Vestibular Physical Therapy Treatment of Individuals Exposed to Directed Energy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MILITARY MEDICINE, 00, 0/0:1, 2021
Vestibular Physical Therapy Treatment of Individuals Exposed
to Directed Energy
LTC Carrie W. Hoppes, SP, USA*; Karen H. Lambert, DPT†; Brooke N. Klatt, DPT, PhD‡;
Orlando D. Harvard, DPT‡; Susan L. Whitney, DPT, PhD‡
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
ABSTRACT
Introduction:
Following suspected sonic attacks on U.S. Embassies, a subset of individuals presented with a unique cluster of symptoms
believed to have resulted from exposure to directed energy. Directed energy has been described as exposure to a unique
sound/pressure phenomenon such as infrasonic or ultrasonic acoustic or electromagnetic energy. The Joint Force does not
have an established protocol to guide vestibular physical therapy for individuals exposed to directed energy. Therefore,
we have provided evidence-based guidance for the treatment of oculomotor- and vestibular-related impairments from
similar populations.
Materials and Methods:
Published evidence was used to inform suggestions for clinical best practice. We offer resources for the management of
non-oculomotor- and non-vestibular-related impairments, before discussing physical therapy interventions for dizziness
and imbalance.
Results:
The physical therapist should design a treatment program that addresses the individual’s health condition(s), body
structure and function impairments, activity limitations, and participation restrictions after suspected directed energy
exposure. This treatment program may include static standing, compliant surface standing, weight shifting, modified
center of gravity, gait, and gaze stabilization or vestibular-ocular reflex training. Habituation may also be prescribed.
Interventions were selected that require little to no specialized equipment, as such equipment may not be available in all
settings (i.e., operational environments).
Conclusions:
Evidence-based guidance for prescribing a comprehensive vestibular physical therapy regimen for individuals exposed to
directed energy may aid in their rehabilitation and return to duty. This standardized approach can help physical therapists
to treat complaints that do not match any previously known medical conditions but resemble brain injury or vestibular
pathology.
INTRODUCTION electromagnetic energy.2 Twenty-five diplomatic personnel
In 2016 and 2017, U.S. government personnel in U.S. reported dizziness, unsteadiness, cognitive impairments, otal-
Embassies in Havana, Cuba, and Guangzhou, China, reported gia, tinnitus, and hearing loss following the suspected sonic
exposure to a sound/pressure phenomenon. Following these attack in Cuba.1 These complaints did not match any previ-
suspected sonic attacks, a subset of individuals presented ously known medical conditions but resembled impairments
with a unique cluster of symptoms believed to have resulted typically associated with mild traumatic brain injury and/or
from exposure to directed energy. Directed energy has vestibular pathology. It is possible that the externally directed
been described as exposure to a unique sound/pressure forces may have caused injuries to the peripheral vestibu-
phenomenon1 such as infrasonic or ultrasonic acoustic or lar apparatus (semicircular canals and/or otoliths), vestibular
nerve, or central vestibular pathways. Such injuries could
* U.S. Army Medical Center of Excellence, Army-Baylor University explain their complaints of dizziness and imbalance and
Doctoral Program in Physical Therapy, Fort Sam Houston, TX 78234, USA would require vestibular physical therapy to facilitate reha-
† Hearing Center of Excellence, San Antonio, TX 78236, USA bilitation and return to duty.
‡ Department of Physical Therapy, University of Pittsburgh, Pittsburgh, Jauchem and Cook described three categories of poten-
PA 15219, USA tial effects of audible, acoustic energy: (1) aural effects
The views and information presented are those of the authors and do not (temporary or permanent effects on hearing), (2) extra-aural
represent the official position of the U.S. Army Medical Center of Excellence,
effects because of activation of the sympathetic nervous sys-
U.S. Army Training and Doctrine Command, Hearing Center of Excellence,
Department of the Army, Department of the Air Force, Defense Health tem (increased heart rate and blood pressure), and (3) non-
Agency, Department of Defense, or U.S. government. aural effects (pain, vertigo, nausea, and vomiting).3 The
doi:10.1093/milmed/usab202 auditory organs could be injured by focused sound with large-
Published by Oxford University Press on behalf of the Association of amplitude pressure waves via direct pressure transmission
Military Surgeons of the United States 2021. This work is written by (a) US
Government employee(s) and is in the public domain in the US.
into the cochlea.4 The possible effects of infrasonic and
MILITARY MEDICINE, Vol. 00, Month/Month 2021 1
PT Treatment Following Directed Energy Exposure
low-frequency acoustic energy were less clear.3 It has been without associated headache requires non-urgent referral
hypothesized that multiple sources of ultrasound (acoustic to optometry/ophthalmology.10 Uncontrolled headache with
frequencies higher than humans can perceive) can, through photophobia requires non-urgent referral to neurology/neuro-
non-linear interactions, form a focal composite wave pro- ophthalmology.10
ducing audible sensations and inducing biologic disruption.5 Sleep disturbance was reported by 86% (18 out of 21)
Others have proposed that the symptoms reported in Cuba of individuals exposed to directed energy with 71% (15 out
could be because of mild brain injury, a functional disorder, of 21) requiring medication.9 Individuals who report sleep
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
or even mass hysteria or mass psychogenic illness.6 disturbance can be managed according to the Management
Hoppes et al. proposed a physical therapy evaluation pro- of Sleep Disturbances Following Concussion/mTBI: Guid-
tocol for individuals exposed to directed energy.7 However, ance for Primary Care Management in Deployed and Non-
there is no established protocol to guide vestibular physi- Deployed Settings DoD Clinical Recommendation (available
cal therapy interventions for individuals exposed to directed at https://health.mil/Reference-Center/Publications/2020/07/
energy. The primary purpose of this manuscript is to pro- 31/Management-of-Sleep-Disturbances-Following-Concussi
vide evidence-based guidance for the treatment of persons onmTBI-Clinical-Recommendation).
exposed to directed energy who present with oculomotor- Specific interventions for anxiety following directed
and vestibular-related impairments. Individuals exposed to energy exposure have not been published. However, individ-
directed energy have also reported cognitive deficits, otalgia, uals with anxiety following directed energy exposure may be
tinnitus, hearing loss, epistaxis, headache, photophobia, sleep managed similar to those with an anxiety/mood clinical profile
disturbance, anxiety, and neuroendocrine dysfunction (NED). following sport-related concussion. Management may include
We offer resources for the management of non-oculomotor- psychoeducation, behavioral regulation, addressing sleep dis-
and non-vestibular-related impairments, before discussing turbances, physical activity, desensitization to environmental
physical therapy interventions for dizziness and imbalance in stimuli, and/or psychotherapy.11
greater detail. Interventions were selected that require little Symptoms of NED may include fatigue, insomnia, cog-
to no specialized equipment, as such equipment may not be nitive impairments (to include difficulty concentrating), and
available in all settings (i.e., operational environments). emotional and mood disturbances.12 Individuals with NED
can be managed according to the Indications and Conditions
for Neuroendocrine Dysfunction Screening Post Mild Trau-
Management of Non-Oculomotor- and matic Brain Injury DoD Clinical Recommendation (available
Non-Vestibular-Related Impairments at https://health.mil/Reference-Center/Publications/2020/07/
Individuals exposed to directed energy who report cogni- 31/Indications-and-Conditions-for-Neuroendocrine-Dysfunc
tive impairments can be managed according to the Cognitive tion-Screening-Post-Mild-TBI). Similar to individuals with
Rehabilitation for Service Members and Veterans Following post-concussion syndrome who present with ongoing cen-
Mild to Moderate Traumatic Brain Injury DoD Clinical Rec- tral and systemic physiologic regulatory dysfunction after
ommendation (available at https://health.mil/Reference-Cen traumatic brain injury,13 we believe that individuals exposed
ter/Publications/2020/07/30/Cognitive-Rehabilitation-for-Fo to directed energy with NED benefit from an individually
llowing-Mild-to-Moderate-TBI-Clinical-Recommendation-F prescribed, symptom-guided aerobic exercise program.
ull). Those with otalgia, tinnitus, and hearing loss may benefit
from referral to an otolaryngologist and/or audiologist. Beck
Treatment of Oculomotor Impairments
et al. offer a treatment algorithm for epistaxis.8
Headache was reported by 76% (16 out of 21) of indi- Smooth Pursuit
viduals exposed to directed energy with 57% (12 out of 21) Swanson et al.9 reported that 91% (10 out of 11) of indi-
requiring medication for management of their headache.9 viduals exposed to directed energy had pursuit impairments.
Individuals who report headache can be managed according Abnormalities in smooth pursuit eye movements are usually
to the Management of Headache Following Concussion/Mild associated with central vestibular or cerebellar disorders.14
Traumatic Brain Injury: Guidance for Primary Care Manage- To address this impairment, the individual is asked to fol-
ment in Deployed and Non-Deployed Settings DoD Clinical low a slowly moving target (fingertip or pen tip) horizontally,
Recommendation (available at https://health.mil/Reference- vertically, diagonally, or circularly. The individual should
Center/Publications/2020/07/31/Management-of-Headache- be instructed to, “follow the target as accurately as possible
Following-ConcussionmTBI-Clinical-Recommendation). with your eyes.” We found no evidence describing smooth
Photophobia was reported by 82% (9 out of 11) pursuit exercise prescription for this or similar populations.
of individuals exposed to directed energy.9 Depending Therefore, based on expert opinion, the authors recommend
on comorbid symptoms, complaints of photophobia may prescribing 5-10 repetitions of smooth pursuit three times
require referral. As an acute ocular symptom, severe pho- daily for a total of 10-12 minutes per day. So as not to exceed
tophobia is considered a serious concern and warrants the limits of the smooth pursuit system, the target speed must
urgent referral to ophthalmology/optometry.10 Photophobia be below 100◦ /second.15 The physical therapist can use the
2 MILITARY MEDICINE, Vol. 00, Month/Month 2021
PT Treatment Following Directed Energy Exposure
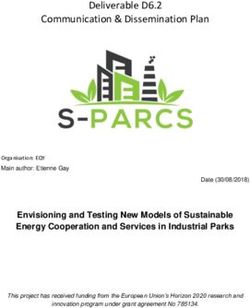
testing parameters described in the Vestibular/Ocular Motor impairment. The VORx1 viewing exercise is prescribed for
Screening, moving the target at a rate requiring ∼2 seconds to the treatment of gaze instability. In this exercise, the indi-
go fully from left to right (a distance of 0.91 m (3 feet)) when vidual fixates on a stationary target, while they slowly move
seated 0.91 m from the individual.16 Smooth pursuit training their head left and right (Fig. 2).18 The speed of head move-
can be varied by changing the target speed, distance from the ment should be just below the point at which the patient
target, and the complexity of the background. reports that the target begins to move or blur. We found no
published literature describing use of VORx1 viewing in this
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
Saccades population; however, it is commonly used for treating VOR
Swanson et al.9 reported that 82% (9 out of 11) of indi- impairments. For the treatment of acute unilateral peripheral
viduals exposed to directed energy had abnormal saccades. vestibular hypofunction, Hall et al. recommended perform-
Abnormalities in saccadic eye movements are usually associ- ing VORx1 viewing three times daily for a total of 12 minutes
ated with central vestibular or cerebellar disorders.14 To treat per day.19 For the treatment of chronic unilateral peripheral
impaired saccades, an individual is asked to rapidly shift gaze vestibular hypofunction, Hall et al. recommended increasing
between two targets (horizontally and/or vertically). The indi- the frequency to three-five times daily for a total of 20 minutes
vidual should be instructed to, “shift your gaze quickly and per day.19 This intervention is typically first performed in the
accurately between these two targets.” We found no evidence horizontal plane against a plain background. The physical
describing saccadic exercise prescription for this population, therapist may also prescribe this exercise in the vertical plane.
however, Clark et al. describe training using saccadic eye The VORx1 exercise can be varied by changing the speed of
charts for individuals with sport-related concussion.17 Clark head movement, the complexity of the background, and the
et al. recommended performing 20 minutes of saccadic train- distance to the target.20,21
ing two times per week in an athletic population.17 Further
research is needed to determine exercise prescription for indi- Subjective Visual Vertical
viduals exposed to directed energy. Saccade training can be Two studies1,9 have reported abnormal vestibular-evoked
varied by changing the speed, distance from the charts/targets, myogenic potentials in a group of individuals exposed to
and the complexity of the background. directed energy. Vestibular-evoked myogenic potential testing
assesses the function of the otoliths, and there is no estab-
Vergence lished treatment for normalizing otolith functioning. Utricular
Swanson et al.9 reported that 67% (10 out of 15) of individuals impairments can result in impaired subjective visual vertical
exposed to directed energy had a near point of convergence (SVV). Hoffer et al.1 reported that 22 of 25 individuals (88%;
greater than 6 cm. To treat convergence, the individual is prevalence 99% CI 65%-98%) exposed to directed energy had
asked to follow a target slowly moving toward their nose in an abnormal SVV. There is no established treatment for nor-
the sagittal plane. There are multiple variations of this exer- malizing SVV. Chetana and Jayesh reported on performance
cise. During pencil push-ups, the patient focuses on a pencil on the bucket test (a low-cost method for SVV assessment)
eraser as it is slowly moved toward the nose. Brock’s string in 100 individuals with vestibular disorders.22 Although SVV
(a string with multiple, colored beads spaced along its length) normalized in most individuals with vestibular neuritis and
can also be used; with the string held to the tip of their nose, benign paroxysmal positional vertigo within 1 month,22 it is
the individual is asked to focus on one of the colored beads and not known if normalization was because of vestibular reha-
then to fixate on a different colored bead (shifting their gaze bilitation, repositioning maneuvers, or spontaneous recovery.
nearer or further) (Fig. 1). Because of the binocular visual If SVV is impaired, working on aligning to the earth’s grav-
system, the individual perceives an “X” made by the string, ity with the use of a mirror (a tape/plumb line indicating true
crossing at the colored bead they have fixated on. To advance vertical can be placed on the mirror for visual feedback) with
this exercise, over time the beads can be moved closer to the head/body tilts might be helpful to re-establish the perception
nose to further challenge the convergence system. We found of true vertical. The patient is asked to, “close your eyes and
no published literature describing dosing parameters for use lean to one side, then, come back to the position where you
of Brock’s string in this population; however, Clark et al. feel like you are straight up and open your eyes to check your
describe Brock’s string training for individuals with sport- position in the mirror.”
related concussion.17 Convergence training can be varied by
changing the speed, distance between the beads, the angle of Visual Motion Sensitivity
the string, and the complexity of the background.
A clinical practice guideline on vestibular rehabilitation for
peripheral vestibular hypofunction recommends habituation
Treatment of Vestibular Impairments
exercises as a treatment when busy visual environments exac-
Vestibular-Ocular Reflex erbate dizziness.19 Although common in individuals with
Swanson et al.9 reported that 71% (15 out of 17) of individuals vestibular disorders, the prevalence of visual motion sensitiv-
exposed to directed energy had vestibular-ocular reflex (VOR) ity in individuals exposed to directed energy is not known.
MILITARY MEDICINE, Vol. 00, Month/Month 2021 3PT Treatment Following Directed Energy Exposure
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
FIGURE 1. Use of Brock’s string (a string with multiple, colored beads spaced along its length). With the string held to the tip of their nose, the individual is
asked to focus on one of the colored beads and then to fixate on a different colored bead (shifting their gaze nearer or further).
FIGURE 2. VORx1 viewing exercise for gaze instability. The individual fixates on a stationary target (“X”), while they slowly move their head right and left.
A simple means to habituate visual motion sensitivity is to to fixate on their thumb as they rotate their head and trunk en
ask the patient to face a visually complex area (e.g., physical bloc 80◦ to the right and left (Fig. 3). The individual perceives
therapy gym). With their arm outstretched, the patient is asked blurring of the visual world. The use of optokinetic stimuli and
4 MILITARY MEDICINE, Vol. 00, Month/Month 2021PT Treatment Following Directed Energy Exposure
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
FIGURE 3. Habituation exercise for visual motion sensitivity. While facing a visually complex area and with their arm outstretched, the patient is asked to
fixate on their thumb as they rotate their head and trunk en bloc 80◦ to the right and left.
virtual reality environments has been shown to decrease visual dwelling adults is a mean score of 11.88 (5.40).28 Scores
vertigo symptoms when incorporated into a rehabilitation reg- on the Functional Gait Assessment ranged from 18 to 30
imen.23,24 Exposure to optokinetic stimuli has been used in the (lower scores indicate greater impairment) with a mean of
treatment of service members with traumatic brain injury.25 26 in 17 individuals exposed to directed energy.9 Scores on
Following sport-related concussion, a combination of vestibu- the Sensory Organization Test ranged from 20 to 78 (lower
lar, oculomotor, and optokinetic treatment was effective in scores indicate greater impairment) with a mean of 55 in 15
decreasing symptoms and postural instability in a professional individuals exposed to directed energy.9
ice hockey player.26 Although optokinetic stimuli are often Klatt et al. have proposed six different exercise categories
utilized by clinicians, evidence-based stimulus parameters for when developing a balance program aimed at improving
delivery of optokinetic stimuli are not yet known. There is postural control: static standing, compliant surface stand-
preliminary evidence supporting the use of a fixation target ing, weight shifting, modified center of gravity, gait, and
during habituation exercises.27 The authors recommend this gaze stabilization or VOR training.18 The authors believe this
treatment approach for patients with visual motion sensitiv- approach can be used in the population exposed to directed
ity after directed energy exposure. The training can be varied energy. Progression of exercises includes five stance posi-
by changing the complexity, contrast, speed, and direction of tions (in order of increasing difficulty as the base of support
moving visual stimuli. becomes narrower: feet apart, feet together, semi-tandem
Romberg, tandem Romberg, and single-leg stance) and four
surface types (in order of increasing difficulty: firm, firm with
Static and Dynamic Balance incline, firm with decline, and foam).18 The patient can be
Swanson et al.9 described static and dynamic balance deficits further challenged by closing their eyes in all exercise cate-
in individuals exposed to directed energy. Scores on the gories except VOR training (during which visual fixation is
Balance Error Scoring System ranged from 7 to 50 (higher required).18 Static to dynamic standing can be progressed by
scores indicate greater impairment) with a mean score of 29 including upper extremity movements with no weight, light
in 16 individuals exposed to directed energy.9 The sample weight, heavier weight, or by decreasing the speed at which
reported in Swanson et al. had a mean age of 43 years; nor- lifting movements are performed.18 Head movement can be
mative performance for 40-49 year old healthy, community- progressed by incorporating pitch plane and then yaw plane
MILITARY MEDICINE, Vol. 00, Month/Month 2021 5PT Treatment Following Directed Energy Exposure
head movement.18 Cognitive or manual dual-tasks can also triggering or exacerbating headache because of overworking
be used to progress the difficulty of a balance program during the oculomotor system.
both standing and gait. Based on the specific vestibular impairment, gaze stability
The environment can also affect the difficulty of a balance and/or habituation exercises may be prescribed. For individu-
exercise. Whether or not the environment is quiet or loud, als with impaired gaze stability, VORx1 viewing is indicated.
empty or crowded, high or low visual contrast, and predictable Although Hall et al. provided specific dosage recommen-
or unpredictable will all affect performance.29,30 Similarly, dations for the treatment of acute and chronic unilateral
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
the type of compliant surface (foam density, carpet type, out- peripheral vestibular hypofunction,19 dosage after directed
door surface type, and consistency of surface type); the type energy exposure has not been established. Interventions for
of lighting (fluorescent, iridescent, and natural) and amount otolith dysfunction or deficits in SVV are also not estab-
of light; the presence or absence of physical assistance (from lished. Dosage recommendations for the treatment of visual
the support of a physical therapist, family member, assistive motion sensitivity in individuals exposed to directed energy
device, or even a wall or other stable object/surface for sup- are not known. Although Klatt et al. have proposed a log-
port); and the tone/inflection of the tester’s instructions or ical sequence in progressing balance exercises for persons
commands will all affect performance.29 Light touch can be with vestibular disorders,18 exercise progression after directed
applied during balance training to reduce body sway.31 energy exposure is lacking. In the absence of evidence-based
Gait training can be progressed from self-selected pace to recommendations, treatment should focus on the individual’s
fast and finally to slow speed.32,33 Walking forward can be activity limitations and participation restrictions. During the
progressed to walking backward. Other gait variations can be physical therapy interventions suggested above, patient symp-
included to further challenge a patient such as changing gait toms should be monitored and exercise prescription modified
speeds within a given trial, incorporating quick stops/starts, based on the patient’s response.
stepping over objects of different sizes, sidestepping, braid-
ing, marching, completing 180◦ and 360◦ turns, walking CONCLUSIONS
on toes, and/or walking on heels.34 Cognitive and/or manual Evidence-based guidance for prescribing a comprehensive
dual-tasks can also be incorporated into gait training. vestibular physical therapy regimen for individuals exposed
to directed energy may aid in their rehabilitation and return to
DISCUSSION duty. As there was no established protocol to guide rehabil-
Although non-lethal, the reported effects of directed energy itation in this population, we provided evidence-based guid-
exposure on the U.S. government personnel negatively ance for the treatment of oculomotor- and vestibular-related
impacted their health and ability to effectively perform their impairments in similar populations (individuals with central
diplomatic mission. The Joint Force does not have an estab- and peripheral vestibular disorders). We also offered resources
lished protocol to guide vestibular physical therapy for indi- for the management of non-oculomotor- and non-vestibular-
viduals exposed to directed energy. The Joint Requirements related impairments. Further research is needed to advance
Oversight Council Memorandum 019-19 (issued on March the care of individuals exposed to directed energy whose
18, 2019) stated that the DoD is lacking knowledge and presentation does not match any previously known medical
understanding of such threat sources, the pathophysiological conditions but resembles brain injury or vestibular pathology.
response within the body leading to the clinical symptoms,
and the ability to identify, diagnose, treat, and clinically
ACKNOWLEDGMENTS
manage exposed personnel. This evidence-based guidance for
The authors wish to thank MAJ Jamie Morris and 1LT Stefanie Faull for their
vestibular physical therapy is a first step in addressing gaps in assistance with the figures.
treating and clinically managing exposed individuals. Basing
our vestibular physical therapy treatment recommendations
on the body structure and function impairments, activity lim- FUNDING
None declared.
itations, and participation restrictions reported by a small
cohort of individuals and published en masse is a limita-
tion of this work, and further research and case studies are CONFLICT OF INTEREST STATEMENT
needed. None declared.
Hoppes et al. proposed a physical therapy evaluation pro-
tocol for individuals exposed to directed energy.7 Following REFERENCES
the examination, treatment should address the individual’s 1. Hoffer ME, Levin BE, Snapp H, Buskirk J, Balaban C: Acute find-
body structure and function impairments, activity limitations, ings in an acquired neurosensory dysfunction. Laryngoscope Investig
Otolaryngol 2019; 4(1): 124–31.
and participation restrictions. Based on the specific oculomo-
2. Lubner RJ, Kondamuri NS, Knoll RM, et al: Review of audiovestibular
tor impairment, smooth pursuit, saccades, and/or vergence symptoms following exposure to acoustic and electromagnetic energy
exercises may be prescribed. When prescribing exercises outside conventional human hearing. Front Neurol 2020; 11(234):
for oculomotor impairment, care should be taken to avoid 1–12.
6 MILITARY MEDICINE, Vol. 00, Month/Month 2021PT Treatment Following Directed Energy Exposure
3. Jauchem JR, Cook MC: High-intensity acoustics for military non- 18. Klatt B, Carender W, Lin C, et al: A conceptual framework for the
lethal applications: a lack of useful systems. Mil Med 2007; 172(2): progression of balance exercises in persons with balance and vestibular
182–9. disorders. Phys Med Rehabil Int 2015; 2(4): 1–20.
4. Occupational Safety and Health Administration: Occupational 19. Hall C, Herdman S, Whitney S, et al: Vestibular rehabilitation
noise exposure 1910.95. Available at https://www.osha.gov/laws-regs/ for peripheral vestibular hypofunction: an evidence-based clinical
regulations/standardnumber/1910/1910.95; accessed May 5, 2021. practice guideline: from the American Physical Therapy Asso-
5. Mickelson AM: Medical Consequences of Radiological and Nuclear ciation Neurology Section. J Neurol Phys Ther 2016; 40(2):
Weapons. Office of the Surgeon General, Department of the Army, and 124–55.
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab202/6283513 by guest on 18 November 2021
Borden Institute; 2012. 20. Herdman SJ, Schubert MC, Das VE, Tusa RJ: Recovery of dynamic
6. Popkirov S, Baguley DM, Carson AJ, Brown RJ, Stone J: The neu- visual acuity in unilateral vestibular hypofunction. Arch Otolaryngol
rology of the Cuban “sonic attacks”. Lancet Neurol 2019; 18(9): Head Neck Surg 2003; 129(8): 819–24.
817–8. 21. Strupp M, Arbusow V, Maag KP, Gall C, Brandt T: Vestibular exercises
7. Hoppes CW, Lambert KH, Harvard OD, Whitney SL: Vestibular improve central vestibulospinal compensation after vestibular neuritis.
physical therapy evaluation of individuals exposed to directed energy. Neurology 1998; 51(3): 838–44.
Mil Med 2020; 1–8. https://academic.oup.com/milmed/advance- 22. Chetana N, Jayesh R: Subjective visual vertical in various vestibular
article/doi/10.1093/milmed/usaa562/6046745. disorders by using a simple bucket test. Indian J Otolaryngol Head
8. Beck R, Sorge M, Schneider A, Dietz A: Current approaches to epis- Neck Surg 2015; 67(2): 180–4.
taxis treatment in primary and secondary care. Dtsch Arztebl Int 2018; 23. Pavlou M, Bronstein A, Davies R: Randomized trial of supervised
115(1–2): 12–22. versus unsupervised optokinetic exercise in persons with periph-
9. Swanson RL, Hampton S, Green-McKenzie J, et al: Neurological eral vestibular disorders. Neurorehabil Neural Repair 2013; 27(3):
manifestations among US government personnel reporting directional 208–18.
audible and sensory phenomena in Havana, Cuba. JAMA 2018; 24. Pavlou M, Lingeswaran A, Davies RA, Gresty MA, Bronstein AM:
319(11): 1125–33. Simulator based rehabilitation in refractory dizziness. J Neurol 2004;
10. DoD Clinical Recommendation: Assessment and management of 251(8): 983–95.
visual dysfunction associated with mild traumatic brain injury. 2020. 25. Rábago CA, Wilken JM: Application of a mild traumatic brain injury
Available at https://health.mil/Reference-Center/Publications/2020/ rehabilitation program in a virtual realty environment: a case study. J
07/31/Assessment-and-Management-of-Visual-Dysfunction-Associa Neurol Phys Ther 2011; 35(4): 185–93.
ted-with-Mild-TBI-Clinical-Recommendation; accessed December 26. Mucci V, Meier C, Bizzini M, et al: Combined optokinetic treatment
23, 2020. and vestibular rehabilitation to reduce visually induced dizziness in a
11. Sandel N, Reynolds E, Cohen PE, Gillie BL, Kontos AP: Anxiety and professional ice hockey player after concussion: a clinical case. Front
mood clinical profile following sport-related concussion: from risk Neurol 2019; 10: 1–7.
factors to treatment. Sport Exerc Perform Psychol 2017; 6(3): 304–23. 27. Hoppes CW, Sparto PJ, Whitney SL, Furman JM, Huppert TJ: Func-
12. DoD clinical recommendation: indications and conditions for neuroen- tional near-infrared spectroscopy during optic flow with and without
docrine dysfunction screening post mild traumatic brain injury. 2021. fixation. PLoS One 2018; 13(3): 1–14.
Available at https://health.mil/Reference-Center/Publications/2020/ 28. Iverson GL, Kaarto ML, Koehle MS: Normative data for the balance
07/31/Indications-and-Conditions-for-Neuroendocrine-Dysfunction- error scoring system: implications for brain injury evaluations. Brain
Screening-Post-Mild-TBI; A accessed February 9, 2021. Inj 2008; 22(2): 147–52.
13. Leddy JJ, Kozlowski K, Fung M, Pendergast DR, Willer B: Regula- 29. Voss DE, Ionta MK, Myers BJ, Knott M: Proprioceptive Neuro-
tory and autoregulatory physiological dysfunction as a primary char- muscular Facilitation: Patterns and Techniques. Harper & Row;
acteristic of post concussion syndrome: implications for treatment. 1985.
NeuroRehabilitation 2007; 22(3): 199–205. 30. Umphred DA, Lazaro RT: Neurological Rehabilitation. Elsevier
14. Huh Y-E, Kim J-S: Bedside evaluation of dizzy patients. J Clin Neurol Health Sciences; 2012.
2013; 9(4): 203–13. 31. Saini A, Burns D, Emmett D, Song YS: Trunk velocity-dependent
15. Meyer CH, Lasker AG, Robinson DA: The upper limit of human Light Touch reduces postural sway during standing. PLoS One 2019;
smooth pursuit velocity. Vision Res 1985; 25(4): 561–3. 14(11): e0224943.
16. Mucha A, Collins MW, Elbin R, et al: A brief vestibular/ocular motor 32. Bruijn SM, van Dieën JH, Meijer OG, Beek PJ: Is slow walking more
screening (VOMS) assessment to evaluate concussions: preliminary stable? J Biomech 2009; 42(10): 1506–12.
findings. AJSM 2014; 42(10): 2479–86. 33. Fritz S, Lusardi M: White paper:“walking speed: the sixth vital sign”.
17. Clark JF, Colosimo A, Ellis JK, et al: Vision training methods for J Geriatr Phys Ther 2009; 32(2): 2–5.
sports concussion mitigation and management. J Vis Exp 2015; (99): 34. Earhart GM: Dynamic control of posture across locomotor tasks. Mov
1–11. Disord 2013; 28(11): 1501–8.
MILITARY MEDICINE, Vol. 00, Month/Month 2021 7You can also read