BNF CHAPTER 13: SKIN - Southend CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BNF CHAPTER 13:
SKIN
Some of the emollients listed in this chapter are classed as appliances and are listed in part IXA of the Drug Tariff
(DT) e.g. Epimax® cream, Hydromol® ointment and products from the Zeroderma range (list not exhaustive). Please
prescribe only preparation listed in the DT or licensed as medicinal product (http://www.medicines.org.uk/emc/ )
Warning: Paraffin-based emollients are flammable. Dressings and clothing that have contact with paraffin-based
products are easily ignited by a naked flame. Advise patients to keep them away from fire or flames and not smoke
when using them. The risk of fire should be considered when using large quantities of any paraffin-based emollient.
Products should be applied in direction of hair growth to prevent folliculitis
Ensure that the indication is a documented dermatological condition. Prescribing of emollients for non-clinical
cosmetic purposes such as dry skin in the absence of a diagnosed dry skin condition such as eczema or psoriasis is not
supported and should be stopped.
1
NHS Castle Point and Rochford CCG / NHS Southend CCG
Integrated Dermatology Service South East Essex May 202013.1 MANAGEMENT OF SKIN CONDITIONS
Prescribe pump dispensers to minimize the risk of bacterial contamination, when they are available for the patient’s
selected emollient. For Preparations that come in pots, using a clean spoon or spatula (rather than fingers) to remove
the emollient helps to minimize contamination.
Use licensed medicines whenever they are likely to be of benefit. Prescribe Dermatology Specials only from the
BAD list
BNF 13.2 EMOLLIENT AND BARRIER PREPARATIONS
Suitable quantities of Emollients to be prescribed for specific areas of the body:
Cream / ointment Lotion
Area of the body
One week supply One month supply One week supply One month supply
Face and neck 15 – 30g 60-120g 100ml 400ml
Both hands 25 – 50g 100-200g 200ml 800ml
Scalp 50 – 100g 200-400g 200ml 800ml
Both arms or both legs 100 - 200g 400-800g 200ml 800ml
Trunk 400g 1600g 500ml 2000ml
Groins and genitalia 15 – 25g 60-100g 100ml 400ml
These amounts are usually suitable for an adult for twice daily application.
2
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020 Generally the greasier the product the more effective it is as emollient, as it is able to trap more moisture in the skin.
However, greasier emollients can be less acceptable or tolerable.
Products listed in the tables below follow cost criteria in ascending order.
EMOLLIENT LOTIONS
First Choice
Product Name Potential Sensitisers
Lanolin/Derivatives
E45 Lotion Hydroxybenzoates (Parabens)
Benzyl Alcohol
Alternatives
Product Name Sensitisers
Cetyl/Cetostearyl/Stearyl Alcohol
QV skin lotion Hydroxybenzoates (Parabens)
Cetyl/Cetostearyl/Stearyl Alcohol
Cetraben Lotion Phenoxyethanol
Lotions have a higher water content than creams, which makes them easier to spread but less effective as emollients.
They may be preferred for very mildly dry skin, as well as for hairy areas of skin.
3
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020EMOLLIENT CREAMS
First Choice
Product Name Potential Sensitisers
Cetyl/Cetostearyl/Stearyl Alcohol
Epimax® Cream – Easy Squeeze – Flexi dispenser
Phenoxyethanol
Alternatives
Product Name Potential Sensitisers
Epimax® ExCetra Cream - Easy Squeeze – Flexi dispenser Cetyl/Cetostearyl/Stearyl Alcohol/ Phenoxyethanol
Cetyl/Cetostearyl/Stearyl Alcohol
Epimax oat® Cream - Easy Squeeze – Flexi dispenser
Chlorocresol/Benzyl alcohol/Phenoxyethanol/ Isopropyl palmitate
Cetyl/Cetostearyl/Stearyl Alcohol/ Lanolin/Derivatives/
Zerocream® - Pump
Phenoxyethanol
Cetyl/Cetostearyl/Stearyl Alcohol
Zerobase® Cream - Pump
Chlorocresol
Cetyl/Myristyl/Stearyl Alcohol
Zeroveen® Cream – Pump Isopropyl palmitate
Benzyl alcohol
EMOLLIENT GELS
First Choice
Product Name Potential Sensitisers
Triethanolamine
Epimax® Isomol Gel – “Easy Squeeze” flexi dispenser Phenoxyethano
Isopropyl mysristate
4
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Alternatives
Product Name Potential Sensitisers
Triethanolamine
Zerodouble® Gel – Top down bottle Phenoxyethano
Isopropyl mysristate
Creams and gels are emulsions of oil and water and their less greasy consistency often makes them more cosmetically
acceptable.
EMOLLIENT OINTMENTS
First Choice
Product Name Potential Sensitisers
Epimax® ointment Cetyl/Cetostearyl/Stearyl Alcohol
Alternatives
Product Name Potential Sensitisers
White soft paraffin None
Zeroderm® ointment Cetyl/Cetostearyl/Stearyl Alcohol
SPC: Cetostearyl alcohol
Emulsifying ointment Phenoxyethanol
50:50 White soft and liquid paraffin ointment None
Hydromol® ointment Cetyl/Cetostearyl/Stearyl Alcohol
5
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020 Ointments are the greasiest preparations, being made up of oils or fats. They do not usually contain preservatives and
may be more suitable for those with sensitivities. However, they can exacerbate acne, can cause folliculitis when
overused and they should not be used where infection is present.
Emollients should be applied in the direction of hair growth to reduce the risk of folliculitis.
EMOLLIENTS WITH ANTIMICROBIALS
First Choice
Product Name Potential Sensitisers
Cetyl/Cetostearyl/Stearyl Alcohol
Dermol 500® lotion Phenoxyethanol
(for weeping infected skin) Benzalkonium chloride
Cetostearyl Alcohol; Cetomacrogol; Phenoxyethanol; Disodium
Dermol® cream Phosphate Dodecahydrate; Sodium Dihydrogen Phosphate Dihydrate;
(for dry infected skin) Benzalkonium chloride
Antiseptic products are more likely to cause skin sensitisation reactions and may cause bacterial resistance
Preparations containing an antibacterial (e.g. Dermol) should be avoided unless infection is present or is a
frequent complication.
Use should be targeted and short term.
EMOLLIENTS CONTAINING UREA
First Choice
Product Name Potential Sensitisers
Cetyl/Cetostearyl/Stearyl Alcohol
Imuderm® Urea Emollient Benzalkonium Chloride; Phenethyl Alcohol
Cetrimonium Bromide
6
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020 Emollient products containing urea are not all interchangeable. The urea content of products varies widely and some
contain additional active ingredients such as salicylic acid or lactic acid (keratolytic properties), or lauromacrogols
(reputed to reduce itch). Ensure that product(s) selected are indicated for the intended use.
It is reasonable to target use of emollients containing urea (a keratin softener and hydrating agent) to specific
groups, e.g. those with scaling skin, or those who have tried other emollients without success.
BATH AND SHOWER EMOLLIENTS AND SOAP SUBSTITUTES
Evidence around the use of bath and shower preparations is limited. Many standard emollients can be used as a soap
substitute. Any ointment (except 50:50) can be dissolved in some hot water and added to the bath water as a bath additive.
Bath additives and shower gels are not recommended for prescribing
It is recommend to use a standard emollient as a soap substitute (e.g. by applying it to the skin before bathing/showering
then rinsing it off), as they believe this provides better moisturisation of the skin.
Regardless of the type of product the person uses to wash with, it should not replace the regular use of a leave-on emollient.
Please, advise people to continue using standard emollients in addition to any bath/shower product or soap substitute used.
7
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020BNF 13.4 TOPICAL CORTICOSTEROIDS
Fingertip units of topical corticosteroid cream or ointment to apply to specific areas
Number of fingertip units
Trunk (back) inc.
Age Face & neck One arm & hand One leg & foot Trunk (front)
buttocks
Adult 2.5 4 8 7 7
3-6 month old child 1 1 1.5 1 1.5
1-2 month old child 1.5 1.5 2 2 3
3-5 month old child 1.5 2 3 3 3.5
6-10 month old child 2 2.5 4.5 3.5 5
Suitable quantities of corticosteroid preparations to be prescribed for specific areas of the body - These amounts are
usually suitable for an adult for a single daily application for 2 weeks.
Area of body Creams and Ointments
Face and neck 15 – 30g
Both Hands 15 – 30g
Scalp 15 – 30g
Both Arms 30 – 60g
Both Legs 100g
Trunk 100g
Groins and genitalia 15 – 30g
8
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020 Topical corticosteroids should be spread thinly on the skin but in sufficient quantity to cover the affected areas. The
length of cream or ointment expelled from a tube can be measured in terms of a fingertip unit (the distance from
the tip of the adult index finger to the first crease, equivalent of approximately 500mg).
Match the potency of topical corticosteroid to the severity of the condition, taking into account the patient’s age
and site of application.
Use topical corticosteroids short term or intermittently wherever possible. Regular emollient use and strategies such
as treating frequently flaring atopic eczema with topical corticosteroid for two days a week, or the use of non-steroid
based treatments in between topical corticosteroid courses in psoriasis can support this.
Use the more potent topical corticosteroids with appropriate caution. Potent or very potent topical corticosteroids
may be contraindicated or restricted to use under specialist supervision depending on the age of the person, the
condition being treated and the site of application.
Topical corticosteroids are contraindicated in acne, rosacea, perioral dermatitis and untreated bacterial, fungal,
or viral skin lesions. They should not be used for the routine treatment of urticaria or pruritis of unknown cause,
and they may worsen ulcerated lesions.
Small packs of hydrocortisone 1% (alone or combined with other ingredients) and clobetasone butyrate 0.05% are
available over the counter (OTC) for short-term use (maximum seven days) in skin conditions such as mild to moderate
eczema, dermatitis and insect bites. The licence of OTC products is more restrictive, but when appropriate patients can be
directed to purchase items for self care.
Products listed below are generally with the generic name first, except where a brand is available at a lower price to the
Drug Tariff price, where brand name is listed first.
9
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020The list of excipients listed below correspond to the brand names as generic products contain different excipients
depending on their manufacturer
MILD TOPICAL CORTICOSTEROIDS – cost less than £0.20 per gram or ml - £6 per 30g or 30ml
First Choice
Hydrocortisone 1% cream
Alternatives
Synalar 1 in 10 Dilution® (fluocinolone acetonide 0.0025% cream)
MODERATE TOPICAL CORTICOSTEROIDS – cost less than £0.10 per gram or ml - £3 per 30g or 30ml
First Choice
Audavate RD® 0.025% cream/ointment (betamethasone valerate)
Alternatives
Clobavate® 0.05% ointment (clobetasone butyrate)
Modrasone® 0.5% cream (alclometasone dipropionate)
Haelan® (fludroxycortide 0.0125% cream/ointment)
Ultralanum Plain® cream (fluocortolone pivalate 0.25%, fluocortolone hexanoate 0.25%)
Ultralanum Plain® ointment (fluocortolone monohydrate 0.25%, fluocortolone hexanoate 0.25%)
10
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Eumovate® (clobetasone butyrate 0.05% cream)
Alphaderm® (hydrocortisone 1%, urea 10% cream)
Synalar 1 in 4 Dilution® (fluocinolone acetonide 0.00625% cream/ointment)
POTENT TOPICAL CORTICOSTEROIDS – cost less than £0.10 per gram or ml - £3 per 30g or 30ml
First Choice
Audavate® 0.1% ointment (betamethasone valerate)
Betnovate® (betamethasone valerate 0.1% lotion)
Alternatives
Betnovate® 0.1% cream/ointment (betamethasone valerate)
Locoid® (hydrocortisone butyrate 0.1% cream/ointment)
Locoid 0.1% Lipocream® (hydrocortisone butyrate)
Locoid Crelo® 0.1% emolsion (hydrocortisone butyrate)
VERY POTENT TOPICAL CORTICOSTEROIDS – cost less than £0.10 per gram or ml - £3 per 30g or 30ml
First Choice
Clobaderm® 0.05% cream/ointment (clobetasol propionate)
Alternatives
11
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Dermovate® (clobetasol propionate 0.05% cream/ointment)
PRODUCTS CONTAINING ANTIMICROBIALS OR ANTIFUNGALS
The benefit of including antibacterials or antifungals with a topical corticosteroid is uncertain. NICE advise that use
of topical antibiotics in children with atopic eczema, including those combined with topical corticosteroids, should be
reserved for cases of clinical infection in localised areas and limited to a maximum of two weeks treatment. Longer
use increases the risk of resistance and sensitization.
Limiting use to a maximum of two weeks for adults and children
Only issuing these items as acute issues and reviewing any currently prescribed as repeats
Potency of corticosteroid: Mild
Product Active Ingredients
Canesten HC – 30gr hydrocortisone 1%, clotrimazole 1%
Daktacort® cream/ ointment - 30gr hydrocortisone 1%, miconazole nitrate 2%
Hydrocortisone 0.5%, Benzalkonium chloride 0.20%,
Timodine cream
nystatin 100 000 units/g
Terra-Cortril® ointment - 30gr hydrocortisone 1%, oxytetracycline (as hydrochloride) 3%
Fucidin H® cream - 30gr hydrocortisone acetate 1%, fusidic acid 2%
Potency of corticosteroid: Potent
Product Active Ingredients
Synalar N® cream/ ointment – 30gr fluocinolone acetonide 0.025%, neomycin sulfate 0.5%
12
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Fucibet® cream/lipid cream - 30gr betamethasone (as valerate) 0.1%, fusidic acid 2%
Lotriderm® cream - 30gr betamethasone dipropionate 0.064%, clotrimazole 1%
TAPES AND PLASTERS
The use of these products should be short term but it can be intermittent and under the supervision of a specialist:
Haelan® tape is polythene adhesive film impregnated with fludroxycortide 4 micrograms/cm2
Betesil® medicated plasters contain betamethasone (as valerate) 2.25 mg
BNF 13.5.2 PREPARATIONS FOR PSORIASIS
Use licensed medicines whenever they are likely to be of benefit. Prescribe Dermatology Specials only from the BAD list
except in special circumstances. They can be prescribed by GP after initiation by specialist and prescriptions can be taken to
hospital pharmacy (Basildon Hospital) or fax to Hospital Pharmacy (Southend hospital), see Specially made up ointments
and creams - Process to follow for Southend Hospital input and review.
Vitamin D and analogues
First Choice
Tacalcitol 4 micrograms/g ointment (Curatoderm®)
Calcipotriol 50 micrograms/g ointment (Dovonex®)
Alternative
Calcipotriol 50micrograms/ml scalp solution
Calcipotriol 0.005% / Betamethasone 0.05% gel
Calcipotriol 50micrograms/g / Betamethasone dipropionate 500micrograms/g foam (Enstilar®)
Tars
13
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020First Choice
Psoriderm® cream - coal tar 6%, lecithin 0.4%
Cocois® scalp ointment - coal tar solution 12%, salicylic acid 2%, precipitated sulfur 4%, in a coconut oil emollient basis
Alternative
Exorex® lotion - coal tar solution 5% in an emollient basis
Sebco® scalp ointment - coal tar solution 12%, salicylic acid 2%, precipitated sulfur 4%, in a coconut oil emollient basis
Prescribing information for Calcipotriol/Betamethasone
In adults apply no more than 15g/day (or 100g per week). The body surface area treated with calcipotriol containing
medicinal products should not exceed 30%. Side effects: hypercalcaemia if > 100g/ week. Local skin reactions:
itching, erythema, burning, paraesthesia, dermatitis, are common.
Further counselling points: Application under occlusive dressings should be avoided since it increases the systemic
absorption of corticosteroids. Not recommended to take a shower or bath immediately after application of Dovobet®
ointment or gel. Hands must be washed after each application.
When different calcipotriol containing preparations are used together, the maximum total calcipotriol dose is 5mg in
any one week (e.g. 60ml calcipotriol scalp solution with 30g ointment or 30ml scalp solution with 60g ointment).
Calcipotriol/Betamethasone is contraindicated in patients with known disorders of calcium metabolism. Also contra-
indicated in erythrodermic, exfoliative and pustular psoriasis. Do not use on facial or flexural
References
1. National Institute for Health and Care Excellence (NICE). Clinical Guideline 153. The assessment and management of psoriasis. October 2012. Available
http://www.nice.org.uk/guidance/cg153
2. SPC. Dovobet® gel. Leo Laboratories Ltd. Last updated 29/10/14.
3. SPC. Dovobet® ointment. Leo Laboratories. Ltd Last updated 29/10/14.
14
NHS Castle Point and Rochford CCG
NHS Southend CCG
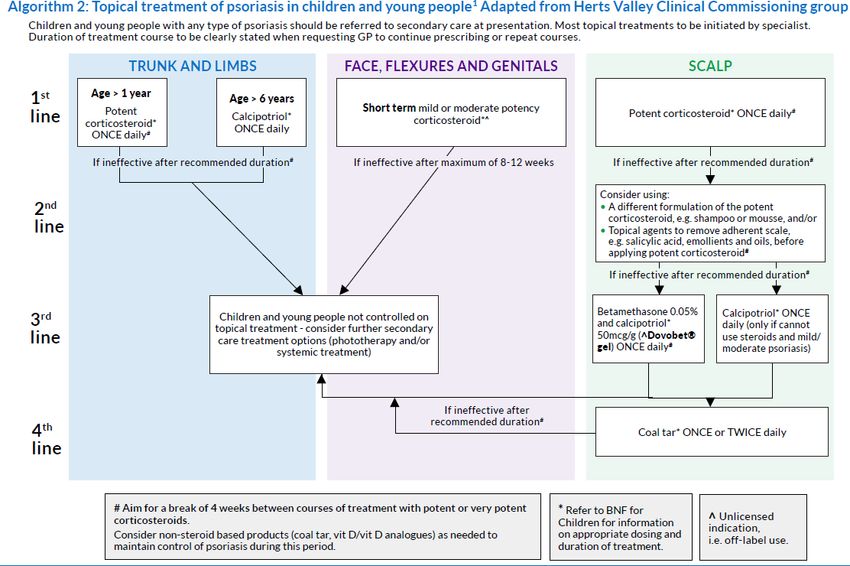
May 2020Algorthm 1: Topical treatment of psoriasis in adults. Adapted from Herts Valley Clinical Commissioning Group
TRUNKS AND LIMBS FACE, FLEXURES AND GENITALS SCALP
Topical agents to remove adherent scale, e.g.
1st Potent corticosteroid DAILY plus vitamin D / vitamin D
Short term mild or moderate potency corticosteroid^ applied
ONCE or TWICE daily. Maximum of 2weeks#
salicylic acid, emollients, before applying potent
line analogue DAILY (apply separately, one in the morning and corticosteroid#
the other in the evening) for up to 4 weeks#
Potent corticosteroid ONCE daily for up to 4
If ineffective or continuous treatment required to maintain control weeks#
and serious risk of steroid induced local side effects
If ineffective after maximum of 8 weeks treatment
If ineffective after 4 weeks#
nd Calcineurin inhibitor (tacrolimus or pimecrolimus) TWICE
2 daily for up to 4 weeks.
Consider using a different formulation of the potent
VitaminD / vitamin analogue TWICE DAILY corticosteroid, e.g. shampoo or mousse
line ONLY to be initiated by healthcare professionals with
expertise in psoriasis
If ineffective after a further 4 weeks#
If ineffective after maximum of 8-12 weeks
Vit D/Vit D analogue
Betametasone 0.05%
ONCE daily for 8 weeks
and Calcipotriol
3rd Potent corticosteroid Coal tar preparation ONCE or 50mcg/g ONCE daily
(only if cannot use
TWICE daily for 4 weeks TWICE daily steroids and
line for up to 4 weeks#
mild/moderate psoriasis)
If these cannot be used or require once daily product to increase If ineffective after treatment duration
adherence
Very potent Referral to a
th REFER adults not controlled on topical treatment to secondary Coal tar
corticosteroid specialist for
4 Betametasone 0.05% and Calcipotriol 50mcg/g ONCE daily care for further treatment options (phototherapy and/or TWICE daily
ONCE or
support and
for up to 4 weeks systemic treatment) TWICE daily
line for 2 weeks# advice
Psoriasis that cannot be controlled by topical treatment should be referred to secondary care for further assessment and treatment
options (these include phototherapy and systemic treatment)
^ Unlicensed indication,
i.e. off-label use.
# Aim for a break of 4 weeks between courses of treatment with potent or very potent corticosteroids.
Consider non-steroid products (coal tar, vit D/vit D analogues) as needed to maintain control of psoriasis during this period
15
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202016
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020BNF 13.5.3 DRUGS AFFECTING THE IMMUNE RESPONSE
There are topical and systemic drugs affecting the immune response which are used for eczema or psoriasis; please use them
only under specialist supervision.
BNF 13.6 ACNE AND ROSACEA
ACNE
Antibacterial resistance of Propionibacterium acnes is increasing; there is cross-resistance between erythromycin and
clindamycin. To avoid development of resistance:
when possible use non-antibiotic antimicrobials (such as benzoyl peroxide or azelaic acid);
avoid concomitant treatment with different oral and topical antibacterials;
if a particular antibacterial is effective, use it for repeat courses if needed (short intervening courses of benzoyl
peroxide may eliminate any resistant propionibacteria);
do not continue treatment for longer than necessary (however, treatment with a topical preparation should be
continued for at least 6 months).
Mild to moderate acne – Topical preparations
Start with a lower strength and increase the concentration of benzoyl peroxide gradually (Over The Counter).
Topical antibacterials are probably best reserved for patients who wish to avoid oral antibacterials or who cannot
tolerate them.
Topical retinoids
Moderate to severe acne – Oral antibiotics. For women only - co-cyprindiol
Severe acne – Refer to dermatologist
Isotretinoin is a Red Traffic Light drug that should be prescribed only by a Secondary Care.
17
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Benzoyl peroxide and azelaic acid
First Choice Alternative
Benzoyl peroxide 2.5-5-10% 40g (Over the Counter) Skinoren® - Azelaic acid 20% cream-30g
Topical antibacterials
First Choice
Dalacin T®
Topical solution, clindamycin 1% (as phosphate), in an aqueous alcoholic basis-30mL
Lotion, clindamycin 1% (as phosphate) in an aqueous basis-30mL
Prescribing benzoyl peroxide (Over the Counter) and Dalacin T® (clindamycin 1%) separately is more cost effective than combined
products. If two separate products are used, they should be applied 12 hours apart. Typically, benzoyl peroxide is applied at night and
the topical antibiotic in the morning.
Topical retinoids
First Choice
Isotrexin® - Gel, isotretinoin 0.05%, erythromycin 2% in ethanolic basis-30g
Oral antibacterials
Topical benzoyl peroxide may also be required.
First Choice Alternative
Oxytetracycline Doxycycline
Tetracycline Lymecycline
18
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020KEY LEARNING POINTS when using antibiotics
The right antimicrobial
• Benzoyl peroxide is the topical antimicrobial of first choice
• When an antibiotic is clinically justified, combine topical⁄systemic therapy with benzoyl peroxide to combat
resistance
• Topical delivery is preferable to oral when acne is localised
For the right patient
• When topical non-antibiotic remedies have failed to bring about adequate control
• For moderate or severe acne while awaiting referral to secondary care
• For extensive inflammatory acne on the trunk
For the right time
• Keep courses of antibiotics short (preferably 3–4 months)
• Use to achieve control but not to maintain control
ROSACEA
Topical ivermectin Gel (Soolantra®) – applied once daily for 4 months with sunscreen. Treatment can be repeated
ONCE only in 12 month period. Discontinue after 3 months if no improvement.
The pustules and papules of rosacea respond to topical metronidazole or to topical azelaic acid
Alternatively, oral administration of oral antibiotics, see above recommendation as for acne
Isotretinoin is occasionally given in refractory cases. Specialist only.
19
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202013.7 PREPARATIONS FOR WARTS AND CALLUSES
Preparations of salicylic acid, formaldehyde, gluteraldehyde or silver nitrate are available OTC for purchase by the
public; they are suitable for the removal of warts on hands and feet.
Anogenital warts
The treatment of anogenital warts (condylomata acuminata) should be accompanied by screening for other sexually
transmitted infections through referral to GUM clinic
First Choice
Podophyllotoxin 0.15% cream - direct medical supervision for lesions greater than 4cm2
Podophyllotoxin 0.5% solution - direct medical supervision for lesions in the female and for lesions greater than 4cm2
Alternative
Imiquimod 5% (Aldara®) – Specialist initiation under GUM
13.8.1 SUNSCREENS PREPARATIONS
To be able to prescribe Sunscreens, ACBS (borderline substance) criteria needs to be satisfied, this is, protection against
ultraviolet radiation in abnormal cutaneous photosensitivity resulting from genetic disorders or photodermatoses, including
vitiligo and those resulting from radiotherapy; chronic or recurrent herpes simplex labialis. Preparations with SPF less than
30 should not be prescribed.
For optimum photoprotection, sunscreen preparations should be applied thickly and frequently (approximately 2 hourly). In
photodermatoses, they should be used from spring to autumn. As maximum protection from sunlight is desirable,
preparations with the highest SPF should be prescribed.
20
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020First Choice
Sunsense® Ultra Lotion (UVA and UVB protection; UVB-SPF 50+).
Please prescribe 125ml or 500ml pump pack
Alternative
Uvistat® cream (UVA and UVB protection; UVB-SPF 50) – 125g
Anthelios® SPF50+ melt – 50ml
Photodamage
An emollient may be sufficient for mild actinic keratosis lesions
Diclofenac gel is suitable for the treatment of superficial lesions in mild disease.
Fluorouracil cream is effective against most types of non-hypertrophic actinic keratosis; a solution containing fluorouracil and salicylic
acid is available for the treatment of low or moderately thick hyperkeratotic actinic keratosis
Imiquimod 3.75% (Zyclara®) and Imiquimod 5% (Aldara®) are used for lesions on the face and scalp when cryotherapy or other
topical treatments cannot be used.
Use of preparations containing Fluorouracil and Imiquimod will require counselling on side effects and consider referral to a specialist
if concerns about diagnosis or suitability of treatment.
First Choice
Diclofenac sodium 3% Gel
Fluorouracil 5% Cream
Fluorouracil 0.5%, salicylic acid 10%
Alternative
Imiquimod 3.75% (Zyclara®) | Imiquimod 5% (Aldara®)
21
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202013.8.2 CAMOUFLAGERS
ACBS (borderline substance) criteria: Post-operative scars and other deformities and as an adjunctive therapy in the relief
of emotional disturbances due to disfiguring skin disease, such as vitiligo.
First Choice
Dermacolor® Camouflage crème 25ml / Fixing powder 60g
Alternative
Keromask® Masking cream 15ml / Finishing powder 20g
13.9 SHAMPOOS AND OTHER PREPARATIONS FOR SCALP AND HAIR CONDICIONS
Psoriasis - Avoid tar shampoos as only ingredient – very low clinical efficacy. Capasal shampoo – coal tar, salicylic acid
and coconut oil is accepted.
Seborrhoeic dermatitis - medicated, anti-dandruff shampoos containing agents such as zinc pyrithione, selenium sulphide
or ketoconazole can be used regularly
Corticosteroids – See section 13.4
Psoriasis – See section 13.5
22
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020First Choice
Selenium sulfide 2.5% Shampoo (Selsun®) - 150 ml
Alternative
Ketoconazole 2% shampoo - 120 ml
Hirsutism
Weight loss can reduce hirsutism in obese women.
Women should be advised about local methods of hair removal, and in the mildest cases this may be all that is required.
Co-cyprindiol (section 13.6.2) may be effective for moderately severe hirsutism.
Metformin (section 6.1.2.2) is an alternative in women with polycystic ovary syndrome [unlicensed indication].
Systemic treatment is required for 6–12 months before benefit is seen.
Eflornithine (as hydrochloride monohydrate) 11.5% (Vaniqa®) cream is not included in the formulary as offers
very little benefit for the management of facial hirsutism in women and there is limited evidence for efficacy and
patient satisfaction with its use, see Eflornithine position statement (NHS England – Low value medicine)
23
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202013.10. ANTI-INFECTIVE SKIN PREPARATIONS
For more information see our Chapter 5 - Infections Formulary
Antibacterial preparations
Topical antibacterials should be avoided on leg ulcers unless used in short courses for defined infections; treatment of
bacterial colonisation is generally inappropriate.
To minimise the development of resistant organisms it is advisable to limit the choice of antibacterials applied topically to
those not used systemically
First Choice
Fusidic acid 2% cream/ointment (Fucidin®)
Alternative
Rozex® - metronidazole 0.75% cream/gel
Mupirocin should be used only to treat meticillin-resistant Staphylococcus aureus
Silver sulfadiazine is used in the treatment of infected burns.
Antifungal preparations
First Choice Alternative
Clotrimazole 1% cream Terbinafine hydrochloride 1% cream
Miconazole nitrate 2% cream Zinc undecenoate 20%, undecenoic acid 2% (Mycota®)
Amorolfine 5% medicated nail lacquer remains non formulary item as there is limited evidence of effectiveness
24
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020Antiviral preparations
First Choice
Aciclovir 5% cream
Parasiticidal preparations
These amounts are usually suitable for an adult for single application
Suitable quantities of parasiticidal preparations
Area of body Skin creams Lotions Cream rinses
Scalp (head lice) — 50–100 mL 50–100 mL
Body (scabies) 30–60 g 100 mL —
Body (crab lice) 30–60 g 100 mL —
These amounts are usually suitable for an adult for single application.
First Choice
Dimethicone 4% - Head lice only. Less active against eggs and treatment should be repeated after 7 days.
Alternative
Lyclear® dermal cream - Permethrin 5% Malathion 0.5% Liquid in an aqueous basis
Products for head lice should be bought Over The Counter (OTC) in Community Pharmacies.
25
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202013.11. SKIN CLEANSERS, ANTISEPTICS, AND DESLOUGHING AGENTS
Alcohols and saline – Sodium Chloride 0.9%
First Choice Alternative
Flowfusor® Bellows pack (120ml) Clinipod® pod (25x20ml)
Irriclens® aerosol (240ml) Sal-e Pods® pod (25x20ml)
The exact number of containers (ie aerosols, bellows packs, bottles, cans, pods, pour bottles or sachets) should be prescribed
Chlorhexidine salts
First Choice Alternative
Hydrex® - chlorhexidine gluconate 2.5% in denatured
Hibiscrub® - chlorhexidine gluconate 4%
ethanol 70%
Iodine
First Choice Alternative
Betadine® dry powder spray – povidone-iodine 2.5% Savlon® dry - dry powder spray – povidone-iodine 1.14%
Oxidisers and dyes
First Choice Alternative
Hydrogen peroxide 6% (20 vols) Permitabs® - Potassium Permanganate 400mg tablets
Wound Care – Octenilin® Bottle 350ml. Refer to EPUT Wound Formulary.
MRSA Decolonisation - Octenisan®. Refer to Management of High Risk MRSA Colonised/Infected Adult Patients
in Nursing Homes and Primary Care Settings
26
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 202013.12. ANTIPERSPIRANTS
First Choice
Aluminium chloride hexahydrate 20% in an alcoholic basis - OTC
Alternative
Antimuscarinics in tablet form
Oxybutynin 5mg BD
Refer patients to Integrated Dermatology Services to try next step – Iontophoresis – Botulinum toxin A
Botulinum toxin type A complex (Botox®) injections can be prescribed and administered in specialist clinics (needs
agreement)
27
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020
Formulary Chapter 13 SKIN
Date ratified by D&T Committee April 2016
1st review – update bath emollients information following position statement April 2017
Date ratified by D&T Committee April 2017
2nd review – Introduce Isomol® gel, Zeroveen®, update bath emollients information following September 2017
advice from dermatologists
Botulinum toxin type A included
Date ratified by D&T Committee September 2017
3rd review – Epimax OAT® added. Bath additives, shower gels and bath oils remove from
formulary. Dovobet® to Enstilar® changed. Corticosteroid creams reviewed, Timodine®
added. Scalp Psoriasis reviewed. Treatment for Acne and Rosacea reviewed, Isotrex® and
November 2018
Stiemycin® removed as discontinued. Treatment for Anogenital warts to be started in
Secondary Care. Imiquimode 5% added for photodamage. Refer to Dermatology Services for
Iontophoresis – Botulinum toxin A.
Date ratified by D&T Committee November 2018
Next Review Date November 2020
4th review – Logos changed January 2019
Skinoren® - Azelaic acid 20% cream-30g, OTC removed as it is a Prescription Only Medicine
(POM)
Date ratified by D&T Committee February 2019
Next Review Date February 2021
5th review – April 2020
Ingenol removed from Photodamage section as discontinued.
Epimax® range edited as names changed.
Date ratified by D&T Committee May 2020
Next Review Date May 2022
28
NHS Castle Point and Rochford CCG
NHS Southend CCG
May 2020You can also read