Approvisionnement plus sécuritaire et utilisation de la MLLU Panel interdisciplinaire québécois de discussions - Équipe de soutien clinique et ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Approvisionnement
PROPOSITION plus sécuritaire
et utilisation de la MLLU
Panel interdisciplinaire québécois
de discussions
Équipe de soutien clinique et organisationnel en dépendance et itinérance
1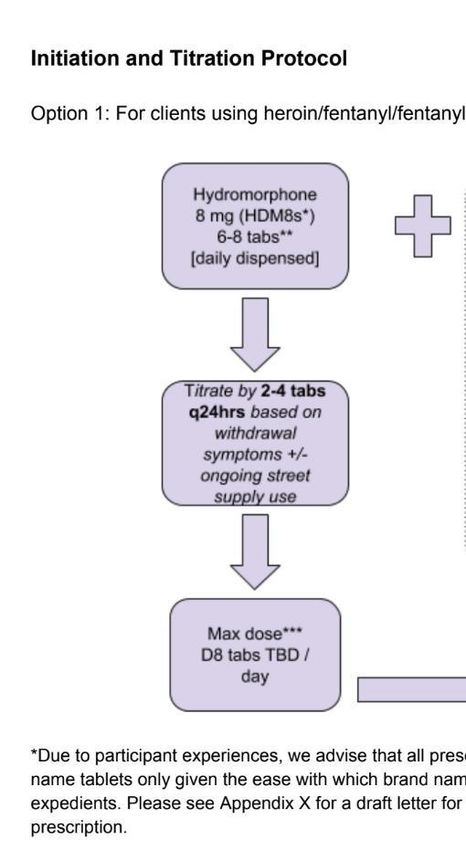
© Équipe de soutien clinique et organisationnel en dépendance et itinérance, 2021
Divulgation de conflits d’intérêts potentiels
Kenneth Wong, directeur Méta d’Âme : Aucun conflit
Sofiane Chougar, infirmier, CHUM : Aucun conflit
Caroline Fauteux, IPS-PL, CIUSSS E CHUS : Aucun conflit
Leslie Chalal, travailleuse sociale, CIUSSS CCSMTL : Aucun conflit
Dre Amanda Violato, médecin, CIUSSS CCSMTL : Aucun conflit
Stéphanie Foucher-Laurent, pharmacienne communautaire : Aucun conflit
2
Regent Park Safer
Opioid Supply
Program
Marysia (Mish) Waraksa RN(EC) NP PHC
Nurse PractitionerNo conflict of interest
Downtown East Collaborative SOS
Program
• Street Health
• Regent Park
Community
Health Centre
• South Riverdale
Community
Health CentreDowntown East Collaborative SOS
Program
Each team consists of:
1 Nurse Practitioner
Primary care, Safer Opioid Supply Prescribing
1 Registered Nurse
Primary care supports, harm reduction, care co-
ordination
1 Community Health Worker
Case management, support with housing, replacing
ID, accessing community resources
Each site has a safe injection site on premisesRole of Nurse Practitioner
NP-led care – autonomous provision of SOS Prescribing and
primary care
Ontario – no restrictions on NP prescribing
Limits to scope of practice at this time: ordering CT/MRI,
completion of some forms (insurance, hearing aid funding),
POC testingReferral & Intake Process
Majority of referrals are internal from safe injection site
staff
CHW & RN run weekly drop-in intake session to screen for
eligibility
If eligible, are booked with the Nurse Practitioner for
intakePrioritization Criteria
Marginalized • Indigenous, black, people of colour
Populations • Women, two spirit, LGBTQ2SI
• Homeless, precariously housed
Housing Status • Living alone
OD History • History of non-fatal overdose
Complications • HIV, Hep C, endocarditis, spinal abscesses,
sepsis, osteomyelitis, prolonged
of Use hospitalization related to useEligibility
Opioid Use Disorder per DSM V
Self-reported regular illicit opioid use
Previous unsuccessful OAT monotherapy, or decline OAT
Positive UDS
No medical contraindication to unsupervised SOS
Severe respiratory, liver disease
Hx GI obstruction or paralytic ileus
Severe CKD
Alcohol use disorder, or unpredictable ETOH intake
Sedative, anxiolytic or hypnotic substance abuseRegent Park SOS Clients
24 clients total have received an SOS prescription
Housing
8 with permanent housing
16homeless, living in shelters, or have precarious
housing
Medical complications
8 with previous hx of treated/cleared HCV
8 with positive HCV RNA at intake
2 coinfected with HCV/HBV
5 hx of endocarditisSOS Dosing
Initial doses
Kadian 100-200mg observed daily
Dilaudid 8mg x 8-12 tabs dispensed daily
Titration
Kadian titrated q48hrs x 100-200mg/day
Dilaudid 8mg titrated q48 hours x 2-6 tabs/day
Maximum doses
Kadian 1600mg
Dilaudid 8mg – 30 tabs dailyDosing – Typical Titration Schedule
Visit Kadian (SROM) Dilaudid 8 mg (# daily
dispensed)
1st visit 200mg 12 tabs
2nd visit 200mg ↑18 tabs
3rd visit ↑400mg 18 tabs
4th visit 400mg ↑24 tabs
5th visit ↑500mg 24 tabsLong Acting Medications
Methadone (5)
Kadian (15)
Suboxone (1)
Hydromorphone
Contin (2)
None (1)Missed doses
If client misses dispensing x 2 days, prescription is held
and prescriber must be contacted
Kadian – decreased per BCCSU SROM Guidelines
Dilaudid – per clinical judgment – working towards a
standardized protocol
Reductions also guided by client’s use patterns – a more
modest reduction may be used if client has high fentanyl
use during period of missed dosesUrine Drug Screening
On enrollment to confirm presence of illicit opioids
On follow up, q~1 Month to confirm presence of SOS
medications in urine
UDS collected unobserved
Emphasis placed on non-punitive approach to UDS
Presence of illicit opioids does not lead to discharge from
programProgram issues
High missed appointment rate
Difficult provider coverage
Client access – lack of phones
Inadequate response to dilaudids
Future alternatives?
Drug shortages
Dilaudid, APO-hydromorphone
Kadian – upcoming?Stigma and interaction with other
providers
Hospitalization
++Difficulties with continuity of care
Dose de-escalation
IV vs. PO dose equivalency issues
Restrictions
in maximum doses of IV dilaudid allowed to
be administered in non-ICU units
Clientshesitant to request PRN doses, or not aware of
availability
Clients frequently leaving “against medical advice” due
to intolerable withdrawal symptomsStigma and interaction with other
providers
Incarceration
++Difficulties with continuity of care
Existing OAT providers
Mixed responses received
Pharmacists
Key partners in SOS program!
Mostly positive responses
Some issues with client experience of stigma and denial
of careSOS Case #1 – Typical Presentation
42yo female, Indigenous, previous long history of homelessness, now in a
rooming house.
History of multiple witnessed non-fatal ODs requiring naloxone and O2
administration
Hx hepatitis C, spontaneously cleared
Was previously on Methadone, up to 80mg, but with frequent missed doses,
only on 30mg at intake
Was using 2 “points” fentanyl IV on intake
Initiated on 200mg Kadian and 8 tabs dilaudid daily
Now on program x 4 months
Dose Kadian 500mg OD and 16 tabs daily
Uses 4 tabs IV or PO – about 50/50 oral and IV dosing
Uses 1-2 points of fentanyl IV/weekSOS Case #2 – High dose SROM
32yo male, LGBTQ, housed
Using 8-10 points fentanyl IV on intake to program
Initiated on 300mg Kadian and 12 tabs dilaudid daily
8 months in program – Kadian 1000mg po od, 28 tabs
Dilaudid daily
Abstinence from fentanyl in the last month
Now taking Dilaudid oral-only
Wishes to stay on current SOS doses but attend outpatient
treatment for OUDSOS Case #3 – Suboxone with SOS
40yo Male, precarious housing, hx of previously treated hep C,
substance-induced psychosis
Came to program on 12mg Suboxone, using 4-6 points fentanyl
IV daily
Initiated on 8 tabs dilaudid dispensed daily
In program x 8 months – currently continues on Suboxone 12mg
OD, 14 tabs Dilaudid. 1-3 tabs PO/IV/dose
Infrequent fentanyl use
++ Psychosocial stabilization during program
Client now plans for transition to Suboxone only OATBenefits seen in program thus far Improvements to quality of life Connections with community services Housing Financial stability Reduction in overdoses Access & engagement with primary care
PRÉSENTATION DE CAS DR CHARLES-ANTOINE BREAU MD, CCFP (AM,EM)
CONFLITS D’INTÉRÊTS • AUCUN
PATIENT X
• Âge: 32 ans
• Première consommation : 12 ans – cocaïne
• Première consommation IV : 21 ans – diacétylmorphine
• ATCD : PTSD, Anxiété, Dépression,Endocardite,VHC
• Rx: Sertraline,Seroquel XR
• Consommation journalière:
• Fentanyl: 1-2 g IV
• Crystal Meth: 10-20$
• Tabac: ½ paquetPATIENT X
• Environ 1-2 surdoses par semaine
• Dépistage de drogues dans les urines à la première visite :
• MET+ FYL+
• AMP+ MOP+
• COC+ BZO+
• Tx antérieurs :
• Méthadone – dose maximale: 155 mg
• Buprénorphine/naloxone: 24 mgPATIENT X
• Débuté avec du safer supply:
• MLLU (KadianMC): 400 mg po die
• Hydromorphone (DilaudidMC) 8mg: 12 co servis die
• MLLU (KadianMC): augmenté de 200 mg chaque 2-3 jours
• Hydromorphone (DilaudidMC) 8mg augmenté de 4 co chaque 2-3 jours
• Dose actuelle :
• MLLU (KadianMC): 1600 mg po OD
• Hydromorphone (DilaudidMC) 8 mg 26 co servis die
• Consommation actuelle :
• Crystal Meth 10-20$, fentanyl 2-3 points par semaineLIGNE DIRECTRICE
• Débuter Hydromorphone 8 mg (DilaudidMC) de
6-8 co par jour
• 8-12 co en pratique
• Augmenter de 2-4 co q24h
• Dose max : 24-30 co selon la réponse
• DilaudidMC préférable, si générique -APOPATIENTY
• Âge : 41 ans
• Première consommation: 19 ans – percocet
• Première consommation IV: 32 ans - M EslonMC
• ATCD:Dépression,TPL,VHC,VIH
• Rx:aucun
• Consommation journalière :
• Crack
• Speed
• Fentanyl 3-4 points par jour
• Tabac ½ paquet par jour
• Cannabis 1 g par jourPATIENTY
• Surdose x 3 dans le dernier mois
• Dépistage de drogues dans les urines à la première visite :
• Positif pour:MET,AMP,FYL,OXY,MOP,BZO
• Tx antérieur : Méthadone 130 mgPATIENTY
• Débuté avec du safer supply:
• Méthadone 30 mg po die
• Hydromorphone (DilaudidMC) 8 mg: 8 co servis die
• Méthadone augmentée jusqu’à 60mg
• et patient voulait cesser méthadone
• Hydromorphone (DilaudidMC) 8 mg: augmenté jusqu’à 30 co par jour
• Dose actuelle:
• Hydromorphone (DilaudidMC) 8 mg, 30 co par jour
• Méthadone: 0 mg
• Consommation actuelle : 0 fentanyl !PATIENT Z
• 23 ans
• Vu aux urgences avec fracture cheville gauche et engelure
• Consommation: Fentanyl IV 2g / jour
• Dernière consommation remonte à plus de 6h
• Nécessite :
• 1. Contrôle de la douleur
• 2. Sédation conscientePATIENT Z
• Traitement de la douleur (double vérification)
• Hydromorphone (DilaudidMC) 32 mg IV
• Fentanyl 400 mcg IV
• Kétamine 0.3 mg / kg – 20 mg IV
• À la grande surprise de mes collègues, patient alerte, orienté. Aucune somnolence.
• Se dit à 5-6/10 de sa consommation habituelle
• Douleur 10/10, maintenant 4/10
• Sédation
• Propofol 140 mg IVPériode de questions
Reconnaissance
© Équipe de soutien clinique et organisationnel en dépendance et itinérance, 2021
Avec la participation de :
Santé Canada
Ministère de la Santé et des Services Sociaux
37Mentions
© Équipe de soutien clinique et organisationnel en dépendance et itinérance, 2021
« Les vues exprimées ici ne reflètent pas
nécessairement celles de Santé Canada. »
« Les vues exprimées ici ne reflètent pas
nécessairement celles du ministère de la
Santé et des Services sociaux. »
38Merci
PROPOSITION
L’Équipe de soutien clinique et organisationnel en dépendance et
itinérance
Téléphone ou texto: 514 863-7234
Courriel: soutien.dependance.itinerance.ccsmtl@ssss.gouv.qc.ca
Site web: http://dependanceitinerance.ca/
39You can also read

















































