Video telephony in the (sub) acute care of ALS patients - Author: Date: Daniël Brummelman
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Video telephony in the (sub) acute
care of ALS patients
Author:
Daniël Brummelman
Date:
December 2007
Video telephony in the (sub)acute care for ALS patients
Video telephony in the (sub) acute
care of ALS patients
Author:
Daniël Brummelman
s0071609
Date:
December 2007
Report nr:
Bachelor thesis
BMT028
BSS 07-40
Committee:
Prof. H. Hermens
Dr. V. Jones
Dr. E. Janssen
Dr. D. Stemerding
2
Video telephony in the (sub)acute care for ALS patients
Acknowledgements
Working on this project has been a instructive experience on how to get from an idea to
starting a pilot. It also showed me that a lot of groups are involved in such a project. It is
wonderful that technology like this exists, but finding the right application is the key to
successful implementation.
I would like to thank all the participating groups for making this project possible: the
members of the committee, the ALS team at Het Roessingh Rehabilitation Centre, the
patients who participated, Rob Kleissen, Geert Schrijver, Vodafone, and anyone else who
helped with this project.
Daniël Brummelman
3
Video telephony in the (sub)acute care for ALS patients
Summary
Introduction
This report describes a study conducted with the team caring for ALS patients at Het
Roessingh Rehabilitation Centre in Enschede, in The Netherlands. ALS is a progressive
neurodegenerative disease for which there is no cure yet. The disease is very rare, it‟s
incidence is only 1,5 to 2 cases per 100.000 citizens. Therefore patients who have ALS live
far apart geographically. Since it‟s such a rare disease, very few care centers and physicians
have expertise in the treatment for this disease. ALS causes patients to have severe muscle
weakness and makes them very tired. This makes travelling a very taxing experience. Due to
the progressive nature and unfamiliarity of the disease (average life expectancy is 3,5 years
after the first symptoms) patients require intensive counseling and support. In the present
situation at Het Roessingh the ALS patients can call the physician‟s mobile phone number 24
hours a day 7 days a week. Many of these calls are not sufficient to deal with the problem and
are followed by a home-visit. Introducing a mobile telephone with the ability to see as well as
hear each other (video telephone) could improve the quality of the contact and thus help
reduce the number of unnecessary home visits.
Goals
The main goal of this research project is to investigate the use of innovative technology
(video telephony over UMTS) in supporting contact between ALS patients and the ALS
team. We investigate if this technology can help support, and improve the quality of, the
health-care process.
Methods
The experiment was designed in the form of a controlled trial with six experimental patients
using video phones and six control patients using regular mobile phones as in the current
practice. The six patients who had a videophone could use it freely for four weeks. Before
and after the four week trial period, questionnaires were given on the quality of life, status of
ALS and on the use of the video phone as a means of communication with their physician.
A second experiment was done which focused on the use of the video phones themselves and
testing indoor coverage at various places in Enschede. These findings were compared to the
Vodafone UMTS coverage map available on the Vodafone website.
Results
Because of unforeseen delays only the baseline questionnaires of four patients using video
phones were available for analysis. From these results it was concluded that three of the four
patients had a positive attitude towards using the video telephone as a means of
communication with their physician and were willing to try it. A fourth patient had a negative
attitude towards care via video telephony and decided to withdraw from the project shortly
after the preliminary questionnaire was applied.
The results of the experiment with UMTS phones and the UMTS network showed that the
UMTS signal strength tended to fluctuate a lot and indoor coverage was a problem. UMTS
signal strength would also vary according to the position in a building. This was especially
noticeable in the Roessingh building where some places, including the physician‟s office, had
no UMTS coverage. The experiment also gave practical experience in the use of the
telephones and calling with video phone.
Conclusion
Overall the technology looks very promising. The UMTS phones are easy to use and making
a video call is almost as easy as making a standard phone call. The patients are willing to try
this technology in their care process. One of the preconditions for introducing this kind of
service is that there is enough UMTS coverage to support use of the video function on the
4
Video telephony in the (sub)acute care for ALS patients
phones. Lack of (indoor) coverage is one of the main limitations encountered.
Recommendations are made for the follow up project by G. Schrijver who will carry out the
full experiment.
5
Video telephony in the (sub)acute care for ALS patients
Table of contents
Acknowledgements .................................................................................................................... 3
Summary .................................................................................................................................... 4
Table of contents ........................................................................................................................ 6
1. Introduction ........................................................................................................................ 7
1.1. Scope ........................................................................................................................... 7
1.2. What is ALS ................................................................................................................ 7
1.3. Problem Definition ...................................................................................................... 8
1.4. UMTS ........................................................................................................................ 10
1.5. Video Conferencing .................................................................................................. 12
1.6. Goals.......................................................................................................................... 13
1.7. Research question ...................................................................................................... 14
1.8. Course of the project ................................................................................................. 15
2. Materials and Methodology ............................................................................................. 17
2.1. Instrumentation.......................................................................................................... 17
2.2. The questionnaires..................................................................................................... 17
2.3. Comparison and coding schemes .............................................................................. 20
2.4. Methodology ............................................................................................................. 20
2.5. Enschede video telephony coverage test ................................................................... 22
3. Results .............................................................................................................................. 24
3.1. Experimental Group: Patient visits ........................................................................... 24
3.2. Preliminary results patient questionnaires................................................................. 25
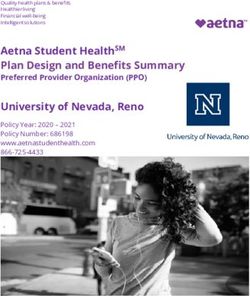
3.3. Results of the Enschede video telephony coverage test ............................................ 29
4. Discussion and Conclusion .............................................................................................. 38
4.1. General conclusion .................................................................................................... 38
4.2. Recommendations ..................................................................................................... 39
4.3. Overall Conclusion .................................................................................................... 39
Reference: ................................................................................................................................ 41
Appendix .................................................................................................................................. 42
Appendix A Introduction letters .......................................................................................... 42
Appendix B. Phone information sheet ................................................................................. 45
Appendix C Detailed specification of the phones............................................................... 47
Appendix D. Walkthroughs (protocol) ................................................................................ 49
Appendix E. Log sheet for use by healthcare professional to log patient contacts.............. 51
Appendix F. Questionnaires................................................................................................. 53
6
Video telephony in the (sub)acute care for ALS patients
1. Introduction
1.1. Scope
The University of Twente has been working with the Roessingh Rehabilitation centre on a
number of different projects concerning Telehealth applications. Two projects have already
been done with ALS patients. Both projects used a desktop based telehealth application.
Telehealth voor patiënten met ALS by E. Meijer in 2005.
Telecare voor patiënten met ALS by H. Zuidinga in 2006.
The project Telehealth by E. Meijer introduced internet consulting hours for patients to
consult with their physician and other healthcare workers. During these internet consulting
hours the patient and physician could see each other via a webcam. Telecare by H. Zuidinga
was a follow-up project for Telehealth. It used the same set-up as Telehealth but investigated
the substitution of the webcam with a high quality camera.
Now two new projects are being started on the use of remote care. This project: Video
Telephony in the (sub) acute care of ALS patients by D. Brummelman, and “The use of
video-telephony in the care process for ALS patients” by G. Schrijver. “Video Telephony in
the (sub) acute care of ALS patients” is a bachelors assignment and it will be the feasibility
study for the masters assignment by G. Schrijver. These two projects will use mobile phones
with video telephony capability and will investigate what the impact is on the care process for
ALS patients.
1.2. What is ALS
Amyotrophic lateral sclerosis (ALS) is in the United States often referred to as “Lou Gehrig‟s
disease” after a famous baseball player who died from the disease. ALS is a progressive
neurodegenerative disease that affects motor nerve cells in the brain and the spinal cord.
Motor neurons reach from the brain to the spinal cord and from the spinal cord to the muscles
throughout the body. When the motor neurons die, the ability of the brain to initiate and
control muscle movement is lost. ALS only affects voluntary muscle movement, like the
arms and legs, but also breathing. The heart and digestive system also have muscles but these
are regulated involuntarily. With voluntary muscle action progressively affected, patients in
the later stages of the disease may become totally paralyzed. Yet, through it all, for the vast
majority of people, their minds remain unaffected.
A-myo-trophic comes from the Greek language. “A” means no or negative. “Myo” refers to
muscle, and “Trophic” means nourishment, “No muscle nourishment.” When a muscle has no
nourishment, it “atrophies” or wastes away. “Lateral” identifies the areas in a person‟s spinal
cord where portions of the nerve cells that signal and control the muscles are located. As this
area degenerates it leads to scarring or hardening (“sclerosis”) in the region.
7
Video telephony in the (sub)acute care for ALS patients
Figure 1: schematic presentation of the effect of ALS
As motor neurons degenerate, they can no longer send impulses to the muscle fibers that
normally result in muscle movement. Early symptoms of ALS often include increasing
muscle weakness, especially involving the arms and legs, speech, swallowing or breathing.
When muscles no longer receive the messages from the motor neurons that they require to
function, the muscles begin to atrophy. Limbs begin to look “thinner” due to muscle wasting.
The progressive degeneration of the motor neurons in ALS eventually lead to death, often
due to failure of the respiratory system.
The average life expectancy of a patient with ALS is 3,5 years after the first symptoms
appear. The progression of ALS is quite variable; no two people will experience the same
evolution of the disease. There are medically documented cases of people in whom ALS
„burns out‟, stops progressing or progresses at a very slow rate. But there is no cure yet.
[1],[2]
Every year between 200 – 350 people in the Netherlands are diagnosed with ALS. The total
number of ALS patients in the Netherlands is estimated to be between the 1000 and 1500
cases. Every year around 300 to 400 people die because of the effects of ALS. The disease is
detected at various ages but in 90 % of cases symptoms appear between the ages of 40 – 60
years. [3]
The treatment of a patient with ALS is primarily a symptomatic treatment. Since the disease
is incurable, the treatment is not focused on curing the patient but on caring for the patient
and enhancing the quality of life for him and his surroundings. The treatment consists of
(psycho)social counseling and practical help, advice and regular contact with the patient. An
important component is the (sub) acute relief of problems caused by ALS. [4]
1.3. Problem Definition
The incidence of ALS is low (1,5-2 cases per 100.000 citizens), this causes patients to be
spread over a large geographical area. Due to the low incidence of ALS there are only a small
number of care centers that expertise in ALS treatment. This also means that there are few
physicians that have expertise in ALS treatment. So physicians that are experienced in ALS
have to cover a large area (by Dutch standards) with relatively few patients.
Another effect of ALS is that it weakens a patients muscles, this causes mobility problems,
respiratory difficulties and they are in general very tired. This makes travelling a very hard
8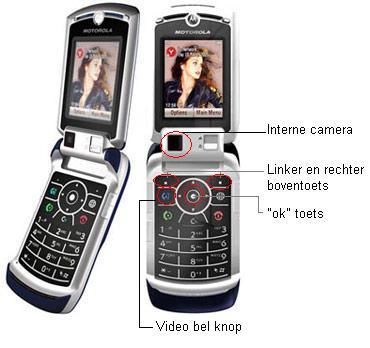
Video telephony in the (sub)acute care for ALS patients
and a taxing experience for the patient. So instead of the patient going to the hospital, the
physician often makes house calls. During the time that the physician has to spend travelling
to a patient, no other patients can be helped. This hinders accessibility of care for ALS
patients, care that the patients do need due to the progressive and distressing nature of ALS.
ALS patients face a lot of new problems in performing daily life activities. This unfamiliarity
creates the need to get information and reassurance from the physician. The cartoon in figure
2 illustrates this well.
Figure 2: “ALS” means “if” in Dutch. The patient asks: If I can’t …walk, swallow, talk, move or breathe?
If I’m a burden to everyone? [5]
Het Roessingh in Enschede in the Twente region of the Netherlands is a rehabilitation center
which has extensive experience in ALS treatment. They have one physician that is
responsible for ALS treatment and he covers the whole province of Overijssel and a piece of
Gelderland. ALS patients can call a telephone number 24 hours a day if they have questions.
Many times these telephone consultations result in a home visit by the physician. This is due
to the fact that problems cannot be properly assessed via speech only. There is a need for a
“richer” medium of communication other than conventional telephony. [4]
Figure 3: map of the Netherlands divided in provinces. The dot in south-east of Overijssel indicates the
city Enschede where het Roessingh is located.
9
Video telephony in the (sub)acute care for ALS patients
1.3.1. ALS telemedicine project
In previous studies with ALS patients conducted in by 2005 and 2006 by E. Meijer and H.
Huizenga, researchers investigated what the use of a PC-based telehealth application could
add to the care process. This telehealth application supported a video conferencing utility, a
chat room and an online library where patients could get information on ALS.
The system was found to work well, and one of the advantages identified was that
videoconferencing allowed the healthcare workers to see the patients in their own
surroundings from a distance. A drawback identified was the internet connection, which was
not fast enough to give a fluent video conferencing connection (sound and video were out of
synch). Another drawback was that healthcare workers had to leave their office and go to a
separate room to use the system and that the system was completely new and unfamiliar to
them. One of the outcomes was a recommendation to use a system which healthcare workers
can use from their own office and fits in their regular schedule. [6][7]
Current developments in mobile technologies mean that now mobile phones with video
conferencing capability could provide health care workers with a communication tool that fits
in their regular schedule and protocol and is usable from their own office (or in principle
from anywhere). In this current research project we conduct a feasibility study to see if there
is justification for a full-scale pilot.
1.4. UMTS
The Universal Mobile Telecommunication System (UMTS) is one of the so-called third
generation (3G) mobile communication systems. It is the successor of the Global Standard for
Mobiles (GSM) (2G) and GPRS/EDGE (2,5G) systems. Here follows a short history of
mobile telephony:
The history of mobile phones starts in 1920s with radio telephony. In 1947 the first mobile
phone network was set up on the highway between Boston and New York. Mobile phones
where generally car-bound. The radio spectrum eventually became too crowded because of
the limited space in the frequency spectrum (every phone had its own dedicated frequency).
Through the introduction of cellular structure in modern automatic telecommunication
systems this scarcity problem was reduced. [8]
It wasn‟t until the introduction of GSM in the 1990‟s that mobile telephony began to be
widely used by the public. This is also represented in the amount of mobile telephony
subscribers, table 1. This table is taken from a TNO study in 2006 [9]and shows that the
Netherlands (which now has 16,3 million inhabitants [10]) has 16,3 million mobile telephony
subscribers. This doesn‟t mean that everybody has a mobile telephone, since a lot of people
have a subscription for private use and a different one for professional use. But it does show
that the mobile telephone is increasingly becoming a common sight in everyday life.
Together with the increase in subscribers, the capabilities and usability of mobile phones
continue to grow, with phones incorporating other functions such as cameras and personal
organizers. [8]
10Video telephony in the (sub)acute care for ALS patients
Table 1: Development of mobile telephone subscriptions in the Netherlands, 1995 – Q1 2006 (TNO study)
The UMTS service in the Netherlands was first introduced by Vodafone in February 2004
(followed by KPN and other telephone operators). Vodafone is aiming to have nationwide
UMTS coverage in the Netherlands by the end of 2007. The UMTS network architecture is
based on the established GSM network architecture and most UMTS phones are backwards
compatible with GSM network. However, unlike GPRS (which uses the GSM network
infrastructure), the rollout of UMTS services depended on installation of a whole new
network infrastructure (antennas and cabling) and therefore represents a huge financial
investment in infrastructure and also operating licenses. The GSM network in the
Netherlands uses 900 MHz or 1800 MHz frequency bands. In the US and Canada GSM uses
the 850 MHz and 1900 MHz bands because the other frequency bands are already allocated.
The UMTS network works on different frequency bands than the GSM. UMTS uses the
1885-2025MHz for uplink and 2110-2200 MHz for downlink. In the US and Canada, the
1700 MHZ frequency band is used for uplink because the 1900 MHz band is already used by
GSM.
UMTS provides a lot more spectrum to users than GSM. It also has a separate frequency
band for uplink and downlink. But that is not the only difference. UMTS also distributes its
frequency space differently. Through these differences UMTS can offer much higher
bandwidth. There are generally three different ways to distribute the frequency space
available:
Time Division Multiple Access (TDMA)
o Assigns each call a certain portion of time on a designated frequency.
Frequency Division Multiple Access (FDMA)
o Puts each call on a separate frequency
Code Division Multiple Access (CDMA)
o Gives a unique code to each call and spreads it over the available frequencies.
GSM uses a combination of TDMA and FDMA and UMTS uses a form of CDMA called
Wideband Code Division Multiple Access (W-CDMA) to distribute its frequency space.
Although W-CDMA offers a higher bandwidth it also brings limitations. Unlike the
TDMA/FDMA system of GSM, W-CDMA doesn‟t have a uniquely determined range or
11Video telephony in the (sub)acute care for ALS patients
capacity. This is due to the high degree of non-linearity, packet technology and mixed data
rates. In W-CDMA coverage, capacity and quality are all interdependent. This means that for
example coverage range decreases as more users use the system (capacity). In GSM systems
coverage depends on the base station and mobile station transmitted power, gains and losses.
The capacity, to certain extent, is a function of the hardware resources. The main difference
in predicting W-CDMA and TDMA/FDMA coverage is that interference estimation is now
critical since users use the same frequency bands and time slots. This interference influences
the coverage, capacity and quality. In a study on the signal penetration of GSM 1800 and
UMTS it was found that GSM and UMTS have globally the same signal penetration. This
could be related to the fact that the frequency bands are close together (1800 and 2100 Mhz
respectively). GSM 900 has a slightly higher penetration value.[11],[12][23]
Table 2 shows a comparison of the 2G, 2.5G and the 3G systems and some of the
applications they can support. The increase in speed that the 3G systems offers, opens a lot of
opportunities for new forms of mobile communication and new applications.
2G Wireless 2.5G Wireless 3G Wireless
The technology of most The best technology now Combines a mobile phone,
current digital mobile phones widely available laptop PC and TV
Features includes: Features includes: Features includes:
- Phone calls - Phone calls/fax - Phone calls/fax
- Voice mail - Voice mail -- Send/receive large email
- Receive simple email -Send/receive large email messages
messages messages - High-speed Web
Speed: 10kb/sec - Web browsing Navigation/maps
Time to download a 3min - Navigation/maps - Videoconferencing
MP3 song: - New updates - TV streaming
31-41 min Speed: 64-144kb/sec Speed: 144kb/sec-2mb/sec
Time to download a 3min Time to download a 3min
MP3 song: MP3 song:
6-9min 11sec-1.5min
Table 2: comparison of 2G 2,5G and 3G wireless networks and their functionality [13]
1.5. Video Conferencing
1.5.1. The technology
Videoconferencing has been around for a while, in 1956 AT&T build the first “picturephone”
system. But up until the turn of the millennium videoconferencing systems were very
expensive. The development of the internet, instant messaging applications and webcams
means that now everyone could have a cheap videoconferencing system at home.
There are different videoconferencing solutions, the most common are listed below.
Rollabout Systems
These are self-contained, mobile units comprising a monitor or television screen atop a
console containing the associated hardware. The console is fitted with wheels or castors, so
that it can be moved between sites, and has sockets for local electrical connections. Rollabout
units, or group systems as they are sometimes known, produce high-quality sound and video
and they are widely used in business.
12Video telephony in the (sub)acute care for ALS patients
Set-top Systems
As the name suggests, these units are also portable but miniaturization puts all of the circuitry
into a single box that sits on top of a conventional television set to give a system of moderate
quality.
Desktop Systems
In these examples, the system box has been dispensed with and the circuitry has been located
on a standard PC card for insertion into a desktop computer. In desktop videoconferencing,
quality is sacrificed for convenience although utility is still high and cost is low. [14]
Wireless mobile phone systems
Wireless mobile phone systems (Video telephones) are the next step in videoconferencing.
This solution offers all the requirements in one small package.
1.5.2. Added value of video
The face is the primary site for communication of emotional states, it reflects interpersonal
attitudes; it provides nonverbal feedback on the comments of others; and some say it is the
primary source of information next to human speech. (Knapp,1978,p263)[15]
Humans communicate using several channels of communication simultaneously: speech,
facial expression, gesture and other kinds of body language. When people are talking on the
phone, they usually use gestures even though the person on the other side can‟t see them.
Non-verbal communication makes it easier for people to understand each other. One of the
most important sources of information about a person‟s emotional or physical state are facial
expressions. This is very helpful during a medical consultation. For the patient and the health
care professional, facial expressions are a powerful tool. Healthcare professionals can for
example reassure people or communicate the severity of a problem. Healthcare professionals
will also have more information to evaluate a consultation and so better respond to it. Patients
could now better explain their problems and get the feeling that they are better understood.
[15]
Eye contact is another important factor during medical interviews. The right level of eye
contact gives the patient the feeling he is understood and that the health care professional is
listening to him. It creates a social bond between health care professional and patient which
improves patient satisfaction. In a study on eye-contact using videoconferencing systems, a
large TV screen, a medium sized screen and a small telephone size screen were compared in
terms of the level of eye contact. One of the outcomes was that the small telephone size
screen had only a small reduction in eye contact moments in comparison to the large and
medium sized screens. It also stated that if patients get used to using a videophone it can be
just as good a tool for a medical interview as a larger desktop videoconferencing system. [16]
1.6. Goals
1.6.1. Goal of this project:
The main goal of this research project is to investigate the use of innovative technology
(video telephony over UMTS) in supporting contact between ALS patients and the ALS
team. We investigate if this technology can help support, and improve the quality of, the
health-care process.
In this Bachelor‟s assignment I focus on a feasibility study conducted as a pilot. The tasks
are:
Design of, and methodological and technical preparation for, the survey (to be
conducted by G. Schrijver as part of his Masters Assignment)
13Video telephony in the (sub)acute care for ALS patients
Conducting the pilot study
Technical investigation of the actual UMTS coverage in Enschede
Preliminary analysis of the results of the pilot
Evaluating the tools used
Videophones are not to replace home visits, more they should reduce the number of
unnecessary home visits because of better information on both the side of the healthcare
professional and the patient as compared with normal telephone contacts.
During this pilot experience will be gained with use of video telephones and of the current
UMTS service, and on the basis of the results of this pilot recommendations will be made as
inputs to the follow-up survey by G. Schrijver.
1.6.2. Expectations of the Roessingh
In the Telehealth study by E. Meijer. The Roessingh (rehabilitation center) formulated the
following hypotheses [6 p:11]:
Video telephony will lead to more efficient use of the physician‟s time so he can use
more time for direct patient contact.
Video telephony will lead to a reduction in overhead activities, especially travelling
time.
The approachable character of video telephony will lead to faster and efficient
medical services.
1.6.3. Possible added value
Video telephony can also be used for inter patient contact. It can be a tool for self help
groups, for example . Between healthcare professionals this could also be a helpful tool.
Patients‟ use of the phones in this way will also be investigated.
1.7. Research question
Does the substitution of ordinary telephones by video telephones improve efficiency and
quality of contacts between ALS patients and the care team?
1.7.1. Sub questions:
The questions shown in Table 3 below all relate to the comparison of regular mobile
telephony to video telephony. A control group will be using regular mobile phones and the
experiment group will use the mobile video telephones. Table 3 shows the questions, and the
instruments used to answer them. The questionnaires to be applied are discussed in detail in
the methodology section in chapter 2.
Following replacement of ordinary mobile Quantitative / Qualitative/
telephones by video telephones: Objective Subjective
Process
- Does the physician spend less time travelling? Log
- Does the frequency of the contacts change? Log
- How many calls result in a visit? Log
Content
- Does the length of the conversation change Log
- Are different topics discussed than right now? Log Telemedicine
satisfaction
questionnaire
14Video telephony in the (sub)acute care for ALS patients
Quality of Contact
- Are patients able to adequately explain their Telemedicine
problems? satisfaction
questionnaire
- Are more problems solved and are they solved Log Telemedicine
more adequately via videophone? satisfaction
questionnaire
- Does the patient find it easier to communicate Telemedicine
with the physician? satisfaction
questionnaire
- Does quality of life increase through the use of Short form 36
video telephony?
Use of technology
- How easy is use is the video phone? Time it takes Telemedicine
to use satisfaction
questionnaire
- How does the video/sound work (quality)? UMTS map/
experiment
- Does the patient have a positive or negative Telemedicine
experience using a videophone? satisfaction
questionnaire
- Does the physician have a positive or negative Telemedicine
experience using a videophone? satisfaction
questionnaire
- Does the current UMTS service provide adequate Telemedicine
performance to support video telephony? satisfaction
- Is the sound quality adequate for questionnaire
professionals?
- Is the video quality adequate for
professionals?
- Is the sound quality adequate for patients? Telemedicine
- Is the video quality adequate for patients? satisfaction
questionnaire
Table 3. Sub-questions and the data sources used to answer them
1.8. Course of the project
The course of this project changed over time. Adjustment of the planning was necessary for
reasons beyond our control. At first the project was to contain a trial over 4 weeks using the
videophones in a “real life” situation in hospital with patients and a doctor. However there
were some unforeseen problems and delays, first with the availability of the mobile phones
and UMTS subscriptions and later with the discovery of problems with indoor UTMS
coverage in the hospital building.
At the same time new insights were gained concerning the trial. The initial idea was to only
observe the patients before and at the end of the 4 week period of the trial (pre- and post-
design). But if the patients are observed in the 4 weeks prior to the trial and 4 weeks after the
trial (a so called A-B-A design) there will more significant data to compare the trial outcomes
with.
15Video telephony in the (sub)acute care for ALS patients
In this Bachelor project the new trial design cannot be fully implemented in the available
time due to the various time-delays experienced. Hence a different practical experiment was
proposed to evaluate the extent of the UMTS coverage problem in reality. This investigation
will support the follow up project. In this experiment the UMTS coverage in Enschede was
analyzed and practical recommendation on the use of a videophone are made. Also a pilot
was conducted by giving the preliminary questionnaires to the patients and analyzing the
results.
16Video telephony in the (sub)acute care for ALS patients
2. Materials and Methodology
2.1. Instrumentation
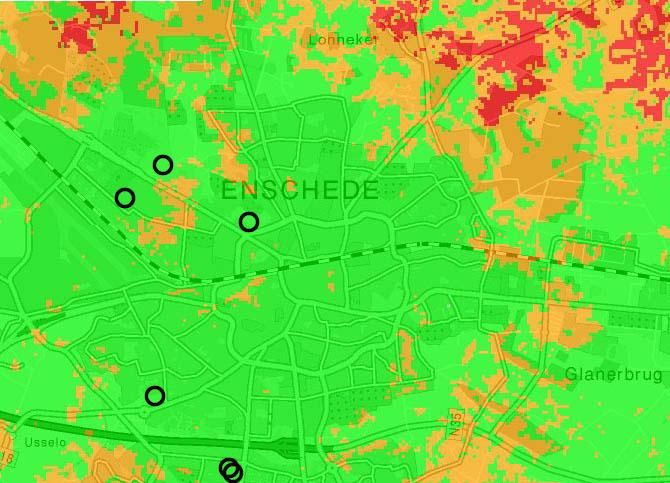
2.1.1. The mobile phones
Figure 4: the Sharp 903 and Motorola RAZR V3x
There are 2 types of phones at our disposal sponsored by Vodafone. The Sharp 903 and the
Motorola RAZR V3x. Both phones have similar specifications. They both run on a java based
operating system and have the ability to communicate via the UMTS network and are
backwards compatible with GSM/EDGE network.
The TFT screen resolution for both phones is 240 x 320 pixels with 0.262 million colors.
The phones feature 2 cameras, an internal one looking towards the user and an external one
looking towards the surroundings. The external camera of the Sharp 903 is 3.2 megapixels
and of the Motorola is 2.0 megapixels. During a video call you don‟t notice the difference in
quality. This is because bandwidth and not camera quality is the restraining factor. Both
internal cameras are VGA 0.3 mega pixel camera‟s which results in a output resolution of
640 x 320 pixels. The internal camera is used to see each other during a video call. During a
video call you can switch from the internal to the external camera to show things to the
person on the other side. For detailed specifications on the phones see appendix B
2.2. The questionnaires
To gather data on the impact of the addition of video on phone conversations different
questionnaires have been used. These questionnaires were selected on the basis that they are
validated instruments. Here follow the considerations for using them. The complete
questionnaires can be found in Appendix F.
17Video telephony in the (sub)acute care for ALS patients
The syntax of the questionnaire codes is: . So AU means:
A = ALSFRS-R questionnaire, applied to group U (UMTS patients = experimental group).
2.2.1. ALSFRS-R: revised ALS functional rating scale
In this project the goal with the ALSFRS-R questionnaire is to check in what stage of ALS
the patients are and how their condition progresses over time during the project. This will
also serve to check the uniformity of the patient group (are all patients generally in the same
stage of ALS?).
There are different questionnaires available to evaluate the progression of the ALS disease,
for example the “ALS Assessment Questionnaire” (ALSAQ) and the “ALS Functional Rating
Scale – Revised” (ALSFRS-R). Both questionnaires have been validated. The ALSAQ is a 40
item ALS specific questionnaire which assesses health related quality of life. The ALSFRS-R
is a 12 item scale which specifically covers the functional rating of a patient. The ALSFRS-R
was chosen because it just measures the disease progression. Health related quality of life
will be assessed with a different questionnaire. In this project a translated Dutch version was
used. It was translated by G. Schrijver and checked by the lead physician. [17],[18]
These will be designations used to indicate the ALSFRS-R questionnaire:
AG ALSFRS-R questionnaire for the GSM group
AU ALSFRS-R questionnaire for the UMTS group
2.2.2. Telemedicine Satisfaction and Usefulness Questionnaire
The Telemedicine Satisfaction and Usefulness Questionnaire (TSUQ) is a validated 26 item
questionnaire. It uses a five point Likert scale. It is designed to evaluate the perceptions of
satisfaction and usefulness as well as actual utilization of various telemedicine services. For
use in this project the questionnaire was translated in Dutch by G. Schrijver. The word
telemedicine was substituted by video telephony. Also a derived form of this questionnaire
was used to measure the expectations of patients for usage of the video phone. This derived
form was made by selecting all the questions that could be answered without using the
technology and asking what the expectations were. [19]
These will be designations used to indicate the TSUQ questionnaire derivatives:
BTU “Bruikbaarheid Telefonie UMTS groep”
Usability Questions GSM phone for the UMTS group
VVU “Verwachtings Vragen UMTS groep”
Expectation Questions UMTS phone for the UMTS group
BTG “Bruikbaarheid Telefonie GSM groep”
Usability Questions GSM phone for the GSM group
BTZ “Bruikbaarheid Telefonie Zorgverlener”
Usability Questions GSM phone for the healthcare professional
VVZ “Verwachtings Vragen Zorgeverlener”
Expectation Questions UMTS phone for the healthcare professional
2.2.3. Shortform 36
Shortform 36 (SF36) is a validated 36 item questionnaire. SF36 is used for different
purposes; it yields an 8 scale profile of functional health and well-being scores as well as
psychometrically-based physical and mental health summary measures and a preference-
based health utility index. It is a general measure, as opposed to one that targets a specific
age, disease, or treatment group. In this project SF36 will be used to evaluate a patients‟
quality of life. Quality of life is evaluated because it is the main goal of the treatment for ALS
18Video telephony in the (sub)acute care for ALS patients
patients, since the disease is incurable. So if this technology contributes to the quality of life
it would be a big incentive to continue the project. [20]
These will be designations used to indicate the SF36 questionnaire:
SFU Shortform 36 for the UMTS group
SFG Shortform 36 for the GSM group
19Video telephony in the (sub)acute care for ALS patients
2.3. Comparison and coding schemes
To compare and evaluate the questionnaires the comparison scheme shown below is used.
This is the original trial design as it was proposed in first instance. The design used a
combination of pre- and post- and controlled trial. The patients would be given questionnaires
before the experiment starts and when the experiment ended. This was done to check the
change over time during the project.
The syntax of the questionnaire codes is:
So AU1 means: A = ALSFRS-R questionnaire, applied to group U (UMTS patients =
experimental group) and the '1' indicates pre-.
Pre- and post-
Comparison of (common) Purpose
questions
By questionnaire and group
Pre- Post-
AU1 AU2 Detect change in ALS status over time
BTU1 BVU2 Compare usability of telephone with video telephone
Patients U VVU1 BVU2 Compare expectations of video telephone with actual
experience
SFU1 SFU2 Detect changes in health status/outcomes over time
Patients AG1 AG2 Detect change in ALS status over time
G BTG1 BTG2 Control for changes in usability responses over time
SFG1 SFG2 Detect changes in health status/outcomes over time
health care BTZ1 BVZ2 Compare usability of telephone with video telephone
professional VVZ1 BVZ2 Compare expectations of video telephone with actual
Z experience
Experimental/control Purpose: Compare experimental and control groups with
respect to:
AG1 AU1 ALS status at pre-
AG2 AU2 ALS status at post-
BTG1 BTU1 usability responses to conventional telephony at pre-
BTG2 BVU2 Comparison of conventional telephony with video telephony
2.4. Methodology
For the testing of medical procedures and medicines the Randomized Controlled Trial (RCT)
design is the gold standard. It is considered reliable because it decreases the chance of
coincidence through the use of a control group and randomization of the participants.
This project will be in the form of a controlled trial and not an RCT because the patient group
is not large enough and not all patients have good UMTS reception from their homes (one of
the prerequisites for use of video telephony). So the control group will be comprised out of
patients that don‟t have UMTS coverage in their home. Another reason for choosing a control
group was because of the small size of the experimental group. Having a control group gives
more data to compare the results with. The experiment group using the video phones will be
called UMTS group and the control group will be called GSM group.
20Video telephony in the (sub)acute care for ALS patients
2.4.1. Patient recruitment
The selection of the patients will be done by the physician. The selection will be based on the
following inclusion and exclusion criteria for UMTS group:
The patient must be in the last stage of ALS
In this stage patients have the most questions, so this means more contact moments to
survey.
UMTS coverage in the patients home
This is necessary to be able to make a video call with the physician.
Able to speak/write Dutch
No other serious diseases
Mentally able to answer questions
Able to use a telephone himself or another person in the vicinity
The GSM group selection is done on the same criteria except for UMTS coverage. After
patients are selected an introductory letter is sent (see Appendix A). In this letter it is
explained that the project is being conducted by the University of Twente in collaboration
with the physician at the Roessingh. The physician will phone in the next few days to ask for
an appointment. The patient is under no obligation to participate and may refuse the
appointment without giving any reason.
Each patient who agrees gets a phone and a number assigned to him/her. Thereafter they are
visited at home by the physician and the researchers and receives a verbal explanation and a
written information sheet (see Appendix B). There will be different versions of the
information sheet, one for the Motorola phone and one for the Sharp phone.
The patient also receives an informed consent letter. If the patient agrees to participate they
are asked to sign. If they want time to think they can keep the information and have a return
visit a few days later.
There are a total of 13 phones. These will be distributed among the physician, the researchers
and the patients. The initial plan was to involve 10 patients using UMTS phones and 10
persons in the control group. However due to the lack of UMTS coverage at some patients‟
homes, the number of patients in the UMTS group was reduced to 6.
2.4.2. The experiment
During the visit the patients are asked to fill in the group specific pre-questionnaires
mentioned in section 2.1.2. Also the videophone are given to patients belonging to the
experimental group. The researcher explains the functions on the UMTS phone, including,
how to make a video call and how to store a number. A detailed list of what the researcher
will do when visiting the patient can be found in the walkthrough in Appendix D.
4 weeks after the patients receive and begin to use the phones, the physician and the
researchers will visit the patients again and let them fill in the post-questionnaires mentioned
in section 2.1.2. During the 4 weeks pilot period the health care professionals log their
contacts with the patients. These logs together with the questionnaire data will be used to
evaluate the use of video telephony.
21Video telephony in the (sub)acute care for ALS patients
2.5. Enschede video telephony coverage test
During planning of the ALS study at Het Roessingh it was discovered that there are problems
with indoor UMTS coverage in certain locations in Enschede, including the Roessingh
rehabilitation center itself. Therefore an additional experiment was designed and
implemented. This experiment is designed to sample a number of indoor locations in
Enschede and record whether there is UMTS coverage there, and if so, record some
qualitative properties of the connection. One location will be the Roessingh rehabilitation
center. Other indoor locations around Enschede are selected to represent patients homes
(which can be anywhere) and would normally be the site from which patients would contact
ALS team members.
A series of tests will be performed to take „snapshots‟ of the actual UMTS coverage indoors.
The results of these snapshots will be compared to the theoretical coverage as stated on the
Vodafone website.
2.5.1. Test method
From a fixed position, being a room at the University of Twente, one person was called from
several locations in Enschede, via video telephony. A fixed point of
control was used to make sure that any differences in connection are
the result of differences in connection strength at the various test
sites in Enschede. From the various locations, a video telephony The 3G symbol on
connection was established, and video and audio quality observed. the Motorola phone
Also, asynchronies (time delays) between video and audio have
been investigated. If possible, experiments will be performed in indoor locations, such as
homes, malls, supermarkets, etc. By performing indoor experiments, we hope to replicate
situations in which the highest signal strengths are required. Also, by performing the
experiment indoors, we emulate the settings in which ALS-patients will contact their
physician, which are likely to be indoors. If UMTS is available, a 3G-logo should appear on
the telephones and establishing a video-call should be possible.
There will be three experiments per location. First, the person measuring at the test site will
call the person at the control point. Once the video telephony connection is established, the
connection will be kept for a minimal time of one minute. Second, the person at the control
point will call the person at the test site. This connection will also be kept for a minimum of
one minute.
To check for asynchronies between the video and audio signal, a clapperboard will be used at
the test site. This clapperboard will be closed five times, and before each clap the number of
the clap will be spoken (“one”…. “clap”….”two”….”clap”….etc) to prevent getting out of
sync. The average time delay between visual clap and the sound of the clap will be
considered as being the time delay between video and audio. The clapperboard experiment
will be recorded on the phone so that delays can be analyzed at a later stage. Sound and audio
quality as well will be judged by eye and will be rated on a numeric rating scale (NRS) from
0 to 10, with 0 being no video/audio at all and 10 being perfect video/ audio quality.
The three experiments will be carried out with both the Motorola Razor as well as the Sharp
903SH. Since the Sharp 903SH has two connection setting (a setting that prioritizes quality
and a setting that prioritizes speed), audio, video and time delays will be judged in both
settings.
As a reference site the Horst building of University of Twente will be used. Here a baseline
experiment will be done. This will be done by two persons sitting in two separate rooms next
to each other (as seen in fig. 5). A video call will be initiated and evaluated. During the
22Video telephony in the (sub)acute care for ALS patients
baseline experiment a test will be done to measure the roundtrip delay time for audio with
various phones and settings.
Figure 5: schematic presentation of the baseline experiment
The audio roundtrip time will be measured as follows. During the video call the person in
room A will make a noise which is audible in room B (through the wall). The person in room
B will have a stopwatch, at the moment that he hears the noise from room A he will start the
timer. When the person in room B hears the noise from room A via his mobile he will stop
the timer.
All other calls will be judged in comparison to the baseline experiment. In table 4 a list of
locations is given which will be visited and tested for UMTS reception. Every location has
been tested twice.
Type of
Location Zipcode
location
University
Universtity of Twente 7522NB
building
Perseusstraat 79 Student home 7521ZB
Sl louwesstraat 85 Student home 7545ES
Livio (Even numbers) Nursing Home 7544 NT
Livio (Uneven numbers) Nursing Home 7544 NX
Revilidation
Roesingh 7522AH
centre
R&D facility of
Roesingh Research and Development 7522AH
the Roesingh
Table 4 Locations used for the UMTS test
23Video telephony in the (sub)acute care for ALS patients
3. Results
3.1. Experimental Group: Patient visits
On the 3rd of September 2007 five patients were visited and introduced to the videophone.
Five patients were visited instead of ten because there was a lack of good UMTS coverage at
other patient homes. The objective was to get preliminary data on how the patients respond to
a videophone and to test the protocols that were made. The “UMTS – group” protocol in
Appendix D was followed. The patients were assigned a study number and given a telephone.
At the patients the project and the functions of the phone were explained. After that four
questionnaires were filled in:
AU1 – ALS questionnaire
BTU1 – Usability questionnaire telephony
SFU1 - Shortform 36
VVU1 – Video telephony expectations questionnaire
It was notable that the leading physician plays a vital role in conducting the patient visits.
During every patient visit the lead physician explained the project and helped the patients and
or family members fill in the different questionnaires. Visiting the patients was a good way to
observe at firsthand how patients initially reacted to the videophone and to see if the chosen
tools were usable. It is apparent that the patients trust the lead physician very much. Also
every patient used the opportunity of the lead physician visiting them at home to ask him
questions (which they could also have asked via the phone).
In the commentary below describing the different patient visits, patients are referred to by
study number. The “U” prefix indicates membership of the experimental group (the group
given UMTS video phones).
U001 was a 51 year old male, living with his wife and 2 daughters. His wife and one of the
daughters filled in the questionnaires for their father since the patient himself was sleeping.
The family of this patient are more likely to call the physician than the patient himself since
ALS is in the final stages. The first symptoms of ALS appeared 20 months ago. The total
score on the AU questionnaire was 24 points of the maximum 60 points, where a score of 60
means no limitations and 0 means the most extreme limitations.
U002 was 74 year old male, living with his wife. His daughter was also present during the
explanation of the project. The patient could fill in the questionnaires himself with a little
help from the lead physician. The first symptoms of ALS appeared 34 months ago The total
score on the AU questionnaire was 44 points of the maximum 60 points.
U003 was a 48 year old female living with her husband. This patient didn‟t have any control
left in her limbs so the lead physician and her husband filled in the questionnaires for her. Her
husband would also be the person to call the physician via the videophone. The first
symptoms of ALS appeared 72 months ago. The total score on the AU questionnaire was 5
points of the maximum 60 points,
U004 was 57 year old male living by himself. He stated that was unsure about participating in
the project because he was unsure if he could understand the technology. The first symptoms
of ALS appeared 15 months ago. The total score on the AU questionnaire was 44 points of
the maximum 60 points. After the preliminary questionnaire this patient decided to withdraw
from the project.
The fifth patient didn‟t want to participate in the project. The patient said that she had very
little affinity with technology and wouldn‟t be able to understand the telephone.
24Video telephony in the (sub)acute care for ALS patients
3.2. Preliminary results patient questionnaires
3.2.1. ALS questionnaire (AU1)
The ALSFRS-R questionnaire shows in what stage of ALS the patient is at the time of the
experiment. These results will be used to check the uniformity of the patient group. In table 5
the results from the ALSFRS-R questionnaire is shown next to the disease duration and the
age of the patients.
Table 5 total score for the ALSFRS-R questionnaire next to disease duration and age.
The thick black line indicates the maximum score of 60 for the ALSFRS-R questionnaire (a
score of 60 means perfect health). This table confirms that no two people have the same
course of the disease and that the patient group is quite variable. U002 and U004 are in
generally the same stage of ALS. The age group is around 50 years of age except for U003.
3.2.2. Shortform 36 (SFU1)
Shortform 36 has a 0 – 100 scale for 8 variables, 0 being the worst and 100 the best score.
This questionnaire shows how the patient perceives his or her own health status. In the table
below the different scores per patient are shown. All variables are shown and a physical and
mental health summary is given. These summaries are average scores for the four mental and
physical components for SF36. The mean scores for both of the physical and mental
summary is 50 (for the general adult population in the US).[20] It is interesting to see that
U001 and U002 are the patients with the highest mental health perception even though U004
is in generally the same or less severe stage of ALS. Another interesting outcome is that
U003 has a higher physical health score than U001 even though U003 is in a very severe
stage of ALS. All patients feel they are severely limited in their physical role but in their
mental health U001 and U002 are above average but U003 and U004 are below average.
Patients U001 U002 U003 U004
Variables
Physical functioning 0 70 0 20
Social functioning 50 75 25 12,5
Role limitations:
Physical 0 0 0 0
25Video telephony in the (sub)acute care for ALS patients
Emotional 100 100 0 0
Mental health 75 90 75 30
Energy/vitality 31,25 81,25 31,25 31,25
Pain 22,5 87,5 45 45
General health perceptions 30 50 20 0
Physical health summary 13 51 16 16
Mental health summary 64 86 32 18
Table 6 outcomes from the Short Form 36 questionnaire
3.2.3. Usability questionnaire telephony (BTU1)
The usability questionnaire shows how the patients see their current situation. This situation
is with a regular mobile phone number that they can call 24 hours a day and 7 days a week.
The total score range for this questionnaire is 0 – 80, 80 being completely satisfied regarding
the usability of regular telephony. Table 7 shows the results of the four patients.This shows
that people are generally satisfied with the use of a regular telephone, except for U004.
Table 7 total scores for the telephony usability questionnaire
Interesting results from the questionnaire:
Patient Number
Totals U001 U002 U003 U004
I can explain my medical problems adequately during Agree 2 1 1
a telephone consultation Neutral 2 1 1
Agree 2 1 1
Talking with a healthcare professional via a telephone Disagree 1 1
gives just as much satisfaction as talking to a
healthcare professional in real life. Totally
disagree 1 1
Agree 3 1 1 1
Telephone consults are a convenient form of
healthcare for me Totally 1 1
disagree
Agree 3 1 1 1
Telephone consults save me time
Neutral 1 1
I prefer a telephone consultation to a face to face Agree 2 1 1
consult Neutral 1 1
26Video telephony in the (sub)acute care for ALS patients
Totally 1 1
disagree
Table 8 selection of results from the questionnaire
In table 8 a selection of questions from BTU1 and their results are shown. As was noticeable
from the total scores of this questionnaire, patient U004 was negative towards usability of
telephony in his care process. Patient U001, U002, U003 however were more positive. The
results show that patients are able to explain their medical problems adequately. Also
interesting to see is that most patients feel that talking on the phone with the health care
professional gives just as much satisfaction as talking to that person in real life. The patients
agree that telephone consultations are a convenient form of a healthcare for them and save
them time. Two of the four patients would prefer a telephone consultation to a face to face
consult.
3.2.4. Video telephony expectation questionnaire (VVU1)
The video telephony expectation questionnaire has higher total scores per patient than the
Telephone usability questionnaire, indicating that the patients have a higher expectation of
the quality of the contacts via videophone than via conventional phone. The max score was
65.
Table 9 total scores for the video telephony expectation questionnaire
Patientnummer
Totals 1 2 3 4
I expect that my healthcare professional can Agree 3 1 1 1
answer my questions via a video consultation Neutral 1 1
I expect that my healthcare professional can get a Agree 3 1 1 1
good understanding of my condition
during a video consultation. Neutral 1 1
I expect that I can explain my medical problems Agree 3 1 1 1
well enough during a video consultation. Neutral 1 1
I expect that talking with a healthcare professional Agree 1 1
27You can also read