Benefits Brochure 2015 - Mecklenburg County
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Mecklenburg County
Benefits
Brochure
2015
Cigna Medical www.mycigna.com 1-800-244-6224
County’s Employee Employee & Spouse/ Employee
Bi-Weekly Rates Employee
Premium & Child(ren) Domestic Partner & Family
Non-Tobacco 12 Month 10 Month 12 Month 10 Month 12 Month 10 Month 12 Month 10 Month
Standard $ 333.20 $ 28.22 $ 33.35 $ 87.32 $ 103.20 $ 148.04 $ 174.96 $ 208.76 $ 246.72
Enhanced $ 386.05 $ 51.19 $ 60.50 $ 147.67 $ 174.52 $ 227.90 $ 269.34 $ 308.14 $ 364.17
Tobacco Use
Standard $ 333.20 $ 61.46 $ 72.63 $ 122.24 $ 144.47 $ 182.96 $ 216.23 $ 243.68 $ 287.99
Enhanced $ 386.05 $ 91.59 $ 108.24 $ 190.09 $ 224.65 $ 270.33 $ 319.48 $ 350.56 $ 414.30
Mecklenburg
Medical Plan Choices for 2015 County offers
Standard Plan Enhanced Plan regular fulltime
Deductibles (Individual/Family) employees a
In-Network $500/$1,000 $250/$500
choice of Cigna
Out-of-Network $1,200/$2,400 $600/$1,800
Standard or Cigna
Out-of-Pocket Maximums
Enhanced Medical
(Individual/Family)
In-Network $3,000/$9,000 $1,500/$4,500 Plans.
Out-of-Network $9,000/$18,000 $4,500/$13,500 Common features of both plans:
Lifetime Maximum Benefit No maximum No maximum Both plans are affiliated with Presbyterian
Co-insurance Hospital and Carolinas Medical Center.
In-Network 20% 15%
Out-of-Network 40% 35% Both plans are PPOs and offer network bene-
fits which include physician services, emergen-
Physician Services
cy care, inpatient and outpatient hospitaliza-
Office Visit $25 copay $20 copay
tion and prescription coverage.
Specialist Office Visit $40 copay $35 copay
Preventative Care No copay No copay The County pays a portion of the total cost of
Routine Gynecological Exam No copay No copay medical insurance for all active regular em-
Maternity $35 copay (first visit) $25 copay (first visit) ployees.
Surgery 20% after deductible 15% after deductible
Allergy Injection (by non- Employees can choose to cover dependents
physician) No charge No charge and are responsible for the additional cost.
Diagnostic X-Ray/Lab (in doctor's
office) 100% after copay 100% after copay
Hospital/Facility
Inpatient Hospital 20% after Deductible 15% after deductible
Outpatient Hospital 20% after deductible 15% after deductible
20% coinsurance $150 20% coinsurance $150
Emergency Room copay copay
Urgent Care Center $25 copay $20 copay
Retail Prescription Drugs (30 day
supply) Medical Plan Opt Out/Waive
Retail Generic $10 copay $5 copay Mecklenburg County Employees only
Retail Preferred Brand 20% coinsurance 20% coinsurance If you have other group coverage and do not
$25 min, $35 max $20 min, $30 max want to participate in the County’s medical
Retail Non-Preferred Brand 40% coinsurance 40% coinsurance plan for 2015, you may choose to opt out/
$50 min, $70 max $45 min, $65 max waive and the County will contribute $400
Mail Order Prescription Drugs 3 month supply for the price of 2 months
to your medical flexible spending account
Vision Care
(FSA). The opt out/waive status will remain
$25 copay (one visit/24 $25 copay (one visit/24
in effect the entire year unless you have a
Routine Eye Exam mths) mths)
qualifying family status change. Employees
Mental Health Benefits/Chemical
Dependency hired during the year receive a prorated FSA
Inpatient Facility 20% after deductible 15% after deductible contribution. Mecklenburg County reserves
Out patient Facility $40 copay $35 copay the right to request proof of coverage of
Office Visit $40 copay $35 copay other medical coverage at any time.
2
Cigna Wellness Programs www.mycigna.com
Cigna offers several health and wellness programs that are free to employees who are enrolled in Cigna
insurance through the County.
Healthy Pregnancy/ Lifestyle Management Program
Healthy Babies Program
This program provides additional Whether you’re looking for help with
support from Cigna staff to ex- weight, tobacco or stress manage-
pecting mothers throughout the ment, our Lifestyle Management Pro-
course of their pregnancy. For more grams are here for you. Each program
information or to enroll call –Cigna is easy to use, available where and
1.800.615.2906 when you need it, and is always no
Enroll in 1st Trimester $150.00 cost to you.
Enroll in 2nd Trimester $75.00 1.866.417.7848- myCigna.com
24 Hour Nurse
Mail Order Prescriptions
1.800.564.9286
Delivered to your home
Get the guidance on medical treat-
ment, or assistance with a health 90 day supply with refills
question 24 hours a day, 7 days a Save time and money by simply calling
week: Cigna to make arrangements to trans-
Speak with a nurse, or fer your existing prescription to
Listen to recorded information Cigna’s mail Order Program. It’s that
on hundreds of medical topics simple! Call Cigna at 1.800.285.4812
(available in English and Span- or enroll online myCigna.com
ish)
Why is Cigna calling me? Mecklenburg County offers Cigna programs to help you get healthy and live well. Cigna is excited to
get to know you, so they call you at home to talk about ways to work together to help you manage your health.
3
Cigna Dental www.mycigna.com 1-800-244-6224
Employee & Spouse/
Bi-Weekly County’s Employee Employee & Child(ren) Employee & Family
Domestic Partner
Rates Premium
12 Month 10 Month 12 Month 10 Month 12 Month 10 Month 12 Month 10 Month
Standard $8.88 $2.21 $2.61 $14.26 $16.85 $11.59 $13.70 $22.80 $26.95
Enhanced $14.60 $3.62 $4.28 $23.42 $27.68 $19.04 $22.50 $37.45 $44.26
Dental Plan Choices for 2015
Standard Plan Enhanced Plan
Calendar Year Maximum (Class I, II, and III Expenses)
(per individual)
In-Network
Regular fulltime employees will
$1,000 $1,500
Out-of-Network $1,000 $1,500 have two options in selecting a
Calendar Year Deductibles (Individual/Family) dental plan: the Standard or En-
In-Network $75/$225 $50/$150 hanced plan. Below are just a
Class I Expenses - Preventive & Diagnostic Care 100% /80% 100% /100% few of the differences between
(In-Network/Out-of-Network) No Deductibles No Deductibles
the two plans:
Oral Exams
Cleanings Standard
Routine X-Rays
Must go to a Network dentist
Fluoride Application
Calendar Year Maximum of
Sealants
$1,000 per individual
Space Maintainers (limited to non-orthodonic treat-
ment) No Orthodontic coverage
Non-Routine X-Rays
Emergency Care to Relieve Pain Enhanced
Histopathologic Exams May go to any dentist
Class II Expenses - Basic Restorative Care 70% /50% 80% /80%
Calendar Year maximum of
(In-Network/Out-of-Network) After Deductible After Deductible
Fillings
$1,500 per individual
Oral Surgery - Simple Extractions Orthodontic Coverage (Life
Oral Surgery - All Except Simple Extractions time Max $1,500 per
Surgical Extraction of Impacted Teeth individual)
Anesthetics
NOTE: Dental cards will NOT be
Major Periodontics
issued to employees. To print a
Minor Periodontics
Root Canal Therapy/Endodontics dental card or to locate a provid-
Relines, Rebases, and Adjustments er, please go to www.cigna.com.
Repairs - Bridges, Crowns, and Inlays
Repairs - Dentures
Class III Expenses - Major Restorative Care 40% / Not Covered 50% / 50%
(In-Network/Out-of-Network) After Deductible After Deductible
Crowns/Inlays/Onlays
Dentures
Bridges
Class IV Expenses - Orthodontia
(In-Network/Out-of Network)
Coverage for Eligibile Children Only (up to age 19) Not Covered 50% / 50%
No Separate Deductible
Lifetime Maximum Not Covered $1,500
Teeth missing prior to coverage under the CIGNA
Missing Tooth Provision Dental plan are not covered.
Available on a voluntary basis when extensive
Treatment Review work in excess of $200 is proposed.
Student Age 26
4
United HealthCare Vision www.myuhcvision.com 1-800-638-3120
Employee & Employee & Spouse/ Employee &
Employee
Bi-Weekly Rates Child(ren) Domestic Partner Family
12 Month 10 Month 12 Month 10 Month 12 Month 10 Month 12 Month 10 Month
Standard $2.23 $2.63 $4.86 $5.74 $4.62 $5.46 $7.64 $9.03
Enhanced $4.54 $5.36 $8.73 $10.31 $8.51 $10.06 $13.27 $15.69
The County offers regular fulltime employees a choice of two voluntary vision plans for a minimal premium which
provides coverage for exams, lenses, frames, contacts, etc. at reduced costs.
Note: Vision cards will NOT be issued to employees as part of this plan.
Vision Plan Choices for 2015
Standard Plan Enhanced Plan
Copays eye exam every 12 months
Comprehensive Exam $10 $0
Materials $20 $0
Contact Lenses
in lieu of eyeglasses Contact Lenses every 12 months
Covered-in-full Contact Lenses Contacts (including disposables), the fitting/evaluation fees,
and up to two follow-up visits are covered-in-full. If covered
disposable contact lenses are chosen, up to 6 boxes are
included when obtained from a network provider.
Laser Vision Benefit
UnitedHealthCare Vision has partnered with the Non-Covered Contact Lenses A $150.00 allowance is applied toward the fitting/evaluation
fees and purchase of contact lenses outside of UnitedH-
Laser Vision Network of America to provide our ealthcare Vision covered-in-full contacts. The materials copay
members with access to discounted laser vision does not apply
correction providers. 1-888-563-4497
Frames Frames every 24 months
Out of Network Reimbursement $50 wholesale frame allowance applied toward the whole-
sale cost of a frame at private practice providers, or
Standard and Enhanced Plan benefits are the same.
a $130 frame allowance applied toward the retail price of a
Network copays do not apply frame at retail chain providers.
Up to
Comprehensive Exam $40 The following lenses and Lens Options are Covered-in-Full
Lenses and Lens Options every 12 months
Lenses Standard Plan Enhanced Plan
Single Vision $40
Lined bifocal Standard Plan Plus:
Bifocal $60
Single Vision High-End Progressives
Trifocal $80
Round & seg. Basic Progressives
Lenticular $80
Lined trifocal Super ET
Frames $45 Scratch Coating Gradient Tint
Plastic bifocals Photochromatic
Contact Lenses (in lieu
Plastic trifocals Polycarbonate
of eyeglasses)
Uv & scratch guard
Elective $150
*Necessary $210 Solid Tint
Transition
You do not need to submit a claim for In- UV Coating (Glass)
Network benefits. However, you must submit a UV Coating (Plastic)
claim to UnitedHealthCare Vision for benefit
Platinum progressive
reimbursement for Out of Network services.
Premium progressive
5
Flexible Spending Accounts
What is A Flexible Spending Account (FSA)?
FSA is a pre-tax program to help reduce health care and dependent care out-of-pocket expenses.
Health Care Spending Account is for regular fulltime employees and eligible depend-
ent healthcare expenses not covered by insurance like co-pays, deductibles, prescrip-
tions, dental or vision care. You may contribute a minimum of $260.00 up to a maxi-
mum of $2500.00 per year.
Dependent Care Account is for regular fulltime employees for dependent care ex-
penses for a child under the age of 13 or a disabled spouse or dependant. If you are
married, you can use this account if you and your spouse both work, are looking for
work, or, in some situations, if your spouse is a full-time student. You may contribute a
minimum of $260.00 to a maximum of $5000.00 per year.
Visit www.flex125.com for a complete list of eligible expenses.
Annual Savings Example*: With FSA Without
Account Account
Annual Salary 35,000 35,000
Pre-tax Contribution 1,500
Taxable income 33,500 35,000
Federal and State Taxes (7,107) (7,597)
How do I contribute to my FSA? After-Tax dollars spent on eligible expenses 0 1,500
Once you make your annual election, Spendable income 26,393 25,903
the amount will be deducted from
Tax Savings with an FSA 490
your pay in equal amounts through-
out the year, before taxes are deduct- *Sample tax savings for a single taxpayer with no
ed. dependents. Actual savings will vary based on your
individual tax situation. Please consult a tax pro-
fessional for more information.
How do I get reimbursed?
Important Note:
A Flex Debit
You may claim expenses incurred from January 1, 2015 through March 15, 2016. Unused
Card will be funds are forfeited and will not be returned to you. Claims must be filed by April 15, 2016
issued to you for reimbursement. Claims filed after April 15, 2016 will be denied.
and you may
use your card to be reimbursed for
eligible expenses and the funds will How do I contact AmeriFlex?
be automatically deducted from your
Mailing Address:
Spending Account. OR simply pay for
AmeriFlex
the eligible expenses and then fax or
700 East Gate Drivek, Suite 510
mail a timely reimbursement request
Mount Laurel, New Jersey 08054 phone: 1-888-868-3539
and receipt to be processed. Forms
are available on MeckWeb intranet
or visit them on the web at:
fax: 1-888-631-1038
site. www.flex125.com
6
Savings and Retirement
Retirement Deferred
Mecklenburg County regular fulltime and part time em- Compensation
ployees are automatically enrolled into the North Caro-
lina Local Government Retirement System upon their Mecklenburg County regular fulltime
employment. Employees contribute 6% of gross wages and part time employees have the op-
and become vested after five years of service. The tion to supplement their pension bene-
County also contributes to fund future benefits. Vari- fit by participating in either a 401(k)
ous retirement options are available. plan and/or a 457 plan. Contacts
Retirement
The NC 401(k) Plan is administered
by Prudential Retirement. North Carolina Local Govern-
ment Retirement System
The County offers a choice of two
457 plans: Phone: 877-627-3287
- 457 plan administered by ICMA-RC Fax: 919-508-5350
- NC 457 plan administered by Pru-
Visit their website at:
Employees retiring from Mecklenburg County may be eli- dential Retirement
http://
gible to remain on the County’s medical insurance. Any- Employees may contribute up to a www.myNCretirement.com
one employed by Mecklenburg County for the first time total of $17,500 to the 457 plans _______________________
after July 1, 2010 will not be eligible to remain on the
combined and up to $17,500 to the
County’s medical insurance upon retirement. Please refer
NC 401(k) Plan. Special catch up 457 Plan
to the Benefits section of the Human Resources Policy for
allowances that allow for additional ICMA-Retirement Corporation
a full description of the eligibility requirements.
contributions are available in all
Phone: 800-669-7400
plans for employees who are 50 or
529 College Savings Plan older this year. Visit their website at:
Mecklenburg County provides http://www.icmarc.org/
_______________________
matching contributions of up to 5%
of gross salary when the employee
401(K) Plan and 457 Plan
contributes to one or a combination Prudential
of these plans.
Phone: 866-627-5267
The county also contributes 5% of
gross salary into the NC 401(k) plan
Visit their website at:
for sworn law enforcement officers http://www.prudential.com/
as mandated by the State of North ncplans
Employees can save for college through payroll deduc-
tion with the North Carolina 529 College Savings Plan.
The plan offers a wide range of investment options Savings Bonds
from conservative to aggressive. Investments can be
used at any college for qualified educational expenses Mecklenburg County supports the US Savings Bond Program.
such as tuition, books, and room and board. Employees can invest in savings bonds through Treasury Di-
rect, a free online system offered by the Department of the
To enroll in the plan, contact the College Foundation of Treasury. Employees can begin purchasing bonds by going to
North Carolina (CFNC) toll free at 800-600-3453 or visit www.treasurydirect.gov and creating an account. If you have
www.NC529.org . Once you have enrolled and selected any questions or need assistance, please call the Employee
the payroll deduction option, a representative from Services Center at 704-432-6947.
CFNC will contact the County to advise that you’ve re-
quested that your contributions be payroll deducted.
7
Life and Disability Benefits
Basic Term Life Insurance Short Term Disability
Regular fulltime employees are automatically covered with basic This benefit is provided to assist a fulltime employee who is disa-
term life insurance in the amount equal to their annual salary. bled due to a non-work related illness or accident. Sixty percent
Dependent/Spouse coverage of $10,000 is available. of the employee’s weekly earnings will be paid for up to 26
weeks, after a 25-day waiting period. Short Term Disability be-
gins 90 days after employment and excludes pre-existing condi-
tions.
Supplemental Term Life Insurance Long Term Disability
The County offers fulltime employees the opportunity to pur- Long Term disability replaces 40% of a fulltime employee’s sala-
chase up to six (6) times their annual salary (or up to ry for up to 5 years should he or she become disabled. This ben-
$1,000,000) in supplemental term life insurance. Proof of good efit is provided by the County for regular employees who have
health is not required if requested coverage does not exceed less than 5 years of service with the County. Employees with 5
four (4) times the annual salary or $300,000 and if enrollment or more years will refer to the NC Retirement System plan for
begins immediately upon eligibility. The policy includes an ac- benefits. Employees can also purchase an additional 20% of
celerated death benefit for those with terminal illnesses as well coverage. Restrictions apply.
as Accidental Death and Dismemberment (AD&D) benefits.
Rates are based on age, smoking habits, and amount of insur-
ance requested.
8
Voluntary Accident Benefit
Accidents happen in places where you and your family spend the most time; at work, in the home and on the
playground and they're unexpected. How you care for them shouldn't be.
What is Accident Insurance? With the Accident Plan, you get a
When an accident happens, you don't want to worry about how you will pay health and wellness screening
for the initial care, especially if you have to go to the doctor's office, urgent benefit up to $50 per covered per-
care facility or the emergency room for x-rays or ride in an ambulance.
son per calendar year.
• Accident Emergency Treatment - $125
• X-Ray Benefit - $30 Wellness Benefit:
• Ambulance - $200 The Accident Plan provides a benefit if the cov-
• Air Ambulance - $2,000 ered person has one health screening test pre-
formed. This benefit is payable once per calen-
Accident Insurance is designed to help you fill some of the gaps caused by dar year per person.
increasing deductibles, co-payments and out-of-pocket costs related to an
accidental emergency. Remember, accidents can happen anywhere at any Tests include:
time. • Blood test for triglycerides
• Bone marrow testing
• Sports Injuries •Car Accident • Lifting Injuries
• Broken Bone • Laceration • Chip a Tooth • Breast ultrasound
• Bee Sting • Insect Bite • Knee Injury • CA 15-3 (blood test for breast cancer)
• CA 125 (blood test for ovarian cancer)
What does the Accident Plan cover? • Carotid doppler
• CEA (blood test for colon cancer)
The Accident Plan provides you with several benefits to assist with costs asso- • Chest x-ray
ciated with certain accidents both on and off the job. You have coverage 24
hours a day, 365 days a year. The benefits are paid directly to you and are
• Colonoscopy
offered for everyone in your family if chosen. Children are covered to the age • Echocardiogram (ECHO)
of 25, even if they are not a full-time student. Sport injuries are covered and • Electrocardiogram (EKG, ECG)
you have the ability to add disability protection for your spouse if you choose. • Fasting blood glucose test
• Flexible sigmoidoscopy
The Accident Plan covers, but is not limited to:
• Emergency Room Treatment
• Hemoccult stool analysis
• Doctor’s Office / Urgent Care • Mammography
• Surgical Care • Pap smear
• Transportation / Lodging • PSA (blood test for prostate cancer
• Hospital Admission and Confinement • Serum cholesterol test to determine
• Follow-up Care YOU GET 24/7
• Physical Therapy
level of HDL and LDL
• Appliances COVERAGE • Serum protein electrophoresis (blood
• Follow-up Visit test for myeloma)
Other Features: • Stress test on a bicycle or treadmill
• You are covered WORLDWIDE • Skin cancer biopsy
• This plan is portable; you can take it with you if you change jobs or retire • Thermography
• You are paid benefits regardless of any other insurance you may have
• ThinPrep pap test
• Virtual colonoscopy
Regular fulltime employees interested in obtaining more information or enrolling in this Voluntary Acci-
dent plan should call the Employee Services Center at (704) 432-6947.
9
Voluntary Cancer Benefit
The risk of developing cancer, unfortunately, is very real. In the United States, according to the American
Cancer Society, 1 in 2 men and 1 in 3 women have a lifetime risk of developing cancer. 62% of the costs asso-
ciated with cancer treatment are now considered out-of-pocket expenses not covered by your major medical
insurance.
If you are diagnosed with cancer, how will you pay for what your health insurance won't?
Direct Costs Most Major Medical Plans Cover: Indirect Costs You Pay:
• Hospital charges • Loss of wages or salary
Only 38% of cost You cover 62%
• Surgeon fees • Deductibles or coinsurance
covered of costs
• Physician Fees • Travel expenses to/from treatment centers
• Medication & drug costs • Lodging and meals
• Radiological fees • Child care
• Nursing costs
What does the Cancer Plan cover? With the Cancer Plan, premiums are
The Cancer Plan pays for a variety of inpatient or outpatient benefits TAX-FREE so you will receive an average
related to cancer treatment including, but not limited to:
• Hospital confinement
savings of 30%.
• Ambulance
• Air ambulance Wellness Benefit:
• Private, full-time nursing services Under the cancer plan, each covered in-
dividual can receive reimbursement for
Other inpatient and outpatient treatment benefits include a variety of up to $125.00 once per calendar year for
other items such as those listed below:
• Radiation/chemotherapy
a cancer or wellness screening.
• Anti-nausea medication The screenings include, but are not lim-
• Experimental treatments ited to:
• Blood / Plasma / Platelets / Immunoglobulin
• Hair prosthesis / External breast / Voice box prosthesis • Chest x-ray
• Medical imaging studies
• Peripheral stem cell transplant
• Pap smear
• Supportive / Protective care drugs and colony simulating factors • Mammography
• Bone marrow stem cell transplant. • Breast ultrasound
• PSA - blood test for prostate cancer
The Cancer Plan covers items you may not typically think of. • Biopsy of skin lesion
Oftentimes, there are costs associated with cancer treatment that you
may not typically consider. Those costs listed below are covered under
• Colonoscopy
the Cancer Plan.
What else does the cancer benefit
• Travel expenses include?
• Companion transportation and lodging
• Surgical procedures including skin cancer The cancer plan also offers extended
• Second medical opinions
care benefits such as coverage for:
• Anesthesia
• Prosthetic or artificial limbs
• Outpatient surgical center • Skilled nursing care facility
• Reconstructive surgery • Family care
• Hospice
• Home health care service
• Waiver of Premium
Regular fulltime employees interested in obtaining more information or enrolling in this Voluntary Cancer plan
should call the Employee Services Center at (704) 432-6947.
10Voluntary Medical Bridge Benefit
As major medical plans move toward larger deductibles and higher co-payments, you may be left with more gaps to fill. How will
you cover all of those medical expenses?
Medical Bridge 3000, hospital confinement indemnity insurance, or for short, Medical Bridge, is designed to fill the gaps in your
health insurance and help protect against those out-of-pocket expenses, including deductibles and co-pays, that occur when it
comes to you or your family members’ healthcare.
What is Medical Bridge and how does it work? With the Medical Bridge Plan,
The Medical Bridge Plan helps to “bridge the gaps” in your health insurance. premiums are TAX-FREE and
family coverage is available.
Take a look at the chart below to see how out-of-pocket medical expenses can
quickly add up. Medical Bridge will assist you with these costs. Wellness Benefit:
The Medical Bridge Plan pays $50 for
EXAMPLE: 80/20 PPO one of the wellness tests listed below.
25% of the $8,000 is
YOUR responsibility
The plan pays one test per calendar
Outpatient Surgery: $8,000 Total year for employee-only coverage; or
without Medical
Your Deductible: - $500 Bridge
two tests per calendar year combined
for family coverage. This benefit helps
Balance: $7,500
reimburse you for part of the expense
x 20% Co-Insurance of tests you normally have each year.
$1,500 Co-Insurance
• Blood test for triglycerides
+ $500 Deductible • Breast ultrasound
• CA 15-3 (blood test for breast can-
YOUR COST: $2,000
cer)
The following benefits are payable due to a covered accident or covered sick- • CA 125 (blood test for ovarian can-
ness: cer)
• Outpatient Surgical Procedure Benefit • CEA (blood test for colon cancer)
pays a lump-sum benefit when a covered person requires a surgical pro-
cedure and is not confined to a hospital at the time of the surgery. The
• Chest x-ray
procedure must be performed in a hospital or an ambulatory surgical • Colonoscopy or virtual colonoscopy
center. Refer to the outline of coverage for the calendar year maximum • Fasting blood glucose
and the list of covered procedures. • Flexible sigmoidoscopy
• Hospital Confinement Benefit • Hemoccult stool analysis
pays a lump-sum benefit if any covered person is confined. This benefit
can help you pay for the deductibles associated with a hospital confine-
• Mammography
ment. • Pap smear of thin prep pap
• Rehabilitation Unit Benefit • PSA (blood test for prostate cancer)
pays $100 per day up to 15 days per confinement with no more than 30 • Serum protein electrophoresis
days per calendar year if any covered person is transferred to a rehabili- (blood test for myeloma)
tation unit immediately after a period of hospital confinement.
• Waiver of Premium Benefit
• Serum cholesterol test for HDL &
waives the premium for the policy and any attached riders once the LDL
named insured has been confined to a hospital for 30 continuous days. • Stress test on a bicycle or treadmill
The premium is then waived as long as the confinement in a hospital or • Thermography
rehabilitation unit continues.
Regular fulltime employees interested in obtaining more information or enrolling in this Voluntary Accident plan
should call the Employee Services Center at (704) 432-6947.
11myTotalHealth
Your Employee Wellness Program!
Mecklenburg County is committed to employee health. The myTo-
talHealth Employee Wellness program is designed to offer programs and
services that promote health and well-being. The Wellness Ambassadors
in each department can help you get connected to the program offerings.
Programs Include:
Camp Wellness - onsite Health Fairs, Flu Shots and Mammography Screenings
All employees are invited to participate in this annual event. Learn about new and innovate ways
to stay well at our health fair. We also offer flu shots at no cost to employees and a convenient
Mammography Screenings through the mobile van.
Biometric screening
The screenings are offered onsite to increase your awareness and
identify your potential health risk for lifestyle related disease. Test
measure height, weight, blood pressure, cholesterol and blood sugar.
Health Challenges
Health Challenges are a great way to keep your
health a priority! Our team challenges are both
health and activity based. The Team format
helps keep you on track. Everyone is a winner
when it comes to good health!
Onsite Health and Wellness Classes
Learn new ways to stay healthy and Access to onsite and Park and Recreation Fitness Centers
well at work and at home with our Our on-site fitness center is located at the Hal Marshall
onsite educational classes. We offer Building at 700 North Tryon Street. In addition, various Park
various health and wellness topics in a and Recreation Fitness Centers around the county offer dis-
Lunch and Learn format. count memberships to county employees and their families.
For a complete list visit MeckWeb main page and click on
the “Wellness” icon.
Wellness Contact Information:
Phone: 980-314-2711
Email: mytotalhealth@ mecklenburgcountync.gov
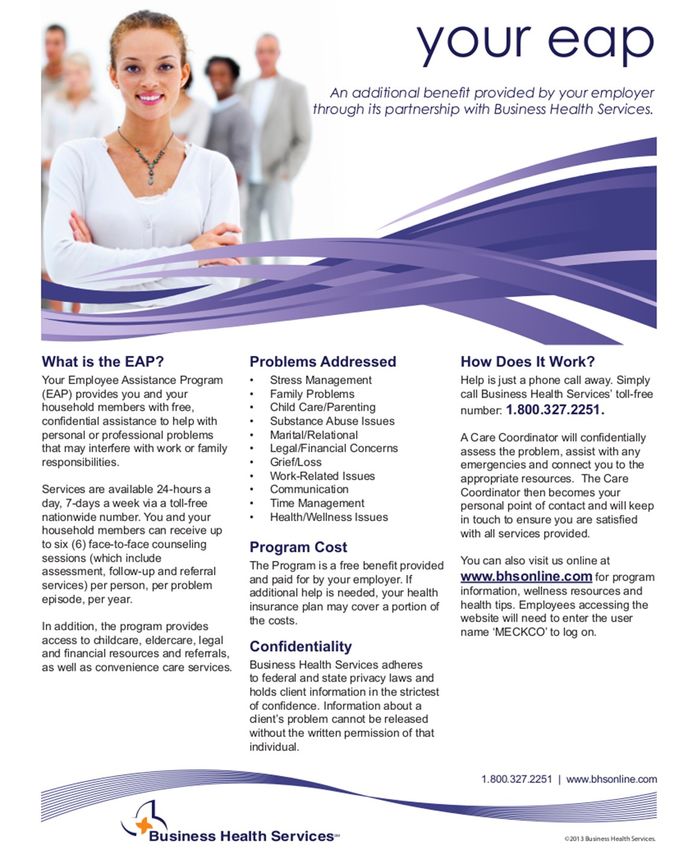
12Employee Assistance Program
13Holidays and Leave
Holidays (10 Annually—Regular Fulltime Employees)
New Year’s Day Labor Day
MLK’s Birthday Thanksgiving Day
Good Friday Friday after Thanksgiving
Memorial Day Christmas Day Vacation Leave_____________________________
For regular fulltime and part time employees, vaca-
tion leave begins accruing on the first day of em-
*Independence Day One other day @ Christmas
ployment. The accrual rate is based upon years of
service. Employees who do not use sick leave or
*12 Month Employees only
leave without pay for 7 consecutive pay periods
earn an additional 4 hours of vacation.
Bereavement Leave______________________________________ Vacation Accrual Rate
Mecklenburg County allows time away from work for the death of an Days per Year
immediate family member. Regular fulltime employees may take up Years of Service
12 Month 10 Month
to 24 consecutive work hours paid leave.
0-1 10 8.5
2-4 12 10.2
Leaves of Absences_______________________________________ 5-9 15 12.7
10-14 18 15.2
There are specific types of absences which may be approved as peri-
ods of time away from work. Mecklenburg County recognizes the fol- 15-19 21 17.8
lowing types of leave. Restrictions apply. 20+ 24 20.3
At the end of each calendar year, employees may
Administrative Leave – unpaid up to 30 days
carry a maximum of 30 days vacation into the New
Family/Medical Leave – unpaid up to 12 work weeks
Year, and any excess leave over 30 days will be
Military Caregiver Leave – unpaid up to 26 work weeks
rolled into the employee’s accumulated sick leave
Extended Medical Leave – unpaid up to 52 work weeks
Extended Family Leave – unpaid up to 52 work weeks balance.
Military Leave
Disaster Response Leave
Sick Leave (12 days annually)__________________________
For regular fulltime and part time employees, sick leave is accrued on a
bi-weekly basis at a rate of 0.04615 hours (12 days annually) for each
regularly scheduled hour worked. There is no maximum accrual limit.
Sick Leave Donation: In long-term medical situations, employees may
donate sick leave to other employees subject to certain conditions.
14Key Things You need to Know
Coverage for Eligible Family Members
County employees may cover eligible family members by paying a bi-weekly payroll deducted
premium. Eligible family members include:
Your legally married spouse
A same sex domestic partner (affidavit required)
You may cover a biological, foster, adopted or step-child/ren up to age 26.
Proof may be required if child or spouse has different last name than employee.
Do you have a Change in your Family and/or Financial Situation?
Family Status Change
It is the employee’s responsibility to advise the Employee Services Center within 31 days of a qualifying family
status change (birth/adoption, marriage/divorce, graduation of child, death, etc) if a dependent needs to be
dropped or added. After the 31 day period, no dependents can be added or dropped. Premium refunds will not
be made and coverage will end as soon as the dependent becomes ineligible for coverage. See Forms and Infor-
mation in this brochure for contacting the Employee Services Center.
What types of changes can I make throughout the year?
Add or drop dependent coverage, based on a qualifying event (such as marriage,
birth of a child or dependent has reached maximum age).
Change or update your life insurance beneficiary information
Enroll or change participation level in the 401K or 457 Defined Contribution Plan.
Enroll or change participation in the NC529 College Savings Plan.
Need More Information?
Benefit forms and information are available to County employees on
the intranet (MeckWeb). Customer Service is available by phone at
our Employee Services Center at (704) 432-6947 and by email at
myHR@mecklenburgcountync.gov.
15Mecklenburg County Employee Benefits
STATEMENT OF
EQUAL EMPLOYMENT OPPORTUNITY AND AMERICANS
WITH DISABILITIES ACT
It is the policy of the County to provide equal employment opportunity without regard to race, color,
religion, sex, sexual orientation, genetic information, political affiliation, age, disability, national origin,
or other status protected by federal, state or local law.
Discrimination against any person in the recruitment, examination, appointment, training, promotion,
retention, discipline, or any other aspect of personnel administration because of race, color, religion,
sex, sexual orientation, genetic information, political affiliation, age, disability, national origin, or other
status protected by federal, state or local law is prohibited.
Discrimination on the basis of age, sex, or physical disability is prohibited except where age, sex, or
disability requirements constitute a bona fide occupational qualification necessary for performance of
the essential functions of a job.
The County will comply with the Americans with Disabilities Act (ADA) which prohibits discrimination
on the basis of a disability. The County will make reasonable accommodations upon requests of other-
wise qualified disabled applicants and employees to enable them to perform essential job functions
except where such accommodations may constitute an unreasonable hardship or jeopardize the health
and safety of employees, applicants or the general public.
________________________________________________________________________________________________________________________________
16The employee benefits program is administered by Mecklenburg County
Human Resources Department
700 East 4th Street
Charlotte, NC 28202
Employees Services Center:
(704) 432-6947 phone
(704) 336-2731 fax
www.charmeck.org
For additional information about any benefits described in this brochure, please consult Mecklen-
burg County policies, the applicable summary plan description (SPD), or the actual plan. In the
event that there is any conflict between the information in this brochure, the SPD, the policies,
and/or a plan, the plan document always governs.
Participation in any of the County’s benefit plans does not create and should not be viewed as a
contract of employment. While Mecklenburg County intends to provide these benefits for an in-
definite period of time, it reserves the right to terminate, suspend, withdraw, amend, or modify a
plan at any time. Any such change or termination of benefits will be based solely on the decision
of the County.
IMPORTANT NOTICES
Rate Notice for 10 Month Employees
In order to provide continuous medical coverage for 10 month staff, the County de-
ducts additional amounts in the 10 months (22 pay periods) worked to cover the
approximate 2 months in the summer (4 pay periods) in which staff do not receive a
paycheck and are not paying premiums.
Revised 1/2015
17You can also read