Why Channel 4's Embarrassing Bodies is in rude health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Why Channel 4's Embarrassing Bodies is in
rude health
Voyeuristic, sensationalist, revolting… Embarrassing Bodies is accused of being all of these.
So why are people prepared to share their unsightly medical problems with a record-breaking
TV audience?
o Eva Wiseman
o The Observer, Sunday 5 September 2010
Dr Christian Jessen
with Doctors Dawn Harper and Pixie McKenna. Photograph: Channel 4
A sweaty morning at Thorpe Park, and the smell of sunblock and ketchup hangs heavy in the
air. In the shade of Saw, a freefall rollercoaster based on the torture-porn franchise, and beside
a grey but warming lake, a crowd is gathering by the Embarrassing Bodies truck. For one day
only, Dr Christian Jessen and Dr Dawn Harper will be consulting in the back of their well-lit
van, a televised surgery open to anybody passing between rides. Provided, of course, that
they're within the 70% of the population suffering from an embarrassing illness – varicose
veins, excess hair, stretchmarks, alopecia, IBS, obesity. Something that oozes, preferably.
Something swollen.
Rosie and Kelly are 13 years old, and so excited to be in the presence of Dr Christian that
they're quivering, visibly. As fans of Embarrassing Bodies, the Channel 4 show that offers
contributors lengthy medical attention in exchange for a close-up of their glittering piles,
they're recalling their favourite episode from the three series so far. Was it the episode with
the interior designer's oversized labia? Was it the one about the woman with the udder-like
breasts? The one with Christina's anal warts? They remember all of those, but their favourite
was the episode where Dr Christian stood in a locker room to compare the penis sizes of a
whole rugby team. "It was brilliant," they say. "He was brilliant. I'd definitely go on the show,
if I had something wrong." Then I ask Rosie and Kelly, as I will ask many people over the
next few days, the question most asked about Embarrassing Bodies: if the problem
embarrasses them, why do patients choose to go on telly with it? They answer, but I'll come to
that.
Embarrassing Bodies, produced by Maverick TV, first appeared on Channel 4 in 2007, an explosion of incontinence and skin rashes, with Ashley Jensen's voiceover explaining the statistics around the illnesses shown. In the Evening Standard, Victor Lewis-Smith wrote that the show was "admirable, unpalatable, fascinating and repulsive in roughly equal measure". Since then it's become furiously successful, the most watched programme on Channel 4 this year, consistently winning audiences of up to four million, double the average ratings for its 9pm time slot. The show has covered 120 different conditions to date. After last month's special episode, about a nine-year-old girl called Charlotte who visited the clinic with extreme verrucas – her feet were covered in molluscs – and was found to need a bone marrow transplant, the Anthony Nolan Trust reported a 4,000% increase in enquiries. Embarrassing Bodies's Bafta- award-winning website is responsible for 42% of Channel 4's web traffic, and its STI checker has, at last count, been used by one million people. More than 150,000 viewers took their online autism spectrum test, creating the world's largest test of its kind. The website is also used as an example of how television is moving towards a "multiplatform" future – spikes in Embarrassing Bodies's web traffic during the show proved viewers are watching with their laptops open, tapping their own questions into the message boards, clicking through the "vulva gallery" or applying to be on the show. Adam Gee, cross-platform commissioning editor for factual programming at Channel 4, explains, "It was the first evidence that multiplatform for factual could work and find an audience." Along with Drs Dawn Harper and Pixie McKenna, Dr Christian Jessen is the face of Embarrassing Bodies. The face, the arms, the muscular chest, the skin of which can often be seen peeking from a carelessly buttoned polo shirt, the colour of cured meat and the size of a healthy bottom. We meet as he comes off the rollercoaster Colossus, where he's been testing his heart rate for a piece about stress levels. He happily poses for photographs for fans and gives me an apologetic grin as he signs another autograph. Last year Jessen hit the headlines when Gordon Brown's spin doctor, Damian McBride, sent an email to Labour blogger Derek Draper, suggesting they spread the unfounded story that David Cameron had suffered from a sexually transmitted disease. He also suggested "inserting [a] picture of Dr Christian Jessen", implying the Embarrassing Bodies doctor, also a practising Harley Street GP, had treated the now Prime Minister. "I can't say I've never met David Cameron," Jessen said at the time, also unable to deny it. "It's interesting, because if you say, 'No, someone's not a patient', is that also a breach of confidentiality?" His main gripe with the story, he said, was the suggestion that treatment for an STI could have brought down a government. "I was particularly disappointed because there I am, slogging away, trying to make people feel more comfortable talking about these things, and then this idiot undoes it all in one email by implying it is shameful and embarrassing. It made me very cross." Jessen is very posh, very clever and very charming. He grew up in Fulham, west London, went to boarding school and graduated from UCL in 2000, when he moved to Kenya and Uganda to research HIV and malaria in children. Now 32, he lives with his partner and miniature Pinscher in London.

When he joined the show, he didn't think it would last. "I didn't think piles and verrucas would be exciting to a Channel 4 audience," he says, "but I soon realised that people hadn't seen the novelty of haemorrhoids before, because we're usually pretty crap about talking about this stuff. Yes it's a bit gross, but we never treat it in a sensationalistic way. It's good, practical telly, and that's why it works." I can't help but comment on his muscles. They're glinting in the sunlight, swelling like hams in my sightline. He thanks me. "I like it when people think I don't look like a doctor – that's why we were cast. We're not bow-tied, spectacled, dull. There's a need for normal-looking people in the medical profession I think, a crying need for doctors who are approachable." On screen, they're referred to as Dr Christian, Dr Dawn. "It's a very closed business, very secretive and reverential. And our harshest critics are other doctors." Dr Dee Dawson, medical director of the Rhodes Farm eating disorder clinic, has watched Embarrassing Bodies from her London sofa. She says the show "sensationalises serious illnesses and pleases ghoulish audiences with its tabloid format". But, she continues, "in doing that, it also alerts them to potential problems, and I'm sure people are more likely to see their doctors after watching an episode relevant to them, in the same way that we saw a spike in smear tests after Jade Goody talked about her cervical cancer. It's horrendous," she says, "and so overly dramatic, but it's a positive thing, in the end. In fact, my father only had a melanoma diagnosed after watching a medical programme on TV." Inside the Embarrassing Bodies truck, a screen separates the surgery set and a tiny waiting room, where a bowl of pink orchids erupts on the coffee table. The first patient to walk in from the park is 23-year-old Natasha, who wants to talk about irritable bowel syndrome. Her boyfriend, Peter, waits patiently by the fence. "We love the show," he tells me. "My mother died of skin cancer this year and the programme showed me the warning signs to look out for. Plus all the blokes with their tackle out – they ask questions I wouldn't dare!" As the cameras roll, Dr Christian asks Natasha about her loose stools. "The message," he says, after a brief conversation, "is don't panic, but be insistent. Fight for help, and find a GP that will ask for more tests." Outside in the sunshine Natasha is elated. "That was so fantastic," she says. "He gave me the confidence to go back to my doctor. And yes, it's an embarrassing problem, but when you finally talk about it you feel so much better." Why did you decide to go on TV with it? "Well," she says, "I love the show. And I love that the doctors make themselves so approachable. GPs, usually, are so busy they don't have time to listen. And I honestly think the show is changing young people's views on how they communicate about their bodies." Rosie and Kelly, still lurking for another glimpse of Dr Christian, agree. They say that their friends wouldn't laugh at them if they appeared on Embarrassing Bodies because the fact it's on TV legitimises the problem – takes the shame away. Dr Dawn Harper, who's an NHS GP in Gloucestershire when not filming, says one of the reasons people decide to take their problems on the show is the brand recognition. "They've

seen us on TV, so they trust us. Plus, there's a huge sector of society that thinks: 'If it's not life threatening, I mustn't bother my doctor', or they've felt a lack of sympathy from them in the past. And while women are always registered with the doctor for their smear test, men are often still registered at their mum's GP. Viewers feel like they know us a bit. They've seen how we interact with patients so they know what to expect. And we have support from more and more specialists as the show grows, so there's the availability of things that aren't offered on the NHS." I hear all Harper's reasons repeated by patients as the day goes on. Kelly Coulter, who's brought her 18-month-old son to the truckstop to talk about a problem with his gums, says she'd "absolutely get my breasts out on the show if I was guaranteed a boob job". Plastic surgery is a subject often broached in the programme. Jessen (who talked to the Daily Mail about his hair transplant in May) tells me, "I'm for plastic surgery, as long as the industry doesn't take advantage and prey on us." One of the surgeries Jessen recommended on an episode in 2008 was a patient's labioplasty. In her book Living Dolls, Natasha Walter details how uneasy this made her feel. "[In this episode] a young woman consulted a doctor about the fact that her labia minora extended slightly beyond her labia majora and that this caused her embarrassment. Instead of reassuring her that this was entirely normal, the doctor recommended, and carried out, surgery on her labia. The comments left on the programme's website showed how this decision to carry out plastic surgery to fit a young woman's body to a so-called norm made other young women feel intensely anxious. 'I'm 15 and I thought I was fine, but since I've watched the programme I've become worried, as mine seem larger than the girl who had hers made surgically smaller! It doesn't make any difference to my life, but I worry now that when I'm older and start having sex I might have problems!' one girl said. "This idea that there is one correct way for female genitals to look is undoubtedly tied into the rise of pornography… If the rise of pornography was really tied up with women's liberation and empowerment, it would not be increasing women's anxiety about fitting into a narrow physical ideal," wrote Walter. I ask Jessen whether this patient's referral was a difficult decision. "It's a hugely controversial subject, but she was having dreams about cutting off her labia. To me, that justifies the treatment – she was grossly psychologically disturbed." Is he concerned that with this decision he might encourage female viewers to seek surgery when there's no medical problem? He sighs. "It's our job to show all available treatment. And if it creates a forum for girls to talk about their bodies… We try our best – there's no malice in what we do." A few days later, in their Birmingham clinic/studio, a set lit so whitely it feels like a 1960s vision of heaven, I meet John. I'd heard about John. Once, over lunch, a friend told me about the programme she'd watched the night before. Wide-eyed, she used her hands to describe an operation they'd shown, where, in order to cure the man's perianal abscesses, they'd stretched his anus open with metal pegs, so that, square, it filled the TV screen neatly. The image stays with her still. When John, now 27, returns to Embarrassing Bodies, it's after 15 operations; he says he's feeling "the best I have in four years". The problem began when he was 23, and a prison officer in Nottingham. One night, an inmate threw a television from the floor above – it landed inches from where John was standing and
he had a panic attack. He took a week off due to stress and it was then that he noticed the first swelling. When the abscess burst inside him, it spread. The pain, he says, was like "being kicked in the spine", and once it caused him to black out. But worse than the pain, he says, was the humiliation of asking his girlfriend, who he'd met while recovering from his eighth operation, to regularly clean his seeping wounds. "He'd had to wear a nappy in his pants," Dr Pixie McKenna tells me. "It was so, so sad." The episode of Embarrassing Bodies which concentrated on Charlotte Wilson's verrucas inspired John to seek them out – John chased their truck stops around Britain, finally getting a walk-in appointment with Dr Pixie when he'd just come off a night shift. "I saw that they'd saved that little girl's life, so I wanted them to fight my corner," John tells me. "And I thought if they could help me out, then showing my backside on national TV would be a small price to pay." When John's episode aired, he found out later, his prison colleagues had thrown an Embarrassing Bodies party, where, during the screening of his operation, someone had thrown up on their pepperoni pizza. Today, after shyly admitting that his girlfriend has agreed to marry him, he's happy to drop his trousers and show his scars to Dr Pixie, who gasps with pleasure. "That is not the same bottom that I first met!" she cries. Michelle, 45, is birdlike, and woke at five to drive down from Lancaster, where she's proud to live in an Area of Outstanding Natural Beauty. When she told her 19-year-old son she was thinking of approaching Embarrassing Bodies about her constipation after a post- hysterectomy prolapse, he said he wasn't happy about it, but that if it would help, he'd support her. Sitting in the surgery, camera angles mean she must answer Dr Pixie's question – "Do you get any soiling?" four times. Her examination is over in seconds – a rectocele is diagnosed – and the screen where I'm sitting fills with an internal HD image. "Embarrassing Bodies doesn't believe in pixilation," the executive producer, Steph Harris, tells me. "It implies shame." I talk to Michelle over a cup of tea. "I was very apprehensive, yes," she says. She's sitting up straighter than she was before she entered the surgery – she seems to take up more space, somehow. "I was especially scared about the young cameraman, but he made me feel completely at ease. There was no pressure and lots of explanation. I'm so happy to have come." But why choose to broadcast your problem, I ask. "I come from a nursing background and this is one of my favourite shows, so I knew I'd get an honest consultation. And if nothing else, I wanted to highlight how common this problem is to other women. I'm not the only one of my friends to watch it either – I have a friend who's in hospital today after diagnosing herself with carpal tunnel syndrome when she saw it on the programme." For all the reviews pointing out Embarrassing Bodies's "crypto-pornographic nature", the criticism of the show's relationships with cosmetic surgeons, and the format, which relies on suspenseful ad breaks and the promise of genital close-ups, it's the patients who convince me that the programme does good, helping viewers talk about worries they'd otherwise hide.
Dr Dawn tells me about a recent event she went to with her NHS colleagues. "They tease me, of course they do, but that night 40 out of the 60 doctors there told me they'd seen patients purely off the back of the show." Interestingly, I think this is the only show in the makeover genre to include both male and female contributors. And while the occasional woman's saggy belly is hacked away by surgeons, the overall message is one of practical medicine: less about how you feel about your body, more about the body itself. And it's the only programme on telly where the haemorrhoid's the star. Embarrassing Bodies series four begins on C4 on 17 September. Can I Just Ask? (Hay House, £12.99) by Dr Christian Jessen, a collection of questions doctors are asked when off-duty, is published on 1 November Charlotte's story The case which turned the show into a national treasure In the autumn of 2008, nine-year-old Charlotte Wilson's mother, Sofia, led her into Dr Christian's clinic, seeking help for her verrucas. When he saw her feet, he was briefly speechless, but viewers saw his brain whirring into action. Verrucas, a common viral infection which most people's immune systems can quickly defeat, covered her toes in a terrifying crust. Dr Christian realised that this was an indication that Charlotte's immune system was losing the battle. She was referred to Great Ormond Street Hospital where the diagnosis was confirmed. The immunologist warned that in time Charlotte would be vulnerable to life- threatening infections. She needed a bone marrow transplant. Luckily, blood tests revealed that her sister Isabelle was a perfect match. Charlotte received chemotherapy in an isolation room, and after months away from home, she celebrated her 10th birthday in hospital, waiting for the bone marrow to take root. When the show aired, the Embarrassing Bodies website encouraged viewers to sign up for the Bone Marrow Register and the following day the Anthony Nolan Trust received 1,400 requests for information, as opposed to the usual 30. This week, the show's producer received an email from Sofia Wilson. "Charlotte looks fantastic," wrote her mother. "Lots of curly hair and a suntan... [Recovery] is going to take longer than we thought (Charlotte has to learn to stick a needle under her skin so that she can do her gamma-globulin infusion herself), but you saved our daughter's life".
More than 40% of domestic violence victims are male, report reveals Campaign group Parity claims assaults by wives and girlfriends are often ignored by police and media The Observer, Sunday 5 September 2010 Article history Assaults on men represent more than 40% of domestic violence in the UK. Photograph: Sakki/Rex Features/Sakki/rex About two in five of all victims of domestic violence are men, contradicting the widespread impression that it is almost always women who are left battered and bruised, a new report claims. Men assaulted by their partners are often ignored by police, see their attacker go free and have far fewer refuges to flee to than women, says a study by the men's rights campaign group Parity. The charity's analysis of statistics on domestic violence shows the number of men attacked by wives or girlfriends is much higher than thought. Its report, Domestic Violence: The Male Perspective, states: "Domestic violence is often seen as a female victim/male perpetrator problem, but the evidence demonstrates that this is a false picture." Data from Home Office statistical bulletins and the British Crime Survey show that men made up about 40% of domestic violence victims each year between 2004-05 and 2008-09, the last year for which figures are available. In 2006-07 men made up 43.4% of all those who had suffered partner abuse in the previous year, which rose to 45.5% in 2007-08 but fell to 37.7% in 2008-09.
Similar or slightly larger numbers of men were subjected to severe force in an incident
with their partner, according to the same documents. The figure stood at 48.6% in 2006-
07, 48.3% the next year and 37.5% in 2008-09, Home Office statistics show.
The 2008-09 bulletin states: "More than one in four women (28%) and around one in six men
(16%) had experienced domestic abuse since the age of 16. These figures are equivalent to
an estimated 4.5 million female victims of domestic abuse and 2.6 million male victims."
In addition, "6% of women and 4% of men reported having experienced domestic abuse in
the past year, equivalent to an estimated one million female victims of domestic abuse
and 600,000 male victims".
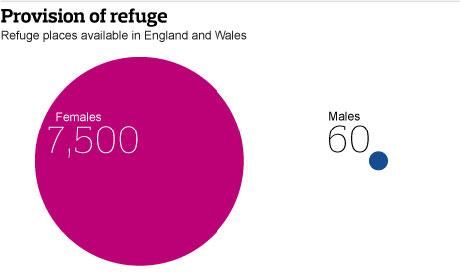
Campaigners claim that men are often treated as "second-class victims" and that many
police forces and councils do not take them seriously. "Male victims are almost invisible to
the authorities such as the police, who rarely can be prevailed upon to take the man's
side," said John Mays of Parity. "Their plight is largely overlooked by the media, in official
reports and in government policy, for example in the provision of refuge places – 7,500 for
females in England and Wales but only 60 for men."
The official figures underestimate the true number of male victims, Mays said. "Culturally
it's difficult for men to bring these incidents to the attention of the authorities. Men are
reluctant to say that they've been abused by women, because it's seen as unmanly and
weak."
The number of women prosecuted for domestic violence rose from 1,575 in 2004-05 to
4,266 in 2008-09. "Both men and women can be victims and we know that men feel under
immense pressure to keep up the pretence that everything is OK," said Alex Neil, the
housing and communities minister in the Scottish parliament. "Domestic abuse against a
man is just as abhorrent as when a woman is the victim."
'Male victims are
almost invisible to the authorities,' says John Mays of Parity. Photograph: Guardian
Mark Brooks of the Mankind Initiative, a helpline for victims, said: "It's a scandal that in
2010 all domestic violence victims are still not being treated equally. We reject the
gendered analysis that so many in the domestic violence establishment still pursue, thatthe primary focus should be female victims. Each victim should be seen as an individual and helped accordingly." CASE STUDY Ian McNicholl, 47, has painful memories to remind him of the terror he endured when he found himself a male victim of domestic violence. His then fiancee, Michelle Williamson, punched him in the face several times, stubbed out cigarettes on his body, lashed him with a vacuum cleaner tube, hit him with a metal bar and a hammer and even poured boiling water on to his lap. That at 6ft he was almost a foot taller than her made no difference. He still has burn marks on his left shoulder from when she used steam from an iron on him. Williamson, 35, is now serving a seven-year jail sentence for causing both actual and grievous bodily harm. During the trial last year McNicholl told the court that, during more than a year of attacks and intimidation, he had lost his job, home and self-respect. He had been too scared to go to the police and had considered suicide. She was only arrested after two neighbours saw her punch him. Sentencing her at Grimsby crown court last year, judge John Reddihough told Williamson: "Over the period of time you were with him you destroyed him mentally and seriously harmed him physically, leaving him with both physical and mental scars." Video (2min 00sec), Watch Keira Knightley in an anti-domestic violence ad 2 Apr 2009: Atonement actor stars in ad for Women's Aid aiming to raise awareness of domestic violence
The children who have two homes Ned and Nancy live half the week with their mother, the other half with their father. The model of a good divorce – or a recipe for confusion? By Lucy McDonald Tuesday, 28 September 2010 Richard Mildenhall Half and half: Kathleen Saxton with her children Ned and Nancy, have found a way of living that works It is Friday afternoon and Ned and Nancy Flaherty are being picked up from school by their mother, Kathleen. They look much like any other family. Nancy, 11, is chatting about swimming and Ned, 13, is complaining about homework. But this is the first time the kids have seen their mum since last weekend. After their parents split up eight years ago, Ned and Nancy divide their time equally between them. They spend Friday, Saturday and Sunday nights with mum, weekdays are spent a mile away with their dad, Adrian, a 38-year-old teacher. Holidays are split down the middle and everyone gets together for birthdays. They have two homes, two bedrooms, two games consoles and two toothbrushes. Their cats Sooty and Abigail move between houses with them. Kathleen Saxton, 37, who lives in Kent and runs a headhunting company, says: ―When Adrian and I broke up we were determined to make it as easy for the children as possible. It was really important for us to both be involved in their lives, so we focused on putting the children first. It is amazing what emotional pain can be put aside. It‘s worked well and the kids love having both of us as a big part of their lives.‖ Kathleen and Adrian managed to see through the acrimony and bitterness that can characterise a break-up. Twenty years ago it was unthinkable that following a relationship breakdown, children would live anywhere other than with the mother. Typically, visits from dad would happen twice weekly and there was little room for manoeuvre, but these days residency – it is
no longer called custody – is more fluid. Women‘s increased economic clout and the recognition of fathers‘ rights led to a change in society‘s – and the judiciary‘s – attitudes. Conrad Webbe, from support group The Association of Shared Parenting, says: ―Shared parenting is not necessarily about two homes. It‘s about supporting the idea that a child has a right to contact with both parents after separation or divorce. To cut a child off from a parent alienates them from their grandparents and half their heritage. For a child to be a balanced adult they need a father and mother.‖ Ned and Nancy agree. They could not conceive a life in which either parent did not play a full and varied role. Ned says: ―I‘m glad we don‘t live with just one parent because it would give you a feeling that there is another part of you that isn‘t in your life. I feel very lucky to have two houses and two parents.‖ Nancy says: ―I‘m happy because I get to see both mummy and daddy and if I didn‘t I would be homesick for them. It is fun having two bedrooms because you can have a different style in each room.‖ One in three couples – about 250,000 adults – divorce or separate every year and 350,000 children are affected. A study by the law firm Mishcon de Reya found that a third of children whose parents had broken up over the last 20 years had sought solace in drugs, while 10 per cent felt suicidal or became involved in crime. More than a third of children lose touch with a parent after separation. Conrad Webbe says: ―Our experience shows that when parental issues are put to one side, a shared parenting arrangement works well and dramatically reduces the short- and long-term potentially damaging effects on the children of family breakdown. It means they continue to have a real family life with both parents, which makes them feel more loved. It creates equity between the parents.‖ Shared parenting is popular in Europe, Australia and parts of America. Britain is lagging behind, although there are celebrity advocates. Blur guitarist Graham Coxon told a newspaper last year that he shares the parenting of his daughter with his ex-girlfriend. He says: ―My nine-year-old daughter, Pepper, stays with me on Friday, Saturday and Sunday, so it‘s an early start on those days ? she lives with her mum the rest of the week, but I drive her to school on a Monday.‖ Shared parenting sounds like the most child-friendly solution to the damage caused by family breakdown. Why isn‘t it enshrined in law and why don‘t more people do it? Karen Woodall, of the advice group the Centre for Separated Families, believes Britain holds deep-seated social and cultural beliefs that men are the providers and women the carers. Until we can shake off these stereotypes, shared parenting will never be fully embraced. She says: ―Part of the problem is that we‘re still clinging to the idea that a child without its mother is going to be damaged. We need to move beyond that. After separation children do best if both parents are involved. Many mothers who share parenting say they feel they‘re being judged for failing their children.‖ There is no official data on shared parenting but it is estimated that 500,000 households do it.
The Children and Family Court Advisory Support Service (Cafcass) – a government body that helps children in family proceedings – supports shared parenting (indeed, it is almost impossible to find a dissenting voice among those involved in family policy). Chief executive Anthony Douglas says that nowadays mothers and fathers have equal residency rights. He says: ―When you take out domestic abuse and parenting capacity issues, there is no gender bias in the family justice system. This is a sea change from 30 years ago.‖ Fathers‘ rights groups say the most important advance is not a 50/50 time split but the underlying admission of parental equality. We may embrace the idea of shared parenting but would we have chosen, or even wanted it as children, and would we want to explain its alleged social benefits to a child who just wants to sleep in the same bed every night? And a report by a former judge found that Australian law reforms regarding shared parenting had negatively affected children from violent and abusive backgrounds. Many women‘s groups and academics believe shared parenting is not always in children‘s interests. Deborah McIlveen, a spokeswoman for the domestic violence charity Women‘s Aid, says: ―We‘re concerned that contact is sometimes ordered without a proper risk assessment or consideration of the needs and wishes of the child and we will continue to campaign and work with the Ministry of Justice and other agencies until women and children are safe.‖ Around 10 per cent of family breakdowns end up in court – normally because of safety concerns or a parental power struggle. Cafcass says parents should avoid the financial and emotional drain of a legal battle and instead seek advice from support groups or through Parent Information Programmes – available through the courts or solicitors. A written agreement – however informal – is a solid bedrock for shared parenting. It should detail cultural values, parental boundaries, rules – even bedtimes. Karen Woodall says: ―Children fare well when parents set similar parameters. They don‘t have to move from vastly different cultural experiences.‖ Linda Blair, a psychologist and author of The Happy Child, advises: ―Accept that you and your partner no longer have an emotional relationship but a business relationship. Your business is bringing up your children. If you treat it like that you are less prone to be hurt and reopen old wounds.‖ Although putting aside old grudges can be tough, the results are worth it. All the research shows that children thrive when both parents play a big role in their life. www.sharedparenting.org.uk
GM food battle moves to fish as super- salmon nears US approval Consumer groups fear green light for engineered species will bring environmental disaster to the oceans A genetically modified salmon, rear, and a non-genetically modified salmon, foreground. Photograph: AP Buried in a prospectus inviting investors to buy shares in a fledgling biotech company is an arresting claim attributed to the UN's Food and Agriculture Organisation. "Commercial aquaculture is the most rapidly growing segment of the agricultural industry, accounting for more than $60bn sales in 2003. While land-based agriculture is increasing between 2% to 3% per year, aquaculture has been growing at an average rate of approximately 9% per year since 1970." And then the prospectus for the US company AquaBounty offers this observation to tantalise prospective investors: "The traditional fishery harvest from the ocean has stagnated since 1990." So what is to be done to satisfy the world's seemingly insatiable appetite for fish? An appetite that will see the consumption of farmed fish outpace global beef consumption by nearly 10% within five years, according to the UN? AquaBounty, whose shares are sold on London's Alternative Investment Market, thinks it has the answer. And if, as looks increasingly likely, the US government agrees, the implications for global food production will be enormous. Welcome to the new world heralded by the "GM salmon". The company's dream of selling genetically modified salmon eggs that allow the fish to grow to maturity in half the normal time received a giant fillip last week when it announced that the US Food and Drug Administration (FDA) was close to granting approval.
A positive FDA response would see salmon become the first GM-engineered animal marketed for human consumption. Dramatically speeding up the time it takes to harvest a mature salmon could stimulate a huge rise in production, making salmon plentiful and cheaper, GM enthusiasts say. AquaBounty expects to receive the nod by the end of this year, meaning GM salmon could be on supermarket shelves within three years. The company's share price doubled on the strength of the announcement. But the euphoria the company and its investors experienced following last week's announcement quickly evaporated amid a furious backlash from consumer groups. "The furore over this fish puts paid once and for all to the myth that US consumers are content eating GM food," said Eve Mitchell, European food policy adviser at Food and Water Watch Europe, which opposes GM food. "Consumers are not, and in fact jammed up the White House telephone lines last week protesting any approval. Quite understandably the salmon industry is not happy either, as people will simply avoid all salmon rather than risk getting this stuff. Only those who stand to gain financially think this is a good idea." Predictably, vested fishing interests have waded into the row. Local radio stations from Ireland to Canada carried interviews with angry fishermen who fear that initial reluctance to consume GM salmon will be overcome by simple economics. "Genetically modified food is just a bad deal," a commercial fisherman in Charleston, South Carolina, told his local station. "This will attack our marketplace. It'll come on the market so cheap that people will buy it, because we're all on a budget." Ronald Stotish, AquaBounty's chief executive officer, is keen to play down these particular fears. His company is more interested in selling its technology to the burgeoning markets of Chile, China and Asia rather than competing with Atlantic fishermen. "The global salmon market is very, very large and the opportunity is in areas that cannot raise salmon," Stotish told the Observer. "We don't believe it need threaten any national markets, particularly for the high-value premium markets. We are hopeful that people don't regard us as an economic threat, but simply look to us as a technology that maybe can become part of the future." If Stotish, a biochemist by training and an urbane advocate for his cause, succeeds, other companies are waiting in the wings to exploit similar GM technologies. AquaBounty itself is looking at GM trout, according to its prospectus, and has conducted trials on catfish. Up to six other species of fish – including tilapia and cod – are viewed by biotech companies as ripe for genetic modification, according to experts. Not that Stotish enjoys being the vanguard of a GM food revolution. "It would be far easier to be the third or fourth or fifth [company to bring a GM animal to market]. If you are the first, you attract all of the attention and the burden of attention falls to you. It's a difficult position for a small firm like us." AquaBounty is also battling dire warnings that its chief product threatens the natural food chain. The company's genetic technology ensures that more than 98% of its salmon cannot reproduce, Stotish says. In addition, the eggs it produces (which are all female thus ensuring the GM fish cannot reproduce among themselves) will be sold only to strictly monitored growers operating fish farms under licence from the FDA.
"This biological and physical containment almost certainly guarantees no interaction with wild salmon," Stotish pledged, pointing out that about 95% of the world's salmon is already produced in farms. But Helen Wallace, of the anti-GM group GeneWatch, said she had serious concerns. "AquaBounty admit that they expect more than 1% of their fish to be able to reproduce," Wallace said. "If, as they intend, they end up producing large numbers of eggs, that's a large risk." Escaped GM salmon could "outcompete" its wild counterpart by reproducing earlier and threatening its food supply. Some researchers have suggested that even a small number of escaped GM salmon could cause extinction of wild populations in as little as 40 generations. With potentially weak constitutions, the new salmon might then struggle to adapt to life outside captivity. Food and Water Watch goes as far as to suggest the GM salmon "may only last long enough in the wild to prevent natural populations from reproducing, leading to a total extinction of salmon in open waters". Escapes are not uncommon. In March, nearly 100,000 farmed Atlantic salmon escaped into the wild from just one hole in a net at a UK fish farm. Such concerns take place against the backdrop of a much wider battle between pro-GM groups and an increasingly vocal organic movement. GM crop production is promoted aggressively on the grounds that it can help eliminate global hunger and bring down food prices. Opponents claim the promised GM revolution that saw crops made resistant to potent herbicides – something that could dramatically reduce farmers' spraying time – has resulted in the rise of superweeds across vast tracts of US farmland. Experts said they had been expecting the battle over GM food to move to fish for some time because they are easier to modify. Stotish said his company was focused purely on aquaculture. But GM pork already looks a real possibility. The Enviropig, a trademarked pig that has been genetically modified to excrete less polluting phosphorous in its faeces, has been developed by researchers in Canada. Genetically modified chickens capable of laying eggs containing proteins needed to make cancer-fighting drugs have been created by Scottish scientists. A goat that produces a spider's web protein – paving the way for silk to be farmed – is under development. GM goats have also been raised to produce human breast milk and to deliver a special protein for people whose blood cannot flow smoothly. And then there is the GloFish, a genetically modified fluorescent zebrafish that, according to its sales blurb, would grace any aquarium and comes in three "striking colours" – starfire red, electric green and sunburst orange. But amid the rush to spread GM's reach and scope, at least one government has recently had second thoughts. Muhyiddin Yassin, Malaysia's deputy prime minister, last week announced his government would not be releasing genetically modified male Aedes mosquitoes capable of sterilising female mosquitoes. "We must consider several aspects of the proposed release, including its impact on the environment," Yassin said. "In addition, the release of the mosquitoes must be endorsed by several international organisations." For GM opponents, the U-turn was a cause for celebration, a sign that politicians still accept that the technology carries massive risks. But the ultimate victory in the argument about
genetically modified food comes down to the invisible hand of the market. Both sides agree it is significant that none of the big GM technology companies such as Monsanto is attempting to create GM meat or fish, preferring to focus on more lucrative GM crop production. "The process of genetically modifying animals has been a commercial failure," Wallace said. "Too many scientists and small biotech companies have engineered animals just because they can, without thinking through the technical, economic, marketing, animal welfare, environmental or social issues." Yet Stotish senses opportunity for his fledgling industry. "Once the [GM] technology was adapted for plant systems, the size of that opportunity dwarfed the efforts on the animal side. We've lagged behind." If the FDA gives the green light to GM salmon, expect a frantic game of catch-up. THE RISE OF GM 1980 First biotechnology patent granted: US researchers awarded a patent that allows them to make human insulin from genetically modified bacteria. 1982 US government approves tests to evaluate how genetically engineered bacteria can control frost damage in potatoes and strawberries. 1986 The US Environment Protection Authority approves the first GM crop - a virus-resistant tobacco plant. 1990 The first successful field trial of GM herbicide-tolerant cotton is conducted in the USA. In the same year the first GM dairy cow is created. 1994 The first genetically engineered food product, the Flavr Savr tomato, receives US Food and Drug Administration approval. 2002 Researchers sequence the DNA of rice, the first crop plant to have its genome decoded. 2003 UK approves a GM herbicide-resistant corn used for cattle feed. 2005 Cow genome sequence published. 2006 GM rice approved for human consumption in the US. 2007 Scottish researchers genetically modify chickens to lay eggs capable of producing drugs that fight cancer.
As Private Tutoring Booms, Parents Look at the Returns By PAUL SULLIVAN Published: August 20, 2010 WITH only a few weeks left until school starts, the tutoring business is gearing up. And it is one industry in America that seems immune to recession. More parents are paying for tutors for their children. Spending on tutors is growing at more than 5 percent a year, said Steve Pines, executive director of the Education Industry Association. This is down from yearly growth of 8 to 10 percent in 2007, when the education research firm EduVentures estimated the size of the tutoring industry at $5 billion to $7 billion a year. But it is still strong, given the state of most people‘s personal finances. And Sandi Ayaz, executive director of the National Tutoring Association, said the number of tutors her organization had certified had grown 18 percent in each of the last five years. While tutors once focused on helping children who were falling behind in particular subjects or had a learning disability, they are now being used far more to guide students through particularly tough courses, insure their grades are equal to or above their peers‘ and, in the end, polish a child‘s college application. This costs parents a lot of money, and the question is, What returns should they expect for their investment? And how does that desire mesh with what is right? Before I go further, I want to address the question of fairness, which is ever-present in the world of high-priced tutors. The simple answer is that it is surely not fair that wealthy children can have private tutors when poor children cannot. But many things in life are not fair, and I want to look at tutoring from an investment point of view. Is there any way to measure what parents and children are getting for all this money? What can a tutor reasonably be expected to do? Is this money well spent? SHOPPING AROUND Even with the increase in the use of tutors, parents are not necessarily spending money the way they once did. Some are, of course, since money is still no object when it comes to their children. Yet even in Manhattan, where tutors are particularly popular, plenty of parents are shopping around for less expensive options. ―People have been pulling back for tutors charging $250 to $400 an hour,‖ said Sandy Bass, editor and publisher of Private School Insider, an online newsletter. ―They‘re still using tutors, but they‘re searching around for more reasonably priced help. In Manhattan, $85 to $150 is the acceptable range for reasonably priced.‖
Mr. Pines of the Education Industry Association said he had seen the same reassessment in the rest of the country, where the average rate was $45 to $65 an hour. Parents who once would have had in-home tutors are going to tutoring centers, while some using the centers have cut back on hours or moved to online-only platforms. He said a rising player in this field is TutorVista, an online education company based in Bangalore, India, that charges $99.99 a month for help on an Internet platform. Where access to tutors appears to be drying up is for people with limited means. In the past, the issue was not whether they could afford it, but rather whether they could finance it. And Jeffrey Cohen, the president and chief executive of Sylvan Learning Centers, which operates one of the largest chains of tutoring franchises in the country, said the lack of financing had been a big blow to less wealthy families. ―Programs do exist, but they‘re hard to come by,‖ Mr. Cohen said. ―Prerecession families with a decent credit score could get approved to finance these programs. They could put themselves on a multiyear monthly payment schedule.‖ HELP OR HINDRANCE? Money can‘t buy you love, the song says, but what should it buy? The cardinal sin of tutoring is writing a student‘s college essay. This is the murkiest part of the industry. After all, the first line in the National Tutoring Association‘s ethics code is: ―I understand that my role as a tutor is to never do the student‘s work for him or her.‖ Not surprisingly, people in the industry cringe when the issue is brought up, particularly with online tutoring. ―That‘s where the parent has to play a role of oversight,‖ Mr. Pines said. ―It has to be monitored at home, and I can‘t let Mom and Dad off the hook for that.‖ But the bigger question that springs from this is, How do you make sure the money you‘re spending is benefiting your child? Helping children improve in areas where they are struggling is clearly important. But Ms. Bass said any tutoring should bolster standardized test scores. ―You‘re not going to go from a 550 to an 800 on the SAT, but you can count on a 100-point rise,‖ she said. ―A lot of that is just getting a kid used to taking the test.‖ This has reached its absurd extreme. Ms. Bass said most private schools in New York had started to discount the Early Childhood Admissions Assessment, more commonly called the E.R.B. after the Educational Records Bureau, the company that administers it, because parents hired tutors to coach their 4-year-olds on acing it. While this is one way to spend your money, it may not be the best way to teach children the long-term skills they will need after they get into that top kindergarten. It may also hinder them more than help them.
―I always say be careful in doing this,‖ said Lloyd Thacker, a former college admissions officer and the executive director of the Education Conservancy. ―Not only does it jeopardize your child‘s ‗studenthood‘ — those qualities that make learning happen — but someone finding your way for you and packaging you in the process jeopardizes your ability to be yourself.‖ In other words, hiring a tutor to help a child who is struggling in math is a good use of money. Hiring one so the child does not have to push himself is a bad one. ―In an ideal world, students should realize they can do it themselves,‖ said Mr. Thacker, an admitted opponent of the hyper-tutoring culture. And many of them could, but would parents risk letting them try? HARVARD OR BUST A financier I know who was educated at a trifecta of top institutions — St. Paul‘s School, Yale and Columbia Law — observed that wealthy parents today were paying for tutoring and private school as a forward contract on the Ivy League, with anything less being a disappointment. This was a cynical take, for sure, but it stuck with me: what constitutes success after paying for thousands of hours of tutoring at $100-plus an hour? The argument for this extra attention as a means to create well-rounded students is not convincing, since private tutoring in college tends to be for remedial help. School competition is clearly part of parents‘ thinking, but it‘s not just for college. ―Parents are concerned about how their children rank against their friends, their neighbors, kids in the next town over, the next state over, even the next country over,‖ Mr. Cohen said. On the positive side, for children, tutors can often comfort them and let them talk to someone beyond their parents. ―They can say what they want and that person will translate it to Mom and Dad,‖ Ms. Bass said. ―That‘s what the kid needs because they‘re afraid of letting Mom and Dad down.‖ This therapeutic value is one good use of the money, but so, too, is how it can make a child feel about school. ―The more qualitative measures of success are things like attitude, self-confidence and the willingness to finish homework,‖ Mr. Pines said. ―Parents appreciate when kids can get their homework done without Mom hovering over them.‖ It‘s not Harvard, but it could lead to happiness.
A day in the life of an 80-year-old carer
In 20 years I have saved the state half a million pounds. Yet its
adherence to regulations is a malaise money can't cure
guardian.co.uk, Monday 27 September 2010 12.04 BST
Today Phil has to visit hospital for tests – a difficult undertaking
because she is bedbound and has been now for some 15 years. She is
doubly incontinent and the swan neck deformity which began 20 years
ago in all fingers of both hands has now twisted them to a state of
utter uselessness. Little is yet known about the myalgic
encephalopathy (ME), which she was diagnosed with back in 1986.
Indeed, at that time, the medical profession tried to pretend ME was
all in the minds of their patients – medics never like having to admit
they are stumped.
Because we enjoy the late-night TV, it is not until getting on for 9am
that I am awakened by calls from the next room. I struggle in bleary-
eyed to change incontinence pads and to prepare and feed Phil some
breakfast. She was always a very independent woman, an athlete as
well as an academic, making it particularly galling to be in this state of
utter dependence on others, but she rarely complains. Even eating is a
problem: ME being a muscle disease, Phil cannot chew, so all her food
has to be pureed and then fed to her.
Having been told I have high cholesterol and so might be prone to
strokes, I set in motion the installation of an alarm for Phil to operate.
Her twisted hands cannot use the alarm button supplied and three
months later we are still waiting for the company to come up with a
solution. I did follow things up the other day by asking if they thought
they might be able to supply our needs before we had both died. They
were not amused, neither did they seem concerned.
But, back to today: we buy in care for two hours each morning and
evening. The supplying company is chaotic but the carers are highly
skilled and very caring. Today's carer gives Phil a good wash and
freshen up and, just before she leaves, we ease her into a dressing
gown so that she is more respectable for her journey to hospital.
Paying for all this care has now used up more than half of our joint
savings, although I have estimated saving the state about half a million
pounds during my 20 years of caring in retirement. In London we weregranted £10,000 a year in direct payments for care, but our new borough considers us too rich to need financial help. About a year ago ,when Phil last had a hospital appointment, the men in green when they arrived said they were not licensed to use the hoist to get Phil off the bed and into their carrying equipment. Today, two crews arrive to get Phil down two floors of a very high Georgian house to the front door. That seems to cause them no problem but the initial job of getting her off her bed and into the carrying chair is a different matter. They say they were told there would be a carer present who would use the hoist. Last time they went away without doing anything because they are "not licensed to use hoists". Stalemate once again because I, who am half the size and at least twice the age of any one of them, am proving stubborn too. In the middle of all this the phone rings – it is someone from the ambulance depot who tells me all the rules and regulations. Why, I cannot imagine, but it makes me finally blow my top. The four men in green are so moved by this that they decide to act whatever rules and regulations they may be breaking. With a virago in their midst they clearly won't risk their chances. Forthwith, very smoothly and easily, they lift Phil into the carrying chair and take her on the perilous journey downstairs with her feet sticking well out in front because her knees won't bend. Finally, in the ward, the nurses seem doubtful whether they can find Phil a bed, but after a while she is safely tucked up. There can't be any more problems now can there? Yes of course there can! Back I go by bus across town to get incontinence pads because clearly no one is going to bother to find any from elsewhere in the hospital. Later, I receive the message that the exploratory operation is over: Phil has come round and is ready to return home. No. Cancel that. They cannot get an ambulance till the next day. Neither money nor more legislation will cure this malaise of the health service. It demands a change of attitude: put the patient first and to hell with the regulations.
You can also read