A Broad Exploration of Anxiety Workbook June 2021 - Advanced Clinical Group - TA ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A Broad Exploration of Anxiety
Workbook
June 2021 – Advanced Clinical Group
TA Training Organisation
The Horsforth Centre for Psychotherapy
138 Low Lane
Horsforth, Leeds, LS18 5PX
Office: 0113 258 3399
Jane Williams: 07766752437
Andy Williams: 07780677697
janeaireleeds@gmail.com
andywilliams@therapysecure.com
Page: 1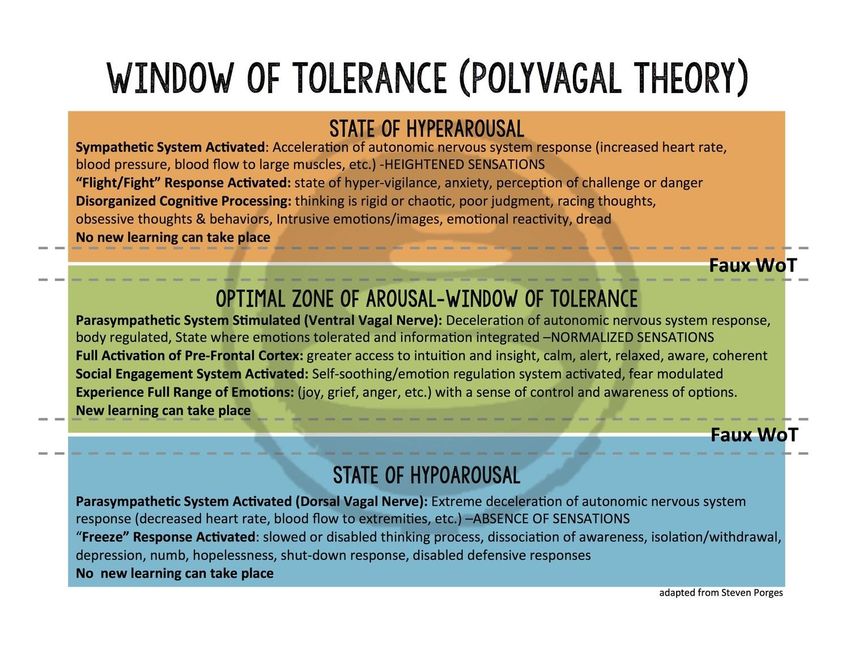
Timetable for the day
0930 to 1030 Part 1 Check-In
1030 to 1100 Part 2 DSM – V and the range of presentations
11.00 to 11.30 BREAK BREAK
11.30 TO 12.30 Part 3 Psycho-Education &
Polyvagal Theory
12.30 to 1.30 LUNCH LUNCH
1.30 to 2.30 Part 4 Conceptulisation and Exercise
2.30 to 2.45 BREAK BREAK
2.45 to 3.15 Part 5 Anxiety involving Contamination and Discounting
Berne’s four stages of cure.
3.15 to 4.00 Part 6 Anxiety as a Racket Process
4.00 to 4.30pm Part 7 The existential & ACT
Key Texts – please see handbook plus:
Cognitive Therapy of Anxiety Disorders: A Practice Manual and Conceptual Guide
Adrian Wells. 1997. Wiley, Chichester.
DSM-V. Diagnostic and Statistical Manual of Mental Disorders.
American Psychiatric Association. 2013.
Page: 2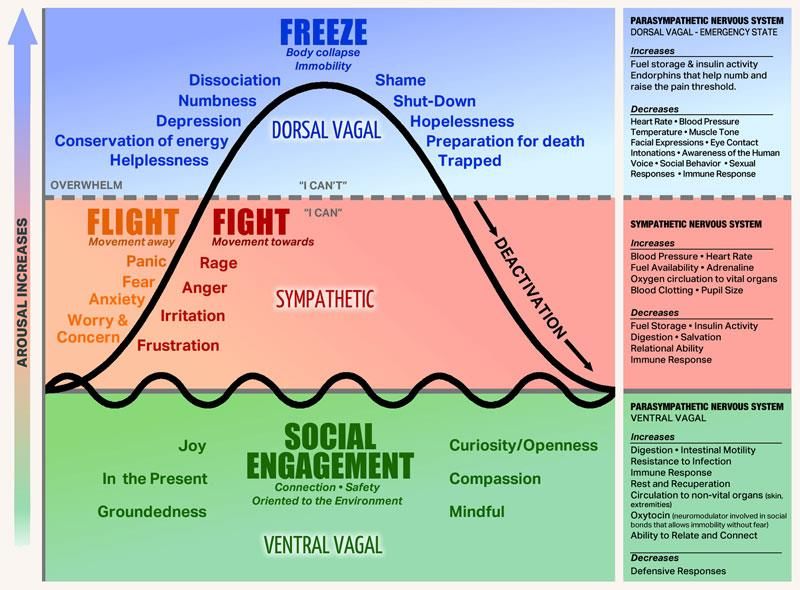
UNDERSTANDING THE RANGE OF DISORDERS
There was a significant update in how presentations of distress were categorised between DSM-IV
and DSM-V. In effect, a new category of distress was acknowledged that now includes PTSD.
Anxiety disorders include disorders that share features of excessive fear and anxiety and related
behavioral disturbances. Fear is the emotional response to real or perceived imminent threat,
whereas anxiety is anticipation of future threat. Obviously, these two states overlap, but they also
differ, with fear more often associated with surges of autonomic arousal necessary for fight or
flight, thoughts of immediate danger, and escape behaviors, and anxiety more often associated
with muscle tension and vigilance in preparation for future danger and cautious or avoidant
behaviors. Sometimes the level of fear or anxiety is reduced by pervasive avoidance
behaviors. Panic attacks feature prominently within the anxiety disorders as a particular type of
fear response. Panic attacks are not limited to anxiety disorders but rather can be seen in other
mental disorders as well.
What is the difference between different anxiety disorders? DSM-V suggests two key components
to look at:
1. The difference in the types of objects or situations that are inducing anxiety.
2. The difference in the associated cognitive ideation – and we must always consider MENTAL
IMAGES TOO – when we are considering working with anxiety
A way to conceptulise anxiety is to think of it as a developmental problem – developmental
normative fear or anxiety becoming:
1. Excessive – taking cultural factors into consideration.
2. Persisting beyond developmentally appropriate periods.
Page: 3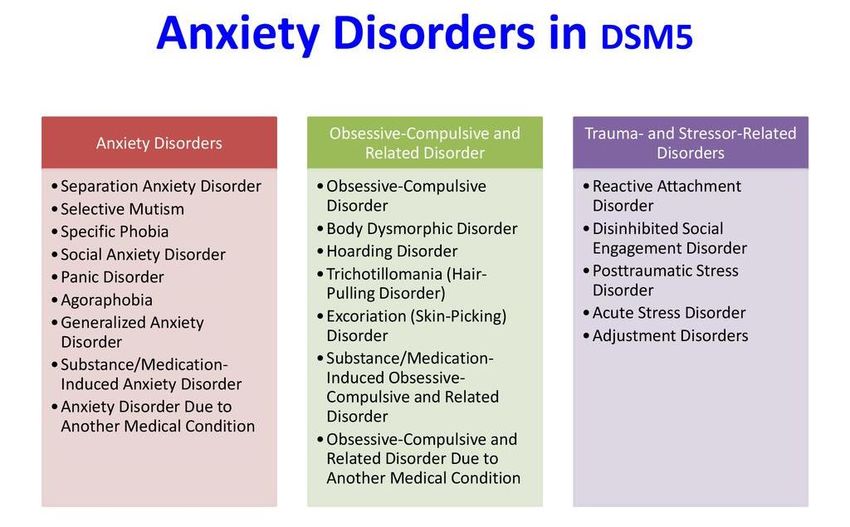
Selective Mutism
A consistent failure to speak in social situations in which there is an expectation to speak, although
speaks in other situations.
Specific Phobia
Fearful or anxious about, or avoid circumscribed objects or situations.
- Usually no specific cognition associated
- Fear, anxiety or avoidance usually out of proportion.
Social Anxiety
Avoids social situations, with a fear of being scrutinized.
- Fear of negative evaluation by others leading to embarrassment, humiliation, offending or
being rejected by.
Panic Disorder
Recurrent, unexpected panic attacks with a fear of recurrent panic attacks too.
A panic attack is an abrupt surge of intense fear accompanied by physical and cognitive symptoms.
Expected or unexpected panic attacks.
Agoraphobia
Fear or anxiety around public transportation, open spaces, enclosed spaces.
- Thoughts that escape may be hindered plus other fears.
Generalised Anxiety Disorder
Persistent and excessive worry about various domains that is difficult to control.
Physical symptoms including restlessness, keyed up and on edge, easily fatigued, difficulty
concentrating, mind going blank, irritability, muscle tension and sleep disturbance.
Notes about Panic Attack Specifier – PANIC ATTACK IN ITSELF IS NOT A MENTAL DISORDER AND
CANNOT BE CODED IN DSMV. Panic Attacks can occur in the context of ANY anxiety disorder as well
as other mental disorders. An abrupt surge of intense fear or intense discomfort that reaches a
peak within minutes, and during which time four (or more) of the following symptoms occur: (Note:
The abrupt surge can occur from a calm state or an anxious state.)
1. Palpitations, pounding heart, or accelerated heart rate.
2. Sweating.
3. Trembling or shaking.
4. Sensations of shortness of breath or smothering.
5. Feelings of choking.
6. Chest pain or discomfort.
7. Nausea or abdominal distress.
8. Feeling dizzy, unsteady, light-headed, or faint.
9. Chills or heat sensations.
10. Paresthesias (numbness or tingling sensations).
11. Derealization (feelings of unreality) or depersonalization (being detached from
oneself).
12. Fear of losing control or "going crazy."
13. Fear of dying.
Note: Culture-specific symptoms (e.g., tinnitus, neck soreness, headache, uncontrollable
screaming or crying) may be seen. Such symptoms should not count as one of the four required
symptoms.
Page: 4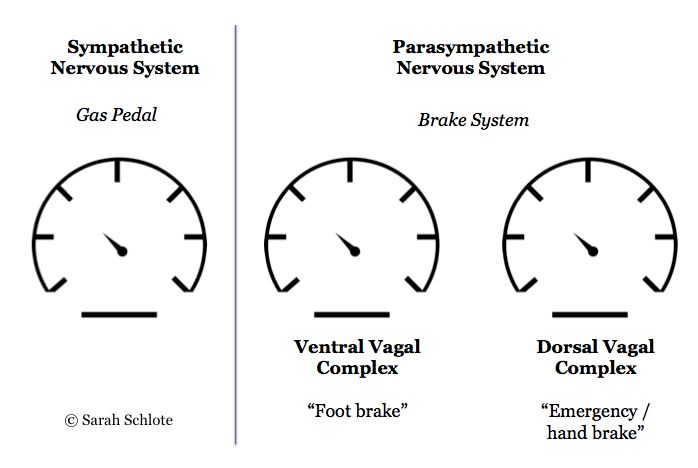
The different meanings and concepts of “Anxiety”
No. 1 – A model of tension and relief.
“Anxiety - the feeling which arises when a conscious or unconscious tension is stirred up and seeks a
method of relief” Berne (1947/1969) p 398
Here Berne is describing Anxiety as a feeling – that manifests when there is psychic tension. We could
think about this idea around energy, cathexis and perhaps Impasse theory?
No. 2 – Anxiety as Process / Anxiety as Response.
Friedman, M. & Shmukler, D. (1982) Transactional Analysis Journal. Vol. 12, No. 2. An Integration of
Major Theoretical Aspects of Anxiety, Creative Behaviour, or Rackets.
IN ADULT LIFE, EXPOSURE TO ANY SIGN OF
POTENTIAL MUTILATION OR ANNIHILATION WILL
TEND TO REACTIVE THE SEEMINGLY OUTGROWN
PATTERNS OF EMOTIONAL RESPONSE WHICH HAD
ORIGINALLY BEEN ELICITED AND REINFORCED
DURING THE STRESS EPISODES OF EARLY
CHILDHOOD.
Is anxiety a response to a stimulus, or is it a more complex process in itself? Response is identified as
a conditioned response resulting from a traumatic experience. This would fit with a model of early
conditioning and early childhood decision making.
Process is seen as having a “mediating and motivating function”. Faced with a situation requiring
creativity or problem solving the response of the person will depend on their cognitive interpretation
of effectiveness in achieving the desired outcome.
This article also contains an interesting quote by Janis (1958 – book – Psychological Stress)
So we could see that Anxiety clearly a manifestation and re-enactment of Life Script – a learnt way of
behaving in early life that has been “blessed and commissioned” and reinforced by potent caregivers?
No. 3 – Defensive Response in the Psychoanalytic Model.
James and Chang draw on psychoanalytic thinking and identify anxiety as a defensive response when
1) self-image is threatened in some way.
2) Achieving recognition or acceptance is hindered
3) There is conflict between the need for love and expression of hostility
Page: 5No. 4 - Is anxiety an authentic feeling?
Functions of Authentic Feelings Thompson (1983)
Table below identifies the feeling, the event or stimulus it deals with and the associated timeframe.
Feeling Deals with Time frame
Anger Intrusion/Damage Present
Sadness Loss Past
Fear Danger Future (imminent?)
Happiness All ok Any
This article is in the tradition of classical TA, it looks at ideas around emotional literacy, the different
functions of feelings and how they motivate problem solving.
No. 5 – The Anxiety Equation
Work by Christine Padesky (CBT)
If you think of an equation where you have A = and A is anxiety, and then you have a ratio. And on the
top line of the ratio, you have over overestimation of danger, and on the bottom line, you have
underestimation of coping and resources.
Now it is important to be anxious without our estimation of danger being greater than our estimations
of our ability to cope or the resources available to help us cope. For example, if you were approaching
a roller coaster, you might see there being a certain amount of danger, but if you think the safety
mechanisms in place and your abilities to cope with the thrill of the ride are great enough, you're going
to feel excitement and not anxiety.
But if you approach that roller coaster, and you think there's danger there, and you've recently read
about safety errors and roller coasters going off the tracks and this and that, and you're thinking, oh
my gosh, if that happens, I wouldn't know what to do. I don't know how to cope, you're going to feel
anxious.
So, it's that relationship between estimations of danger – which we know when we get anxious, we
tend to overestimate; and the closer we get to something we're afraid of, the more we overestimate
danger. And we also, in dangerous situations, underestimate our ability to cope and the resources
available to us.
Page: 6So that is kind of a framework for thinking about anxiety because, in terms of treatment methods, we
can either work at reducing people's sense of danger, or we can work at increasing people's confidence
that they can cope and awareness of resources that can help them. That's a general kind of model of
working with anxiety. Christine Padesky.
Page: 7Page: 8
Page: 9
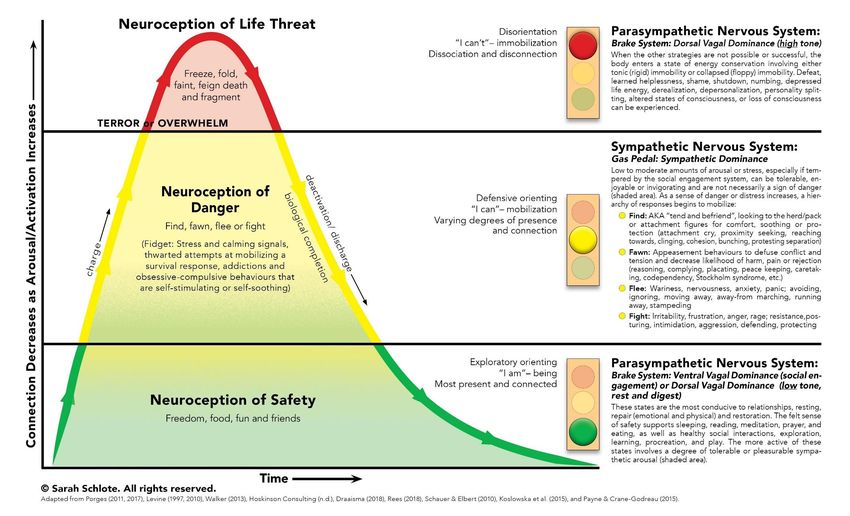
POLYVAGAL THEORY & PSYCHOEDUCATION
The author of the Polyvagal Theory is Dr Stephen Porges. This theory argues that we come into the
world ready to connect and with our autonomic nervous system as our surveillance system – always
on guard – asking the question “Is it safe?”. This is not perception but NEUROCEPTION, scanning for
cues of safety, danger and life threat.
AUTONOMIC NERVOUS SYSTEM is made up of two main branches, the sympathetic and the
parasympathetic branches and responds to signals and sensations via three pathways each with a
characteristic pattern of response. Through each of these pathways we react in service to our survival.
The sympathetic branch is found in the middle part of the spinal cord and represents the pathway that
prepares us for action. It responds to cues of danger and triggers the release of adrenaline which fuels
the fight or flight response.
In the parasympathetic branch the remaining tooth pathways are found in a nerve called the vagus.
Vegas means wanderer and it's aptly named. From the brain stem at the base of the skull the vagus
nerve travels in two directions downward through the lungs heart diaphragm and stomach and
upward to connect with nerves in the neck throat eyes and ears.
The veigas is divided into 2 parts the ventral vagal pathway and the dorsal vagal pathway. The ventral
vagal pathway responds to cues of safety UN supports feelings of being safely engaged and socially
connected. In contrast the dorsal vagal pathway responds to cues of extreme danger. It takes us out
of connexion, out of awareness, and into a protective state of collapse when we feel frozen numb
dissociated or we have flopped to the ground then the dorsal vagus has taken control.
The most ancient pathway is the dorsal vagal pathway of the parasympathetic branch. The
sympathetic branch and its pattern of mobilisation was next to develop. The most recent addition the
ventral vagal pathway of the parasympathetic branch brings patterns of social engagement that are
unique to mammals.
When we are firmly grounded in our ventral vagal pathway, we feel safe and connected calm and
social. A sense of danger can trigger us out of this state and backwards on the evolutionary timeline
into the sympathetic branch. Here we are mobilised to respond and take action. Taking action can
help us return to the safe and social state. It is when we feel as though we are trapped and cannot
escape the danger that the dorsal vagal pathway pulls us all the way back to our evolutionary
beginnings. In this state we are immobilised. We shutdown to survive. From here, it is a long way back
to feeling safe and social and a painful path to follow
Page: 10Page: 11
CONCEPTULISATION OF THE ANXIETY PROBLEM
Themes Behaviour Thoughts
Danger
Avoidance
What if.....
(failure to learn)
Threat
Self as Vulnerable
Safety Catastrophic
Behaviours Imagery
Weakness
What are the key themes that we identify around anxiety?
What are the key behaviours? – are there more “internal, covert, thinking behaviours?”
What are the key cognitive components?
What if?
What's GAD Worry process
the Specific fears
danger? Phobias
Criticism and rejection
Social Anxiety
Intrusive Thoughts
OCD
Catastrophic misinterpretation of
Panic physical symptoms
Fatal illness.
Health Anxiety
Page: 12Key Helpful Principles when assessing the problem
1. The Principle of managing anxiety, not eliminating anxiety
2. The Principle of approaching the difficulty, not avoiding it. Curiosity.
UNLESS IT IS “THE EDGE OF CLIFFS” YOU
SHOULD BE RUNNING TOWARDS WHAT
FRIGHTENS YOU, AS FAST AS YOU CAN!
APPROACH NOT AVOID
A wise person.
3. Vague assessment = vague treatment. Be as specific as you can
4. What is going through your mind? – NOT – What were you thinking?
5. What is the worst you can imagine?
6. Look for images and memories
7. Pictures, sounds, smells, movement, sense, - danger – vulnerability.
8. Approach rather than avoid.
9. Bring anxiety into the room – heighten not flatten
10. Search for safety behaviours.
Page: 13BERNE’S FOUR STAGES OF CURE: TREATMENT PLAN FOR ANXIETY
Stage of Cure Therapeutic interventions. Facilitating Client in:
Symptomatic relief:Historical information on family - alert to Strengthening Adult.
potentially significant experiences.
Client gains some Assessment using Script System.
Adult control over Provide information on:
symptoms • Information about physiology of anxiety
• Relaxation techniques
• General mental health and well-being
assessment – exercise, nutrition,
stimulants, sleep.
• Support networks and encouragement to
seek help and reassurance.
• Coping strategies.
Cognitive work around thought triggers.
Social control: Explore beliefs about self, others and the world. Strengthening Adult
Identify contaminated beliefs – Parent prejudice Decontaminating Adult
Decontaminates and Child delusions.
Adult Facilitating Decontamination
Closes Escape Structural analysis to identify ego state content.
hatches. What are the Parent Contaminations – beliefs
about fear and the future.
Parent beliefs around ability to provide protection
around the fear. The person may not have had
the opportunity to integrate information about
the function of fear re danger and the possibility
of coping in the presence of fear.
Adult diminished abilities for attention, reasoning
and evaluating and remembering
Repetitive thoughts about danger, such as sudden
death, physical catastrophe striking a loved one,
fainting in public, humiliating situations, cardiac
accidents or a situation in which the person is
criticised or rejected.
In my reading Child contamination – archaic
responses or “delusions” (more severe) seen as a
major contributing factor – for example fear of
being afraid, catastrophic perception, anxiety
producing images.
Normalising feelings and emotional literacy work
Strategies for self-care and self-soothing.
Page: 14Explore and confront fantasies.
Making sense of the experience and of the
physical sensations – thinking of clients who have
somatic disorders who are not able to recognise
the feelings and misinterpret them as disease
Identifying the Reinforcing memories
Escape hatch closure
(fear might destroy me or drive me crazy) possibly
Suicide hatch open
Particularly important in working with clients who
experience anxiety due to nature of beliefs about
fear and panic – often clients are afraid of fear
itself.
Eg in having panic attacks believe will go crazy,
have heart attack, faint choke etc.
Need to put in protection for Child who is not
protected by Parent to take a decision that this
will not happen.
Transference cure: Permission to feel as they do/be who they are.
Introjects new Parent
messages from
Introjects new Explore experience and content of significant therapist
Parent messages memories Builds a new robust
from therapist Facilitate expression of authentic feelings positive nurturing and
positive controlling
Parent.
A new experience of
security from the
therapist.
Script cure Exploration of model of attachment – how does Expression of unmet
De confuses Child the person to make themselves feel safe. child needs and de
ego state Exploration of unmet needs from childhood/Child confusion of Child.
Resolves Impasses confusion - the need for safety and security. Realises creates own
Makes a redecision Impasse work. security.
Page: 15THE SCRIPT (RACKET) SYSTEM
Erskine, R. & O’Reilly-Knapp,M. (2010) Erskine R., & Zalcman, M.J. (1997)
THE SCRIPT SYSTEM
SCRIPT BELIEFS/FEELINGS SCRIPT DISPLAYS REINFORCING MEMORIES
Beliefs about: Observable Behaviours Current Events
(stylised,repetitive)
Self Old Emotional Memories
Others Reported Internal Experiences
(somatic ailment, physical sensations)
Quality of Life
Fantasies Result of Fantasies
The best that could happen
The worst that could happen
(Intrapsychic Process)
(Provide evidence and justification)
Needs and Feelings
Repressed at the time of the Script decision.
Page: 16THE SCRIPT SYSTEM
SCRIPT BELIEFS/FEELINGS SCRIPT DISPLAYS REINFORCING MEMORIES
Beliefs about: Observable Behaviours Current Events
Self Agitation and restlessness (8) Parental illness (1)
I’m a worrier (7) Over working. (6) Bereavement.(1)
I don’t cope well with life. (7) Checking for health or illness Problems with family.(5)
I have to get things right to be (7) Relationship problems. (3)
ok (8) Visits to doctor to check out Social Environment
My needs are not important symptoms. (7) Stress at work. (4)
compared to others. (8) Panic attacks. (3) Family responsibilities. (4)
I have to keep others happy. (4)
I don’t know how to feel safe (7) Old Emotional Memories
Reported Internal Experiences Illness/accident or injury. (4)
Others (somatic ailment, physical Bereavement (3)
Cope much better with feelings sensations) Threat of danger (1)
and get on better in life. (7) Headaches, stomach pain, Parents worrying. (6)
Need me to protect them. (4) back pain– somatisation (5) Being given too much
Need me to make them happy. Feeling sick, racing heart, responsibility (6)
(5) muscle tremors, sweaty palms Repeated criticism. (4)
I need others to make me feel (5).
safe.(5) Panic (4)
Pain/discomfort in body. (5)
The World. Poor concentration. (3)
Is scary, threatening and Low self-confidence (6)
uncertain. (6)
(Intrapsychic Process)
Repressed feelings Fantasies Result of Fantasies
Sadness (8) I have a fatal illness. (3) I will die eventually. (3)
Anger (8) I will have a panic attack and I have panic attacks but I don’t
die. (2) die – yet...(3)
I will start to get anxious and I get anxious and eventually
not be able to calm down. (5) calm down. 95)
Someone will find the answer No one is able to help me.
to what is wrong with me and I feel worse - keep having
tell me what to do. (5) panic/anxiety attacks. (3)
I’m going crazy. (4)
Repressed Needs
Need for security (7)
Need for emotional regulation
(5)
To rely on someone (5)
To be a child (7)
To make mistakes and it be ok
(7)
To be important (7)
Page: 17Eight clients presenting with generalized anxiety. i
i
Eight clients were:
1) GP surgery then PP female 30s N. Irish
2) Female 60’s referred from GP strong health anxiety death of father early illness and giving birth
trauma
3) Female 50’s health anxiety recent death of mother and brother
4) Male 30’s somatic back pain and anxiety. Death of sibling when a child, Mum attempted suicide,
single parent family lots of responsibility
5) Female 20’s, modelled from Mum, anxious sister, childhood accident
6) Female late 20’se30s. parental separation when young, controlling and critical parent.
7) Male 40’s difficult birth, friend involved in car accident, teenage S.ab.
8) ??
EXISTENTIALISM
“Existential psychotherapy is a dynamic approach to therapy which focuses on concerns that are
rooted in the individual’s existence.”
Yalom, Irvin Existential psychotherapy. Basic Books, 1980.
Existentialism is a philosophy that emphasizes the uniqueness and isolation of the individual
experience in a hostile or indifferent universe, regards human existence as unexplainable and stresses
freedom of choice and responsibility for the consequences of one’s acts.
American Heritage Dictionary of the English Language, Third Edition © 1992 by Houghton Mifflin
Company
Existentialism is a philosophical system which sees meaning as something that is constructed internally
rather than a knowable externally intrinsic thing and therefore each person is responsible for their
own life and their own construction of meaning in the world. The resulting responsibility and freedom
this generates gives rise to deep dread and existential anxiety.
Death and Existential Psychotherapy
The physicality of death destroys us, the idea of death saves us.
Yalom 1980
Death (annihilation) anxiety is our absolute primal fear
We construct defences to deal with this primal anxiety. ‘Death is a… primary fount of psychopathology’
(Yalom 1980. p29)
Death is the condition that makes it possible for us to live life in an authentic fashion (p.31)
Draws on the ideas of Heidegger in his discussion of how we death can be the stimulus for us to move
to a different state of existence.
Heidegger saw that we had two modes of existence:
1) A state of forgetfulness of being
2) A state of mindfulness of being
Page: 18Fully embracing death can ‘promote a truly authentic immersion in life’ (p187)
Yalom identifies a number of key life events that can stimulate unconscious death anxiety - beginning,
committing to, or ending relationships, births, deaths, job changes, children leaving home etc
Yalom identifies two primary defences against death anxiety: Specialness and Ultimate Rescuer
fantasies.
Specialness can lead us to compulsive rescuing, workaholism, grandiosity and is often expressed as
narcissism.
Death anxiety can be temporarily soothed, or avoided by ‘Santa Claus fantasies’- scripts which
perpetually seek Rescuers.
Individuation can propel people into direct conflict with their death anxiety. Death reminds us of our
limitations.
Freedom and Responsibility
We are all condemned to freedom (Sartre)
Awareness of our freedom, self-creation and need to take full responsibility can lead to a situation of
‘groundlessness.’
Yalom says that in its existential sense freedom refers to absence of external structure.
“the individual is entirely responsible for - that is, the author of – his or her own world, life design,
choices and actions.”
This fundamental freedom confronts us with existential isolation.
The extent to which we are unaware of those forces which influence us, we are controlled by them
(drives, instincts, the unconscious, environment, oppression etc) Otto Rank
Self-awareness requires a striving to become aware of these influences on our freedom and to accept
the anxiety our freedom generates. It is only through knowing ourselves that we can truly be in
relationship with others
Conformity can be a way of avoiding freedom and responsibility. Uncritical allegiance to beliefs,
perspectives and values (religious, political, theoretical) renders individuals no longer authentic.
Our clients will often seek us to make decisions for them, soliciting advice and so forth. Beginning
therapists often fall into the trap of suggesting courses of action, thus allowing clients to avoid
responsibility.
Acceptance of responsibility for what we have done to contribute to our situation in life is central.
Isolation
Yalom identifies three types of isolation:
Interpersonal Isolation Loneliness, isolation from others
Intrapersonal Isolation Fragmentation & dissociation from aspects of the self
Existential Isolation The realisation that ultimately we face the world alone
Facing and accepting our Isolation can provoke deep anxiety but can also be a liberating process.
Page: 19‘To care for another means to relate in a selfless way: one lets go of self-consciousness and self-
awareness; one relates without the overarching thought, what does he think of me? Or, what’s in it
for me? One relates in the moment solely to the other person… with one’s whole being’ (Yalom 1980
p373)
‘If one relates selflessly, one is free to experience all parts of the other rather than the part that serves
some utilitarian purpose… To care for another means to care about the being and growth of the
other… one endeavours to help the other become fully alive in the moment of encounter… caring is
reciprocal. To the extent one truly ‘turns toward the other’ one is altered. To the extent one brings
the other to life, one also becomes more fully alive’ (Yalom p373)
Individuals with deep isolation anxiety believe they need others. They long for fusion reaching out
because they believe they have to rather than because they want to.
Meaning and Meaninglessness
We are condemned to meaning (Merleau-Ponty)
We live in a meaningless and irrational universe and our search for order and meaning often brings us
into conflict
Existential Vacuum - this occurs when a person enters an experience of doubt over the meaning of
their life.
We need models and organisational structures to make sense and meaning of the world
These structures by definition force oversimplification of abstract concepts.
‘Making sense’ increases an individual’s sense of control, reduces anxiety, offers reasons, explanations
and reduces our sense of aloneness.
Therapeutic Objectives in Existential Psychotherapy
Death: Do we in our ‘humanistic positivity’ sometimes encourage an unrealistic optimism which robs
clients of opportunities for adjusting to death?
The “existential” therapist’s task is to repeatedly expose their clients to their fear of death. It is often
useful to dissect the fear into its component parts - fear of helplessness, pain etc.
Freedom : The therapist needs to be mindful of the double message inherent in some methods of
therapy- ‘Assume responsibility the patient is told… and I’ll tell you precisely how, when and why to
do it’ (Yalom p250)
Yalom believes group process can provide a unique opportunity to promote responsibility assumption.
Individuals move through the following sequence:
1) Learning how our behaviour is viewed by others
2) Learning how our behaviour makes others feel
3) Learning how our behaviour creates the opinions others have of us
4) Learning how our behaviour influences our opinions of ourselves
‘The therapist helps the patient realise that not only is the individual responsible for his situation but
that only he is responsible. The corollary of this realisation is that the individual is also solely
responsible for the transmutation of his or her world’ (Yalom, 1980. p292)
Page: 20Isolation: and Psychotherapy
The task of the therapist is to help the client recognise what they do in their relationships with others
to promote or prevent ‘real, mature, need-free relating’.
Some clients need help in learning how relationships can enrich their inner world, what true
connection feels like and the inherent value of relating. Some clients may need to learn what they can
and cannot get from relationships. Therapy can also assist clients in facing and acknowledging their
existential isolation
Page: 21You can also read