Chronic idiopathic constipation in adults: epidemiology, pathophysiology, diagnosis and clinical management
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Narrative review
Chronic idiopathic constipation in adults:
epidemiology, pathophysiology, diagnosis
and clinical management
Christopher J Black, Alexander C Ford
C
hronic idiopathic constipation (CIC) is one of the most Summary
common gastrointestinal disorders worldwide.1 CIC can
Chronic idiopathic constipation (CIC) is one of the most common
be divided into three subtypes: dyssynergic defaecation gastrointestinal disorders, with a global prevalence of 14%. It is
(DD), which is a problem with rectal evacuation; slow transit commoner in women and its prevalence increases with age.
constipation; and normal transit constipation, which is the most There are three subtypes of CIC: dyssynergic defaecation, slow
common subtype.2 This Narrative Review examines the epide- transit constipation and normal transit constipation, which is
miology, pathophysiology and clinical management of CIC in the most common subtype.
adults. It is based on a synthesis of relevant evidence from articles Clinical assessment of the patient with constipation requires
listed in PubMed from inception until January 2018, including careful history taking, in order to identify any red flag
original research articles, consensus guidelines and opinion symptoms that would necessitate further investigation with
articles. colonoscopy to exclude colorectal malignancy.
Screening for hypercalcaemia, hypothyroidism and coeliac
disease with appropriate blood tests should be considered.
Definition
A digital rectal examination should be performed to assess for
evidence of dyssynergic defaecation. If this is suspected,
Patients with CIC usually present with symptoms including hard
further investigation with high resolution anorectal
or lumpy stools, reduced frequency of defaecation, a sensation of
manometry should be undertaken.
incomplete evacuation or blockage, straining at stool, and some
Anorectal biofeedback can be offered to patients with dyssynergic
may also report abdominal pain and bloating.3 In general, symp- defaecation as a means of correcting the associated impairment
toms are deemed to be chronic if they have been present for at least of pelvic floor, abdominal wall and rectal functioning.
3 months. Lifestyle modifications, such as increasing dietary fibre, are the
first step in managing other causes of CIC. If patients do not
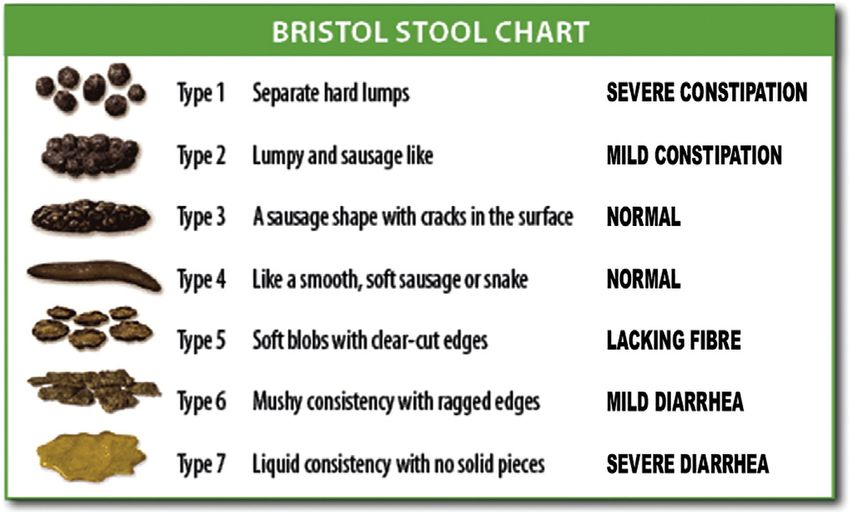
The Bristol Stool Form Scale (BSFS) (Box 1) is a validated tool that respond to these simple changes, then treatment with
describes the different consistencies of stool a patient may experi- osmotic and stimulant laxatives should be trialled.
ence.4 Stool types 1 and 2 are indicative of hard stools, and types 6 Patients not responding to traditional laxatives should be
and 7 are loose or watery stools. The stool consistency has been offered treatment with prosecretory agents such as
shown to correlate well with colonic transit time,5,6 whereas the lubiprostone, linaclotide and plecanatide, or the 5-HT4 re-
overall frequency of defaecation may not,6,7 although the majority ceptor agonist prucalopride, where available.
of patients presenting with CIC have normal colonic transit.8 This If there is no response to pharmacological treatment, surgical
is also referred to as functional constipation and is defined by the intervention can be considered, but it is only suitable for a
Rome IV diagnostic criteria (Box 2). In practice, these criteria can be carefully selected subset of patients with proven slow transit
difficult to apply and, because abdominal pain is so often reported constipation.
in functional constipation, it can be difficult to distinguish func-
tional constipation from irritable bowel syndrome with con-
stipation (IBS-C).9,10
Normal colonic physiology
Epidemiology To understand the investigation and treatment of CIC, it is helpful to
briefly consider the normal physiological functioning of the colon.
A previous meta-analysis across 45 population-based studies
showed a pooled global prevalence of CIC of 14%, with little Motility
variation by geographical region, although data from the Middle
Although peristalsis is observed in the colon, the main mechanism
East, Central America and Africa were scant.11 It has traditionally
of propulsive motility is via mass movements, which occur a few
been held that the prevalence of CIC increases with age, with
times each day, ultimately leading to defaecation.15 They arise
higher rates reported in older people,12 a trend that was confirmed,
16 July 2018
from the inhibition of distal haustral segments and contractions of
albeit modestly, by this meta-analysis.11 Regarding gender, most
the proximal bowel wall. The primary motor pattern associated
chronic gastrointestinal disorders, including IBS, are more com-
with these mass movements is called a high amplitude propa-
mon in women,13 and the same is true of CIC. The meta-analysis
gating contraction,16 which arises from the contraction of colonic
indicated that the prevalence of CIC among women was almost
j
smooth muscle, although the underlying neurophysiological
MJA 209 (2)
twice that in men.11 Finally, low socio-economic status has been
mechanism remains incompletely understood.
identified as a risk factor for CIC.14 There was a modest increase in
the prevalence of CIC among patients of lower compared with Peristalsis, on the other hand, is predominantly mediated by se-
higher socio-economic status, but not when comparing medium rotonin, or 5-hydroxytryptamine (5-HT), which is synthesised and
with higher socio-economic status.11 released by enterochromaffin cells.17 Serotonin activates receptors,
86
Leeds Institute of Biomedical and Clinical Sciences, University of Leeds, Leeds, UK. A.C.Ford@leeds.ac.uk j doi: 10.5694/mja18.00241Narrative review
methane production25 and affect epithelial function, all of which can
1 The Bristol Stool Form Scale*
alter colonic motility and fluid secretion, resulting in constipation.26
As with other functional gastrointestinal disorders, there are also
dietary and other lifestyle, behavioural and psychological factors
that may be involved in the aetiology of symptoms.27-29
Rectal evacuation disorders
These constitute the second most common cause of CIC. Emptying
the rectum requires coordination of the rectal and abdominal
wall muscles, the anal sphincters and the pelvic floor muscles.
DD, which is the most common disorder of rectal evacuation,
arises when this coordination is impaired in some way, leading to
paradoxical anal contraction, failure or impairment of anal relax-
ation, or inadequate rectal and abdominal propulsive force.30
Slower colonic transit is often present concurrently.31
* Source: Cabot Health, Bristol stool chart. http://cdn.intechopen.com/pdfs-wm/46 DD is an acquired and learned behavioural problem, often result-
082.pdf. u ing from dysfunctional toilet habits. In one study, sexual abuse was
reported in 22% of cases, and physical abuse in 32%,32 and there
which send signals via the myenteric nerve plexus, propagating a was a significant impact on health-related quality of life. Problems
wave of intestinal smooth muscle contraction and propelling with rectal evacuation can coexist with a structural cause, such as a
luminal contents. The interstitial cells of Cajal act as a pacemaker, rectocele, rectal prolapse or rectal intussusception.33
mediating between the signals of the enteric nervous system and
intestinal smooth muscle.18 Slow transit constipation
Colonic contents can also move in a retrograde direction, which is Among patients with slow transit constipation, which is the least
more marked after a meal and potentially provides a “brake” to prevalent subtype of CIC, there may be a limited, or absent, increase
prevent rapid rectal filling.19 At the same time, there is also a in postprandial motor activity,34 and normal retrograde colonic
general postprandial increase in colonic motor activity — the so- propulsion may also be impaired.35 These patients may exhibit
called gastrocolic reflex. delayed emptying of the proximal colon,36,37 and either a reduction
or complete absence of high amplitude propagating contrac-
Fluid and electrolytes tions.35,37,38 Mediation of peristalsis via 5-HT can also be impaired.16
The colon has an important role in managing intestinal fluid and Moreover, individuals with severe slow transit constipation can
electrolyte content, and reabsorbs about 1e2 L of fluid per day.20 exhibit abnormal or reduced numbers of interstitial cells of Cajal.39,40
Prosecretory drugs can increase intestinal luminal fluid and electro-
lyte content sufficiently to saturate this process, thereby altering stool Clinical assessment and investigation
consistency and reducing colonic transit time.21 Alternatively, os-
motic laxatives increase luminal water content by creating an osmotic A thorough history is the most important element in the clinical
gradient across the intestinal epithelium, with similar effects.22 assessment of the patient with constipation. The physician must be
vigilant for the presence of red flag symptoms, such as weight loss
Pathophysiology or rectal bleeding, which should prompt urgent investigation with
colonoscopy or cross-sectional imaging as appropriate, primarily
Normal transit (functional) constipation to exclude colorectal or other intra-abdominal malignancy (Box 3).
Otherwise, colonoscopy is not a useful investigation for con-
Despite normal transit constipation being the most prevalent sub-
stipation in general. Any association between chronic constipation
group of CIC, the pathophysiology remains unclear.23 Changes in
and the development of colorectal cancer is controversial; a 2013
the colonic microbiota can increase bile acid metabolism,24 promote
meta-analysis argues against such a link.41
2 The Rome IV diagnostic criteria for normal transit Enquiring about the patient’s medical history is important.
(functional) constipation Constipation can arise secondary to neurological conditions, such
as Parkinson disease and multiple sclerosis; endocrine disorders,
Diagnosis of normal transit constipation requires the presence of the
following criteria for the past 3 months, with symptom onset more such as hypothyroidism and hypercalcaemia; and prescribed
than 6 months prior to diagnosis medications, such as opiates or tricyclic antidepressants. Blood
MJA 209 (2)
Presence of two or more of the following criteria: tests for thyroid function and calcium should be considered, as
B straining during > 25% of defaecations; well as testing for coeliac disease. Although more commonly
B Bristol stool form types 1 and 2 for > 25% of defaecations; associated with symptoms of diarrhoea, weight loss and
B sensation of incomplete evacuation for > 25% of defaecations; abdominal pain, coeliac disease was associated with constipation
in 10% of patients in a large cohort study.42
j
B sensation of anorectal obstruction or blockage for > 25% of
16 July 2018
defaecations;
B manual manoeuvres to facilitate > 25% of defaecations An obstetric and gynaecological history is also important when
(eg; digital manipulation); and assessing symptoms of constipation in women.43 One study noted
B less than three spontaneous bowel movements per week
that the odds of obstructive defaecation increased twofold in
Without the use of laxatives, loose stools are rarely present women who had undergone vaginal or laparoscopic hysterec-
Insufficient criteria for irritable bowel syndrome tomy,44 and vaginal delivery and higher parity have both been
Adapted from Mearin et al3 u shown to increase the risk of defaecatory symptoms arising from 87
pelvic floor dysfunction.45Narrative review
capsule containing 20 radio-opaque markers is swal-
3 Recommended management algorithm for patients with chronic
lowed by the patient and a plain abdominal x-ray is
idiopathic constipation
taken 5 days later. Retention of five or more markers is
indicative of slow transit, but care must be taken not to
overinterpret the result, with a recent study showing
that the number of retained markers does not correlate
with symptom severity or quality of life in CIC.51
Colonic transit can also be measured using other mo-
dalities, including colonic scintigraphy,52 where patients
are given a radioisotope-labelled meal and timed mea-
surements of residual radioactivity are made to calcu-
late transit, and wireless motility capsule,53 which uses
changes in pH along the gastrointestinal tract to deter-
mine transit time. In practice, these investigations are
used in a limited number of specialist centres, and are
not routine in investigating patients with constipation.
Management
Lifestyle
Modification of lifestyle factors, including diet, hydra-
tion and exercise, is usually the first step in managing
CIC (Box 3).
Diet. Patients with CIC are often told to increase their
dietary fibre intake, with guidelines suggesting 25e30 g
of fibre per day. This should be introduced slowly, with
gradual titration to avoid side effects. Insoluble fibres,
such as wheat bran, may accelerate gastrointestinal
transit, thereby increasing stool frequency.54 However,
negative effects have been reported, particularly in pa-
tients with IBS-C, for whom insoluble fibre may worsen
symptoms, including abdominal pain and bloating.
Soluble fibre such as psyllium, derived from ground
ispaghula husk, when ingested with water increases
stool bulk and frequency.55 Sterculia may be an alterna-
tive in those who experience side effects with psyllium.
A systematic review by Suares and Ford,56 which
* Only for proven slow transit constipation, and if all other therapies have failed. u
included six randomised controlled trials (RCTs) of sol-
uble and insoluble fibre, found evidence of limited
benefit overall in CIC, but suggested that soluble fibre
Digital rectal examination has been shown to be reliable for iden- was more effective than placebo, and led to improvements in indi-
tifying DD in patients who have chronic constipation,46 with a vidual symptoms. A further systematic review with meta-analysis
sensitivity and specificity of 75% and 87% respectively.47 The by Christodoulides and colleagues57 also suggested that soluble
presence of two of the following features is required: impaired fibre was effective for treating CIC, but highlighted that it may also
perianal descent, paradoxical anal contraction or impaired push cause unwanted gastrointestinal side effects, such as increased
effort.48 If DD is suspected, based on digital rectal examination, flatulence. Overall, the quality of evidence was low and the findings
physiological testing with high resolution anorectal manometry should be interpreted cautiously, due to a high risk of bias among all
may be useful to confirm the diagnosis. included studies. Both these systematic reviews identified a need for
further large studies of fibre for the treatment of CIC.
High resolution manometry enables measurement of both anal
16 July 2018
resting and squeeze pressures and the rectal pressure during Probiotics. Whether probiotics have a role in CIC is unclear. There
simulated defaecation, and can therefore help in identifying DD.49 is some suggestion they might improve gut transit time, stool fre-
However, many manometry patterns that were once considered quency and stool consistency.58 However, more rigorous RCTs are
abnormal have been observed in healthy asymptomatic in- needed to overcome the potential biases that blight the currently
j
dividuals, which may limit utility.49 It is important to correlate the available studies.59
MJA 209 (2)
result with patient symptoms, and careful clinical judgement must
Hydration. There is no evidence that CIC can be successfully
be exercised. Defaecation proctography, traditionally using fluo-
treated by increasing fluid intake, unless there is evidence of dehy-
roscopy and, more recently, magnetic resonance imaging, can
dration.60 In the only study to date of increased fluid intake alone,
elucidate obstructive causes of defaecation, such as rectal intus-
117 adult patients, for whom constipation was defined as fewer than
susception or rectocele.33
three bowel movements per week, were randomly allocated to
88 The standard means of assessing colonic transit is the radio-opaque either unrestricted fluid intake or 2 L of mineral water daily, over a
marker test,50 which is relatively simple and widely available. A 2-month period.61 Stool frequency increased by 1.3 stools per weekNarrative review
in the control group and 2.4 stools per week in the intervention also significantly more likely to reach the primary endpoint of three
group. However, the results are unreliable, as baseline data were or more spontaneous bowel movements per week. Diarrhoea was
assessed by patient recall and the mineral water contained the most frequent side effect experienced by those taking linaclotide,
magnesium, which could have exerted a laxative effect. Another resulting in discontinuation of the drug in 4% of patients.
study examined the effects of adding extra water to ingested wheat
In RCTs of plecanatide for treating CIC,76,77 the drug improved
bran, but found no beneficial effect on stool frequency or form.62
constipation-related symptoms, when compared with placebo,
Exercise. A study in patients with IBS found that increased over 12 weeks, but diarrhoea was again the predominant side ef-
physical activity improved gastrointestinal symptoms and was fect. Patients taking plecanatide had significantly more sponta-
also protective against a deterioration in symptoms,63 effects which neous bowel movements per week, as well as significant
might be mediated through positive effects on anti-inflammatory improvements in stool consistency.
and anti-oxidant pathways, as well as immune function.64 In CIC
5-HT4 receptor agonists. Prucalopride is a selective 5-HT4 re-
specifically, although intervention programs to increase physical
ceptor agonist which stimulates gastrointestinal and colonic
activity may be of some help in older patients,62 there is no evi-
motility. An integrated analysis of six phase 3 and 4 RCTs showed
dence to suggest that increasing levels of physical activity in
that significantly more patients with CIC achieved a mean of three
younger people is beneficial.23
or more spontaneous bowel movements per week with treatment
with prucalopride 2 mg once daily for 12 weeks compared with
Pharmacological treatments placebo.78 Overall, the drug was well tolerated; common side ef-
fects included diarrhoea and headache. The dose should be
Medications for treating constipation principally include osmotic
reduced to 1 mg once daily in older patients or those with renal or
or stimulant laxatives, prosecretory drugs and 5-HT4 receptor
hepatic impairment.
agonists.
Emerging drug treatments. Drug development continues with
Osmotic laxatives. If patients fail to respond to lifestyle measures,
new treatments for CIC on the horizon. Like prucalopride, velu-
osmotic laxatives such as polyethylene glycol and lactulose are the
setrag and naronapride are both selective 5-HT4 receptor agonists
first-line drug treatment. A meta-analysis that included six RCTs
with prokinetic effects.79,80 These drugs have shown some promise
comparing osmotic laxatives with placebo for treating CIC found
in phase 2 clinical trials, but are yet to be evaluated any further.
that, overall, osmotic laxatives were more effective, with a number
needed to treat of three.65 In individual RCTs, polyethylene glycol Elobixibat, which is currently being evaluated in two large phase 3
appeared to be superior to both lactulose66 and prucalopride, a 5- RCTs, is an inhibitor of the ileal bile acid transporter, which
HT4 receptor agonist,67 when compared directly. Lactulose may effectively induces a state of bile acid malabsorption, resulting in
also be poorly tolerated, as it frequently causes bloating. increased colonic motility and fluid secretion.81 It may be a valu-
able new pharmacological therapy for CIC.
Stimulant laxatives. Stimulant laxatives may be used if there is no
response to osmotic laxatives. Bisacodyl and sodium picosulfate are
Other treatments
both well tolerated and improve bowel function, symptoms and
quality of life in RCTs.68,69 Interestingly, a systematic review and
network meta-analysis found bisacodyl to be superior not only to Anorectal biofeedback
sodium picosulfate but also to prosecretory drugs and 5-HT4 receptor Anorectal biofeedback, which is a behavioural training technique,
agonists.70 Senna, an anthraquinone laxative, is frequently prescribed can be used in the treatment of DD. It comprises measurement of
in CIC, but to date there are no placebo-controlled trials assessing its anorectal physiology, with the abnormal responses shown to the
efficacy. Bisacodyl can also be given as an enema. Although other patient in real time and targeted training to correct them, thus
stimulants given per rectum, such as glycerol suppositories or improving anorectal function. It employs a combination of tech-
phosphate or sodium citrate enemas, may provide individual pa- niques, which can include training to improve abdominal straining
tients with more predictability and control over their bowel habits, and push effort, training to relax the pelvic floor during defaeca-
there are no RCTs to support their efficacy.71 There is no evidence to tion, the simulation of defaecation by expulsion of a balloon from
suggest that patients become dependent on stimulant laxatives.72 the rectum, and sensory retraining when rectal sensation is
Prosecretory agents. If a patient fails to respond to conventional impaired.82 It has been shown to be effective in RCTs when
laxatives, prosecretory drugs may be tried. Lubiprostone, linaclo- compared with both standard treatment for CIC and sham thera-
tide, and plecanatide all work by increasing fluid and electrolyte pies.83 However, a Cochrane review84 reported that the quality of
flux into the intestinal lumen, although, at the time of writing, none evidence for use of biofeedback was poor overall and recom-
of these drugs were available in Australia. Lubiprostone achieves mended that larger RCTs were conducted.
this by activating chloride 2 channels on the luminal epithelial cells,
MJA 209 (2)
whereas linaclotide and plecanatide activate the cystic fibrosis Transanal irrigation
transmembrane conductance regulator (CFTR) chloride channel by
Transanal irrigation is a commonly used treatment for disordered
increasing luminal cyclic guanosine monophosphate. A meta-
defaecation. In adults, this is predominantly in the context of
analysis by Li and colleagues,73 summarising data from nine
neurogenic bowel, for which it is reimbursable in Australia, rather
j
RCTs of lubiprostone versus placebo in CIC and IBS-C, found
16 July 2018
than CIC.85 It is a generally safe intervention and can be considered
significant improvements in severity of constipation, stool consis-
for treating CIC in adults when pharmacological treatments have
tency and degree of straining after one month, but there was no
proved to be ineffective and, particularly, before irreversible sur-
longer a significant difference between groups by 3 months.73 Side
gical procedures are considered.86 However, a recent study
effects, particularly nausea, are commoner with lubiprostone.74
revealed that although it can lead to significant improvements in
Treatment of CIC with 12 weeks of linaclotide was found to signif- bowel function and quality of life among patients with CIC at
icantly reduce bowel and abdominal symptoms when compared 12 months, more than one-third of patients discontinue it within 89
with placebo in two RCTs.75 Patients treated with linaclotide were the first year, largely due to an unsatisfactory effect.87Narrative review
Surgery simple dietary manipulation and the use of conventional laxa-
Surgical procedures include total colectomy with either ileorectal tives. Further research in CIC should focus on understanding
anastomosis or ileostomy formation. However, they are rarely the neuropathophysiology responsible for normal transit con-
indicated, and strict patient selection criteria are vital. Surgery is stipation, including additional exploration of the role of both
only suitable for patients with proven slow transit, for whom other the microbiome and probiotics in CIC. Larger RCTs investi-
correctible causes of constipation have been excluded, and who gating biofeedback for treating DD are needed, in conjunction
have failed to respond to all available pharmacological treat- with improving access to biofeedback for patients, as well as
ments.23 This patient group may benefit from total colectomy with larger trials of dietary fibre. We need to better understand
ileorectal anastomosis.88 Outcomes can be very good when strict which investigations assess colonic physiology most accurately
selection criteria are applied, with high levels of patient satisfaction in clinical practice, how to make them more acceptable to
and improvements in quality of life reported.89 Surgery is not patients, as well as more representative of real life; for example,
suitable for patients with IBS-C, or for those with pure DD. When assessing defaecatory function with the patient sitting instead of
slow transit constipation and DD coexist, DD should be corrected lying down, as is currently the case. Finally, head-to-head
before surgery. If this is not achievable, then formation of an comparisons of the efficacy of existing prosecretory drugs for
ileostomy is the only suitable surgical intervention.23 treating CIC are required, and the results of further trials of
drugs in development are also awaited.
Conclusion Competing interests: No relevant disclosures.
Provenance: Commissioned; externally peer reviewed.-
CIC is a very common disorder. In the past 15 years, patients
have benefitted from an expansion in treatment options, beyond ª 2018 AMPCo Pty Ltd. Produced with Elsevier B.V. All rights reserved.
1 Peery AF, Crockett SD, Barritt AS, et al. Burden of symptoms: a population based study in 15 000 symptoms, colonic transit, and methane production in
gastrointestinal, liver, and pancreatic diseases in the Australian adults. Gut 2001; 49: 66-72. female patients with chronic constipation.
United States. Gastroenterology 2015; 149: 1731-1741.e3. Gastroenterology 2016; 150: 367-379.e1.
15 Holdstock DJ, Misiewicz JJ, Smith T, Rowlands EN.
2 Shahid S, Ramzan Z, Maurer AH, et al. Chronic idiopathic Propulsion (mass movements) in the human colon and 27 Markland AD, Palsson O, Goode PS, et al. Association of
constipation: more than a simple colonic transit disorder. its relationship to meals and somatic activity. Gut 1970; low dietary intake of fiber and liquids with constipation:
J Clin Gastroenterol 2012; 46: 150-154. 11: 91-99. evidence from the National Health and Nutrition
3 Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Examination Survey. Am J Gastroenterol 2013; 108:
16 Smith TK, Park KJ, Hennig GW. Colonic migrating motor
Gastroenterology 2016; 150: 1393-1407. complexes, high amplitude propagating contractions, 796-803.
4 Lewis SJ, Heaton KW. Stool form scale as a useful guide neural reflexes and the importance of neuronal and 28 Mazlyn MM, Nagarajah LH, Fatimah A, et al. Stool
to intestinal transit time. Scand J Gastroenterol 1997; 32: mucosal serotonin. J Neurogastroenterol Motil 2014; 20: patterns of Malaysian adults with functional
920-924. 423-446. constipation: association with diet and physical activity.
Malays J Nutr 2013; 19: 53-64.
5 Degen LP, Phillips SF. How well does stool form reflect 17 Spencer NJ. Constitutively active 5-HT receptors: an
colonic transit? Gut 1996; 39: 109-113. explanation of how 5-HT antagonists inhibit gut motility 29 Chan AO, Cheng C, Hui WM, et al. Differing coping
6 Saad RJ, Rao SS, Koch KL, et al. Do stool form and in species where 5-HT is not an enteric mechanisms, stress level and anorectal physiology in
frequency correlate with whole-gut and colonic transit? neurotransmitter? Front Cell Neurosci 2015; 9: 487. patients with functional constipation. World J
Results from a multicenter study in constipated Gastroenterol 2005; 11: 5362-5366.
18 Radenkovic G, Radenkovic D, Velickov A. Development of
individuals and healthy controls. Am J Gastroenterol interstitial cells of Cajal in the human digestive 30 Rao SS, Welcher KD, Leistikow JS. Obstructive
2010; 105: 403-411. tract as the result of reciprocal induction of defecation: a failure of rectoanal coordination. Am J
7 Chaussade S, Khyari A, Roche H, et al. Determination of mesenchymal and neural crest cells. J Cell Mol Med 2018; Gastroenterol 1998; 93: 1042-1050.
total and segmental colonic transit time in constipated 22: 778-785. 31 Nullens S, Nelsen T, Camilleri M, et al. Regional colon transit
patients. Results in 91 patients with a new simplified 19 Lin AY, Du P, Dinning PG, et al. High-resolution anatomic in patients with dys-synergic defaecation or slow transit
method. Dig Dis Sci 1989; 34: 1168-1172. correlation of cyclic motor patterns in the human colon: in patients with constipation. Gut 2012; 61: 1132-1139.
8 Tornblom H, Van Oudenhove L, Sadik R, et al. Colonic evidence of a rectosigmoid brake. Am J Physiol 32 Rao SS, Tuteja AK, Vellema T, et al. Dyssynergic
transit time and IBS symptoms: what’s the link? Am J Gastrointest Liver Physiol 2017; 312: G508-G515. defecation: demographics, symptoms, stool patterns,
Gastroenterol 2012; 107: 754-760. and quality of life. J Clin Gastroenterol 2004; 38:
20 Sandle GI. Salt and water absorption in the human
9 Whitehead WE, Palsson OS, Simren M. Biomarkers to colon: a modern appraisal. Gut 1998; 43: 294-299. 680-685.
distinguish functional constipation from irritable bowel 33 Perniola G, Shek C, Chong CC, et al. Defecation
syndrome with constipation. Neurogastroenterol Motil 21 Thomas RH, Luthin DR. Current and emerging treatments
for irritable bowel syndrome with constipation and proctography and translabial ultrasound in the
2016; 28: 783-792. investigation of defecatory disorders. Ultrasound Obstet
chronic idiopathic constipation: focus on prosecretory
10 Wong RK, Palsson OS, Turner MJ, et al. Inability of the agents. Pharmacotherapy 2015; 35: 613-630. Gynecol 2008; 31: 567-571.
Rome III criteria to distinguish functional constipation 34 Bassotti G, Iantorno G, Fiorella S, et al. Colonic motility
from constipation-subtype irritable bowel syndrome. Am 22 Krogh K, Chiarioni G, Whitehead W. Management of
in man: features in normal subjects and in patients with
16 July 2018
J Gastroenterol 2010; 105: 2228-2234. chronic constipation in adults. United European
chronic idiopathic constipation. Am J Gastroenterol 1999;
Gastroenterol J 2017; 5: 465-472.
11 Suares NC, Ford AC. Prevalence of, and risk factors for, 94: 1760-1770.
chronic idiopathic constipation in the community: 23 Camilleri M, Ford AC, Mawe GM, et al. Chronic
35 Dinning PG, Wiklendt L, Maslen L, et al. Colonic motor
Systematic review and meta-analysis. Am J constipation. Nat Rev Dis Primers 2017; 3: 17095.
abnormalities in slow transit constipation defined by
Gastroenterol 2011; 106: 1582-1591; quiz 1, 92. 24 Abrahamsson H, Ostlund-Lindqvist AM, Nilsson R, et al.
j
high resolution, fibre-optic manometry.
MJA 209 (2)
12 Vazquez Roque M, Bouras EP. Epidemiology and Altered bile acid metabolism in patients with Neurogastroenterol Motil 2015; 27: 379-388.
management of chronic constipation in elderly patients. constipation-predominant irritable bowel syndrome and
36 Bassotti G, Gaburri M, Imbimbo BP, et al. Colonic mass
Clin Interv Aging 2015; 10: 919-930. functional constipation. Scand J Gastroenterol 2008; 43:
movements in idiopathic chronic constipation. Gut 1988;
1483-1488.
13 Ford AC, Bercik P, Morgan DG, et al. Characteristics of 29: 1173-1179.
functional bowel disorder patients: a cross-sectional 25 Triantafyllou K, Chang C, Pimentel M. Methanogens,
37 Dinning PG, Zarate N, Hunt LM, et al. Pancolonic
survey using the Rome III criteria. Aliment Pharmacol methane and gastrointestinal motility.
spatiotemporal mapping reveals regional deficiencies in,
Ther 2014; 39: 312-321. J Neurogastroenterol Motil 2014; 20: 31-40. and disorganization of colonic propagating pressure
90 14 Bytzer P, Howell S, Leemon M, et al. Low socioeconomic 26 Parthasarathy G, Chen J, Chen X, et al. Relationship waves in severe constipation. Neurogastroenterol Motil
class is a risk factor for upper and lower gastrointestinal between microbiota of the colonic mucosa vs feces and 2010; 22: e340-e349.Narrative review
38 Bassotti G, Chiarioni G, Vantini I, et al. Anorectal constipation. Aliment Pharmacol Ther 2011; 33: 73 Li F, Fu T, Tong WD, et al. Lubiprostone is effective in the
manometric abnormalities and colonic propulsive 895-901. treatment of chronic idiopathic constipation and
impairment in patients with severe chronic idiopathic irritable bowel syndrome: a systematic review and meta-
57 Christodoulides S, Dimidi E, Fragkos KC, et al.
constipation. Dig Dis Sci 1994; 39: 1558-1564. analysis of randomized controlled trials. Mayo Clin Proc
Systematic review with meta-analysis: effect of
39 Lyford GL, He CL, Soffer E, et al. Pan-colonic decrease in 2016; 91: 456-468.
fibre supplementation on chronic idiopathic
interstitial cells of Cajal in patients with slow transit constipation in adults. Aliment Pharmacol Ther 74 Cryer B, Drossman DA, Chey WD, et al. Analysis of
constipation. Gut 2002; 51: 496-501. 2016; 44: 103-116. nausea in clinical studies of lubiprostone for the
40 Tong WD, Liu BH, Zhang LY, et al. Decreased interstitial treatment of constipation disorders. Dig Dis Sci 2017; 62:
58 Dimidi E, Christodoulides S, Fragkos KC, et al.
cells of Cajal in the sigmoid colon of patients with slow 3568-3578.
The effect of probiotics on functional constipation in
transit constipation. Int J Colorectal Dis 2004; 19: adults: a systematic review and meta-analysis of 75 Lembo AJ, Schneier HA, Shiff SJ, et al. Two randomized
467-473. randomized controlled trials. Am J Clin Nutr 2014; 100: trials of linaclotide for chronic constipation. N Engl J Med
41 Power AM, Talley NJ, Ford AC. Association between 1075-1084. 2011; 365: 527-536.
constipation and colorectal cancer: Systematic review 59 Ford AC, Quigley EM, Lacy BE, et al. Efficacy of 76 DeMicco M, Barrow L, Hickey B, et al. Randomized
and meta-analysis of observational studies. Am J prebiotics, probiotics, and synbiotics in irritable clinical trial: efficacy and safety of plecanatide in the
Gastroenterol 2013; 108: 894-903; quiz 4. bowel syndrome and chronic idiopathic treatment of chronic idiopathic constipation. Therap Adv
42 Spijkerman M, Tan IL, Kolkman JJ, et al. A large variety constipation: systematic review and meta-analysis. Gastroenterol 2017; 10: 837-851.
of clinical features and concomitant disorders in celiac Am J Gastroenterol 2014; 109: 1547-1561; quiz 6, 62. 77 Miner PB Jr, Koltun WD, Wiener GJ, et al. A randomized
disease - A cohort study in the Netherlands. Dig Liver Dis 60 Müller-Lissner SA, Kamm MA, Scarpignato C, Wald A. phase III clinical trial of plecanatide, a uroguanylin
2016; 48: 499-505. Myths and misconceptions about chronic constipation. analog, in patients with chronic idiopathic constipation.
43 Park SK, Myung SJ, Jung KW, et al. Biofeedback therapy Am J Gastroenterol 2005; 100: 232. Am J Gastroenterol 2017; 112: 613-621.
for female patients with constipation caused by radical 61 Anti M, Pignataro G, Armuzzi A, et al. Water 78 Camilleri M, Piessevaux H, Yiannakou Y, et al.
hysterectomy or vaginal delivery. J Gastroenterol Hepatol supplementation enhances the effect of high-fiber diet Efficacy and safety of prucalopride in chronic
2013; 28: 1133-1140. on stool frequency and laxative consumption in adult constipation: an integrated analysis of six
44 Varma MG, Hart SL, Brown JS, et al. Obstructive patients with functional constipation. randomized, controlled clinical trials. Dig Dis Sci 2016;
defecation in middle-aged women. Dig Dis Sci 2008; 53: Hepatogastroenterology 1998; 45: 727-732. 61: 2357-2372.
2702-2709. 62 Ziegenhagen DJ, Tewinkel G, Kruis W, Herrmann F. 79 Goldberg M, Li YP, Johanson JF, et al. Clinical
45 Kepenekci I, Keskinkilic B, Akinsu F, et al. Prevalence of Adding more fluid to wheat bran has no significant trial: the efficacy and tolerability of velusetrag, a
pelvic floor disorders in the female population and the effects on intestinal functions of healthy subjects. J Clin selective 5-HT4 agonist with high intrinsic activity,
impact of age, mode of delivery, and parity. Dis Colon Gastroenterol 1991; 13: 525-530. in chronic idiopathic constipation - a 4-week,
Rectum 2011; 54: 85-94. 63 Johannesson E, Simren M, Strid H, et al. Physical activity randomized, double-blind, placebo-controlled,
46 Talley NJ. How to do and interpret a rectal examination improves symptoms in irritable bowel syndrome: a dose-response study. Aliment Pharmacol Ther 2010;
in gastroenterology. Am J Gastroenterol 2008; 103: randomized controlled trial. Am J Gastroenterol 2011; 32: 1102-1112.
820-822. 106: 915-922. 80 Camilleri M, Vazquez-Roque MI, Burton D,
47 Soh JS, Lee HJ, Jung KW, et al. The diagnostic value of a 64 Hajizadeh Maleki B, Tartibian B, Mooren FC, et al. et al. Pharmacodynamic effects of a novel
digital rectal examination compared with high- Low-to-moderate intensity aerobic exercise training prokinetic 5-HT receptor agonist, ATI-7505,
resolution anorectal manometry in patients with chronic modulates irritable bowel syndrome through in humans. Neurogastroenterol Motil 2007; 19:
constipation and fecal incontinence. Am J Gastroenterol antioxidative and inflammatory mechanisms in women: 30-38.
2015; 110: 1197-1204. results of a randomized controlled trial. Cytokine 2017; 81 Acosta A, Camilleri M. Elobixibat and its potential role in
48 Tantiphlachiva K, Rao P, Attaluri A, Rao SSC. Digital 102: 18-25. chronic idiopathic constipation. Therap Adv
rectal examination is a useful tool for identifying 65 Ford AC, Suares NC. Effect of laxatives and Gastroenterol 2014; 7: 167-175.
patients with dyssynergia. Clin Gastroenterol Hepatol pharmacological therapies in chronic idiopathic 82 Bleijenberg G, Kuijpers HC. Biofeedback
2010; 8: 955-960. constipation: Systematic review and meta-analysis. treatment of constipation: a comparison
49 Basilisco G, Bharucha AE. High-resolution anorectal Gut 2011; 60: 209-218. of two methods. Am J Gastroenterol 1994; 89:
manometry: an expensive hobby or worth every 66 Lee-Robichaud H, Thomas K, Morgan J, Nelson RL. 1021-1026.
penny? Neurogastroenterol Motil 2017; 29: Lactulose versus polyethylene glycol for chronic 83 Rao SS, Seaton K, Miller M, et al. Randomized controlled
doi: 10.1111/nmo.13125. constipation. Cochrane Database Syst Rev 2010; (7): trial of biofeedback, sham feedback, and standard
50 Hinton JM, Lennard-Jones JE, Young AC. A new method CD007570. therapy for dyssynergic defecation. Clin Gastroenterol
for studying gut transit times using radioopaque 67 Cinca R, Chera D, Gruss HJ, Halphen M. Randomised Hepatol 2007; 5: 331-338.
markers. Gut 1969; 10: 842-847. clinical trial: macrogol/PEG 3350þelectrolytes versus 84 Woodward S, Norton C, Chiarelli P. Biofeedback
51 Staller K, Barshop K, Ananthakrishnan AN, Kuo B. prucalopride in the treatment of chronic constipation e for treatment of chronic idiopathic constipation in
Number of retained radiopaque markers on a colonic a comparison in a controlled environment. Aliment adults. Cochrane Database Syst Rev 2014; (3):
transit study does not correlate with symptom severity Pharmacol Ther 2013; 37: 876-886. CD008486.
or quality of life in chronic constipation. 68 Kamm MA, Mueller-Lissner S, Wald A, et al. Oral 85 Coggrave M, Norton C. Management of faecal
Neurogastroenterol Motil 2018; 30: e13269. bisacodyl is effective and well-tolerated in patients with incontinence and constipation in adults with central
52 Ziessman HA. Gastrointestinal transit assessment: role chronic constipation. Clin Gastroenterol Hepatol 2011; 9: neurological diseases. Cochrane Database Syst Rev 2013;
of scintigraphy: Where are we now? Where are we 577-583. (12): CD002115.
going? Curr Treat Options Gastroenterol 2016; 14: 69 Mueller-Lissner S, Kamm MA, Wald A, et al. 86 Christensen P, Krogh K. Transanal irrigation for
452-460. Multicenter, 4-week, double-blind, randomized, disordered defecation: a systematic review. Scand J
53 Diaz Tartera HO, Webb DL, Al-Saffar AK, et al. Validation placebo-controlled trial of sodium picosulfate in Gastroenterol 2010; 45: 517-527.
of SmartPill((R)) wireless motility capsule for patients with chronic constipation. Am J Gastroenterol 87 Juul T, Christensen P. Prospective evaluation of
MJA 209 (2)
gastrointestinal transit time: intra-subject variability, 2010; 105: 897-903. transanal irrigation for fecal incontinence and
software accuracy and comparison with video capsule 70 Nelson AD, Camilleri M, Chirapongsathorn S, et al. constipation. Tech Coloproctol 2017; 21: 363-371.
endoscopy. Neurogastroenterol Motil 2017; 29: 1-9. Comparison of efficacy of pharmacological treatments 88 Knowles CH, Grossi U, Horrocks EJ, et al. Surgery
54 Payler DK, Pomare EW, Heaton KW, Harvey RF. The for chronic idiopathic constipation: a systematic for constipation: Systematic review and practice
effect of wheat bran on intestinal transit. Gut 1975; 16: review and network meta-analysis. Gut 2017; 66: recommendations. Colorectal Dis 2017; 19:
j
16 July 2018
209-213. 1611-1622. 101-113.
55 Marteau P, Flourie B, Cherbut C, et al. Digestibility and 71 Mueller-Lissner SA, Wald A. Constipation in adults. BMJ
89 Hassan I, Pemberton JH, Young-Fadok TM, et al.
bulking effect of ispaghula husks in healthy humans. Gut Clin Evid 2010; 0413.
Ileorectal anastomosis for slow transit
1994; 35: 1747-1752. 72 Wald A. Is chronic use of stimulant laxatives constipation: Long-term functional and quality
56 Suares NC, Ford AC. Systematic review: the effects of harmful to the colon? J Clin Gastroenterol 2003; 36: of life results. J Gastrointest Surg 2006; 10:
fibre in the management of chronic idiopathic 386-389. 1330-1336. -
91You can also read