2020-2021 MAHC GRAND ROUNDS PROGRAM COMMITTEE MEMBERS: DR. DAVE MCLINDEN (CO-CHAIR) DR. JESSICA REID (CO-CHAIR)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2020-2021 MAHC Grand Rounds Program Committee Members: Dr. Dave McLinden (Co-Chair) Dr. Jessica Reid (Co-Chair) Dr. Scott Whynot Dr. Allison Small Dr. Khaled Salem Dr. Dave Johnstone Krista Hailstone

All SPC members have signed a COI form. All speakers have been emailed the certification/accreditation requirements for their presentation and have signed a COI and a speaker release form. Each presentation is reviewed by the Education Coordinator prior to its delivery. The coordinator will be looking for any signs of bias including use of brand names and logos. If bias is detected in the presentation the SPC would review it and the speaker would be notified so that the bias can be corrected before the presentation is given. If the bias cannot be corrected or removed the session would be cancelled. If a bias is detected by a planning committee member during the presentation they would question the speaker about it. All reported biases would be reviewed at the next SPC meeting.

Your Scientific Planning Committee has taken the
following precautions for security and confidentiality
purposes:
These sessions are being broadcast but not recorded.
All attendees are placed in a ‘waiting room’, the Education Coordinator acts as a moderator during the
sessions and is required to permit entrance to each attendee. If the moderator does not recognize a
name, she will message them privately to determine if they should actually be attending.
Case presentations have been de-identified as follows:
Intervals have been used for ages.
No specific dates have been used. Only the qualifier ‘early, mid or late’ and the month are indicated.
Patients’ initials (if used) have been altered.
CONFIDENTIALITY REMINDER We all have a responsibility to ensure that any confidential information discussed during a Grand Rounds remains that way. Please ensure you are attending from an appropriate location and that this session can not be overheard by unintended audiences. No recording of any kind (audio, photo, video or other) is permitted.

Participant certificates will be based on the attendance list. Anonymous evaluations will be collected using a survey monkey link which Krista Hailstone will send via email to participants following the session. Please use the “Chat” feature to ask questions or share comments you have To unmute yourself click on this icon found at the bottom left hand corner of your screen. If you are having connectivity issues, try using ‘audio only’ by clicking on this icon to turn your video off

“Maskne” STRATEGIES TO CLARIFY THE DIAGNOSIS… AND THE SKIN!
Objectives
By the end of the program, participants will be able to:
Develop a differential diagnosis for the various skin
disorders that may present as “maskne”
Identify strategies to differentiate between “maskne”
causes
Outline broad treatment options to improve “maskne”
Disclosure of Affiliations, Financial Support, and Mitigating
Bias
Speaker Name: Dr. Kersti Kents
Session Information: “Maskne”. Strategies to Clarify the Diagnosis… and the
Skin!
I have no relationships with for-profit or not-for-profit organizations.
Please note I will be discussing off-label use of some medications, which
will be indicated with an asterisk *
“Maskne”
“Maskne”, or facial rash that is distributed in the location of a face mask, is
not a new phenomenon
It’s incidence has increased since COVID-19 prevention strategies have
mandated mask-wearing
It can cause significant distress to patients, from both a physical discomfort
as well as emotional standpoint
Not all redness or bumps on the face are caused by acne
What are some barriers surrounding the diagnosis and treatment of
“maskne”?
“Maskne” causes
The differential diagnosis of “maskne” includes:
Acne
Rosacea
Perioral dermatitis
Seborrheic dermatitis
Allergic contact dermatitis
Irritant contact dermatitis
Atopic dermatitis (not covered today)
Facial psoriasis (not covered today)Acne Vulgaris
Prevalence in adolescents from 35% to over 90%, predominantly males
Post-adolescent acne more common in females
Patients with acne can experience significant psychological morbidity,
with increased risk of suicide
Delayed treatment can result in scarring, which can be permanent
Comedones are the sine qua non characteristic lesionPathogenesis - acne vulgaris
Inflammatory disorder of the pilosebaceous unit
4 main factors are involved:
Follicular hyperkeratinization
Increased sebum production
Cutibacterium acnes (formerly Propionibacterium acnes) within the follicle
InflammationOther Contributing Factors
Androgens
Stimulate the growth and secretory function of sebaceous glands
External Factors
Soaps, detergents, astringents – poorly washed mask
Repetitive mechanical trauma – poorly fitting mask, overscrubbing face
Acne mechanica or cosmetics – this can be a large component of acne due to masks
Diet
Nurses’ Health Study showed association between acne and intake of milk1
Case-control study of 205 patients showed possible association between more than 3
portions per week of milk and moderate to severe acne 2
No randomized trials have evaluated milk and its relationship to acne
1 Adebamowo CA, Spiegelman D, Danby FW, et al. High school dietary dairy intake and teenage acne. J Am Acad Dermatol 2005; 52:207.
2 Di Landro A, Cazzaniga S, Parazzini F, et al. Family history, body mass index, selected dietary factors, menstrual history, and risk of moderate to severe acne
in adolescents and young adults. J Am Acad Dermatol 2012; 67:1129.Other Contributing Factors
Family History
Stress
Anyone else out there stressed out due to COVID-19?
Receptors for corticotropin releasing hormone, a hormone involved in the stress
response, are present in sebaceous glands 1
Sebaceous gland cells exhibit stronger staining for CRH in acne-involved skin than in
normal or uninvolved skin
Insulin Resistance
May stimulate increased androgen production
Is associated with increased serum levels of insulin-like growth factor, which has been
linked to increased facial sebum excretion 2
1 Ganceviciene R, Graziene V, Fimmel S, Zouboulis CC. Involvement of the corticotropin-releasing hormone system in the pathogenesis of acne vulgaris. Br J
Dermatol 2009; 160:345.
2 Vora S, Ovhal A, Jerajani H, et al. Correlation of facial sebum to serum insulin-like growth factor-1 in patients with acne. Br J Dermatol 2008; 159:990.Clinical Features - acne vulgaris
Comedones are the sine qua non characteristic lesion
Lesions occur most commonly on areas of body with largest, hormonally-
responsive sebaceous glands
Face, neck, chest, upper back, upper arms
Open and closed comedones, inflammatory lesions, scarring, post-
inflammatory hyperpigmentation (most common in skin of colour).
Adult women may have predominant involvement to lower face and
neck, often associated with premenstrual flares
Benefit from hormonal therapiesAcne Lesions Closed Comedos Open Comedos Inflammatory Thiboutot, D., Zaenglein, A. Pathogenesis, clinical manifestations, and diagnosis of acne vulgaris. In: UpToDate, Dellavalle, R (Ed), UpToDate, Waltham, MA, 2020.
Acne Lesions Nodules Hyperpigmentation ?? Thiboutot, D., Zaenglein, A. Pathogenesis, clinical manifestations, and diagnosis of acne vulgaris. In: UpToDate, Dellavalle, R (Ed), UpToDate, Waltham, MA, 2020.
Management - acne vulgaris
New guidelines published in 2016
Asai, Yuka et al. Management of Acne: Canadian clinical practice guideline
CMAJ. 2016 Feb 2;188(2):118-26.
Recommendations made for 3 categories of acne severity:
Comedonal acne
Mild-to-moderate papulopustular acne: inflammatory lesions that are mostly
superficial
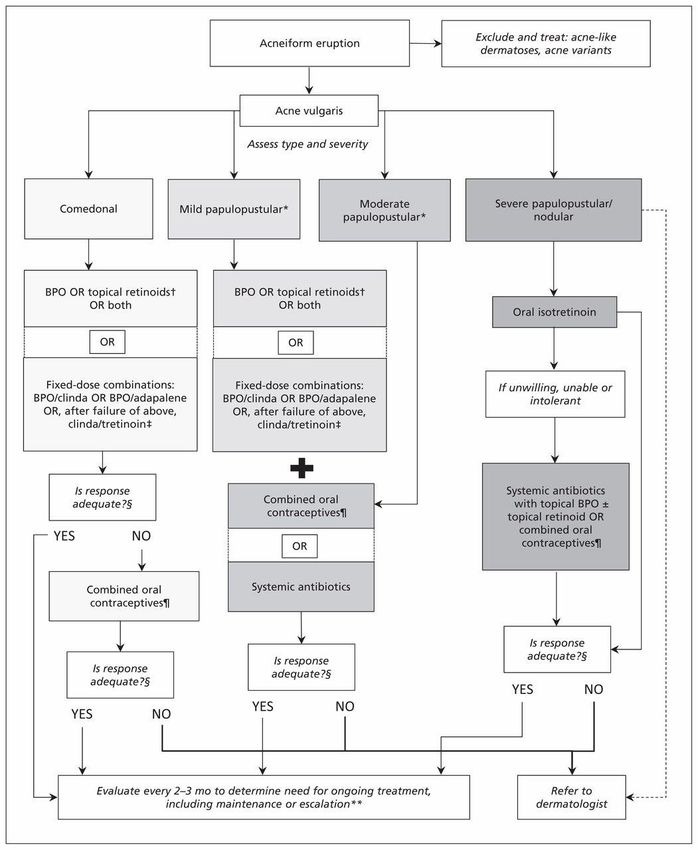
Severe acne: deep pustules and/or nodulesClassification of Acne Asai, Yuka et al. Management of Acne: Canadian clinical practice guideline CMAJ. 2016 Feb 2;188(2):118-26)
Clinical treatment algorithm for acne.
Yuka Asai et al. CMAJ 2016;188:118-126
©2016 by Canadian Medical AssociationManagement - Comedonal Acne
Topical therapies: retinoids, benzoyl peroxide (BPO), and fixed-dose combinations of retinoids with BPO or clindamycin
Creams and lotions are less drying for dry, sensitive skin
Oily skin patients may prefer gels
BPO:
antibacterial, comedolytic, fast onset of action, available OTC, effective towards antibiotic-resistant C Acnes, but can stain hair
and linens
Retinoids:
comedolytic and anti-inflammatory
adapalene and tazarotene are superior to tretinoin for comedonal acne, with tazarotene possibly more irritating than
adapalene1
In women, consider adding combined oral contraceptive
Azaleic acid:
not part of these guidelines, but is mildly comedolytic, antibacterial, anti-inflammatory, and lightens pigmentation
has been shown to improve both inflammatory and non-inflammatory lesions of acne 2
1 Nast A, Dréno B, Bettoli V, et al.; European Dermatology Forum. European evidence-based (S3) guidelines for the treatment of acne. J Eur Acad
Dermatol Venereol 2012;26 Suppl 1:1–29
2 Webster, G. Combination azelaic acid therapy for acne vulgaris. J Am Acad Dermatol 2000; 43:S47-50Management - localized mild to
moderate papulopustular acne
Can start with topical therapies
Recommend any of topical retinoids, BPO or fixed-dose combinations
(clindamycin-tretinoin)
Determine best option by considering type of vehicle, ease of use, cost
If areas of acne not easily accessible to topical therapy (eg. back), consider
adding systemic therapies IN ADDITION to topical treatmentsManagement - extensive moderate
papulopustular acne
Recommend systemic antibiotics IN ADDITION to topical medications already
recommended for localized papulopustular acne
Antibiotic-resistance if antibiotics used on their own
Discourage use of penicillins, macrolides and flouroquinolones as these are used in
other community-acquired infections
Minocycline is associated with increased risk of drug-induced lupus and hepatitis1, as
well as potentially irreversible pigmentation to various tissues (skin, thyroid, nails,
sclera, teeth, conjunctiva, tongue, bone)
Use tetracycline or doxycycline, as “the evidence does not support the conclusion
that the more expensive extended-release preparation is safer than standard
minocycline preparations”1
Re-evaluate at 3-4 months to minimize bacterial resistance2
In women, can consider addition of OCPs to topical medications
1Garner SE, Eady EA, Popescu C, et al. Minocycline for acne vulgaris: efficacy and safety. Cochrane Database Syst Rev 2003;(1):CD002086.
2 Zaenglein et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol 2016;74:945-73Management - severe acne
Oral tretinoin
Prescribing should be done by physicians familiar (ie. Trained and experienced) with
it’s use, monitoring and pregnancy-prevention measures
Oral antibiotics in combination with BPO, with or without topical retinoids
Oral Isotretinoin versus high-dose doxycycline and fixed-dose combo1
Total of 226 subjects with severe facial acne, with 5 or more nodules and 20 or more
inflammatory lesions
“When a 75% reduction of lesions was considered, fixed combination of
adapalene/BPO plus doxycycline (200mg) demonstrated a comparable benefit/risk
to isotretinoin over 20 weeks in the treatment of severe acne with nodules.”2
For women, consider OCPs
1 Tan J, Humphrey S, Vender R, et al, the POWER Study Group. A treatment for severe nodular acne: a randomized investigator-blinded, controlled, non-inferiority trial
comparing fixed-dose Adapalene/BPO plus doxycycline vs oral isotretinoin. Br J Dermatol 2014, 171(6):1508-16
2 Layton A. Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris. Dermatol Clin 34 (2016) 147-157Spironolactone*
Post-adolescent acne can be
unresponsive to traditional therapy in
more than 80% of cases, and some
patients experience relapse following
isotretinoin (up to 30% of cases)1
Acts by reducing the circulating
testosterone via increased liver
clearance
Competes with dihydrotestosterone for
cutaneous androgen receptors which
reduces testosterone binding
Predominance of inflammatory papules
located a jawline, chin and cheeks
1 Kim g, Del Rosoo JQ. Oral spironolactone in post-teenage female patients with Layton A. Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris.
acne vulgaris practical considerations for the clinical based on current data and Dermatol Clin 34 (2016) 147-157Rosacea
Usually in patients with lightly pigmented skin (skin phototypes I and II)
Prevalence in fair-skinned people range from 1-10%
Typically over age of 30
Women > men (except when phymatous skin changes)
When occurs in adolescents, often mistaken for acne vulgaris, and can co-
existPathogenesis - rosacea
Pathogenesis is not well understood
Proposed contributing factors include:
Abnormalities in innate immunity
Production of abnormal cathelicidin peptides that have vasoactive and inflammatory properties 1
Studies involving injection of mouse skin with cathelicidin peptides from patients with rosacea lead to
inflammation and vascular dilatation 2
Ultraviolet damage
UVB radiation can stimulate cutaneous angiogenesis in mice, and induce secretion of vascular
endothelial growth factor and fibroblast growth factor from keratinocytes 3
Vascular dysfunction
Increased blood flow has been detected in the skin of some patients 4
Skin microorganisms fostering inflammatory reactions
1 Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci 2009; 55:77.
2 Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med 2007; 13:975.
3 Brauchle M, Funk JO, Kind P, Werner S. Ultraviolet B and H2O2 are potent inducers of vascular endothelial growth factor expression in cultured keratinocytes. J Biol Chem 1996; 271:21793.
4 Sibenge S, Gawkrodger DJ. Rosacea: a study of clinical patterns, blood flow, and the role of Demodex folliculorum. J Am Acad Dermatol 1992; 26:590.Role of microorganisms
Demodex folliculorum
Saprophytic mite that is found in sebaceous follicles
Increased density in patients with rosacea
Meta-analysis of case-control studies showed statistically significant association
between Demodex infestation and rosacea
Degree of infestation more important than rate of infestation1
Bacillus olenorium
Bacterium isolated from Demodex mite
Study found antigens from B. oleronius stimulated proliferation of peripheral blood
mononuclear cells from 16 out of 22 patients with rosacea, versus only 5 out of 17
patients without rosacea2
1 Zhao YE, Wu LP, Peng Y, Cheng H. Retrospective analysis of the association between Demodex infestation and rosacea. Arch Dermatol 2010; 146:896.
2 Lacey N, Delaney S, Kavanagh K, Powell FC. Mite-related bacterial antigens stimulate inflammatory cells in rosacea. Br J Dermatol 2007; 157:474.Exacerbating factors Exposure to extremes of temperature Spicy foods Sun exposure Alcohol Exercise Sensitive skin to topical applications Emotions: anger, embarrassment Drugs: nicotinic acid and vasodilators
Clinical Features - Rosacea
We are all familiar with the 2002 National Rosacea Society’s standard
classification system
4 distinct subtypes of rosacea
Erythematotelangectatic
Papulopustular
Phymatous
Ocular
Increasing understanding of pathophysiology of rosacea has encouraged
modification to this classificationErythematotelangectatic
www.rosacea.orgPapulopustular
www.rosacea.orgPhymatous
www.rosacea.orgOcular rosacea
Lid margin telangectasias
Interpalpebral conjunctival
injection
“Honey crust” and cylindrical
collarette accumulation at the
base of lashes
Irregular lid margin
Gallo RL et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee.
J Am Acad Dermatol. 2018 Jan;78(1):148-155New classification recommendation
Global Rosacea Consensus (ROSCO) Panel recommends a phenotype-
based approach to diagnosis and classification of rosacea
Although rosacea’s various phenotypes may appear in different
combinations and at different times, they may all be manifestations of the
same continuum
Describes clinical features of rosacea
Flushing and erythema may progress to papules and pustules and phymas
Treating papules and pustules may not address flushing
Divided into diagnostic, major, and secondary (or minor) phenotypes
Requires at least 1 diagnostic or 2 major phenotypesROSCO panel recommendations Gallo RL et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018 Jan;78(1):148-155
Management - rosacea
There is no cure, only symptomatic management
Not all characteristics of rosacea respond to same treatments
Pharmacologic agents, in combination with medical devices, result in
better results than either treatment alone
Goal of treatment is to relieve acute flares with rapid-acting treatments
and maintain results with lifestyle modification and prolonged combination
therapy
Avoidance of triggers (especially sun exposure)
Gentle skin care with frequent moisturizationManagement - rosacea- erythema
Brimonidine tartrate gel 0.33%
Alpha-2 adrenergic receptor agonist
Reverses skin vasodilation
Results within 30 minutes
Can have transient rebound erythema
Oxymetazolone*
Potent alpha-1 and partial alpha-2 receptor agonist
Case-reports of efficacy on facial erythema (using nasal solution applied to skin)
A 1% cream is now FDA approved, but not available in CanadaManagement - rosacea - PPR
Metronidazole
Antimicrobial, anti-inflammatory, antioxidant
Used BID, however studies do suggest once daily dosing is equivalent 1
Improvement in 2-4 weeks, with full results over 8-9 weeks of treatment
Relapses often occur when discontinued, may require long-term treatment
Azelaic acid
Naturally occurring dicarboxylic acid with anti-inflammatory and antioxidative properties
Mechanism not well understood
Available as 20% cream or lotion, or 15% foam or gel
Initial improvement within first few weeks, full results after 12-15 weeks
Package insert suggests BID, but randomized trial of 72 patients showed no difference with once daily application 2
May be more effective than metronidazole 3
1 Dahl MV, Jarratt M, Kaplan D, et al. Once-daily topical metronidazole cream formulations in the treatment of the papules and pustules of rosacea. J Am Acad
Dermatol 2001; 45:723.
2 Thiboutot DM, Fleischer AB Jr, Del Rosso JQ, Graupe K. Azelaic acid 15% gel once daily versus twice daily in papulopustular rosacea. J Drugs Dermatol 2008; 7:541.
3 Elewski BE, Fleischer AB Jr, Pariser DM. A comparison of 15% azelaic acid gel and 0.75% metronidazole gel in the topical treatment of papulopustular rosacea:
results of a randomized trial. Arch Dermatol 2003; 139:1444.Management - rosacea - PPR
Topical ivermectin
Anti-inflammatory and antiparasitic
Available as a 1% cream
Applied once daily as thin layer to affected areas
Has been shown to be safe and effective for up to 52 weeks of use
16-week randomized trial compared ivermectin once daily to metronidazole 0.75% cream
in 962 adults with PPR 1
Topical ivermectin was more effective for reducing inflammatory lesions
Longer remissions
Metronidazole is less expensive
In patients with sensitive skin, try metronidazole or ivermectin (azelaic acid greater irritant)
1 Taieb A, Ortonne JP, Ruzicka T, et al. Superiority of ivermectin 1% cream over metronidazole 0·75% cream in treating inflammatory lesions of rosacea: a
randomized, investigator-blinded trial. Br J Dermatol 2015; 172:1103Management - rosacea - systemic
Modified-release Doxycycline 40mg once daily
Anti-inflammatory effects with sub-antimicrobial dosing
Immediate release of 30mg, delayed release of 10mgOptimal doxycycline dosing
Del Rosso JQ, Sclessinger J, Werschler P. Comparison of antiinflammatory dose
doxycycline versus doxycycline 100mg in the treamtent of rosacea. J Drugs
Dermatol. 2008;7(6):573-576
Randomized, double-blind trial
All patients used metronidazole gel 1%
Either doxycycline 100mg* or 40mg delayed release over 16 weeks
No statistically significant difference in efficacy
Increased side effects in higher dose group (nausea, vomiting, diarrhea, abdominal
pain)
May choose to start at higher dose of doxy (50-100mg BID for 4-12 weeks) to
rapidly decrease inflammation, then maintain on 40mg daily
For flare-ups, can prescribe short-courses (10 days) of higher-dose doxyManagement - rosacea
Oral isotretinoin* reserved for severe cases
Reduces size of sebaceous glands and sebum production
Has anti-inflammatory, immunomodulatory, and antineoplastic properties
Has also been used for recalcitrant rosacea with relapses
Continuous microdose isotretinoinLasers and light treatments
Pulsed dye laser
Wavelengths correspond with oxyhemoglobin absorption peak, thus targets superficial
vessels
Improves erythema and telangectasias as well as associated symptoms
Intense pulsed light
Able to target deep vessels, as well as large areas of telangectasia, erythema, and flushing
Requires clinical expertise
Systems provide large spot size which makes treatments faster and more comfortable
CO2 laser and erbium:yttrium-aluminium-garnet laser (Er:YAG)
For rhinophyma
Other surgical techniques have been shown to improve disfigurementPerioral (Periorificial) Dermatitis (POD)
Occurs worldwide in patients of all racial and ethnic backgrounds
Majority are female, aged 16-45
Can occur in children, even infants as young as 3 months of age
Usually considered a benign and self-limiting disorder
It can resolve in a few months without treatment, or can persist for several
yearsPathogenesis - POD
Not well understood
Patients often have atopy and deficiencies in skin barrier function, but the
role of these has not been established
There are often reports of topical corticosteroid (TCS) use
Rash seems to improve initially with TCS, but then recurs or worsens with
continued use or attempts to stop the TCS
Can be due to inhaled steroids, oral steroids, or from application of TCS to other
family members or pets without cleansing the skin afterwards
Appears to be a connection with more potent TCS formulations 1
Skin biopsy shows perivascular chronic inflammation, similar to rosacea
1. Wilkinson DS, Kirton V, Wilkinson JD. Perioral dermatitis: a 12-year review. Br J Dermatol. 1979;101(3):245.Clinical Features - POD
Classic:
Multiple, 1-2mm erythematous papules, papulovesicles, or papulopustules with
or without mild scale
There can also be features of a mild atopic dermatitis as well, and this can be
the more prominent feature
Locations:
Perioral region, with sparing of the vermillion border
Periorbital and perinasal areas
Less often to cheeks, chin, forehead and neck (steroid-induced rosacea – with
telangiectasia)
May describe burning or stinging sensations, or asymptomaticClassic POD https://dermnetnz.org/topics/periorificial-dermatitis-images/
Clinical Features - POD
Granulomatous
Typically occurs in pre-pubescent children
Numerous small, flesh-coloured, yellow-brown or red-brown inflammatory
papules in the perinasal, perioral or periocular areas
Pustules and vesicles usually absentGranulomatous POD https://www.semanticscholar.org/paper/Facial-granulomatous-periorificial- http://www.pcds.org.uk/clinical-guidance/childhood-granulomatous-periorificial- dermatitis-in-a-Zaouak/bcd74257a5275752dee44ff20462fdd575e0b36f dermatitis-syn.-facial-afro-caribbean
Management - POD
Zero therapy
Elimination of corticosteroids and irritants
Includes skin care products and cosmetics
Supported by the fact that placebo-treated patients in randomized controlled
trials have improved within 2-3 months without active therapy1
Stopping the steroid can result in a flare – Hold the course!!
Tapering the frequency of application or the strength of the steroid is of unproven
benefit
1 Schwarz T, Kreiselmaier I, Bieber T, et al. A randomized, double-blind, vehicle-controlled study of 1% pimecrolimus cream in adult patients with perioral dermatitis.
J Am Acad Dermatol 2008; 59:34.Management - POD - mild
Topical calcineurin inhibitors*
Tacrolimus (ointment) and pimecrolimus (cream), use BID
Improvement within 1 month of use
FDA boxed warning on topical CNI due to concerns about association with malignancies
(lymphoma, NMSC)
“Available data on lymphoma following TCI use were inconsistent and insufficient to draw a
conclusion about the causal role of TCIs. We found no evidence indicating that melanoma or
nonmelanoma skin cancer is associated with TCI use.” 1
Randomized trial (pimecrolimus versus vehicle cream) 2
124 adults, treated for 4 weeks
50% reduction in disease severity score in 40% of treated patients after 8 days, versus 11% of those
using placebo. Those previously on topical steroid responded best. At day 29, disease severity scores
were similar in both groups.
Post-treatment flares did not occur after stopping pimecrolimus
1. Tennis P et al. Evaluation of cancer risk related to atopic dermatitis and use of topical calcineurin inhibitors. British Journal of Dermatology 2011; 165: 465
2. Schwarz T, Kreiselmaier I, Bieber T, et al. A randomized, double-blind, vehicle-controlled study of 1% pimecrolimus cream in adult patients with perioral
dermatitis. J Am Acad Dermatol 2008; 59:34.Management - POD - mild
Topical metronidazole*
1% gel is covered on provincial drug plan
Use BID for at least 8 weeks, but may require longer treatment for complete
clearance
Can discontinue treatment upon resolution of PODManagement - POD - Mod to Severe
Oral tetracyclines*
Mechanism of how these improve POD is unknown, ?secondary to anti-inflammatory
mechanisms
Tetracycline 250-500mg BID
Doxycycline 50-100mg BID or 100mg daily
Minocycline 50-100mg BID or 100mg daily
No randomized trials of doxycycline or minocycline, recommendations are
extrapolated from tetracycline studies1
Can consider sub-antimicrobial dosage
If cannot tolerate tetracycline, can use macrolide (erythromycin 500mg BID)
Course of antibiotics generally 8 weeks in duration
1. Reichenberg, J. Perioral (periorificial) dermatitis. In: UpToDate, Callen, J (Ed), UpToDate, Waltham, MA, 2020.Management - POD - Alternatives
Topical ivermectin*
No randomized trials have studied it
Works well in rosacea
Topical azelaic acid*
Open studies have shown benefit
Can work in rosacea
Low-dose oral isotretinoin*
Case reports in refractory granulomatous POD
Recurrence is common, and if occurs, can resume previous treatment
modalitiesSeborrheic Dermatitis (SD)
Chronic, relapsing, and usually mild form of dermatitis
Can affect infants (first peak between 2 weeks and 12 months of age) and
adults (second peak in the 3rd and 4th decade)
Men more affected than women
Has been associated with HIV infection, Parkinson’s disease, use of
neuroleptic medicationsPathogenesis - SD
The cause is not known
Sebaceous glands appear to be necessary for the development of SD, but
it is not a disease of these glands
Malassezia (fungi) is lipid-dependent, and thrives at the sites with
predilection for SD
Studies have not found higher density of Malassezia of affected patients
Most effective treatments of SD have antifungal activity
But can be due to the anti-inflammatory effects of azoles1
? Host response to Malassezia or its byproducts
1. Paulino LC, New perspectives on dandruff and seborrheic dermatitis: lessons we learned from bacterial and fungal skin microbiota. Eur J Dermatol. 2017;27(S1):4.
2. Faergemann J et al. Seborrhoeic dermatitis and Pityrosporum (Malassezia) folliculitis: characterization of inflammatory cells and mediators in the skin by immunohistochemistry.
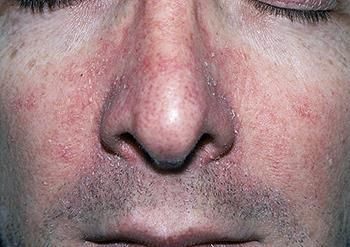
Br J Dermatol. 2001;144(3):549.Clinical Features - SD
Scalp: dandruff to patchy-orange to pink plaques covered with yellow, greasy scales, can extend behind ears
Face:
Salmon-pink, thin, scaly, ill-defined plaques
Forehead below hairline, eyebrows, glabella, nasolabial folds
Can also extend to cheeks
Beard and mustache area in men with facial hair
Periocular: blepharitis
Trunk: 5 patterns described:
Intertrigo: moist, erythematous (axillae, inframammary folds, umbilicus, gentocrural areas)
Petaloid pattern: fine scale, thin plaques to sternum or interscapular area
Annular or arcurate: round to oval plaques, fine scale, central clearing
Pityriasiform: mimics pityriasis rosea, oval, scaly lesions along skin-tension lines
Psoriasiform: larger, red plaques with thicker scaleClinical Features - SD
https://dermnetnz.org/topics/seborrhoeic-dermatitis/ Sasseville, D. Seborrheic dermatitis in adolescents and adults. In: UpToDate,
Fowler, J (Ed), UpToDate, Waltham, MA, 2020.Clinical Features - SD
https://dermnetnz.org/topics/seborrhoeic-dermatitis/Management - SD
Goal is to reduce symptoms and clear visible signs of the disease
Chronic condition, so repeated or long-term maintenance treatment often required
Topical Antifungals
Ketoconazole 2% BID, other azoles, ciclopirox
Decrease Malassezia furfur population, also anti-inflammatory
Topical anti-inflammatory agents
Topical corticosteroids
Topical calcineurin inhibitors*
Topical crisaborole (Eucrisa)* - case report 1
Selenium sulfide shampoo (antifungal), zinc pyrithione (antibacterial and antifungal), coal
tar (keratolytic), salicylic acid (keratolytic)
1. Liu, D et al. Chronic nasolabial fold seborrheic dermatitis successfully controlled with crisaborole. JDD, 2018 May; 17(5) 577.Management - SD
Oral antifungals
Limited evidence
Can consider if multiple body sites or for recalcitrant disease
Itraconazole, ketoconazole, fluconazole, terbinafine
Prevention of relapse
Not well studied for facial SD
Can consider using antifungal cream or shampoo intermittentlyAllergic Contact Dermatitis (ACD)
Delayed (type IV) hypersensitivity reaction which occurs after contact with a particular
substance
Reaction occurs 48-72 hours after re-exposure to offending agent
Rash lasts 2-4 weeks
Common allergens related to ”maskne” includes:
Formaldehyde: commercial masks can be pretreated to disinfect them, also in cosmetics and skin
care products
Quaternium-15: cosmetics and skin care products
Fragrances: in harsh laundry products, used to clean reusable masks, skin care, cosmetics
Products used on the scalp/hair can run down across face to cause dermatitis
Products used on hands can be transferred to face with touching
Think about aerosolized allergens (spray paint, scented candles, perfumes, occupational)Clinical Features - ACD
Well-demarcated
However, can spread beyond the area touched by allergen
Intensely pruritic
Erythematous, indurated, scaly plaques
In severe cases, can see vesicles and bullae
Edema where skin is thin (eyes, lips)
As it resolves, skin becomes more dry and scaly
Chronic: dry, scaly, thicker skin, with lichenification and fissuringClinical Features - ACD Weston, W., Howe, W. Overview of dermatitis (eczema). In: UpToDate, https://dermnetnz.org/topics/contact-allergic-dermatitis-of-the-face-images/ Dellavalle, R (Ed), UpToDate, Waltham, MA, 2020.
Management - ACD
Requires a multipronged approach
Identify and avoid the offending agent (patch testing)
Alternatives to offending products
American Contact Dermatitis Society (requires membership)
Treatment of skin inflammation
Restoration of the skin barrier
Emollient creams
Skin protection
Barrier creams, emollient creamsManagement - ACD
Topical corticosteroids
Low to medium potency, once or twice daily for 1-2 weeks (for face)
Topical calcineurin inhibitors*
Consider topical crisaborole* (Eucrisa)1
Systemic corticosteroids
If over 20% BSA involved, or if acute ACD involving face, hands, feet or genitalia and
want fast improvement
Phototherapy
Narrowband UVB
Systemic immunosuppressive agents*
1. Lynde, C et al. Use of topical crisaborole for treating dermatitis in a variety of dermatology settings. Supplement to Skin Therapy Letter, 2020 Jun; 25(3)Irritant Contact Dermatitis (ICD)
Most common form of contact dermatitis
Due to exposure to substances that cause physical, mechanical, or
chemical irritation of skin
Results from direct cytotoxic effects of irritants
It is not immune mediated
Influenced by 1:
Physical and chemical properties of the irritant
Host-related susceptibility factors
Environmental factors
1. Goldner, R., Fransway, A. Irritant contact dermatitis in adults. In: UpToDate, Fowler, J (Ed), UpToDate, Waltham, MA, 2020.Pathogenesis - ICD
Not completely understood, but multiple mechanisms are involved 1,2:
Disruption of epidermal barrier
By occlusion or chemical or physical irritants (poor-fitting mask, makeup under mask)
Leads to increased cell permeability and transepidermal water loss
Damage of keratinocyte cell membranes
Cytotoxic effect on keratinocytes
Cytokine release from keratinocytes
Sodium lauryl sulfate causes disruption on epidermal barrier, induces release of
proinflammatory cytokines
Activation of innate immunity
Increased humidity and high temperatures under a mask can increase the
penetration of irritants
1. Jakasa I, Thyssen JP, Kezic S . The role of skin barrier in occupational contact dermatitis. Exp Dermatol. 2018;27(8):909.
2. Smith HR, Basketter DA, McFadden. Irritant dermatitis, irritancy and its role in allergic contact dermatitis. JP Clin Exp Dermatol. 2002;27(2):138.Clinical Features - ICD
Usually confined to the site of contact with irritant… initially.
Can spread if prolonged exposure, but less likely than compared to ACD
Ranges from skin dryness and erythema to acute or chronic eczematous
dermatitis or even chemical burns.
Acute ICD:
Erythema, edema, vesicles, bullae, oozing
Burning, stinging, or pain
Chronic ICD:
Erythema, scaling, lichenification, fissuringClinical Features - ICD Goldner, R., Fransway, A. Irritant contact dermatitis in adults. In: UpToDate, https://dermnetnz.org/topics/lip-lickers-dermatitis/ Fowler, J (Ed), UpToDate, Waltham, MA, 2020.
Management - ICD
Almost the same as for ACD, except the use of topical calcineurin
inhibitors are not used (they have not been proven effective, and in some
studies were found to be irritants). 1
Consider topical crisaborole* (Eucrisa)2
Antibiotics for secondary infection
Polysporin can cause irritation, and sometimes allergy, in patients, so tell
them to use plain Vaseline instead.
Removal of irritant results in good prognosis
Improved barrier function in 4 weeks
Skin hyperreactivity can persist for 10 weeks
1. Clemmensen A, et al. Applicability of an exaggerated forearm wash test for efficacy testing of two corticosteroids, tacrolimus and glycerol, in topical formulations
against skin irritation induced by two different irritants. Skin Res Technol. 2011 Feb;17(1):56-62. Epub 2010 Aug 16.
2. Lynde, C et al. Use of topical crisaborole for treating dermatitis in a variety of dermatology settings. Supplement to Skin Therapy Letter, 2020 Jun; 25(3)How to tell all these apart?
Acne:
Look for comedones
Beware as perioral dermatitis and rosacea can coexist
Rosacea:
Look for the telangectasia and centrofacial erythema
Ask about triggers for flushing
Papules and pustules have predilection for cheeks rather than perioral sites
Minimal to no scale
Perioral dermatitis:
Sparing of the vermillion border
Can co-exist with atopic dermatitisHow to tell all these apart?
Seborrheic dermatitis:
Small papules are not typical
Perioral distribution is unusual
Look for it elsewhere: scalp, eyebrows, nasolabial folds and chest
Allergic contact dermatitis:
Distribution is at sites of contact, but can spread beyond area of allergen contact
Intense pruritis
Scale is prominent, especially as it starts to clear
Lesions do not improve with antibiotic therapy
Irritant contact dermatitis:
Not as itchy as ACD, but burning sensation (like POD)
Less scale than ACDA simple approach to divide and
conquer
Consider dividing ”maskne” rash into two broad categories:
1) Rash with papules and pustules
2) Rash with erythematous patches with scale, but no bumpsPapules and Pustules
Consider acne, rosacea and perioral dermatitis
Bland skin care/ Zero therapy
Avoid topical corticosteroids
Consider trial of a tetracycline
Consider topical calcineurin inhibitors
Consider topical ivermectin
Consider azaleic acid
* Note that any of these treatments may be off-label depending on what you
are treating. See previous slides for details. *Erythematous patches with scale (no
bumps)
Consider seborrheic dermatitis, allergic and irritant contact dermatitis
Bland skin care and Zero therapy (can’t hurt!)
Consider topical corticosteroids
Consider topical antifungals
Consider topical crisaborole (Eucrisa)1,2
Patch testing
* Note that any of these treatments may be off-label depending on what you
are treating. See previous slides for details. *
1. Lynde, C et al. Use of topical crisaborole for treating dermatitis in a variety of dermatology settings. Supplement to Skin Therapy Letter, 2020 Jun; 25(3)
2. Liu, D et al. Chronic nasolabial fold seborrheic dermatitis successfully controlled with crisaborole. JDD, 2018 May; 17(5) 577.You can also read