Original Article The effects of different body positions during ventilation on the cardiopulmonary function, blood gas, and inflammation ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
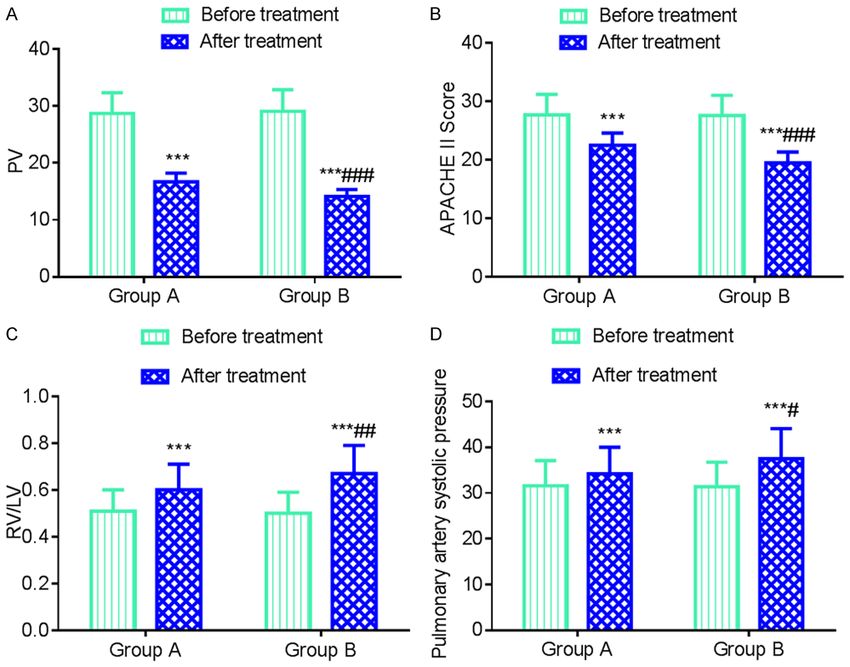
Int J Clin Exp Med 2021;14(5):1919-1927 www.ijcem.com /ISSN:1940-5901/IJCEM0128489 Original Article The effects of different body positions during ventilation on the cardiopulmonary function, blood gas, and inflammation indicators in severe acute respiratory distress syndrome patients Jinyang Zheng1*, Shouyan Liu2*, Junyan Zhang3, Chengyun Zhao4, Jiuhui Zhang5, Yanrong Deng6, Yuguo Wang7 1 Rehabilitation Ward, Taishan Sanatorium of Shandong Province, Taian, Shandong Province, China; Departments of 2Emergency Intensive Care Unit, 3Infection Management, 5Internal Medicine, The First People’s Hospital of Taian, Taian, Shandong Province, China; 4Outpatient Department of Infectious Diseases, The First People’s Hos- pital of Taian, Taian, Shandong Province, China; 6The Second Department of Respiratory, Taian Hospital District, The 960th Hospital of Chinese People’s Liberation Army, Taian, Shandong Province, China; 7Cancer Center Office, Taian Cancer Prevention and Treatment Hospital, Taian, Shandong Province, China. *Equal contributors and co- first authors. Received December 17, 2020; Accepted January 21, 2021; Epub May 15, 2021; Published May 30, 2021 Abstract: Objective: To explore the effects of different body ventilation positions on the cardiopulmonary function, blood gas levels, and inflammatory indicators in severe acute respiratory distress syndrome patients. Methods: Eighty-eight patients with severe acute respiratory distress syndrome were randomly divided into group A (n=44) and group B (n=44). The patients in group A were treated with mechanical ventilation in the supine position, and the patients in group B were treated with mechanical ventilation in the lateral position. The cardiopulmonary function indicator changes (the pulmonary ventilation scores, acute physiology and chronic health scores, pulmonary artery systolic pressure levels, and RV/LV), the blood gas indicators (PaO2, PaCO2, SpO2, PaO2/FiO2), the inflammatory indicators (IL-6, IL-8, TNF-α), the hemodynamic indicators (HR, SBP, DBP), the mechanical ventilation times, hospital stay durations, and the adverse reactions before and after the treatment were compared between the two groups. Results: After the treatment, the PV and APACHE II scores in the two groups were significantly reduced, the RV/LV and pulmonary artery systolic pressures were significantly increased, and the improvement in group B was bigger than it was in group A (P
Ventilation body positions in ARDS
Table 1. Comparison of the general data between the two groups cial bed, which can allow a
_
( x ± sd; n, %) maximum rotation of 124°
Group A Group B
axial rollover, that is, me-
Group t/χ2 P chanical ventilation in a lat-
(n=44) (n=44)
eral decubitus position.
Gender (male/female) 28/16 26/18 0.192 0.661
One experiment revealed
Age (years) 48.6±6.2 49.5±6.7 0.654 0.515
that this position can ef-
Body Mass Index (kg/m2) 21.59±1.84 22.07±1.98 1.178 0.242 fectively improve oxygen-
ICU stay (d) 8.3±2.1 8.7±2.2 0.872 0.385 ation without affecting the
Etiological constitution 1.636 0.201 hemodynamics [8]. It is
Pancreatitis 11 (25.00) 13 (29.55) important because this
Severe pneumonia 15 (34.09) 16 (36.36) position is more labor-sav-
Sepsis 9 (20.45) 8 (18.18) ing than the supine posi-
tion, easy to implement,
Aspiration 4 (9.09) 3 (6.82)
meets more physiological
Postoperative infection 5 (11.36) 4 (9.09)
needs, and improves pati-
Concomitant underlying disease 0.258 0.611 ent comfort. Based on this,
Diabetes 8 (18.18) 9 (20.45) this study explored the
Hypertension 14 (31.82) 15 (34.09) effects of different ventila-
Other 9 (20.45) 7 (15.91) tion body positions on the
cardiopulmonary function,
blood gas levels, and in-
Medicine. Mechanical ventilation is the main flammatory indicators in patients with severe
method of respiratory support therapy. Al- acute respiratory distress syndrome. It is re-
though there have been rapid advances in ported as follows.
modern clinical lung protective strategies for
mechanical ventilation, such as limiting the Materials and methods
platform pressure and low tidal volume mech-
anical ventilation, there is still a high mortality General data
rate among the critically ill patients. The cor-
rect ventilation strategy is the key to saving A total of 88 patients with severe acute res-
patients’ lives [2, 3]. piratory distress syndrome admitted to The
First People’s Hospital of Taian from January
The supine position is the most conventional 2019 to February 2020 were recruited as the
position used for ventilation, and it has a good study cohort and randomly divided into group
effect. However, since the patient is kept in A and group B, with 44 patients in each group.
supine position for a long time, it will com- There was no significant difference in the gen-
press the skin to different extents, resulting in eral data between the two groups (P>0.05).
circulatory disorders and increasing the risk of See Table 1. The study was reviewed and
pressure ulcers [4]. In recent years, a number approved by the Medical Ethics Committee of
of studies have confirmed that supine position The First People’s Hospital of Taian.
ventilation is a salvage treatment for patients
with severe acute respiratory distress syndro- Inclusion criteria
me. It can significantly improve the patients’
oxygenation indicators and reduce their mor- Inclusion criteria: All the patients met the crite-
tality in the short term [5, 6]. However, the ria for the diagnosis of severe acute respiratory
supine position is not a physiological position, distress syndrome according to the European
so it is difficult to achieve the supine position Critical Care Medicine diagnostic criteria for
during ventilation, especially for obese pati- severe acute respiratory distress syndrome,
ents, and there are also many controversies patients whose PaO2/FiO2 levels were ≤100
about the effects of ventilation in the supine mmHg, patients whose PEEP levels were ≥10
position on the patient’s cardiopulmonary cmH2O, patients with an acute onset of the dis-
function [7]. Compared with the ventilation in ease, patients whose X-rays showed an infiltra-
the supine position, the application rate of tion shadow, patients whose mechanical venti-
mechanical ventilation in the lateral decubitus lation times were >72 h, and patients whose
position is lower, and there are few relevant families signed the informed consent form for
studies. Some foreign researchers use a spe- the study [9].
1920 Int J Clin Exp Med 2021;14(5):1919-1927Ventilation body positions in ARDS
Exclusion criteria: Patients with hemodynamic Outcome indicators
instability, patients with tumors, intracranial
hypertension, or spinal injuries, patients who Cardiopulmonary function indicators
had undergone fracture surgery or abdominal
surgery, patients with a head and face injury, The total pulmonary ventilation scores: The
patients with mandatory respiratory depres- pulmonary ventilation (PV) was evaluated using
sion, pulmonary encephalopathy, patients who pulmonary ultrasonography, and the total pul-
abandoned the treatment or who died halfway monary ventilation score was calculated [11];
through the study, obese patients, patients (1) 0 point (N): less than 3 isolated B lines or
with an abnormal immune system, and pati- lung sliding signs were observed in the nor-
ents with a history of tracheal transplantation. mal ventilation area; (2) 1 point (B1): moderate
lung tissue loss of pneumatization, and multi-
Methods ple clear B lines were observed; (3) 2 points
(B2): severe lung tissue loss of pneuma-
All the patients were given anti-infection, acid- tization, and the fusion B line density was
base balance, water and electrolyte balance observed; (4) 3 points (C): lung parenchyma,
corrections, nutritional support and other which could resemble hepatoid structures and
symptomatic treatment according to their bronchial inflation signs; 3 points (C/P): com-
pathogenesis. A Drager Savina 300 ventilator bined pleural effusion, and the worst value
(Draegerwerk AG & Co. KGaA, Germany) was during the ventilation was used as the mea-
used according to the Guidelines for Mechani- surement result, and all the scores were accu-
cal Ventilation in Patients with Acute Res- mulated as PV.
piratory Distress Syndrome, using intermittent
positive pressure ventilation or intermittent APACHE ll scores: The patient’s condition and
mandatory ventilation + pressure support ven- prognosis were evaluated using Acute Phy-
tilation support mode [10]. The respiratory siology and Chronic Health Evaluation (APA-
rate was 14-20 times/min, the respiratory rate CHE ll score), mainly including three parts:
was 1:2, the tidal volume was 6-8 mL/kg, the acute physiology, chronic health status, and
PEEP was 6-10 cmH2O, and the FiO was 40%- age [12]. The final score was the sum of the
60%. Before the ventilation, the each patient’s three, with a total possible score of 71 points,
respiratory secretions were fully cleared, and and the higher the score, the more severe the
after the start of mechanical ventilation, intra- condition.
venous sedation with 5 μg/kg midazolam
RV/LV and pulmonary artery systolic pressure:
(Jiangsu Jiuxu Pharmaceutical Co., Ltd., China)
The ratio of the right ventricular end-diastolic
and 15 μg/kg fentanyl (Langfang Branch of
diameter to the left ventricular end-diastolic
China National Pharmaceutical Industry Co.,
diameter (RV/LV) and the pulmonary arterial
Ltd., China) was required, followed by a con-
systolic pressure were measured using vivid E8
trolled intravenous infusion of 0.3-0.6 μg/
echocardiography (GE, USA).
(kg·min) midazolam and 0.025-0.1 μg/(kg·min)
fentanyl using an infusion pump. If necessary, Blood gas indicators
muscle relaxation was maintained using an
intermittent intravenous injection of 0.08-0.1 Four milliliters of peripheral venous blood were
mg/kg vecuronium (Jiangsu Huatai Chenguang drawn from the patients before and after the
Pharmaceutical Co., Ltd., China). Group A was treatment, and the serum was obtained using
treated with mechanical ventilation in the centrifugation at 2,500 r/min for 15 min. The
supine position, with the head of the bed ele- arterial partial pressure of oxygen (PaO2), the
vated 30°-40°. Group B was treated with arterial partial pressure of carbon dioxide
mechanical ventilation in the lateral decubitus (PaCO2), the saturation (SpO2), and oxygena-
position, and after monitoring each patient’s tion indicators (PaO2/FiO2) levels were mea-
hemodynamic stability, the head was deviated sured using a GEM3000 blood gas analyzer
to the right, and the trunk and buttocks were (Beckman, USA).
inclined to the right, and a soft pillow was used
as padding to prevent the compression of the Inflammatory indicators
facial limbs, and the left leg was rotated 90° to
the right, the right leg was extended, and the Four milliliters of peripheral venous blood were
patient was transferred to supine ventilation drawn from the patients before and after the
1-2 hours later. treatment, and the serum was obtained throu-
1921 Int J Clin Exp Med 2021;14(5):1919-1927Ventilation body positions in ARDS
_
Table 2. Comparison of the cardiopulmonary function between the two groups ( x ± sd)
Group Group A (n=44) Group B (n=44) t P
PV (points)
Before treatment 27.68±3.51 27.57±3.46 0.148 0.883
After treatment 22.45±2.14*** 19.45±1.87*** 7.002Ventilation body positions in ARDS Figure 1. Comparison of the cardiopulmonary function between the two groups. A: PV; B: APACHE II scores; C: RV/LV; D: Pulmonary artery systolic pressure. Compared with the group before the treatment, ***P
Ventilation body positions in ARDS
Table 4. Comparison of the inflammatory indicators between the Adverse reactions
_
two groups ( x ± sd)
Group A Group B
There was no significant differ-
Group t P ence in the incidence rate of
(n=44) (n=44)
adverse reactions between the
TNF-α (μg/mL)
two groups (P>0.05). See Table
Before treatment 17.03±2.98 17.05±3.05 0.031 0.975
7.
After treatment 10.39±2.14*** 8.47±1.52*** 4.852Ventilation body positions in ARDS
Table 7. Comparison of the adverse reactions between the two groups (n, (%))
Group Flatulence Blood pressure decreased Sedation too deep Lung infection Total Occurrence
Group A (n=44) 0 (0.00) 2 (4.55) 1 (2.27) 0 (0.00) 3 (6.82)
Group B (n=44) 1 (2.27) 1 (2.27) 0 (0.00) 1 (2.27) 3 (6.82)
χ2 0.000
P 1.000
[15]. Kong et al. pointed out that mechanical allow a collapse and atelectasis by reducing
ventilation in the lateral decubitus position can this gradient, which is also consistent with the
effectively reduce the inflammatory response thrust of the strategies for the treatment of
in acute respiratory distress syndrome and acute respiratory distress syndrome [18, 19].
ventilation in the lateral position combined 2) With lateral decubitus ventilation, the pul-
with vibration expectoration is better [16]. The monary edema fluid will be redistributed ven-
results of this study pointed out that the in- trally, which promotes the collapse and atelec-
flammatory factor levels in both groups were tasis alveolar recruitment [20]. 3) Gattinoni et
reduced after the treatment, confirming that by al. pointed out that patients with acute res-
improving oxygenation, the inflammatory res- piratory distress syndrome were treated with
ponse can be reduced to a certain extent, and supine mechanical ventilation, and the shunt
the improvement in group B was better than it site was vertically distributed along the axial
was in group A, suggesting that mechanical direction of gravity, resulting in a transpulmo-
ventilation in the lateral decubitus position nary pressure lower than the airway opening
improves oxygenation and has a better effect pressure, affecting the ventilation effect, while
in controlling the inflammatory response. lateral position ventilation can reduce the par-
tial gravity dependence, and then improve the
According to the results of the study, the ventilation effect [21]. 4) Thoracic pressure
improvement in the blood gas indicators in will increase pulmonary vascular resistance,
group B was better than it was in group A, and increase right heart afterload, and lead to
the improvement in the cardiopulmonary func- abnormal cardiac function. The lateral decubi-
tion was better than it was in group A, suggest- tus position can improve the ventilation status
ing that mechanical ventilation in the lateral of the compressed area through the direct
decubitus position is more conducive to im- effect of abdominal organ weight, eliminating
proving patients’ respiratory and cardiopulmo- the compression effect of solid lung tissue and
nary functions. Li et al. pointed out that lateral the compression effect of the lung tissue and
decubitus ventilation can improve oxygenation heart [22, 23]. 5) The lateral decubitus posi-
and airway sputum drainage in patients with tion changes the position of the diaphragm
acute respiratory distress syndrome, but it has and the mode of movement of the phrenic
no significant effect on the hemodynamics and nerve, which facilitates the regulation of the
ventilator mechanical indicators, which is also respiratory movement and improves the venti-
consistent with the results of this study [17]. latory function. At the same time, the lateral
Although the mechanism of improving oxygen- decubitus position is prone to increase the
ation using mechanical ventilation in lateral flow into the large airway due to gravity, which
decubitus position has not yet been clarified, it also facilitates the drainage of secretions and
may be due to the following facts learned from makes the drainage more adequate [24]. 6)
the results of this study: 1) Due to the gravity- The patient is in a supine position for a long
dependent effect, when the patient is in a time without any muscle movement, which can
supine position, the thoracic pressure gradient also easily affect the blood circulation and
will be increased from ventral to dorsal, and the form complications such as deep venous
pulmonary exudate can easily fall in the droop- thrombosis and pressure ulcers. Appropriate
ing lung area, aggravating the regional lesions, turning can also prevent these complications,
which is also an important theoretical basis enhance muscle strength, and have positive
for the postural treatment of the disease. implications for the disease outcome. The re-
Mechanical ventilation in the lateral decubitus sults of this study showed that the hemody-
position can increase lung volume and can namics of patients in both groups were stable
1925 Int J Clin Exp Med 2021;14(5):1919-1927Ventilation body positions in ARDS
during the treatment, and the incidence of Address correspondence to: Shouyan Liu, De-
adverse reactions was also low, indicating that partment of Emergency Intensive Care Unit, The
mechanical ventilation in the lateral decubitus First People’s Hospital of Taian, No. 289 Lingshan
position will not cause severe fluctuations in Street, Taishan District, Taian 271000, Shandong
HR, MAP, etc. due to the change of body posi- Province, China. Tel: +86-15092833298; E-mail:
tion for patients in a critical condition. On the liushouyan1tai@163.com
other hand, our results indicate that this body
References
position is effective and safe for improving the
prognosis, without increasing the patient’s dis- [1] Huppert LA, Matthay MA and Ware LB. Patho-
comfort. The mechanical ventilation and hospi- genesis of acute respiratory distress syn-
tal stays in group B were also higher/longer drome. Semin Respir Crit Care Med 2019; 40:
than they were in group A, indicating that 31-39.
mechanical ventilation in the lateral decubi- [2] Fan E, Brodie D and Slutsky AS. Acute respira-
tus position can also help patients breathe tory distress syndrome: advances in diagnosis
spontaneously as soon as possible and pro- and treatment. JAMA 2018; 319: 698-710.
[3] Reilly JP, Calfee CS and Christie JD. Acute re-
mote the rehabilitation from the disease.
spiratory distress syndrome phenotypes. Se-
min Respir Crit Care Med 2019; 40: 19-30.
In addition, a common complication of mech-
[4] Pan C, Liu L, Xie JF and Qiu HB. Acute respira-
anical ventilation is ventilator-associated lung tory distress syndrome: challenge for diagno-
injury, and the lung-protective mechanical ven- sis and therapy. Chin Med J (Engl) 2018; 131:
tilation strategy can avoid the excessive ex- 1220-1224.
pansion of the alveoli and pull the vascular [5] Saran S, Gurjar M, Kanaujia V, Ghosh PS, Gup-
endothelial cells and alveolar epithelium th- ta A, Mishra P, Azim A, Poddar B, Baronia A and
rough the neap tidal volume and optimal PEEP, Singh R. Effect of prone positioning on intra-
so as to better improve body oxygenation and ocular pressure in patients with acute respira-
enhance the prognosis. Mechanical ventilation tory distress syndrome. Crit Care Med 2019;
47: e761-e766.
in the lateral decubitus position decreases the
[6] Munshi L, Del Sorbo L, Adhikari NKJ, Hodgson
thoracic pressure and reduces the repeated CL, Wunsch H, Meade MO, Uleryk E, Mancebo
opening and closing and overdistension of the J, Pesenti A, Ranieri VM and Fan E. Prone posi-
airways in gravity-dependent and non-gravity- tion for acute respiratory distress syndrome. a
dependent areas of the lungs, thereby redu- systematic review and meta-analysis. Ann Am
cing ventilator-associated lung injuries [25]. Thorac Soc 2017; 14: S280-S288.
[7] Derwall M, Martin L and Rossaint R. The acute
In summary, mechanical ventilation therapy in respiratory distress syndrome: pathophysiolo-
the lateral decubitus position can effectively gy, current clinical practice, and emerging ther-
and safely improve cardiopulmonary function, apies. Expert Rev Respir Med 2018; 12: 1021-
1029.
improve oxygenation, and reduce the in-
[8] Kong L, Li J, Wu P, Xu J, Li H, Long H, Liu P, Wei
flammatory responses in patients with severe
F and Peng W. Effect of lateral position ventila-
acute respiratory distress syndrome. However, tion combined with vibration sputum drainage
there may be bias in the results due to the on patients with acute respiratory distress syn-
small sample size in this study. Due to the in- drome: a prospective randomized controlled
fluence of time, funds and other factors, the trial. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue
study did not explore whether cardiopulmonary 2018; 30: 240-245.
function injury caused by mechanical ventila- [9] Ranieri VM, Rubenfeld GD, Thompson BT, Fer-
tion can be recovered. Since the patients were guson ND, Caldwell E, Fan E, Camporota L and
Slutsky AS. Acute respiratory distress syn-
given relevant symptomatic treatment during
drome: the Berlin definition. JAMA 2012; 307:
the ventilation therapy, which may have also 2526-2533.
affected the study results, it is necessary to [10] Respiratory Critical Care Medicine Group and
prolong the follow-up and related mechanisms Chinese Society of Respiratory Disease. Guide-
in the future for further in-depth studies. lines for mechanical ventilation in patients
with acute respiratory distress syndrome (tri-
Disclosure of conflict of interest al). Chin Med J (Engl) 2016; 96: 5.
[11] Yao YL, Lei M, Li WF and Lin ZF. Value of pulmo-
None. nary ventilation score in assessing extravascu-
1926 Int J Clin Exp Med 2021;14(5):1919-1927Ventilation body positions in ARDS
lar lung water in patients with acute respiratory [20] Spieth PM, Güldner A and Gama de Abreu M.
distress syndrome. J Second Mil Med Univ Acute respiratory distress syndrome: basic
2018; 39: 57-61. principles and treatment. Anaesthesist 2017;
[12] Li L, Yang Q, Li L, Guan J, Liu Z, Han J, Chao Y, 66: 539-552.
Wang Z and Yu X. The value of lung ultrasound [21] Gattinoni L, Busana M, Giosa L, Macrì MM and
score on evaluating clinical severity and prog- Quintel M. Prone positioning in acute respira-
nosis in patients with acute respiratory dis- tory distress syndrome. Semin Respir Crit Care
tress syndrome. Zhonghua Wei Zhong Bing Ji Med 2019; 40: 94-100.
Jiu Yi Xue 2015; 27: 579-584. [22] Zhou Y, Jin X, Lv Y, Wang P, Yang Y, Liang G,
[13] Fielding-Singh V, Matthay MA and Calfee CS. Wang B and Kang Y. Early application of airway
Beyond low tidal volume ventilation: treatment pressure release ventilation may reduce the
adjuncts for severe respiratory failure in acute duration of mechanical ventilation in acute re-
respiratory distress syndrome. Crit Care Med spiratory distress syndrome. Intensive Care
2018; 46: 1820-1831. Med 2017; 43: 1648-1659.
[14] Coudroy R, Chen L, Pham T, Piraino T, Telias I [23] Russotto V, Bellani G and Foti G. Respiratory
and Brochard L. Acute respiratory distress syn- mechanics in patients with acute respiratory
drome: respiratory monitoring and pulmonary distress syndrome. Ann Transl Med 2018; 6:
physiology. Semin Respir Crit Care Med 2019; 382.
40: 66-80. [24] Aoyama H, Uchida K, Aoyama K, Pechlivano-
[15] Cardinal-Fernández P, Lorente JA, Ballén-Bar- glou P, Englesakis M, Yamada Y and Fan E. As-
ragán A and Matute-Bello G. Acute respiratory sessment of therapeutic interventions and
distress syndrome and diffuse alveolar dam- lung protective ventilation in patients with
age. New insights on a complex relationship. moderate to severe acute respiratory distress
Ann Am Thorac Soc 2017; 14: 844-850. syndrome: a systematic review and network
[16] Kong L, Li J, Wu P, Xu J, Li H, Long H, Liu P, Wei meta-analysis. JAMA Netw Open 2019; 2:
F and Peng W. Effect of lateral position ventila- e198116.
tion combined with vibration sputum drainage [25] Constantin JM, Jabaudon M, Lefrant JY, Jaber
on patients with acute respiratory distress syn- S, Quenot JP, Langeron O, Ferrandière M, Gre-
drome: a prospective randomized controlled lon F, Seguin P, Ichai C, Veber B, Souweine B,
trial. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue Uberti T, Lasocki S, Legay F, Leone M, Eisen-
2018; 30: 240-245. mann N, Dahyot-Fizelier C, Dupont H, Aseh-
[17] Qiu ZF, Cui HY, Li QY, Pei JS, Xiang B and Zhang noune K, Sossou A, Chanques G, Muller L, Ba-
GP. Efficacy of lateral position ventilation in pa- zin JE, Monsel A, Borao L, Garcier JM, Rouby JJ,
tients with acute respiratory distress syn- Pereira B and Futier E. Personalised mechani-
drome. Clin Meta-Anal 2015; 30: 51-53. cal ventilation tailored to lung morphology ver-
[18] Grassi A, Foti G, Laffey JG and Bellani G. Nonin- sus low positive end-expiratory pressure for
vasive mechanical ventilation in early acute patients with acute respiratory distress syn-
respiratory distress syndrome. Pol Arch Intern drome in France (the LIVE study): a multicen-
Med 2017; 127: 614-620. tre, single-blind, randomised controlled trial.
[19] Matthay MA, McAuley DF and Ware LB. Clinical Lancet Respir Med 2019; 7: 870-880.
trials in acute respiratory distress syndrome:
challenges and opportunities. Lancet Respir
Med 2017; 5: 524-534.
1927 Int J Clin Exp Med 2021;14(5):1919-1927You can also read

















































