An Evaluation of Connectivity Tables in Waterloo Region
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

An Evaluation of Connectivity Tables
in Waterloo Region
Evidence Insight Action
What is the Connectivity Table?
Connectivity is based on a Community Mobilization Hub Model originating in Prince Albert, Saskatchewan.
The model is a multi-disciplinary, interagency approach to addressing situations of acutely elevated risk on a
case-by-case basis. Locally, each table brings health, social, and justice services together at a weekly meeting to
collaboratively and proactively address situations of elevated risk.
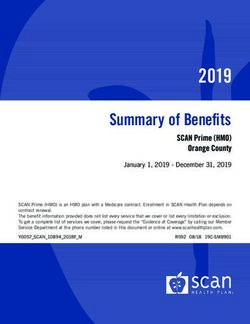
How Does the Connectivity Table Work?
Connectivity Tables work through an intentional 4 filter model using de-identifying information at their weekly
meetings to assess and respond to acutely elevated risk. The following diagram illustrates the process.
UP TO 30 AGENCIES
IN ATTENDANCE
WEEKLY MEETING
PRESENTING OF
SITUATIONS OF
ELEVATED RISK
IDENTIFY AGENCIES
TO COLLABORATE
SHARE
INFORMATION
AND RESOURCES CONNECT INDIVIDUALS
WITH SERVICES
INITIATE A RESPONSE
WITHIN 24-48 HOURS
1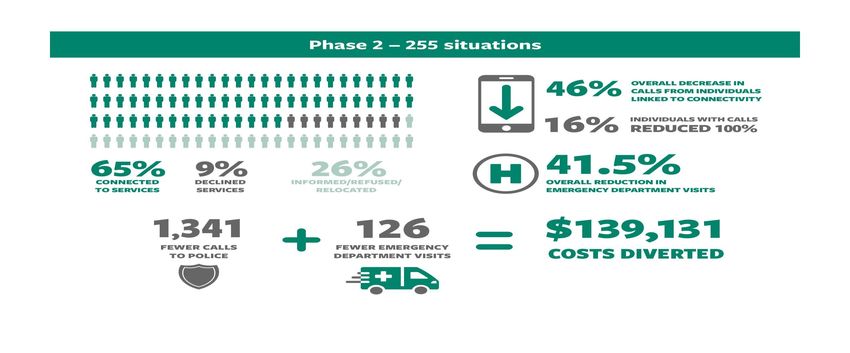
An Evaluation of Connectivity Tables in Waterloo Region 2017
How Did the Waterloo Region Connectivity Tables One of the things that I think that
Get Started? makes the Table work is people
In January, 2014, the Waterloo Regional Police Service (WRPS), in partnership come from their organizations, but
with Langs, adapted and implemented Connectivity, a “Situation Table” in Cam- when that case gets put forward,
bridge-North Dumfries (CND). In partnership with Carizon Family and Commu- that’s who we look at first. We look
nity Services, a second Situation Table became operational covering Kitchener, at those risk factors and we’re not
Waterloo, Wellesley, Wilmot, and Woolwich (KW4) in October 2014. Together, looking at do they fit my criteria,
these two tables are known as Connectivity Waterloo Region. would they fit into our agency–you
know? …We decide who can be of
Why Evaluate Connectivity Tables? best help, not whether or not it’s my
job… Those silos drop, and it’s like
The expected outcome of the Connectivity Table is that individuals are connect- we work for one agency, but we’re
ed to services. However, we know through experience that Connectivity Tables bringing our expertise and our re-
have a greater impact on individuals, families, organizations and the system. With sources… And that’s the way it really
the number of tables established in Ontario, it was timely to look at their impact should be, because if one agency
and develop an evaluation framework that could be replicated for other situa- could handle them, they wouldn’t be
tion tables. Two evaluations were undertaken in Waterloo Region completed by coming here. We need to step up. We
Taylor Newberry Consulting. A Steering Committee helped guide the evaluation can’t allow the clients to fall between
process and input was sought from table members about the evaluation. the cracks. – Connectivity Table
Member, Phase 1 Evaluation
What was the Methodology Undertaken to
Evaluate Waterloo Region Connectivity Tables?
Project Design and Evaluation Methodology
Phase 1 Evaluation Phase 2 Evaluation
An analysis of police calls for service data pre and An analysis of hospital service usage data, including
post Connectivity Table interventions emergency department use, in-patient admissions,
and length of stay. Analysis examined trends
and changes pre and post Connectivity Table
interventions
Key informant interviews with table members and Interviews with service users/clients connected to
external stakeholders services to gather first-hand experiences regarding
the impact of the Connectivity Tables.
Focus groups with table members An analysis of police calls for service data pre and
post Connectivity Table interventions
Key informant interviews with table members and
external stakeholders
There has been absolutely no more contact with police, no more issues in the community, complete stability, housed, healthy, still on medica-
tion, and still followed by a lot of the supports that were put into place as a result of coming to Connectivity. – Connectivity Table Member,
Phase 2 Evaluation
2
An Evaluation of Connectivity Tables in Waterloo Region 2017
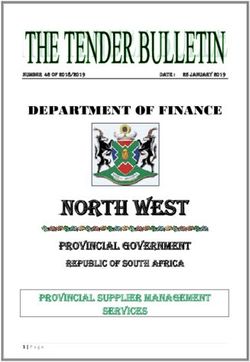
Connectivity Table Process and Expected Outcomes
Connectivity Team Forms • Analysis of presenting needs and risk
• Establish service roles and contact plan
Initial Intervention • Service consent and engagement
• Emergency Department diversion
• Hospitalization
• Service plan created
Outreach and Risk Reduction • Eviction prevention • Connections to services
• Income security made:
• Medication compliance - Psychiatry
‘I just wasn’t taking my medication when I lived • Removal to safety - Primary Care
with my mom. I was skipping some meds I proba- • Clarity of needs and - Support Coordination
bly shouldn’t have skipped, which I realized after appropriate services - Counselling
I moved out how much they actually help and how
- Peer Support
much they don’t actually hurt me” – Connectivity
Table Client, Phase 2 Evaluation
Evaluation Questions
The Phase 2 evaluation focused more heavily on outcomes. The following key evaluation questions guided Phase 2:
• To what extent do individuals engage with the supports and services developed and implemented by Connectivity?
• What new services and supports do individuals access to meet their needs?
• What are individuals’ experiences with new supports and services? Are they experienced as beneficial and
helpful? In what ways? How can services be improved?
• What changes are observed in people’s lives? To what extent are stability and wellness promoted? How is risk
mitigated or removed?
• To what extent have interventions by Connectivity influenced the frequency and duration of emergency
department visits and hospital admissions among Connectivity users?
• To what extent have interventions by Connectivity influenced the frequency of police service calls among
Connectivity users?
“We do have a lot of people in our community who won’t actually be helped if you don’t have
somebody going to the door … the point of Connectivity isn’t just to give them a business card and
say, call me if you want some help. It’s to grab a hold of their arm and look at them in the eye and tell
them, “you need help and here it is”. There aren’t too many agencies out there who do that sort of
work, so for us to round up in groups and go do that, I think is very unique.” – Community Partner
3
An Evaluation of Connectivity Tables in Waterloo Region 2017
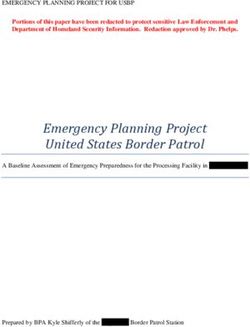
Connectivity Table Outcomes… By the Numbers
Phase 1 – 89 situations
74%
74%
74%
74%
OVERALL
74%
OVERDECREASE
CALLS
CALLS
LINKED
ALL DECREASE
FROM
LINKED
OVERALL
FROM
OVERALL
IN IN
INDIVIDUALS
INDIVIDUALS
TO CONNECTIVITY
TO CONNECTIVITY
DECREASE
DECREASE
IN IN
21%
21%
CALLS
CALLS
FROM
OVERALLFROM
INDIVIDUALS
INDIVIDUALS
DECREASE IN
LINKED
LINKED
TOFROM
CALLS CONNECTIVITY
TO CONNECTIVITY
INDIVIDUALS
76%
76%1313%
% 1111%
%
LINKED TO CONNECTIVITY
CONNE
76%
76%
CONNECTED
CTED
13%
76% 13%
13% 11%
TO SERVICES
11%
TO SERVICES
11%
DECLINED
DECLINED
SERVICES
SERVICES
INFORMED
INFORMED/REFUSED/
/ REFUSED/
RELOCATED
RELOCATED 21%
21%
21%
INDIVIDUALS
INDIVIDUWITH
REDUCED
REDUCED
100%
INDIVIDUALS
ALS WITH
100%
INDIVIDUALS
WITH
CALLS
WITH
CALLS
CALLS
CALLS
REDUCED
REDUCED 100%100%
CONNECTED
CONNECTED DECLINED
DECLINED INFORMED/REFUSED/
INFORMED/REFUSED/ INDIVIDUALS WITH CALLS
REDUCED 100%
CONNECTEDSERVICES
TO SERVICES
TO SERVICES DECLINED
SERVICES INFORMED/REFUSED/
RELOCATED
RELOCATED
Phase 2 – 255 situations
TO SERVICES SERVICES RELOCATED
46%
46% OVERALL
OVERALL
CALLS
DECREASE
CALLS
LINKED
FROM
LINKED
DECREASE
FROM
IN IN
INDIVIDUALS
INDIVIDUALS
TO CONNECTIVITY
TO CONNECTIVITY
46%
46%REDUCED
46%
16%
16% REDUCED
OVERALL
OVERALL
DECREASE
INDIVIDUALS
100%
100%
DECREASE
INDIVIDUALS
LINKED
LINKED
TO TO
LINKED
WITH
IN IN
OVERALL DECREASE IN
CALLS
CALLS
FROMFROM
INDIVIDUALS
INDIVIDUALS
WITH
CALLS
CONNECTIVITY
TO
CALLS
CALLS FROM INDIVIDUALS
CONNECTIVITY
CONNECTIVITY
16%
16%REDUCED
16%
INDIVIDUALS WITH
INDIVIDUALS CALLS
WITH CALLS
41.5%
41.5%
INDIVIDUALS WITH CALLS
REDUCED
100%
REDUCED 100%
100%
65%
65% 9%
9% 26%
26%
41.5%
41.5%
41.5%
CONNECTED
CONNECTED DECLINED
DECLINED INFORMED/REFUSED/
INFORMED/REFUSED/ OVERALL
OVERALL
REDUCTION
REDUCTION
IN IN
6565%
%
65%9%
CONNE
9%
9% 26
TO SERVICES
26%
%
26%
TO SERVICES
CONNECTED
CONNECTED
CTED
SERVICES
SERVICES
DECLINED
DECLINED
RELOCATED
DECLINED INFORMED
RELOCATED
INFORMED/REFUSED/
INFORMED/REFUSED/
/REFUSED/
EMERGENCY
EMERGENCY
OVERALL
OVERALL
DEPARTMENT
DEPARTMENT
ALLREDUCTION
OVERREDUCTION
VISITS
IN ININ
REDUCTION
VISITS
1,1341
,341 126
126 $139,131
$139,131
TO SERVICES
TO SERVICES
TO SERVICES SERVICES
SERVICES
SERVICES RELOCATED
RELOCATED
RELOCATED EMERGENCY
EMERGENCY
EMERGENCY DEPARTMENT
DEPARTMENT
DEPARTMENT VISITS
VISITS
VISITS
1,341
1,1341
FEWER
,341
FEWER
CALLS
TO POLICE
CALLS
TO POLICE
FEWER CALLS
126
126
126
FEWER
FEWER
EMERGENCY
EMERGENCY
DEPARTMENT
DEPARTMENT
VISITS
VISITS
FEWER EMERGENCY
$139,131
$139,131
$139,131
COSTS
COSTS
DIVERTED
DIVERTED
FEWER
FEWER
CALLS
TOCALLS
TO POLICE
POLICE
TO POLICE
FEWER
FEWER
EMERGENCY
EMERGENCY
DEPARTMENT
DEPARTMENT
DEPARTMENT
VISITS
VISITS
VISITS
COSTS
COSTS
COSTS DIVERTED
DIVERTED
DIVERTED
Thanks to our supporters who made this evaluation possible:
Cambridge and North Dumfries
A copy of the executive summary and full report may be accessed at taylornewberry.ca 4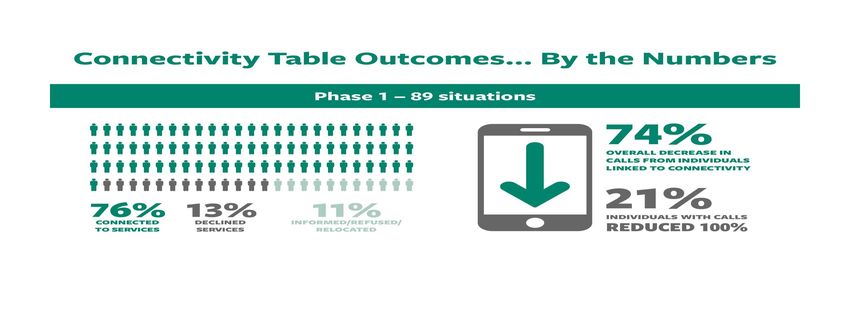
Connectivity Waterloo Region
WWLHIN Presentation
November 14, 2018
What is Connectivity?
• Multi-sectoral model
• Collaboratively and proactively address situations of elevated risk
• Immediately responsive (e.g. same day or next day).
• Long term vision - reduce crime, emergency room admissions,
police calls for service
Background Model introduced to Waterloo Region by WRPS, WWLHIN, and Cambridge Table begins KW4 Table begins WCPC – chaired by Langs – chaired by Carizon Jan 2013 Jan 2014 Oct 2014

Why Connectivity was Needed in Waterloo Region High rates of alcohol use Serious mental health issues High risk of homelessness Growing income disparity Higher youth crime rate 80% of WRPS calls not crime-related

THE CONNECTIVITY TABLE PROCESS

Connectivity Table Members
Health Ministry of Children and Youth Services;
Canadian Mental Health Association; Sexual Assault Domestic Violence Treatment Centre;
Ray of Hope (Youth Addiction Services); Sexual Assault Support Centre;
LHIN Home & Community Care/Elder Abuse Response Team; St. John’s Kitchen/The Working Centre;
Grand River Hospital; Supportive Housing of Waterloo;
Cambridge Memorial Hospital Victim Services Waterloo Region;
House of Friendship – Addictions White Owl Native Ancestry Association;
Community Ward/Health Link; Wilmot Family Resource Centre;
Langs CHC YWCA Kitchener-Waterloo.
Stonehenge;
Justice Services:
Social Services Waterloo Regional Police Service;
Cambridge Self Help Food Bank; Youth Justice Services
Cambridge Shelter Corporation; Ministry of Community Safety and Correctional Services;
Carizon Family and Community Services;
Developmental Services Resource Centre; School Boards
Family and Children Services; Waterloo Catholic District School Board;
Region of Waterloo Social Services, Waterloo Region District School Board
Interfaith Community Counselling Centre;
oneRoof;
LutherwoodCommitment to Working Differently Together
Number of Situations Addressed
2016 2017 Jan to Sept 2018
112 situations 140 situations 97 situations
addressed addressed addressed
78 situations 73 situations 56 situations
mitigated away mitigated away mitigated away
from the table from the table from the tableTop Issues Addressed (2017) Mental Health Physical Health Criminal Involvement Physical Violence Drugs/Addictions Emotional Violence Alcohol Suicide Antisocial Behaviour
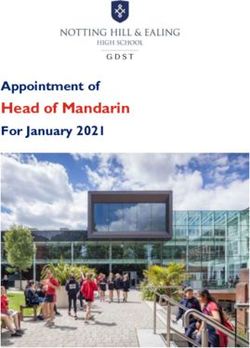
Protective Factors Identified (2017)
160
Number of Protective
Factors Identified
140
120
100
80
60
40
20
0
Total Number Stable Both parents Financial Positive Linked to
of Situations Housing helping with Support Family primary care
childcare Support providerSome Key Milestones to Date 2 External Evaluations 1 International Award 100 Staff and senior leaders oriented about privacy and agreement 69 Guests and visitors from across the province
Connectivity Table Evaluation – Phase 1
Connectivity Table Evaluation – Phase 2
Strategic Links to the LHIN Business Plan Population health approach Addresses health equity Brings together system leaders Improves access to quality, coordinated mental health and addictions services in each sub-region Residents experience impactful change due to the collective impact of community- based initiatives Improved health and wellbeing of the most vulnerable residents across Waterloo Wellington
“I’m doing things way differently because I see real possibility to effect change, whereas before I was just shuffling the same people around. I check into things, knowing we can actually make a difference, whereas before it was…okay, I’ve been to this house 30 times this month, I guess we’ll be there 30 times again next month.” Community Resource Officer, Waterloo Regional Police Service
You can also read