What Do Primary Care Physicians REALLY Need To Know About Bipolar Disorder
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

What Do Primary Care Physicians REALLY Need To Know About Bipolar Disorder J. David Moore MD Clinical Assistant Professor, Associate Residency Training Director Department of Psychiatry and Behavioral Medicine Greenville Health System / University of South Carolina Greenville Greenville, SC
Disclosures • No financial disclosures • In the course of this presentation, medications will be discussed for off- label usage.
Objectives • Let’s make this subject as simple and useful as possible for a busy primary care setting • How to rule out the false positives in bipolar screening/Screening Tools • Differentiate bipolar disorder from other psychiatric disorders • How to treat bipolar disorder in the short-term (
Your patient says WHAT?
• “I have mood swings.”
• “I can’t control my mood. There’s nothing I can do about it… Yes, I try.”
• “I can get mad in a split second…I get upset over nothing.”
• “My Prozac was working, but then it just quit working.”
• “I’m up and down all the time. I must be rapid cycling.”
• “My mind is racing.”
• “It’s like I have a split personality.”
• “My {mom/dad/sibling/child} acts the same way as I do, and they have
bipolar, so I do too, right?”Some general facts about Bipolar Disorder
• Men and women are affected equally
• Mean age of onset is 19yo-25yo
Mean age in unipolar depression is roughly 25yo-35yo
• Cause ????? Unknown, but family and twin studies suggest genetic risk
• Lifetime risk of suicide is 15x higher in bipolar patients as compared to
general population; roughly 15% will complete suicide
• About 1/3 of bipolar patients wait >10 years for accurate diagnosis
• Significant co-morbidities: 59% anxiety, 48% substance abuse,
9% ADHD, 8% eating disordersSchizophrenia vs Bipolar – Common?
• Prevalence (lifetime) in general population of
schizophrenia = 1.1%
• Prevalence (lifetime) in general population of bipolar
disorder=1-2% but it varies, depending whom you ask:
▫ Per DSM-5 = 0.6% for bipolar I
12 month prevalence for all types of bipolar = 1.8%
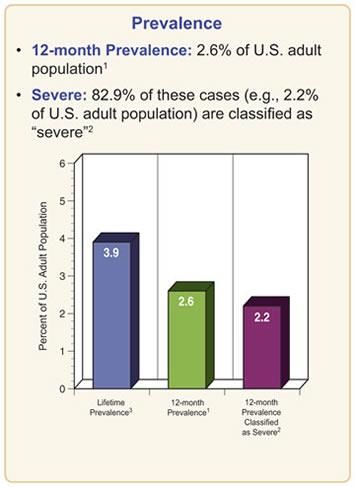
▫ Per NIMH = 3.9% for bipolar I
12 month prevalence for all types of bipolar = 2.6%
Graphic: NIMHBipolar vs Other Disorders– Common? • Prevalence (lifetime) in general population of bipolar disorder=1-2% • Major depression= 12-15% • Anxiety disorders=30% • Borderline personality disorder=1.5% • Adult ADHD=9%
Comparing Apples to Apples: Let’s define ‘BIPOLAR’ • Bipolar I – has manias and depressions • Bipolar II – has hypomanias and depressions • Cyclothymia – has hypomanias and depressive symptoms • Substance/Medication-induced Bipolar Disorder • Bipolar due to Another Medical Condition
Comparing Apples to Apples: Let’s define ‘BIPOLAR’
SUBSTANCES/MEDICATIONS OTHER MEDICAL CONDITIONS
• Any illicit drug • Head trauma, cerebral tumor, CVA
• Indomethacin • Dementia
• Stimulants • Epilepsy
• Interferon, isoniazid • Multiple sclerosis
• Hydralazine, reserpine • Parkinson’s disease
• Corticosteroids • Cushing’s, Addison’s
• Anticholinergics • Hypo- or Hyperthyroidism
• Levodopa • HIV, Mono, Influenza, Hepatitis
• Vincristine, vinblastine • Tertiary syphilis
• Etc. • Toxoplasmosis
• Etc.Let’s define ‘DEPRESSION’: “SIGECAPSS” • S - sleep changes • I – interest less (anhedonia) • G – guilt/worry • E – energy less • C – concentration less • A – appetite changes • P – psychomotor agitation/retardation • S – suicidal thoughts • S – sexual interest low
Comparing Apples to Apples: Let’s define ‘MANIA’
• MANIC = lasts 1 week or longer, of persistently elevated, expansive, or
irritable mood AND increased goal-directed activity or energy AND has
at least 3 symptoms(4 if mood is just irritable) of:
Inflated self-esteem or grandiosity
Markedly decreased need for sleep
More talkative or pressure to keep talking
Flight of ideas or racing thoughts
Distractibility
Increase in psychomotor activity
Excessive involvement in activities with high potential for painful consequences,
such as promiscuity, foolish business investments, unrestrained spending spreesLet’s define ‘MANIA’: “DIGFAST” • D – distractibility • I – indiscretion, irresponsibility • G – grandiosity • F – flight of ideas/racing thoughts • A – activity increased • S – sleep decreased • T - talkativeness
Comparing Apples to Apples: Let’s define ‘HYPOMANIA’
• HYPOMANIC = lasts at least 4 consecutive days, of persistently elevated,
expansive, or irritable mood AND increased goal-directed activity or
energy AND has at least 3 symptoms (4 if mood is just irritable) of:
Inflated self-esteem or grandiosity
Markedly decreased need for sleep
More talkative or pressure to keep talking
Flight of ideas or racing thoughts
Distractibility
Increase in psychomotor activity
Excessive involvement in activities with high potential for painful consequences,
such as promiscuity, foolish business investments, unrestrained spending spreesComparing Apples to Apples: Let’s define ‘BIPOLAR’
• MUST have had a manic or hypomanic episode; but there does NOT
have to have been a major depressive episode for Bipolar I (Bipolar II
requires both hypomania and depression)
• Mania and hypomania have almost the same criteria, with the main
differences in:
1. length of episode (4+ days vs 7+ days)
2. marked impairment (or not) in social or
occupational functioning
3. if psychosis present, then it is NOT hypomaniaComparing Apples to Apples: ‘RAPID CYCLING?’
Yes, it does exist, and here’s when it does:
Can occur in Bipolar I or Bipolar II
Presence of at least 4 mood episodes (mania, hypomania, and depression)
over past 12 months AND:
Episodes are demarcated by full or partial remissions of 2 months between
switches
Must include a full switch to opposite polarity at some point
Must meet all duration and symptom number criteria for each episodeScreening Tool: The MDQ (Mood Disorder Questionnaire)
• The validity of it……
• 3 parts to it:
▫ 1. symptom checklist
▫ 2. “have the symptoms happened during the same period of time?”
▫ 3. “have the symptoms caused moderate to severe problems with work,
family, money or legal troubles, arguments or fighting?”
• Are you prepared to ask many more questions?Psychiatrists don’t get it right either “The Mood Disorders Questionnaire screens for bipolar disorder. This screen was positive, suggesting that bipolar disorder is present. He is irritable. A decrease in sleep has occurred. He has been over-talkative. He describes racing thoughts. He is distractible. He has an increase in sociability and libido.” - this is exact quote from a medical record, in an initial evaluation by a psychiatrist, to justify the diagnosis of a bipolar disorder
Bipolar in children and adolescents
• Prevalence prior to adolescence:
No great studies or data, but likelyDISRUPTIVE MOOD DYSREGULATION DISORDER
• Core feature is chronic, persistent irritability in association with severe
temper outbursts
▫ Inconsistent with developmental age
▫ Occurs 3 or more times per month
▫ Present for >12 months
▫ Occurs in at least 2 settings (at home, at school, with peers)
▫ Not before 6yo, and can be made up to 18yo; symptoms have to have been
present by 10yoTreatment Options in the Primary Care Setting
• Refer out to psychiatry
Are there any psychiatrists in my area?
Is my patient willing to go see THAT kind of doctor?
Do they take insurance? Can my patient afford it?
How about a therapist? If so, what are you going to suggest for medications?
What’s the waiting time to see a mental health provider?
• Treatment
Therapy
MedicationsOptions for Medications
• What kind of patient is this?
Age, child bearing age, fall risk, history of being compliant vs non-compliant
• What are the patient’s other medical issues?
Renal issues, hepatic impairments, dementia, substance use disorders, cardiac
issues
• What other medications are they on?
NSAID’s, steroids, inhalers, stimulantsThe medications FDA-approved in bipolar disorder FOR ACUTE MANIA IN BIPOLAR FOR ACUTE DEPRESSION IN BIPOLAR • LITHIUM • OLANZAPINE/FLUOXETINE • CHLORPROMAZINE • QUETIAPINE (and XR) • DIVALPROEX (and ER) • LURASIDONE • OLANZAPINE • RISPERIDONE • QUETIAPINE (and XR) • ZIPRASIDONE • ARIPIPRAZOLE • CARBAMAZEPINE ER • ASENAPINE
The medications FDA-approved in bipolar disorder FOR MAINTENANCE IN BIPOLAR • LITHIUM • LAMOTRIGINE • OLANZAPINE • ARIPIPRAZOLE • QUETIAPINE (and XR is adjunct only) • RISPERIDONE LAI (CONSTA) • ZIPRASIDONE (adjunct only)
Let’s talk treatment
• LITHIUM has long been considered the first line care and is the gold
standard for bipolar disorder.
• PROS: It works!
Defined serum blood level for efficacy (0.8-1.2)
1 of only 2 proven medications to prevent suicide.
“A little lithium is better than no lithium.”
Inexpensive (the medicine itself)Let’s talk treatment
• LITHIUM has long been considered the first line care and is the gold
standard for bipolar disorder.
• CONS: Need lab work-ups intermittently (can be expensive)
Other entities affect the blood level (dehydration, NSAID’s,
diuretics)
Nuisance side effects: diarrhea, weight gain, tremor, acne
Other side effects: hypothyroidism, hyperparathyroidism,
diabetes insipidus, decreased Cr clearance with long
term use, prolong QTc, pregnancy risks, leukocytosisLet’s talk treatment
LAMOTRIGINE (LAMICTAL)
• PROS: few side effects
proven efficacy in bipolar depression
no lab monitoring
• CONS: very small (Let’s talk treatment
VALPROATE (DEPAKOTE/DEPAKENE)
• PROS: has been around a long time, and many specialties use it and
are comfortable using it
very effective in manias/hypomanias
• CONS: requires lab monitoring
Nuisance side effects: hair loss, nausea/vomiting, weight gain
Other side effects: thrombocytopenia, pregnancy risks,
hepatic effects (increase liver enzymes)
not very effective in bipolar depressionLet’s talk treatment
CARBAMAZEPINE (TEGRETOL)
• PROS: has been around a long time, and many specialties use it and
are comfortable using it
effective in manias/hypomanias
• CONS: requires lab monitoring
Nuisance side effects: nausea/vomiting, rash, diplopia
Other side effects: leukopenia, pregnancy risks,
hepatic effects (increase liver enzymes)
not very effective in bipolar depression
induces own metabolism as well as many other medsLet’s talk treatment
• All the others: SECOND GENERATION ANTI-PSYCHOTICS
ARIPIPRAZOLE (ABILIFY)
• PROS: -no initial labs
-less sedation, less weight gain, less endocrine effects,
less prolactin issues
-samples, coupons, etc.
• CONS: -very expensive (but about to get cheaper)
-akathesia/agitation (dose it in AM)Let’s talk treatment
• All the others: SECOND GENERATION ANTI-PSYCHOTICS
LURASIDONE (LATUDA)
• PROS: -no initial labs
-less sedation, much less weight gain, much less endocrine
effects, rare prolactin issues
-samples, coupons, etc.
• CONS: -very expensive (and not about to get cheaper anytime soon)
-nausea, akathesia, and sedation are main side effects
-dose? – it’s a wide rangeLet’s talk treatment
• All the others: SECOND GENERATION ANTI-PSYCHOTICS
QUETIAPINE (SEROQUEL/SEROQUEL XR)
• PROS: -no initial labs
-sedation can be a really good thing
-rare to no EPS/TD issues
• CONS: -relatively inexpensive
-weight gain and sedation are main side effects
-endocrine effects
-dose? – it’s a wide rangeLet’s talk treatment
• All the others: SECOND GENERATION ANTI-PSYCHOTICS
OLANZAPINE (ZYPREXA) or FLUOXETINE/OLANZEPINE (SYMBYAX)
• PROS: -no initial labs
-sedation can be a really good thing
• CONS: -weight gain and sedation can be more than you ever thought
possible
-endocrine effects are common with olanzapine
PLEASE NEVER PRESCRIBE SYMBYAX! Your referring ‘quality’ psychiatrist
will thank you for never doing that.Let’s talk treatment • Some others: ▫ RISPERIDONE, ZIPRASIDONE, ASENAPINE, PALIPERIDONE
Let’s talk treatment • All the others: FORGET ABOUT THEM!!!! (for bipolar treatment) ▫ GABAPENTIN, TOPIRAMATE, OXCARBAMAZEPINE, LEVETIRACETAM, etc.
“I have 5 minutes. What should I do?”
1. Get rid of problematic medicines/polypharmacy, if you can
stimulants, SNRI’s/tricyclics, non-useful psychiatric meds, reconsider non-
essential asthma meds or steroids
2. Get them to sleep
Benzo’s (lorazepam, clonazepam), zolpidem, quetiapine, olanzapine
3. Think long-term and start LAMOTRIGINE, whether depressed or manic
25mg x2 weeks then 50mg x2weeks then 100mg x2weeks then 200mg qday“I have 5 minutes. What should I do?”
4. Think short-term and start LITHIUM or SGA, if in mania/hypomania
Lithium 300mg bid-tid – check level in 5-6 days at 12 hour trough and adjust;
you can also get baseline labs at that time OR,
Aripiprazole 5-10mg qam OR,
Quetiapine 100-300mg qhs OR,
If you are not yet starting lamotrigine, then valproate 500mg bid is also an
option“I have 5 minutes. What should I do?”
5. Think short-term and start LITHIUM or ANTI-DEPRESSANT, if in
depression
Lithium 300mg bid-tid – check level in 5-6 days at 12 hour trough and adjust;
you can also get baseline labs here OR,
Any SSRI OR,
Bupropion XL 150mg qam (and wait 3-4 weeks and then decide if need to
increase to 300mg qam if not better)What else could this be psychiatrically?
• Anxiety disorder
Generalized anxiety disorder
Panic disorder
PTSD
OCD
• ADHD
• Substance Abuse/Intoxication/Withdrawal
• Unipolar Depression
• Borderline Personality DisorderBorderline Personality Disorder : “I DESPAIRR” • I – identity problem • D – disordered affect • E – empty feeling • S – suicidal behavior/self-harm • P – paranoia/dissociation • A – abandonment terror • I – impulsivity • R – rage • R – relationship instability
The Brownell Center at Greenville Health System USC School of Medicine Greenville 2 locations: 701 Grove Rd and 1409 West Georgia Rd Greenville, SC Simpsonville, SC 864-455-8431 (for both locations)
You can also read