Cardiac Device Summit Basel - Donnerstag, 11.4.2019, 11.15 -18.20 Uhr Kleiner Hörsaal, ZLF - Universitätsspital Basel - Universitätsspital Basel
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cardiac Device Summit Basel
Donnerstag, 11.4.2019, 11.15 -18.20 Uhr
Kleiner Hörsaal, ZLF – Universitätsspital Basel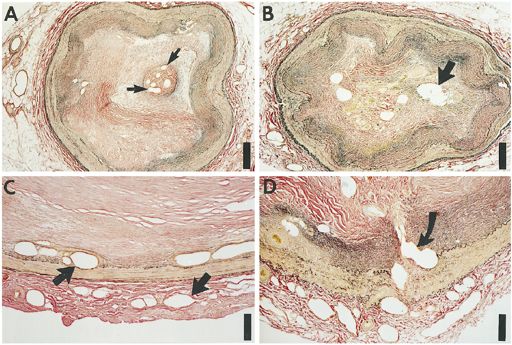
CTO
Chronic Total Occlusion
CHIP
Complex High-Risk Indicated Procedure/Patients
PD Dr. med. Gregor Leibundgut
Leitender Arzt
Leiter Kardiologie und Herzkatheterlabor
Medizinische Universitätsklinik
Kantonsspital Baselland
26.04.2018 | 14:10-14:20 17:20 -17:40 Uhr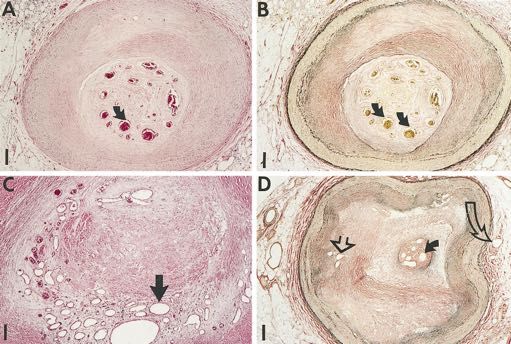
PCI vs CABG bei
Mehrgefässerkrankung inkl. CTO
PCI CABG
Procedural Less invasive Higher procedural risk
Less complete Complete revascularization
Hospital Earlier recovery
Lower initial cost
Later outcomes BMS 10-20% restenosis Ecellent for LIMA, DM
DES 2-8% restenosis SVG closure 40% at 10y
Other complications Repeat procedures Neurologic banormalities
Adhesions/scarring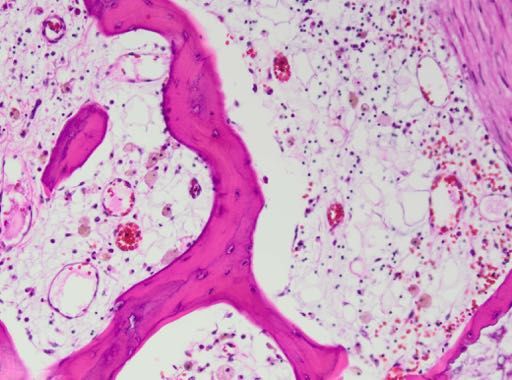
SYNTAX MACE über 5 Jahre Articles
Alle Hauptstamm 3-GE-KHK
A Overall cohort B Left main coronary disease subgroup C Three-vessel disease subgroup
Baseline SYNTAX score 0–22 Baseline SYNTAX score 0–22 Baseline SYNTAX score 0–22
50 CABG p=0·43 p=0·74 p=0·21
PCI
31·5% 33·3%
Cumulative event rate (%)
32·1%
Syntax 0-22
25
28·6% 30·4%
26·8%
0
0 12 24 36 48 60 0 12 24 36 48 60 0 12 24 36 48 60
Months since allocation Months since allocation Months since allocation
Number at risk
CABG 275 226 221 212 197 154 104 87 86 80 74 56 171 137 135 133 123 98
PCI 299 263 255 237 223 168 118 109 108 98 93 68 181 154 147 139 130 100
Baseline SYNTAX score 23–32 Baseline SYNTAX score 23–32 Baseline SYNTAX score 23–32
50 p=0·008 p=0·88 p=0·0008
37·9%
36·0% 32·7%
Cumulative event rate (%)
Syntax 23-32 25
32·3%
25·8%
22·6%
0
0 12 24 36 48 60 0 12 24 36 48 60 0 12 24 36 48 60
Months since allocation Months since allocation Months since allocation
Number at risk
CABG 300 251 248 230 219 172 92 75 74 66 66 51 208 176 174 164 153 121
PCI 310 257 256 236 221 173 103 91 90 79 78 60 207 166 166 157 143 114
Baseline SYNTAX score ≥33 Baseline SYNTAX score ≥33 Baseline SYNTAX score ≥33
50 p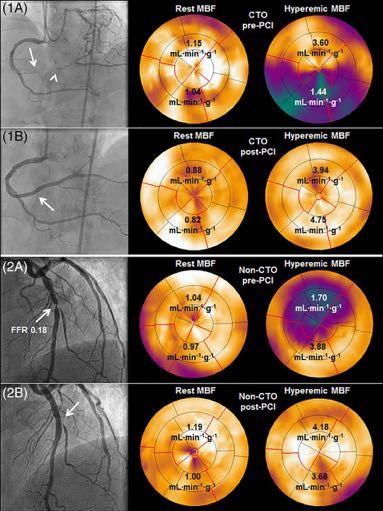
Therapieoptionen
Ohne CTO Mit CTO
9%
22%
18%
47%
73% 31%
ΔPCI = 26%
medikamentös Bypass PCI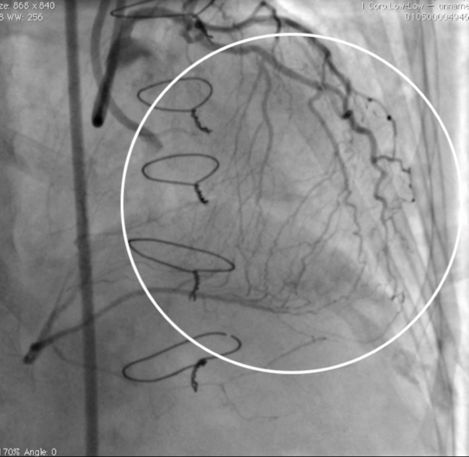
CTO - Chronic Total Occlusion • Kompletter chronischer Verschluss - TIMI 0 grade Blutfluss - antegrade und/oder retrograde Kollateralen • Verschlussdauer > 3 Monate - angiographisch - klinisch • Viabilität ?

Prävalenz und Lokalisation • 15-30% aller Koronarangiographien ! • Gefässbeteiligung - RIA 22% - RCX 18% - ACD 60% - multiple locations 17% - proximal segment 68%
Angiographie

Nativkalk als „Road-map“

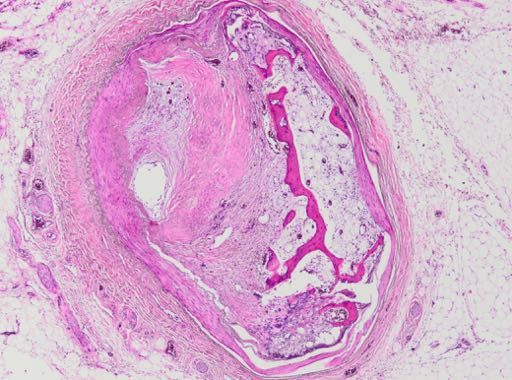
Histologie Srivatsa et al. JACC 1997;29:955-63
Morphologische Charakteristika
Calcification
Calcification Necrotic core
Macrophage infiltration
Ca2+ Necrotic core Ca2+ Hemosiderin deposition
SMC infiltration
Luminal thrombus Proteoglycan deposition
Intravascular neoangiogenesis
NC NC
Akuter Verschluss Frühe CTO
Calcification
Calcification Necrotic core
Necrotic core
Ca2+ Large recanalized channels
Ca2
Collagen matrix surrounded by SMC
Negative remodeling Improvement of distal flow
NC NC Minimal negative remodeling
Späte CTO Späte CTO
mit negativem Remodeling mit physiologischer RekanalisationKoronarknochen
*
*
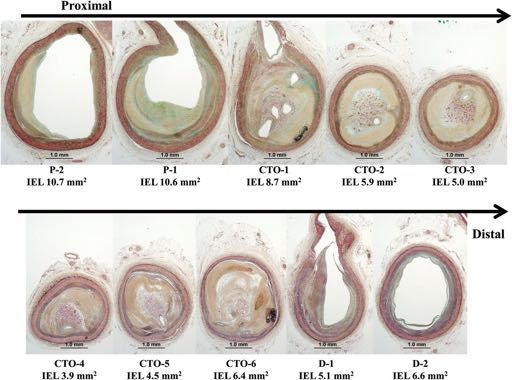
Leibundgut G et al. Circulation 20153D-Charakteristika von
Characteristics of a CTO
CTOs
Proximal fibrous cap Distal fibrous cap
Microchannels Calcified areas
Necrotic areas Hard artherosclerotic
plaquefrom the collateral-supplying vessel into the distal vessel. The
catheter. (B) Kissing wire technique: the retrograde guidewi
from the antegrade direction. Finally, both the antegrade an
Wo liegt der Unterschied?
advanced to the distal vessel.
Source: Courtesy to Dr M Ochiai.
The following is the stepwise approach for the re
Stenose recanalization for CTO:
• Angiographic film and collateral channel analysis
• Retrograde collateral channel access and crossi
presence and tortuosity of collaterals are key is
selecting a retrograde interventional strategy when
CTOs. Nontortuous septal collaterals are preferentia
for the retrograde approach, whereas epicardial
tortuous collaterals are at higher risk of procedure
vessel trauma
• Crossing the CTO: Novel over-the-wire (OTW)
CTO (channel dilator) specifically designed for the ret
approach has been developed for the treatment
Successful channel crossing of the catheter was a
in 96.8%, and the channel dilator successfully ad
into the occlusion reversely during retrograde w
94.4%.39
• Wiring the antegrade guide, snaring, and externa
Of the several available retrograde wiring techniq
reverse CART technique has become the most co
used technique in the Corsair era because retrograde
access is not requiredIt’s all about Collaterals! 958 SRIVATSA ET AL.
HISTOPATHOLOGY OF ANGIOGRAPHIC CHRONIC TOTAL O
385 μm
385 μm
Current fluoroscopy systems allow visualisation Figure
of channels
2. A and B, Low power≥views
250-300 µm
(hematoxylin-eosin and Lawson’s
elastic van Gieson stains) of chronic total occlusion lumen recanaliza-
tion by large central neovascular channels (NCs) (arrows). Scale bar
indicates 385 mm. C, High power view (hematoxylin-eosin stain)
demonstrating extensive small, medium and large intimal plaque (IP)
NCs (arrows). Scale bar indicates 167 mm. D, Low power view (elasticAusreichende Kollateralisation
In nur 20% nach akutem Koronarverschluss (CFI >0.25)
No CAD coronary 3-vessel disease
Frequency (%)
Collateral Flow Index (CFI) Collateral Flow Index (CFI)
CFI = poccl - CVP
paorta - CVP
Meier P et al. Circulation 2007Lebensdauer der Bypässe
Retrospective review of coronary angiograms 1996-2001
Selection bias
Khot,UN et al. Circulation 2004;109:2086-209Inkomplette Revaskularisation • Vorliegen einer CTO ist häufigste Ursache nicht randomisiert zu werden in grossen Studien (BARI, SYNTAX) • 47% Fehlversuche der CTO-PCI in der SYNTAX Studie • Patienten mit inkompletter Revaskularisation haben eine schlechtere Langzeitprognose
(11.9
Figure 1 Kaplan– Meier analysis of cardiac survival in patients
(15.9
with chronic total occlusion (CTO)– percutaneous coronary
Completeness of Revascularization
intervention (PCI) success when compared to patients with
CTO–PCI failure.
siroli
Patients with at least one CTO Di
The
2-yea
differ
and w
with
PCI.
cant
the r
tion
N=344
nitio
succe
Su
val w
Figure
Valenti R et al. EHJ 2008 2 Kaplan– Meier analysis of cardiac survival in patients
survients COURAGE:
PatientsIschämie und
with mod-sev Outcome
ischemia
al. Circulation 2008;117:1283-1291PET Perfusion
PET nach after
Perfusion CTO-PCI
CTO an
p
Schumacher et al. CCI 2018Meta-Analysis of CTO Outcomes
23 Observational Studies, 12,970 patients, mean f/u 3.7±2.1 yrs
100 Khan et al.
all-cause mortality
RR 0.54 (95%-CI 0.446-0.650) pFuture Coronary Occlusion Events
CTO
STEMI
××
RCA
LCX
LAD
RCA LAD LCXJACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 11, 2009
(HR: 1.1, 95% CI: 0.8 to 1.6, p " 0.51).
NOVEMBER 2009:1128 –34 Impact of a CTO on LVEF. In our study population of 3,277 Impact of a
patients, residual LVEF measurements were available in
1,745 patients (53%). A total of 1,674 patients underwent
echocardiography, and 71 patients underwent scintigraphy
Einfluss einer CTO auf die Mortalität beim Herzinfarkt within 30 days after the index event. Median time to LVEF
measurement was 3 days (IQR 2 to 5 days); time to LVEF
measurement was not statistically different among SVD,
Figure 1. Landmark Survival Analysis MVD, and CTO patient groups. Among the 1,745 patientsand 5-year mortality, exclu
Cumulative risk of death during the first 30 days after primary percutane-
had SVD, 386 patients (22%) had MVD, and 200 patients
days (HR: 1.9, 95% CI: 0.8
for whom LVEF data were retrieved, 1,159 patients (66%)
ous coronary intervention (PCI) and thereafter for patients with single-
vessel disease (SVD), multivessel disease (MVD), and a chronic total occlu- (11%) had a concurrent CTO. The baseline clinical of and
MVD without a concurre
sion (CTO). angiographic characteristics of patients with LVEF are
statistically significant inde
shown in Table 1 and compare well to characteristics of the
MVD without CTO group, and 38% in the MVD with total cohort. This indicates that this subset seems amortality
repre- (HR: 1.6, 95% C
concurrent CTO group. sentative sample of the total STEMI cohort.
During the first 30 days after STEMI, the mortality rate forhad
Of the 1,745 patients, a total of 307 patients (18%) 5-year mortality
CTO nicht im excludin
was significantly higher in patients with a concurrent CTO (HR:Infarktgefäss
an LVEF !40%. Figure 2 shows the proportions of patients 1.1, 95% CI: 0.8 to 1
in a non-IRA, compared with patients with SVD (unad- with an LVEF !40% in each patient group. The propor-
justed HR: 5.3, 95% confidence interval [CI]: 4.0 to 7.0, tions of patients with an LVEF !40% were 16%Impact in the of a CTO on LVEF. I
SVD group, 18% in the MVD without CTO group, and
p ! 0.01). Compared with patients with SVD, mortality
was also higher in patients with MVD without a concurrent 28% in the MVD with concurrent CTO group (p ! 0.01).
patients, residual LVEF m
CTO (unadjusted HR: 2.0, 95% CI: 1.5 to 2.7, p ! 0.01). The presence of a CTO in a non–IRA was a significant 1,745 patients (53%). A tot
Table 2 shows the adjusted Cox proportional HRs for death predictor for a residual LVEF !40% (odds ratio [OR]: 2.0,
during the first 30 days, and during 30 days to 5 years after
echocardiography,
95% CI: 1.4 to 2.8). After correction for the presence of and 71 p
primary PCI. After adjusting for the aforementioned vari- MVD without CTO and differences in the aforementionedwithin 30 days after the inde
ables, the presence of a CTO in a non-IRA was still found variables, the presence of a CTO in a non-IRA remained an
to be a strong and independent predictor for both 30-day independent predictor for a residual LVEF !40% with measurement
an was 3 days (IQ
mortality, with an HR of 3.6 (95% CI: 2.6 to 4.7, p ! 0.01) measurement was not stat
OR of 1.8 (95% CI: 1.2 to 2.7, p ! 0.01). Other indepen-
Table 2. IndependentFigure
Predictors1.
for Landmark
Death During theSurvival Analysis
First 30 Days and During 30 Days to 5 Years After Primary PCI MVD, and CTO patient gr
Predictors for Death During the First 30 Days Predictors for Death From 30 Days to 5 for
Yrs whom LVEF data were
Cumulative risk of deathAfter during the first 30 days after primary percutane-
Primary PCI After Primary PCI
ous coronaryHRintervention95% (PCI)
CI
and thereafter p Value
for patients
HR
with single- 95% CI
had
p Value
SVD, 386 patients (22%
Shock
vessel disease (SVD), multivessel disease (MVD), and a chronic total occlu-
7.4 5.8–9.6 !0.01 1.6 1.0–2.4
(11%)
0.04
had a concurrent C
CTO sion (CTO). 3.6 2.6–4.7 !0.01 1.9 1.4–2.8 angiographic
!0.01 characteristics
MVD without CTO 1.6 1.2–2.2 0.01 1.1 0.8–1.6 0.51
LAD-related MI 1.4 1.1–1.7 0.01 1.7 1.3–2.2 shown
!0.01 in Table 1 and comp
Hypertension
Hypercholesterolemia
MVD without 0.7
0.6
CTO0.5–0.9 group, and
0.5–0.9
!0.01
!0.01
38% in 1.1 the MVD0.8–1/5
0.8
with
0.6–1.1
total
0.52
0.12
cohort. This indicates
Smoking
concurrent 0.5 CTO group. 0.4–0.7 !0.01 0.8 0.6–1.0 sentative
0.07 sample of the tota
Post-PCI TIMI flow grade 3 0.4 0.3–0.5 0.6 0.5–0.9
Of the 1,745 patients, a
!0.01 !0.01
Age #60 yrs During the 1.3 first 300.9–1.7 days after STEMI, 0.13 the
3.3 mortality 2.4–4.5rate !0.01
was significantly higher in patients with a concurrent CTO an LVEF !40%. Figure 2 s
Covariates were allowed in the forward stepwise Cox regression model if they influenced the model with a likelihood ratio significance level of p ! 0.05 and removed if its significance level exceeded p " 0.1.
Claessen BE et al. JACC Cardiovasc Intervcompared 2009
Covariates that were included in the analysis but were removed: male sex, diabetes mellitus, and previous MI. The variable “Age #60 yrs” was forced into the model for the first 30 days. The variables “MVD
in a non-IRA, with patients with SVD (unad-
without CTO,” “Hypertension,” “Hypercholesterolemia,” and “Smoking” were forced into the model for the 5 yrs thereafter.
CI " confidence interval; HR " hazard ratio; other abbreviations as in Table 1.
with an LVEF !40% in eaSTEMI im Kollateralen abgebenden Gefäss
T. Fujii et al. / International Journal of Cardiology 218 (2016) 158–163
STEMI in collateral
donor artery
any CTO
of Fujii
-dayMVD T etCTO
mortality
and al. Int30-day
for on
SVD, JMVD
Cardiol 2016
without
mortalityCTO, IRA, and
in STEMI afternon-IRA
primarygroups. The
PCI. The IRA group
impact hadand
of MVD significantly
comorbid greater mortality
CTO lesion thanall-cause
on 30-day did the other groups
mortality (IRA:
was dem5
15.9%,
VD non-IRA:
without 10.9%
CTO (n P b 0.0001).
= 208), and MVD A significant
with CTO (n difference was without
= 69). MVD not shownCTObetween the 30-day
had an impaired mortality
mortality of non-IRA
compared and
with MVD
that without
of SVD; CTO (Ppatien
moreover, = 0.3Prognostic Risk Factors for Mortality in Ventricular
Tachyarrhythmias
1,461 pts with arrhythmias, 20% had CTO
Mortality (mean 18 months) of 46% with CTO vs. 27% without CTO
Behnes et al. EuroIntervention 2019
Behnes et al, Eurointervention 2019Lebensqualität nach erfolgreicher CTO-PCI
Grantham et al Health Stat
Gesundheitszustand nach 1 Monat
SAQ scores
Angina pectoris differed by
analysis. Fin
all patients
Eingeschränkte
Leistungsfähigkeit signed score
possible out
ful PCI on S
Lebensqualität QoL (P# 0.0
and 16, resp
that even un
PCI of a CT
Table 3
Figure 1. Adjusted health status outcomes comparison between subgroups. F
FACTOR successful
Trial and unsuccessful PCI of CTO. Variables used in the of them wer
model included age, sex, prior MI, hypertension, hyperlipidemia, fully recanalUrsachen für Misserfolg
7%
9%
Wire does not cross
11% Balloon does not cross
Inability to dilate
Perforation
73%Prädiktoren für prozeduralen Erfolg
PROGRESS CTOThe Hybrid Algorithm
Wieso Retrograd? • proximale Verschlusskappe - dem arteriellen Druck ausgesetzt → härter, flach • distale Verschlusskappe - dem kollateralen Druck ausgesetzt → weicher, Kanal
CTO body ambiguity CTO of entire RCA
Interventional collaterals
Marker Wire antegrade wire in distal vessel after 1.5 mm Balloon
Wire correction
RAO RAO
before correction after correctionWerkzeug
Core 0.014 CTO guidewire
Coil
Coating
General Use
Finecross Antegrade
SuperCross Turnpike Spiral
Nhancer Pro Mamba
Micro-14
Retrograde Retro &
Fine collaterals Antegrade Ca+ Antegrade
Caravel Corsair Pro Tornus
Turnpike LP Turnpike Turnpike Gold
Mamba Flex TeleportSafety equipment
coils
pericardial drain
Echo
stent graftsMajor Research Areas • Prognosis / Outcomes • CTO Pathophysiology • CTO Techniques and Outcomes • DES/BRS for CTO PCI • New Devices, Case Reports • Complications and Management
SWISS CTO Summit
NOVEMBER 8th & 9th, 2019 | ST.GALLEN, SWITZERLAND
Interactive learning and sharing experience
in chronic total occlusions
T H E DATE ]
[ SAVE 9 th , 201
B E R 8th & 9 ND
NOVEM , SWIT
ZERL A
L L EN
ST. GA
Live cases
International and national faculty
Interactive educational course
Fellow and hands-on workshops
Nurse and cardiovascular technician session
Kantonsspital
St.Gallen
Swiss CTO Community Swiss Working Group
Interventional Cardiology
ORGANIZATION: Margot de Laleu - margot@incathlab-events.com - Tel. +33 (0)6 46 03 22 80Danke
kardiologie@mac.com
swisscto.chYou can also read