2020: The Year of the Respiratory Viruses A Primer on Influenza and COVID-19 - Marilyn N. Bulloch PharmD, BCPS, FCCM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2020: The Year of the Respiratory
Viruses
A Primer on Influenza and COVID-19
Marilyn N. Bulloch PharmD, BCPS, FCCM
Associate Clinical Professor and
Director of Strategic Operations
Harrison School of Pharmacy
Auburn University
Objectives • Review the pathophysiology of influenza and COVID-19 • Compare and contrast symptoms of influenza and COVID-19 • Describe pharmacologic options for the treatment and prevention of influenza • Identify treatment strategies for patients diagnosed with COVID-19 • Discuss pipeline agents being developed for the prevention and/or treatment of influenza and/or COVID-19
Disclosures
• Speaker’s Bureau - Xofluza (Baloxavir)
• Pharmacy Times – contributor
• PowerPak – author (sleep medicine)
None of these disclosures will impact the
content of my presentation today
Glenn Ridenour MD, Infectious Disease
Specialist
Charleston, West Virginia
A Brief History of Influenza
1st (Documented) Pandemic Advance in Lab Research Reason for
Earlier pandemics • 1931 – discovery that influenza can Pandemics
are likely, but were grow in eggs
not recognized or • 1932 – human influenza isolated Identified
documented for • 1935 – 1st egg-based vaccine
historic purposes developed Antigenic shift
studied
1173 1580 1700’s 1930’s 1940’s 1950’s
Initial Recognition Term “Influenza” Growth of Knowledge
Influenza as a disease is Coined • Vaccine given to U.S military
known to be at least 6,000 members during WWII
years old, but was first • 1946 – discovery of antigenic drift
classified as a disease in
the 12th century
http://www.medicalecology.org/diseases/influenza/influenza.htm#sect2.1 (Accessed 11 Mar 2015)
Shope RE. Public Health Reports. 1958;73:165-179
Potter CW. J Applied Microbiol. 2001;91:572-579
Kilbourne ED. History of Vaccine Development.
How Influenza is
Named
Antigenic Type
•A, B, or C
Host of Origin
•I.E. Swine, Chicken, Equine, ect
•No host of origin given if human origin
City of Geographic Origin
Strain Number
•Unique
Year of Isolation
For Influenza A strains
•Hemagglutinin and neuraminidase description in parentheses
•I.E. H3N2
http://www.cdc.gov/flu/about/viruses/types.htm
Source: www.medicalecology.com
2019-20 Flu Season Burden
39-56 Million Influenza 410,000-740,000 24,000-62,000 Deaths
18-26 Million Medical Visits
Illnesses Hospitalizations
https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm
Source: Cruz D. How does the flu change over time? http://spotlight.vitals.com/2015/01/how-does-the-flu-change-over-time/ (Accessed 24 Mar 2015)
History of COVID-19 Photo courtesy of Creative Commons CCO: https://www.researchgate.net/figure/Timeline-showing-the-most-important-events-occurred-in-the-world-from-novel- coronavirus_fig2_342840258
Which is a symptom of COVID-19, but not a symptom of Influenza? A. Fever B. Nausea C. Body aches D. Loss of smell
Symptoms of Influenza
Symptoms vary WIDELY
Headache by patient
Fever (Usually high)
Chills
Patients may not have all or even
Congestion or runny nose most of the known symptoms
Cough (usually non-productive)
Sore throat
Symptoms appear 1-4 days after
Shortness of breath or
exposure
difficulty breathing
People are contagious ~ 1 day
Fatigue before symptoms appear
Muscle or body aches
Most contagious in first 3-4 days, but remain
contagious ~ 7 days (up to 2 weeks in
children and immunocompromised
GI symptoms more common in
Nausea
Vomiting children and with Influenza B
Diarrhea
Cough and fatigue may last > 2 weeks
Symptoms may have abrupt onset
https://www.cdc.gov/flu/symptoms/symptoms.htmSymptoms of COVID-19
Symptoms vary WIDELY by
Headache patient
Fever (may be low grade)
Chills Patients may not have all or even most
Loss of smell of the known symptoms
Congestion or runny nose Symptoms vary even among those in
the same household
Cough
Loss of taste
Sore throat
Symptoms appear 2-14 days after
Shortness of breath or exposure (average 5 days)
difficulty breathing
97.5% of people who develop symptoms
develop them within 11.5 days of exposure
Fatigue
Muscle or body aches
Symptom severity and duration vary widely
by patient
People are contagious ~ 2 days before
Nausea
symptoms appear and remain for 10 days
Vomiting
Diarrhea
Some patients never exhibit any signs or symptoms
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html
Luaer et al. Ann Intern Med. 2020COVID-19 and Hypercoagulability
Proposed Pathophysiology Treatment
Some patients Laboratory Abnormalities Complications
develop • Inpatient DVT
• DVT/PE
• Largely unknown at this time prophylaxis
hypercoagulable • Thrombocytopenia (mild) • Microvascular clots in toes
• May be due to inflammatory • Unclear if treatment
state • Increased D-dimer**** • Catheter clotting
activation of coagulation dose anticoagulation
• Increased ferritin and fibrinogen • STEMI
pathway. should be used.
• Prolonged PT • Large vessel stroke.
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html#clinical-management-treatment%3C
https://www.covid19treatmentguidelines.nih.gov/adjunctive-therapy/antithrombotic-therapy/Patients at High Risk of
Complications
Influenza COVID-19
< 2 weeks post-
Age ≥ 65 years Age < 2 years Pregnancy
partum Increaseing Age Cancer CKD
Diabetes and other Chronic lung
Immunocompromised
endocrine disorders disease
COPD Immunocompromised BMI ≥ 30
Hematologic
Heart Disease Neurologic Diseases (I.E.
Asthma Sickle Cell
and Stroke Conditions
Disease) Serious Heart
Sickle Cell Disease Diabetes
Disease
Children on
Kideny Disease Liver disease BMI ≥ 40 long-term
salicylates
American
Alaskan Natives LTC facilities
Indians
https://www.cdc.gov/flu/highrisk/index.htm
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.htmlPatients Who May Be at Increased
Risk for COVID-19 Complications
Moderate-Severe Cerebrovascular
Cystic Fibrosis Hypertension Immunocompromised
Asthma Disease
Steroid or other
Neurologic Conditions
immunosuppressive Liver Disease Pregnancy Pulmonary Fibrosis
(e.g. dementia)
medications
Children with
congenital
Smokers Thalassemia Type 1 Diabetes cardiovascular, Type A Blood Type
neurologic, genetic, or
metabolic conditions
More to come
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/evidence-table.htmlPotential Complications of COVID-19
Pneumonia
Respiratory
(often ARDS
failure
bilateral)
Cardic events
Multiple-organ
Sepsis (e.g. MI,
failure
Stroke)
Worseing of Secondary
chronic Inflammation bacteria
disease infections
https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm#anchor_1595599580An ounce of prevention gives a glimmer of hope
Flu Vaccine Effectiveness
Overall Influenza Vaccine Vaccine Effectiveness 2019-20
Effectiveness 2010-2020 Flu Season
80% 50% 39% 37% 42% 37%
60% 48% 52% 49% 47% 60% 40% 33% 35%
39% 38% 40% 30%
40% 29% 20%
19%
20% 10%
0% 0%
All 6 mos-8 9-17 18-49 50-64 65 years
years years years years and
older
Vaccine Effectiveness for Circulating Strains 2019-20 Flu Season
60% 44% 45% 39%
38% 39% 38% 42%
40% 31% 29% 28%
22%
20% 4%
0%
All 6 mos - 8 years 9-17 years 18-49 years 50-64 years 65 years and older
H1N1 B/Victoria
https://www.cdc.gov/flu/vaccines-work/2019-2020.html
https://www.cdc.gov/flu/vaccines-work/effectiveness-studies.htmVaccine Prevented Burdens
2017-18 Flu Season 2016-17 Flu Season
Averted Averted Medical Averted Averted Averted Flu Averted Medical Averted Averted
Age Group Age Group
Flu Cases Visits Hospitalizations Deaths Cases Visits Hospitalizations Deaths
All 6,160,213 3,180,360 90,904 5,747 All 5,283,410 2,651,757 72,303 5,217
0-4 years 1,721,215 1,153,214 15,139 68 0-4 years 615,907 412,658 4,294 32
5-17 years 1,151,025 598,533 4,275 110 5-17 years 2,234,364 1,161,869 6,126 43
18-49 years 1,044,837 386,590 6,534 226 18-49 years 528,273 195,461 2,965 78
50-64 years 1,647,176 708,286 16,792 808 50-64 years 1,422,737 611,777 15,088 722
≥ 65 years 595,961 333,738 48,163 4,536 ≥ 65 years 482,130 269,993 43,830 4,341
2015-16 Flu Season 2014-15 Flu Season
Averted Averted Medical Averted Averted Averted Flu Averted Medical Averted Averted
Age Group Age Group
Flu Cases Visits Hospitalizations Deaths Cases Visits Hospitalizations Deaths
All 5,348,579 2,655,362 69,506 6,413 All 1,408,009 702,400 38,776 3,657
0-4 years 1,059,354 709,767 7,385 87 0-4 years 140,406 94,072 979 17
5-17 years 1,521,776 791,324 4,173 32 5-17 years 357,179 185,733 979 23
18-49 years 1,579,966 584,588 8,868 295 18-49 years 247,680 91,642 1,390 28
50-64 years 733,122 315,243 7,775 362 50-64 years 309,102 132,914 3,278 203
≥ 65 years 454,360 254,442 41,305 5,637 ≥ 65 years 353,641 198,039 32,149 3,386
https://www.cdc.gov/flu/vaccines-work/burden-averted.htm2020-21 Influenza Vaccine
Components
A/Guangdong-
A/Hawaii/70/2019(H1N1)
Maonan/SWL1536/2019(H1
pdm09-like virus
N1)pdm09-like virus
A/Hong
A/Hong Kong/45/2019
Kong/2671/2019(H3N2)-like
(H3N2)-like virus
virus
B/Washington/02/2019 B/Washington/02/2019
(B/Victoria lineage)-like virus (B/Victoria lineage)-like virus
B/Phuket/3073/2013-like Cell – or B/Phuket/3073/2013-like
Egg-Based (Yamagata lineage) virus Recombinant - (Yamagata lineage) virus
Vaccines Based Vaccines
https://www.cdc.gov/flu/season/faq-flu-season-2020-2021.htmCDC Recommendations on
Immunization During COVID19
Patients should continue to receive recommended vaccinations
All essential workers need a flu vaccine
All patients at increased risk for severe COVID-19 need a flu vaccine
All patients at increased risk for influenza complications need a flu vaccine
Defer vaccination in patients with suspected or confirmed COVID19 until out of isolation
Screen all patients for COVID19 symptoms
Wear masks and use other precautions
• Patient – cloth
• Immunizer – medical (N-95 not required, even for intranasal vaccine because it is not aerosol-
generating)
Immunizers in areas of high community transmission (e.g. Alabama) should wear eye protection
Safe distancing
• Fill paperwork out electronically
• Ask patients to wait away (e.g. in car) until ready
• Set a specific time for immunizations
https://www.cdc.gov/vaccines/pandemic-guidance/index.htmlInfluenza Vaccine Types
Inactivated Quadrivalent Standard Dose Vaccine
•Grown in eggs – takes 9 months
•Egg-adapted changes may induce difference between vaccine and circulating viruses
•Intradermal IIV has 40% less antigen
Live Attenuated Influenza Vaccine Quadrivalent
•For ages 2-49 who are otherwise healthy
•New H1N1 component since 2017 to address immunity
•Lower IgG response than IIV but high serum IgA mucosal response
•Viral shedding can occur for days after vaccination
High Dose Quadrivalent Vaccine
•For ages ≥ 65 years
•Has 4 times standard antigen
•24.2% more effective vs. IIV and shown to lower risk of hospitalization (esp in LTC patients)
Adjuvant Quadrivalent Vaccine
•For ages ≥ 65 years
•Has MF59 – oil-in-water emulsion of squalene oil
•Promotes immune response and reduces amount of virus needed to produce vaccine
Recombinant Quadrivalent Vaccine
•For ages ≥ 18 years
•Uses DNA from influenza hemagglutinin that is combined with baculovirus and has 3 times more antigen
•Production avoids egg-adapted mutations and is produced faster than egg-based vaccines (within 2 months)
Cell-culture Quadrivalent Vaccine
•For ages ≥ 4 years
•Grown in cultured cells of mammalian origin
•May offer better immunity vs. IIV – more like circulating flu strains
https://www.cdc.gov/flu/prevent/flushot.htmWhich antiviral A. Zanamivir
only requires 1 B. Baloxavir
dose to treat
C. Oseltamivir
uncomplicated
influenza? D. PeramivirInfluenza Antivirals
Oseltamivir
Oral Capsule
(75 mg)
Major ADRs Pearls
Only generic flu
Treatment Prophylaxis Nausea/Vomiting
antiviral
Available as
Twice daily X 5 Once daily x
Skin reactions capsules and
days 10 days suspension
Psychiatric effects
Prodrug
FDA approved CDC/AAP/IDSA FDA approved CDC/AAP/IDSA
(transient)
- ≥ 14 days – Any age - ≥ 1 year - ≥ 3 months
Drug of choice in
Bad taste (suspension)
pregnancy
Uyeki TM, et al. Clin Infect Dis. 2019;68(6):e1-e47
Influenza antiviral medications: summary for clinicians. www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm.
Kawai N, et al. J Infect. 2008;56(1):51-57
Chairat K, et al. Brit J Clin Pharmacol. 2016;81(6):1103-1112
Dutkowski R, et al. Int J Antimicrob Agents. 2010;35(5):461-467.Zanamivir
Inhalation Major ADRS Contraindications Pearls
(2 inhalations)
Diarrhea
Treatment Prophylaxis Bronchospasm Reactive lung
Naseau (less vs. diseases/
oseltamivir) bronchospasms
Minimal/no
Allergic reaction
resistance in
Twice daily Once daily Oropharyngeal/ among
X 5 days x 10 days facial edema influenza
Headache
strains in the
US
Dizziness Allergy to milk
protein
≥ 7 years ≥5 years Cough
Nasal congestion
Uyeki TM, et al. Clin Infect Dis. 2019;68(6):e1-e47;
Heneghan CJ, et al. BMJ. 2014;348:g2547
Influenza antiviral medications: summary for clinicians. www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm.Peramivir
IV
Therapy
Major ADRS Pearls
15-30 minute infusion
Diarrhea Approved primarily
from studies of
Treatment only Skin Reactions Influenza A
Psychiatric Reimbursed as
One dose effects outpatient infusion
(transient) therapy
Indicated for
those
≥ 2 years
Uyeki TM, et al. Clin Infect Dis. 2019;68(6):e1-e47
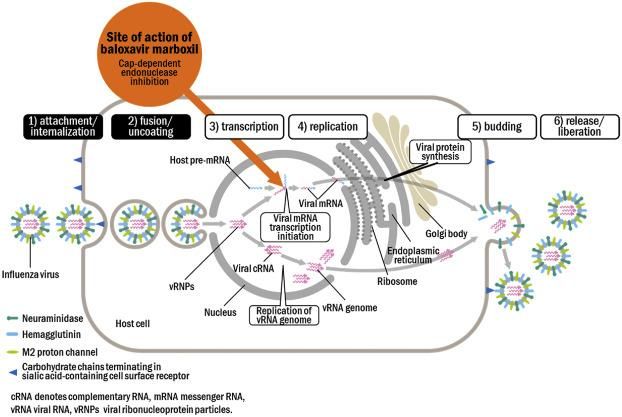
Influenza antiviral medications: summary for clinicians. www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm.Endonuclease inhibitor – blocks influenza viral
replication
Image reprinted from Noshi T, et al. Antiviral Res. 2018;160:115.Baloxavir marboxil - Treatment
Approved for treatment of
uncomplicated influenza in Only Oral “One and Done” Option
patients ≥ 12 years old – may
change by flu season 40 to < 80 kg ≥ 80 kg
(88 lb to < 176 lbs) (≥ 176 lbs)
Dosage and Administration
Two tablets = dose
Tell patients to take at the TWO 20-mg TWO 40-mg
same time Tablets Tablets
-------------------------
Take within 48 hours of
influenza symptom onset
--------------------------------
Dose is based on
patient’s weight
Pharmacists should ensure the right dose is selected
Compound summary baloxavir marboxil. National Center for Biotechnology Information website. pubchem.ncbi.nlm.nih.gov/compound/124081896.
Influenza antiviral medications: summary for clinicians. www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm.Baloxavir marboxil
Pregnancy and
Major ADRs Interactions Administration
Breastfeeding
Live influenza vaccine
Diarrhea Not studied in
Laxatives Avoid taking with pregnancy
Nausea dairy
Antacids
Calcium
No harmful effects
Headache
seen in rat studies
Iron
Bronchitis Magnesium
One dose = 2 tablets
Selenium Excreted into milk of
Nasopharyngitis lactating rats
Zinc
Compound summary baloxavir marboxil. National Center for Biotechnology Information website. pubchem.ncbi.nlm.nih.gov/compound/124081896.
Influenza antiviral medications: summary for clinicians. www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm.Baloxavir marboxil Studies
Baloxavir
Baloxavir marboxil
Placebo P-value
Median Time To Placebo P-value
marboxil
Median to symptom alleviation 73.2 hours 102.3 hours 24 hours
median
difference 25.6
difference 38.6 Median duration of viral shedding 48 hours 96 hoursBaloxavir marboxil Studies
miniSTONE-2
• Otherwise healthy children ages 1-11 years
• Treatment of uncomplicated influenza within 48 hours of symptom onset
• Treatment groups – 5 day
• Baloxavir – 1 dose then placebo
• < 20 kg = 2 mg/kg
• ≥ 20 kg – 40 mg
• Oseltamivir BID per weight dosing for 5 days
ADRS occuring in > 1% of Patients Baloxavir Oseltamivir
(n=80) (n=43)
Baloxavir Oseltamivir Median time to symptom alleviation
138.1 hours 150 hours
Vomiting 6.1% 15.5%
Influenza A H3N2 126.9 hours 118.4 hours
Diarrhea 5.2% 1.7%
Influenza A H1N1 115.8 hours 206.9 hours
Otitis media 2.6% 6..9%
Median fever duration 41.2 hours 46.8 hours
Ear pain 0.9% 3.4%
Median symptom duration 66.4 hours 67.9 hours
URTI 4.3% 3.4%
Median time to normal health 116.5 hours 111.6 hours
Rhinorrhea 3.5% 1.7% Development of flu complication
7.4% 7%
Cough 2.6% 1.7%
Median duration of viral shedding
Bronchitis 2.6% 1.7% 24.2 hours 75.8 hours
Overall ADR incidence
46.1% 53.4%
Baker et al. Pediatr Infect Dis J.2020;39:700-705Baloxavir Placebo Adjusted Risk Ratio
(n=374) (N=375) (95% CI)
Lab confirmed influenza 7 (1.9%) 51 (13.6%) 0.14 (0.06-0.3)
Negative PCR at baseline but contact with 5/344 39/337
0.13 (0.05-0.31)
PCR positive index patient (1.5%) (11.6%)
3/71
Patients < 12 years 11/71 (15.5%) 0.27 (0.08-0.9)
(4.2%)
4/303 40/304
Patients ≥ 12 years 0.1 (0.04-0.28)
(1.3%) (13.2%)
1/46
Patients with high-risk factors 8/52 (15.4%) 0.13 (0.02-0.94)
(2.2%)
Lab confirmed influenza regardless of fever or 49
114 (30.4%) 0.43 (0.32-0.58)
symotoms (13.1%)
PCR confirmed illness 20 (5.3%) 84 (22.4%) 0.24 (0..15-0.38)
Ikematsu et al. N Eng J Med.2020;383:309-320Open-label study of 1,113 adults and children treated in 2006-07 Flu season for
uncomplicated Influenza A or B in the outpatient setting
Duration of Fever
No Treatment Oseltamivir Zanamivir P-valueFever Duration After 1st Dose
Influenza A Influenza B
P-value for Influenza
Patients Patients Fever Duration A vs. B
(n) (n) (hours)
Oseltamivir 472 171 52.7Oseltamivir Peramivir Statistic Evaluation
(n=365) (n= 362)
Hazard ratio (97.5%CI)
Median Time to Symotom Alleviation 81.8 hours 81 hours 0.97 (0.814-1.157)
P-value
Patients afebrile 24 hours after 1st dose 181 (49.7%) 209 (57.7%) 0.0326
Median Time to Normal Activity 171.3 hours 195.5 hours > 0.05
Patients developing flu-related
10 12 >0.05
complication
Patients virus-positive on day 2 82.1% 68% 0.0038
Patients virus-positive on day 8 0.9% 1.5% >0.05
ADRs 288 293 >0.05
Kohno S, et al. Antimicrob Agents Chemother. 2011;55(11):5267-5276.Comparison of Oseltamivir vs.
Zanamivir for Household Contact
Prophylaxis
Household Oseltamivir +
Oseltamivir Zanamivir P-Value
Contacts Zanamivir
[Oseltamivir + [Oseltamivir +
N n/total (%) n/total (%) n/total (%) Overall zanamivir\] vs. zanamivir\] vs.
oseltamivir zanamivir
23/161 25/164 10/141
All patients 466 0.0676 -- --
(14%) (15%) (7%)
Index Patients with 1st dose ≤ 14/81 14/95
232 2/56 (4%) 0.0499 0.014 0.031
24 hours after symptom onset (17%) (15%)
Index Patients with 1st dose ≤
9/80 11/69
24 hours after symptom onset 234 8/85 (9%) 0.4491 -- --
(11%) (16%)
Carrat F, et al; BIVIR study group. Antivir Ther. 2012;17(6):1085-1090.P-Value
Oseltamivir +
Oseltamivir Zanamivir
Zanamivir [Oseltamivir + [Oseltamivir +
(n=176) (n=173) Oseltamivir
(n=192) zanamivir\] zanamivir\] vs.
vs. zanamivir
vs. oseltamivir zanamivir
Median Time to Symptom
3 4 3.5 >0.05 0.015 0.78
Alleviation (days)
Day 2 Influenza RT-PCR
62.5% 40.5% 52.6%Multi-center retrospective study of inpatients treated for Influenza A
Oseltamivir Baloxavir
P-value
(n=431) (n=359)
224/273
Patients with resolution of hypoxia [N/total (%)] 152/348 (75.6%) 0.052
(82%)
Median time from antiviral administration to
71.95 hours 51.717 hoursSingle-center, retrospective, observational study of inpatients treated for
Influenza A
Peramivir
Combination
monotherapy P-value
(n=431)
(n=359)
Oxygen requirement on 224/273
0.082
admission [N (%)] 4 (40%) (82%)
Duration of symptoms prior to 1.9 ± 1.7
2 ± 2 days 0.87
treatment initiation ± SD days
30 day mortality 0 6 (4.5%) 1
2.7 ± 2.9
Mean time to afebrile 2.1± 1.2 days 0.3 days
days
Yoshimura et al. Eur J Infect Dis. 2020;doi:10.1007/s10096-020-03888-7Multi-center observational study of 295 outpatients with Influenza A from 50
Japanese clinics December 1, 2018 to April 30, 2019
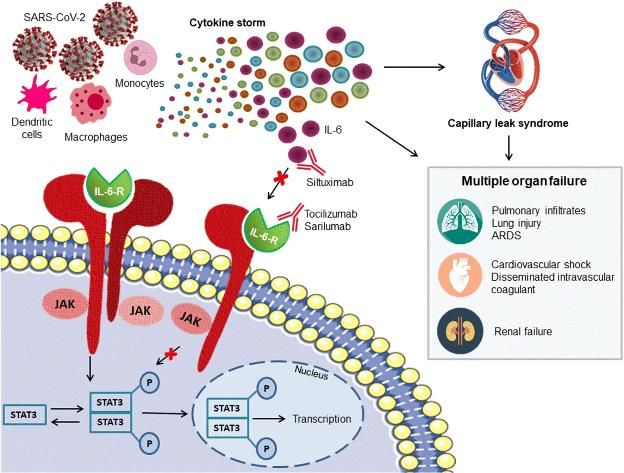
Yoshii et al. Intern Med.2020;59:1509-1513THERAPEUTICS FOR COVID-19
Virus Phase Pulmonary Severe Phase Viral replication Antiviral therapy
Phase and spread
Illness Severity
Anti-inflammatory,
Inflammatory Increased antithrombotic, and
Prothrombot
Response inflammatory state
ic state anticoagulation approaches
“Cytokine storm”
Cell/organ protection
Organ and tissue therapies
Time Course of Illness damage
Steroids
Antivirals Organ
?Anticoagulation?
Steroids
IL-6 Inhibitors support/replacement
Antivirals ?Anticoagulation? Organ failure
JAK Inhibitors
Convalescent
?Famotidine?
Plasma
?Complement
?Famotidine?
inhibitors?
Death
Adapted from https://rebelem.com/the-recovery-trial-dexamethasone-for-covid-19/ Adapted Figure 1. Fernandez et al. J Clin Med. 2020;9:2030Which of the following is recommended in the outpatient management of COVID-19 A. Remdesivir B. Hydroxychloroquine C. Acetaminophen D. Losartan
Outpatient Treatment of COVID-19
• Minimal guidance
• Supportive care
• Fever – acetaminophen
• Antitussive
• Antiemetic
• Hydration
• Therapies in studies
Remdesivir Telmisartan Aspirin Tranexamic acid (UAB)
Hydroxychloroquine Imatinib Rivaroxaban N-acetylcysteine
Lopinavir/ritonavir Colchicine Vitamin C Convalescent plasma (UAB)
Losartan Interferon-beta Zinc Anti-spike (s) SARS-CoV-2
Monoclonal Antibodies
NCT04342728 NCT04365582
NCT04338074 NCT04476602
NCT04501952 NCT04356495
NCT04373460 NCT04372628 NCT04324463
NCT04425629 NCT04419025 NCT04342169Nucleoside analogue with
broad-spectrum antiviral activity
• Causes pre-mature termination of
viral RNA transcription
• Prodrug – thought to convert to For severe COVID-19
Considerations in times active form 2 hours after infusion • Oxygen saturation < 94% on room air
of short supply
• Supplemental oxygen
• Demonstrates most benefit in
• Mechanical ventilation or ECMO
patients on supplemental oxygen
rather than mechanical ventilation
or ECMO
Remdesivir
Long, complex manufacturing
process
(Veklury®) Dose
• 200 mg IV day 1 then 100 mg daily
• Takes 6-8 months
• Inhaled version in development
Duration
Not studied in some
• Supplemental oxygen – 5 days
populations
• Ventilator or ECMO – 10 days
• CrCl < 50 mL/min
• LFTs > 5 times ULN
• Pediatrics (studies ongoing)
Bhimraj et al. IDSA COVID19 guidelines
Ko WC et al. Int J Antimicrob Agents.2020;doi: 10.1016/j.ijantimicag.2020.105933
Dong L et al. Drug Discov Ther.2020;14:58-60Remdesivir Study Summaries
Study Design Population Groups Results
Grein et al Retrospective study Inpatients with oxygen 200 mg day 1 then • 36 (68%) patients had improvement in oxygen-
on compassionate saturation < 94% on room 100 mg daily for 9 support class
use air days • 17 or 30 patients requiring ventilation at baseline
were extubated
53 patients 57% on mechanical • 25 (47%) patients discharged alive
ventilation • 7 (135) patients died
8% on ECMO • ADRs – LFT elevations, diarrhea, rash, kidney
dysfunction, hypotension
Goldman et Open-label Phase 3 Inpatients with oxygen Group 1 – 5 days • Baseline status of patients in 10-day course worse
al. saturationHydroxychloroquine
Old drug with known immunomodulatory effects – including IL-1 and IL-6
Known antiviral activity to other coronaviruses and in vitro activity vs. COVID-19
(exact antiviral mechanism unknown – may inhibit endocytosis and viral replication
and induce interferon response)
Can be safely used – but does have potentially problematic ADRs that need to be
monitored for (e.g. QTc prolongation, hypoglycemia)
Evidence-base is complicated and difficult to interpret
No consistent dosing in clinical trials
Conflicting evidence about efficacy
Bhimraj et al. IDSA COVID19 guidelines
https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/#toc-3Observational Evaluation of HCQ in
Hospitalized COVID19 Patients in
New York
▪ Observational study at New York
Crude
Presbyterian Hospital-Columbia University HCQ No HCQ Hazard
Propensity score
Irving Medical Center Hazard Ratio
(N=811) (n=565) Ratio
(95%CI)
▪ March 7 to April 8, 2020 (95% CI)
▪ Did not enroll patients who were 2.37
Death or 262
intubated, died, or transferred within 24 intubation (32.3%)
84 (14.9%) (1.84 – 0.98 (0.73-1.31)
hours of presentation 3.02)
157
▪ HCQ presented as an option for patients Death (19.36%
75
with oxygen saturations < 94% on room air (13.27%)
)
▪ Dose: 600 mg twice on Day 1 then 400 mg Intubated
154
26 (4.6%)
daily for 4 days (19%)
▪ 85.9% of those in HCQ group received it Intubated
49 (6%) 17 (3%)
within 48 hours of presentation then died
▪ Use of azithromycin was allowed
Discharged 552 473
alive (68%) (83.7%)
Geleris et al. N Eng J Med 2020;382:2411-2418HCQ for Post-COVID19 Exposure Prophylaxis
• Household or occupational exposure to COVID-19
• Distance < 6 feet for > 10 minutes)
• Without appropriate PPE (eye shield, face mask)
• Patients in U.S. and Canada
• Dose
• HCQ 800 mg x 1
• HCQ 600 mg 6-8 hours later
• HCQ 600 mg daily for 4 days
• Did not meet power - Estimated needed 750 per group
• Completion of regimen – poor adherence - HCQ (75.4%) vs. Placebo (82.6%); p=0.01
• Symptom severity of those with symptoms at day 14 did not differ (p=0.34)
• ADRs higher with HCQ (40.1% vs. 16.8%; pHCQ ± Azithromycin in Mild-
Moderate COVID19
Randomized controlled trial at 55 hospitals in Brazil
Adult inpatients with suspected or confirmed COVID-19 within 14 days of symptom onset
Excluded if on oxygen > 4L/min or >40% by Ventury mask (or more aggressive oxygen requirements) or QTc >480 msec
Dose – 400 mg BID for 7 days
HCQ + Effect Estimate (95% CI)
HCQ Control
Azithromycin
(n=159) (n=173) [HCQ + A] vs. Control HCQ vs. Control [HCQ+A] vs. HCQ
(n=172)
Mean days free from respiratory support
11.1 11.2 11.1 0.1 (-0.7 to 0.9) -0.2 (-1.1 to 0.6) 0.3 (-0.6 to 1.1)
within 15 days
Use of high-flow oxygen or non-invasive
16 (9.3%) 17 (10.7%) 16 (9.25) 1.1 (0.6 to 2.03) 1.19 (0.65 to 2.21) 0.92 (0.5 to 1.7)
ventilation within 15 days
Use of mechanical ventilation within 15 days 19 (11%) 12 (7.55) 12 (6.9%) 1.77 (0.81 to 3.87) 1.15 (0.49 to 2.7) 1.54 (0.71 to 3.35)
Hospital length of stay (days) 10.3 9.6 9.5 0.9 (-0.3 to 2.1) 0.2 (-1 to 1.3) 0.7 (-0.6 to 1.9)
In-hospital mortality 5 (2.9%) 7 (4.4%) 6 (3.5%) 0.64 (0.18 to 2.21) 1.47 (0.48 to 4.53) 0.43 (0.13 to 1.45)
Thromboembolic complications within 15
2 (1.2%) 3 (1.9%) 2 (1.2%) 0.89 (0.31 to 2.54) 1.39 (0.53 to 3.65) 0.64 (0.24 to 1.68)
days
AKI within 15 days 6 (3.5%) 4 (2.5%) 5 (2.9%) 1.18 (0.44 to 3.2) 0.88 (0.29 to 2.63) 1.35 (0.47 to 3.84
Cavalcanti et al. N Eng J Med.2020;doi:10.1056/NEJMoa2019014HCQ ± Azithromycin in Mild-
Moderate COVID19
HCQ + Effect Estimate (95% CI)
HCQ Control
Azithromycin
(n=159) (n=173) [HCQ + A] vs.
(n=172) HCQ vs. Control [HCQ+A] vs. HCQ
Control
Median 7-level ordinal score at 15 days 1 (1 to 2) 1 (1 to 2) 1 (1 to 2) 0.99 (0.57 to 1.73) 1.21 (0.69 to 2.11) 0.82 (0.47 to 11.43)
1. Not hospitalized/no limitations on 102
118 (68.6%) 117 (67.6%)
activities (64.2%)
2. Not hospitalized/activities limited 22 (12.8%) 27 (17%) 29 (16.8%)
3. Hospitalized/ no oxygen 15 (8.7%) 12 (7.5%) 8 (4.6%)
4. Hospitalized with oxygen 5 (2.9%) 6 (3.8%) 5 (2.9%)
5. Hospitalized with non-invasive
0 2 (1.3%) 2 (1.2%)
ventilation or high-flow oxygen
6. Hospitalized on mechanical
9 (5.2%) 5 (3.1%) 7 (4%)
ventilation
7. Death 3 (1.7%) 5 (3.1%) 5 (20.9%)
Cavalcanti et al. N Eng J Med.2020;doi:10.1056/NEJMoa2019014OTHER HCQ STUDIES Study Hazard Ratio (95% CI) Ip et al. Adjusted HR 1.02 (0.83 to 1.27) Magagnoli et al Adjusted HR 0.99 (0.5 to 1.92) Mehevas et al. Weighted HR 1.2 (0.4 to 3.3) Rosenbert et al Adjusted HR 1.08 (0.63 to 1.85) Bhimraj et al. IDSA COVID19 guidelines
HCQ + Azithromycin to Prevent
Hospitalization or Death
• Recently completed Phase IIB study
• HCQ dose – 400 mg BID on day 1 and then 200 mg BID
for 6 days
• Stratification based on risk of progression to severe
COVID-19
• High risk – age ≥ 60 years or ≥ 1 specified co-morbidity
• Symptoms < 10 days
• Results TBA
NCT04358068Lopinavir/ritonavir
Not recommended outside of clinical trial
ADRs
• Nausea, anorexia, diarrhea, abdominal discomfort,
acute gastritis, skin reactions, hepatotoxicity,
pancreatitis, QTc prolongation
Many drug interactions
• CYP3A4 inhibition
Bhimraj et al. IDSA COVID19 guidelinesLopinavir-ritonavir in hospitalized adults
with severe COVID-19
Lopinavir-ritonavir Standard Care
Difference (95% CI) ▪ Open-label randomized trial
(n=99) (n=100)
▪ Conducted early in pandemic
Time to clinical improvement HR 1.31 (0.95 to
(median days)**§
15 (13 to 17) 16 (15 to 18)
1.8)
(January 18-February 3, 2020) in
Wuhan China
28 Day Mortality 19 (19.2%) 25 (25%) -5.8 (-17 to 5.7)
▪ Treatment Groups
Clinical improvement
▪ Standard care
Day 7 6 (6.1%) 2 (2%) 4.1 (-1.4 to 9.5)
▪ Lopinavir/ritonavir (400
Day 14 45 (45.5%) 30 (30%) 15.5 (2.2 to 28.8) mg/100 mg) po BID plus
Day 28 78 (78.8%) 70 (70%) 8.8 (-3.3 to 20.9) standard care
14 (12 to ▪ Standard care included
Hospital length of stay (days) 16 (13-18) 1 (0 to 2)
17) oxygenation, antibiotics, sepsis
ICU length of stay (days) 6 (2 to 11) 11 (7 to 17) -5 (-9 to 0) treatment, dialysis, and
Mechanical ventilation
extracorporeal membrane
4 (3 to 7) 5 (3 to 9) -1 (-4 to 2) oxygenation as needed
(median days duration)
Oxygen support (days) 12 (9 to 16) 13 (6 to 16) 0 (-2 to 2)
Time to discharge (median 12 (10 to
14 (11 to 16) 1 (0 to 3)
days) 16)
Time to death (median days) 9 (6 to 13) 12 (6 to 15) -3 (-6 to 2)
** In the modified intention-to-treat analysis that excluded 3 patients with early death, the between-group difference for median time to clinical
improvement
(15 vs. 16 days) was significant)
§ Approximately 14% of lopinavir-ritonavir group did not complete full 14-day course; this was primary due to gastrointestinal adverse effects
Cao B et al. N Eng J Med.2020;doi:10.1056/NEJMoa2001282Image source: https://emcrit.org/pulmcrit/recovery/
RECOVERY Trial
(Randomized Evaluation of Covid-19 Therapy)
• Large international trial designed to evaluate effects
of multiple potential COVID-19 treatments
• Started in March 2020
• Includes hospitalized adults with suspected or
confirmed COVID-19 – pregnant and breastfeeding
women were included
• Excludes patients with medical histories that in the
opinion of the physician would put the patients at
“substantial risk” if they participated
• Open label
• Testing – low dose dexamethasone, azithromycin,
tocilzumamb, convalescent plasma
• June 2020 - ceased testing of HCQ and
lopinavir/ritonavir due to lack of benefit
Horby et al. N Eng J Med.2020;doi:10.1056/NEJMoa2021436
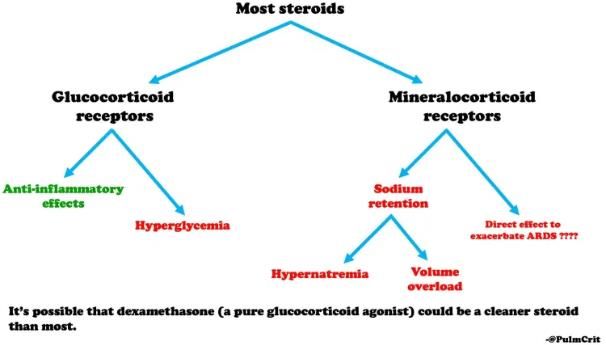
https://www.recoverytrial.net/newsRecovery Trial: Dexamethasone
Dexamethasone Usual Care
Rate Ratio ▪ Dexamethasone 6 mg
(95% CI)
Mean age 66.9 ± 15.4 years 65.8 ± 15.8 years
until hospital discharge
Median days since symptom
8 (5 to 13) 9 (5 to 13)
or for up to 10 days
onset
Median days since hospital
▪ Dexamethasone chosen
2 ( 1 to 5) 2 (1 to 5)
admission because it has the least
28-day mortality [n/total (%) 482/2104 (22.9%)
1,110/4,321
(25.7%)
0.83 (0.75-0.93)
(p 7days) had a
greater mortality benefit with dexamethasone
Horby et al. N Eng J Med.2020;doi:10.1056/NEJMoa2021436Use of Steroids
Hospitalized patients with • Dexamethasone 6 mg IV/po for up to 10 days
severe COVID-19 on • Alternatives – methylprednisolone 32 mg or
oxygen prednisone 40 mg
Patients with COVID-19
• Steroids are not recommended
not requiring oxygen
• Steroids reduced viral clearance and resulted in
Pearls worse outcomes with SARs and MERS-Co-V
• May be required to treat ARDS
• Blood glucose
• Mental status
Important Monitoring
• Adrenal suppression (hemodynamics)
• Secondary bacterial or fungal infections
Bhimraj et al. IDSA COVID19 guidelinesConvalescent Plasma
• Emergency Investigational New • Open-label multicenter RCT in Wuhan
Drug application – March 24, (n=103)
2020 • Patients with severe disease
• Time to clinical improvement significantly
• Plasma from COVID-19 shorter with convalescent plasma (13 vs.
19 days; p=0.03)
survivors into patients • More patients clinically improved at day
14 [(14 (60.9%) vs. 6 (27.3%); p=0.02]
• Early study in 5 patients • Shorter time to discharge (13 days vs 19
days; p=0.05)
showed significant • More virus negative patients at 72 hours
improvement in clinical status [19 (90.5% vs. 7(41.2%); p=0.001]
• All patients
• No difference in time to clinical
improvement, amount of clinical
improvement, length of stay, or 28-day
mortality in all patients
• Significantly more patients virus negative
at 24, 48, and 72 hours
• Patients with life-threatening disease
• No difference in any outcome
Li et al. JAMA.2020;324:460-470
Shen C et al. JAMA.2020;doi:10.1001/jama.2020.4783
Food and Drug Administration. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-continues-facilitate-
development-treatmentsTocilizumab (Actemra)
• Disease-modifying anti-rheumatic drug (DMARD) normally used for rheumatoid arthritis and juvenile idiopathic
arthritis
• Recombinant humanized monoclonal antibody specific for IL-6
• Pathophysiology in severe COVID-19 involves the “cytokine storm” – includes the release of interleukins-6 (IL-6) which
signals other cells to activate the immune system
• Mechanism – blocks IL-6
• Dose – 4-8 mg/kg (max 800 mg dose) for 1-2 doses (separated by 12 hours)
• Potential indications
• COVID-19 pneumonia, worsening pulmonary status, Ferritin > 600 mcg/mL, D-dimer > 1 mg/L and mechanical
ventilation < 24 hours
• Interesting drug-interaction considerations
• Does not inhibit CYP enzymes, but elevated IL-6 levels do – administering tocilizumab may affect drug
metabolism by impacting inflammation
Bhimraj et al. IDSA COVID19 guidelines
Guarald et al. Lancet Rheumatology.2020;2:E474-484
Crisafulli et al. BioDrugs.2020;34:415-422
https://www.aphp.fr/contenu/tocilizumab-improves-significantly-clinical-outcomes-patients-moderate-or-severe-covid-19Tocilizumab (Actemra) CORIMUNO-TOCI Open label RCT • 129 patients inpatients with moderate-severe COVID-19 pneumonia not requiring ICU care on admission • Significantly fewer people in tocilizumab group had the composite outcome of need for ventilation or death at day 14 Retrospective study of 544 inpatients with severe COVID-19 pneumonia • Significantly fewer deaths compared to stand care [13 (7%) vs. 73 (20%); p
Famotidine
• Anecdotal reports from China suggested that patients on famotidine
prior to COVID-19 infection had improved survival vs. those on PPIs
• Potential mechanism of benefit still unclear – may bind and inhibit
COVID-19’s main protease, 3C-like main protease, which processes
proteins needed for viral replication
• IDSA recommends against use just for COVID-19 outside of a clinical trial
• Only one non-randomized study
• Famotine (n=84) vs. No famotidine (n=1,536)
• Decrease in composite outcome of death or intubation (HR 0.42; 95% CI 0.21 to
0.85, p< 0.01)
• Unpublished anecdotal case studies indicate benefit with 40 mg po TID in
mild COVID-19
• Adaptive trial currently recruiting in moderate-severe COVID-19
• Famotidine IV 360 mg/day for up to 14 days vs. placebo
• Could be used for stress ulcer prophylaxis in critically ill patients
Bhimraj et al. IDSA COVID19 guidelines
Freedberg et al. Gastroenterology.2020;doi:10.1053/j.gastro.2020.05.053
NCT04370262The Vitamins and Supplements
Vitamin C (Ascorbic Acid) Vitamin D Zinc
• Antioxidant – may help with • Involved in immunity and • Possible antiviral activity – may
infection and inflammatory issues inflammatory response through inhibit viral RNA polymerase
• Infection may decrease vitamin C in multiple pathways activity and viral replication in
the body • No data in COVID-19 COVID-19
• Dose – 1.5-3 grams IV Q 6 hours for • Inconsistent data about efficacy • Involved in immunity – antibody
up to 10 days involving other infections and WBC production, enzyme co-
• 50 mg/kg IV Q hours for 4 days • Multiple guidelines state there is factor, wound healing
has also been used insufficient evidence to recommend • Dose 220 mg BID for 5 days
• Oral doses of 1 gram for 7 days for or against use. • Retrospective study of inpatients
and 4 grams BID are in studies did not indicate any impact on
• No data in COVID-19 – studies hospital/ICU length of stay, or
underway duration of mechanical ventilation.
Patients were discharged home
• NIH guidelines recommend use in
more frequently and needed lower
non-crucially ill patients and say
level of care
insufficient evidence to recommend
for/against use in critically ill • Long term use (> 10 months) may
cause copper deficiency –
hematologic and neurologic effects
Bauer et al. Cleve Clin J Med. 2020;doi:10.3949/ccjm.87a.ccc046
Li J. Crit Care.2018;22:258 Carlucci et al. Post-ed.2020;doi:10.1101/2020.05.02.20080036
Fowler et al. JAMA.2019;322:1261-1270 Hemila et al. Cochran Database Syst Rev.2013;doi:10.1002/14651858.CD005532.pub3
Gruber-Bzura BM. Int J Mol Sci. 2018;doi:10.10.3390/ijms19082419 Marik et al. J Thorac Dis.2020;12:S84-S88
Aranow C. J Investig Med.2011;59:881-6 Erol A. Doi:10.31219/osf.io/p7ex8
De Smet et al. MedRxiv.doi:10.1101/202005.01.20079376 Kashiouris et al. Nutrients.2020;12:piie292What about NSAIDs?
Theory
• ACE2 is the host cell surface receptor of the SARS-CoV-2 envelope spike protein – COVID-19 causes
downregulation of ACE2 expression leading to excessive production of angiotensin II which causes
increased vascular permeability and lung damage
• NSAIDS (e.g. ibuprofen) upregulate ACE2 allowing COVID-19 more entry into human target cells and
leading to a more severe infection
Concern
• May increase risk of contracting infection and/or cause severe disease
History of complications in bacterial pneumonia
• May impair recruitment of polymorphonuclear cells – results in delayed inflammatory response and
resolution of infection
• Causal relationship not established
Study of 403 patients with COVID-19
• Median age 45 years
• No difference vs. acetaminophen in mortality or need for respiratory support
Indomethacin
• In vitro antiviral activity vs. COVID-19
• No human studies
Bhimraj et al. IDSA COVID19 guidelines
Sridharan et al. Am J Thera.2020;0:1-3
Rinott et al. Clin Microbiol Infect. 2020;doi:10.1016/j.cmi.2020.06.003
Sodhi et al. CHEST.2020;doi:10.1016/j.chest.2020.03.040
Zu et al. doi:10.1101/2020.04.01.017624Other Repurposed Potential
Therapies
Favipiravir (Avigan) Colchicine Heparin
• Anti-influenza antiviral approved in • Anti-inflammatory - may be • Study of 2075 inpatients
Japan and China helpful in reducing cytokine associated with lower
• Blocks RNA-dependent RA storm
polymerase and SARS-Co-V-2 viral mortality (p=0.003) (data
• Dose 1.5 mg LD then 0.5 mg in on route and dose
replication phase 60 mg then 0.5 mg BID for up to
• Dose 1600 mg BID on day 1 then 3 weeks unavailable)
600 mg BID for 7-14 days total
• Study of 105 inpatients in
• ADR of concern – QTc prolongation
Greece shown better clinical
• Max dose of APAP/day – 3 grams outcomes (ventilation or death)
• Study of 240 patients with mild than standard care (1.8% vs.
COVID-19 showed better recovery 14%; p=0.02)
at day 7 vs. umifenovir (71% vs.
56%) • Retrospective review showed no
• Study in 150 patients showed 40% difference in protective effect on
faster time to clinical cure and colchicine for RT-PCR (+) or (-)
28.6% faster viral clearance
(pPotential Repurposed Drugs
Being Explored
Lenzilumab Losamapimod Canakinumab Nitric Oxide
Inhaled
Anakinra Baricitinib Interferons
prostacyclin
Ruxolitinib Siltuximab Sirolimus IvermectinPhase II Study in Adult Outpatients with COVID-19 and Symptoms < 5 days
Povidone-iodine Essential oils Tap water
Control (n=5)
gargle (n=5) gargle (n=5) gargle (n=5)
Viral clearance
5 (100%) 4 (80%) 1 (20%) 0 (0%)
by day 6
Negative RT-PCR
5 (100%) 4 (80%) 2 (40%) 1 (20%)
at day 12
Progression to
more severe
0 (0%) 0 (0%) 0 (0%) 0 (0%)
disease by day
12
10 mL gargle for 30 seconds, three times a day for 7 days
NCT 04410159COVID-19 Vaccines
U.S. government has pledged over $8.2 billion for the development and distribution of various
vaccine candidates
mRNA
•Moderna and NIAID – mRNA-1273
•Encodes pike protein for COVID-19 and uses messenger RNA to tell cells how to make protein to
make antibodies
•2 IM doses – 28 days apart
•The COVE study underway
•Pfizer developing similar vaccine
Adenovirus
•Uses virus that causes common cold with gene from COVID-19 integrated
•1 IM Dose
DNA
•DNA plasmid with electroporation
•2 intradermal or IM doses depending on vaccine
Protein subunit
•Recombinant or native-like trimeric subunit spike protein vaccine
•1-2 IM doses depending on vaccine
Inactivated
•2 IM doses
O’Callaghan KP et al. JAMA.2020;324:437-438
WHO Draft Landscape of COVID-19 candidate vaccines. https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines
https://www.hhs.gov/about/news/2020/08/07/fact-sheet-explaining-operation-warp-speed.html7-point Ordinal Scale
Death 07 Not hospitalized,
01 no limitations on
06 activities
Hospitalized 02
On invasive Not hospitalized,
mechanical 05
Limitations on activities
ventilation or
ECMO
03
04
Hospitalized Hospitalized,
On non-invasive Not requiring
Hospitalized
ventilation or supplemental oxygen
Requiring supplemental
high-flow oxygen oxygen
NCT04315948SOLIDARITY Trial
International open-label, randomized adaptive trial
Coordinated by the World Health Organization
As of July 1, 2020 – 5,500 patients in 21 countries
recruited
Adults hospitalized with confirmed COVID-19 Multiple Treatment Groups
• Remdesivir– ongoing
• HCQ – stopped
• Lopinavir/ritonavir - stopped
Primary Endpoint • Lopinavir/ritonavir with IFN-beta – ongoing
• Standard of care alone. - ongoing
All-cause hospital mortality at 3 weeks
Key Exclusion Criteria
• Life expectancy < 3 months
• LFTs > 5 times ULN
• Acute co-morbidity within 7 days of screening
• QTc > 450 ms
Expected Conclusion • Taking medication with known interaction with study
November 2020 agents.
NCT04321616
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-
for-covid-19-treatmentsDisCoVeRy Trial
Multi-centered Phase 3, randomized adaptive trial
European study similar to SOLIDARITY trail
Adults hospitalized with confirmed COVID-19 and
oxygen saturation < 94% on room air or requiring Multiple Treatment Groups
supplemental oxygen or ventilatory support
• Remdesivir (10 days) – ongoing
• HCQ – stopped
• Lopinavir/ritonavir - stopped
Endpoints • Lopinavir/ritonavir with IFN-beta – stopped
Clinical status on 7-point ordinal scale at day 15 • Standard of care alone. - ongoing
Time to improvement
Time to discharge
Oxygen requirements Key Exclusion Criteria
Length of stay
Mortality • Life expectancy < 3 months
Safety • LFTs > 5 times ULN
• CrCl < 30 mL/min or on dialysis
Expected Conclusion • Acute co-morbidity within 7 days of screening
• QTc > 450 ms
March 2023 • Taking medication with known interaction with study
agents.
NCT04315948REMAP-CAP
Multi-centered embedded randomized adaptive trial
International study based in UK
Multiple Treatment Groups
• Macrolides for immune function
• Alternative steroid strategies
• Antivirals
Endpoints • Immune modulation therapy
• Convalescent plasma
21-day ICU free days • Therapeutic anticoagulation
WHO 8 point ordinal scale at day 15 • Vitamin C
All cause mortality - ICU discharge, hospital
discharge, day 90 Key Exclusion Criteria
Hospital length of stay • > 24 hours since ICU admission
Ventilator free days • > 36 hours treatment with non-trial medications
Expected Conclusion
Ongoing
www.remapcap.orgOther Large COVID-19 Studies
Accelerating COVID-19 Research and Development (ACCORD)
• UK Study of potential drugs
• If medications show promise – they are transitioned into larger studies (i.e.
RECOVERY)
• Drugs – MEDI3506, zilucoplan, bemcentinib, acalabrutinib
PRINCIPLE Trial
• UK study evaluating potential treatments in patients 50 years and older
• Outpatient study
• Currently evaluating azithromycin and doxycycline
Wise et al. BMJ.2020;370:m2670There may or may not be an
answerYou can also read

















































