All that blacks out is not syncope: a neurological view of transient loss of consciousness - Dr Simon Taggart Consultant Clinical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

All that blacks out is not syncope:
a neurological view of transient
loss of consciousness
Dr Simon Taggart
Consultant Clinical Neurophysiologist.
JCUH, Middlesbrough.

Misdiagnosis of Blackouts • Sutula 1981: 20% of patients with refractory epilepsy in tertiary centre had non-epileptic seizures • Smith et al 1999: 25% of patients referred to tertiary epilepsy centre had non-epileptic seizures. • Zaidi et al 2000: alternative diagnosis found in 36% of patients on anti-epileptic drugs

Mortality in Blackouts
• Increased in syncope
– At 5years, 50.5% in cardiac syncope, 24.1% in syncope of unknown
cause
• Increased in epilepsy
– SMR 2.1(1.8-2.4)1, 2.3(1.9-2.6)2
– Related to cause of epilepsy (eg brain tumour)
– Directly or indirectly from epileptic seizures (status epilepticus,
accidental drowning)
– SUDEP: Sudden, unexpected, witnessed or unwitnessed, nontraumatic
and nondrowning death in patients with epilepsy with or without
evidence for a seizure, and excluding documented status epilepticus, in
which post mortem examination does not reveal a (structural or
toxicologic) cause for death.
1. Lhatoo et al Annals of Neurol 2001: 49(3); 336-344 2. Hauser et al,
Epilepsia 1980: 21(4); 399-412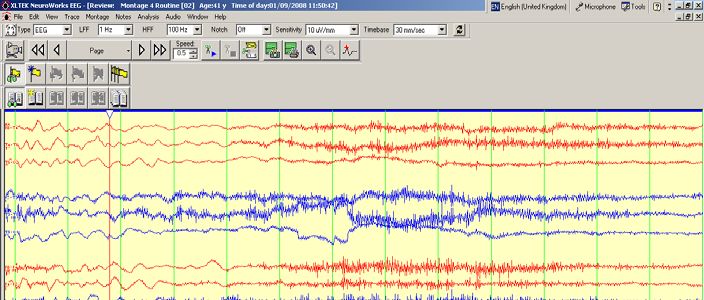
Differential diagnosis of Blackouts
(non-exhaustive)
• Syncope
• Epilepsy
• Psychogenic non-epileptic seizures
• Cataplexy
• Transient CSF obstruction
• Transient ischaemic attack - anterior and posterior
circulation
• Panic attack
• Falls
• Hypoglycaemia
• Basilar migraine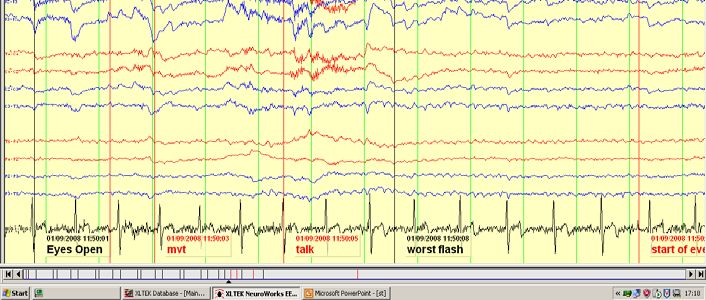
Blackouts – clinical diagnosis:
individual attacks
• Subjective account
– 12 hours before, several hours after
• 1st hand witness accounts
– Second by second account
– Ban medical jargon from descriptions
– Strip out second hand descriptions
– First worst and last episodes
• 2nd hand accounts
– Much less informative, much more misleading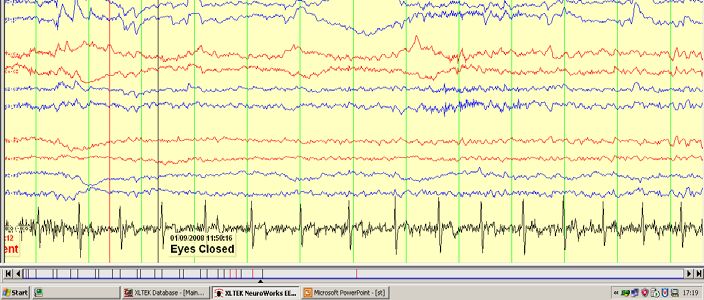
Syncope v GTCS
During blackout Syncope Generalised tonic clonic
seizure
Pallor Common Rare
Cyanosis Rare Common
Duration of loss of 60seconds
consciousness
Movements A few clonic or myoclonic jerks; Prolonged tonic phase (~30
brief tonic posturing (few sec), then prolonged rhythmic
seconds); duration 1 min
consciousness
Lateral tongue biting Rare Common
Hypersalivation Rare Common
EEG Generalised slowing Ictal EEG pattern
Adapted from Hirsch L, Ziegler D, Pedley T. Seizures, syncope and their mimics
In: Rowland L, ed. Merritt’s Neurology, 11th ed. New York: Lippincott Williams & Wilkins; 2005:13–20.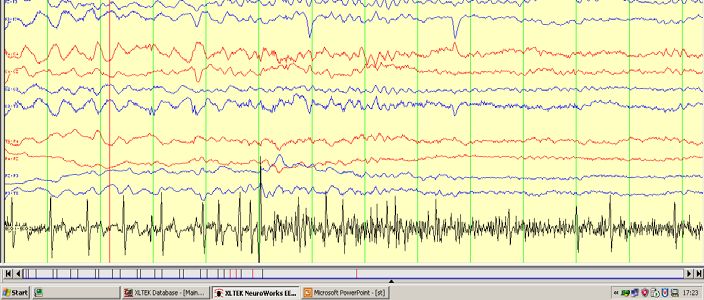
Syncope v GTCS
After blackout Syncope Generalised tonic
clonic seizure
Confusion/disorientation Rare;
Epileptic Seizures The clinical manifestation of excessive and/or hypersynchronous, usually self- limited abnormal activity of neurones of the cerebral cortex
Generalised tonic clonic seizures
• No relation to posture, uncommonly precipitated
• Rigid collapse with LOC: bilateral posturing/rigidity of limbs and
trunk – tonic phase ~20-30 seconds
• Strong rhythmical jerking of limbs – often more apparent in arms
than legs – clonic phase ~1-3mins, gradually slows before stopping
• Deep unconsciousness immediately after jerking stops ~ 30
seconds+
• Gradual recovery of orientation characterised by confusion,
amnesia for early period of recovery, agitation - >5minutesSyncope Abrupt, transient and self-limiting loss of consciousness associated with loss of postural tone, caused by a sudden fall in cerebral perfusion
Convulsive syncope • Limp collapse with LOC – Motor features usually delayed by seconds – Brief tonic phase – Brief myoclonic phase – Brief clonic phase • Rapid recovery of consciousness • No amnesia for early stage of recovery (NB sometimes in elderly) • May be precipitated, related to posture, associated with prodrome but may not.
Other neurological mimics of syncope Epileptic • Tonic seizures • Atonic seizures Psychogenic non-epileptic attacks Transient CSF obstruction Posterior circulation TIAs Meniere’s disease Cataplexy
3rd Ventricle Posterior Fossa Craniocervical Junction
Neurological mimics of epilepsy Intermittent CSF obstruction Causes: Third ventricular tumours, posterior fossa tumours, Chiari malformations Symptoms: Headache associated with cough, brainstem symptoms: vertigo, ataxia, drop attacks Posterior circulation TIAs Drop attacks may occur in isolation May be independent history of attacks of ataxia, vertigo, unilateral, bilateral upper limb dysaesthesia +/- occipital headache Meniere’s disease: Episodic fluctuating rotational vertigo, deafness tinnitus, aural fullness; Severe rotational vertigo can cause drop attacks.
Cataplexy • Occurs as part of symptom complex of narcolepsy: excessive daytime sleepiness, sleep paralysis, cataplexy, hypnagogic hallucinosis • Cataplexy: episodes of loss of postural tone triggered by emotion-laden situations, consciousness preserved,
The appropriate use of
investigations
• Detailed clinical evaluation - repeated
• Video – detailed review
• ECG
• U&Es, glucose (in acute situation)
• Brain imaging
Only then…
• Routine and sleep EEG
• Long-term EEG monitoring
• Tilt tableThe problem with EEG
‘routine interictal EEG is one of the most
abused investigations in clinical medicine
and is unquestionably responsible for
great human suffering.’
David Chadwick 1990Electroencephalography
• 1929 - EEG first recorded form humans in by Hans Berger
• 1957 - Gastaut demonstrated that EEG can differentiate syncope
from epilepsy
• Interictal epileptic discharges associated with clinical diagnosis of
epilepsy
• BUT only 29-55% with diagnosis of epilepsy have abnormal routine
EEG, 0.5% of 17-24 year olds without epilepsy have interictal
epileptic discharge
• Some interictal abnormalities aid in prediction of further seizures3 but
not all
• Abnormalities increase in elderly and with learning disability and in
chronic psychosesFp2-AVG
Fp1-AVG
F8-AVG
F4-AVG
Fz-AVG
F3-AVG
F7-AVG
T4-AVG
C4-AVG
Cz-AVG
C3-AVG
T3-AVG
T6-AVG
P4-AVG
Pz-AVG
P3-AVG
T5-AVG
O2-AVG
O1-AVG
100 µV
1 secElectroencephalography
• Appropriate use of EEG in epilepsy
– To stratify the risk of further epileptic seizures after a single epileptic
seizure
– To classify epilepsy
– When no witness account
– When reviewing diagnosis
– Diagnosis of non-convulsive status epilepticus and convulsive status
epilepticus
• Use routine EEG +/- natural drowsiness
• Long-term EEG if routine EEG doesn’t provide all answers
– Ambulatory EEG for interictal epileptic discharges: sensitivity 80%
– In-patient video-EEG: event capture rate 70%Cardiac effects of epileptic seizures
- and vice versa
• Ictal sinus tachycardia in greater than 90% of seizures:
– Keilson et al Arch Neurol 1989: 46: 1169-70
• Ictal bradycardia or asystole in less than 1% of cases
– Rocamora et al: Epilepsia: 2003:44: 179-185
– Scheule et al: Neurology: 2007: 69: 434-441
– Unclear whether pacemaker insertion of benefit
• Cardiac arrhythmias documented in SUDEP
– Reduced heart rate variability documented in patients with SUDEP
compared to control group – heart rate variability reduced in refractory
temporal lobe epilepsy: Ansakorpi et al: JNNP: 2002: 72: 26-30
• EEG/ECG evidence of hypoperfusion induced epileptic seizuresWilliam Gowers Hans Berger Henri Gastaut
You can also read