Fall 2020 Vertebral Columns isass.orgANESTHESIA 21
Conclusion ized centers that have devoted significant
Numerous techniques ex ist to perform time and resources to advancing the field
awake minimally invasive lumbar fusion of awake lumbar spine fusion. Therefore, it
surger y. Choosing the most appropriate remains to be seen whether these techniques
method to safely deliver care to patients and outcomes are generalizable to other
depends on the comfort and experience of practice environments. Finally, additional
both the surgeon and anesthesiologist. The high-quality studies are needed to assess
data available on this topic are currently short- and long-term outcomes of awake
limited and come from a handful of special- lumbar fusion surgery. n
References
1. Huang M, Brusko GD, Borowsky PA, et al. 8. Kolcun JPG, Brusko GD, Basil GW, Epstein 15. Garg B, Ahuja K, Sharan AD. Awake
The University of Miami spine surgery R, Wang MY. Endoscopic transforaminal spinal fusion. J Clin Orthop Trau-
ERAS protocol: a review of our journey. lumbar interbody fusion without gen- ma. 2020;11(5):749-752.
J Spine Surg. 2020;6(suppl 1):S29-S34. eral anesthesia: operative and clinical
16. Jellish WS, Thalji Z, Stevenson K, Shea
outcomes in 100 consecutive patients
2. Sekerak RJ, Sharan AD, Morris M, et J. A prospective randomized study
with a minimum 1-year follow-up.
al. Awake spinal fusion: compara- comparing short- and intermediate-term
Neurosurg Focus. 2019;46(4):E14.
tive outcome analysis of spinal an- perioperative outcome variables after
esthesia in lumbar fusion [abstract 9. Morris MT, Morris J, Wallace C, et al. An spinal or general anesthesia for lum-
P141]. Spine J. 2019;19:S223. analysis of the cost-effectiveness of spinal bar disk and laminectomy surgery.
versus general anesthesia for lumbar Anesth Analg. 1996;83(3):559-564.
3. Chin KJ, Adhikary SD, Forero M. Erector
spine surgery in various hospital settings.
spinae plane (ESP) block: a new paradigm 17. Riphaus A, Wehrmann T. Sedierung in der
Global Spine J. 2019;9(4):368-374.
in regional anesthesia and analgesia. Curr Endoskopie: Vorbereitung, Medikamente-
Anesthesiol Reports. 2019;9:271-280. 10. Zorrilla-Vaca A, Healy RJ, Mirski MA. A napplikation und Überwachung. Gastroen-
comparison of regional versus general terologie up2date. 2009;5(04):303-319.
4. Hand WR, Taylor JM, Harvey NR, et al.
anesthesia for lumbar spine surgery: a me-
Thoracolumbar interfascial plane (TLIP) 18. Telfeian AE. An awake, minimally-invasive,
ta-analysis of randomized studies. J Neu-
block: a pilot study in volunteers. Can fully-endoscopic surgical technique for
rosurg Anesthesiol. 2017;29(4):415-425.
J Anesth. 2015;62(11):1196-1200. treating lumbar radiculopathy secondary
11. McLain RF, Tetzlaff JE, Bell GR, Lewand- to heterotopic foraminal bone formation
5. Telfeian AE, Moldovan K, Shaaya E, et al.
rowski KU, Yoon HJ, Rana M. Microdis- after a minimally invasive transforaminal
Awake, endoscopic revision surgery for
cectomy: spinal anesthesia offers optimal lumbar interbody fusion with BMP: techni-
lumbar pseudarthrosis after transforam-
results in general patient population. cal note. J Spine Surg. 2018;4(1):162-166.
inal lumbar interbody tusion: technical
J Surg Orthop Adv. 2007;16(1):5-11.
notes. World Neurosurg. 2020;136:117-121. 19. Kolcun JPG, Brusko GD, Wang MY. En-
12. McLain RF, Bell GR, Kalfas I, Tetzlaff JE, doscopic transforaminal lumbar inter-
6. Wang MY, Grossman J. Endoscopic min-
Yoon HJ. Complications associated with body fusion without general anesthesia:
imally invasive transforaminal interbody
lumbar laminectomy: a comparison of technical innovations and outcomes.
fusion without general anesthesia: initial
spinal versus general anesthesia. Spine Ann Transl Med. 2019;7(suppl 5):S167.
clinical experience with 1-year follow-up.
(Phila Pa 1976). 2004;29(22):2542-2547.
Neurosurg Focus. 2016;40(2):E13. 20. Chan AK-H, Choy W, Miller CA, Robinson
13. McLain RF, Kalfas I, Bell GR, et al. Com- LC, Mummaneni PV. A novel technique
7. Butler AJ, Brusko GD, Wang MY.
parison of spinal and general anesthe- for awake, minimally invasive transforam-
Awake endoscopic transforaminal
sia in lumbar laminectomy surgery: a inal lumbar interbody fusion: technical
lumbar interbody fusion: a technical
case-controlled analysis of 400 patients. note. Neurosurg Focus. 2019;46(4):E16.
note. HSS J. 2020;16(2):200-204.
J Neurosurg Spine. 2005;2(1):17-22.
14. Attari MA, Mirhosseini SA, Honarmand
A, Safavi MR. Spinal anesthesia versus
general anesthesia for elective lumbar
spine surgery: a randomized clinical trial.
J Res Med Sci. 2011;16(4):524-529.
isass.org Vertebral Columns Fall 2020You can also read