Chronic Idiopathic Pulmonary Fibrosis in Five Dogs - Vetjournal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Chronic Idiopathic Pulmonary Fibrosis
in Five Dogs
Five dogs presented with chronic and progressive pulmonary illness characterized by progressive
dyspnea, exercise intolerance, and significant inspiratory crackles on auscultation. Radiographi-
cally, there was a widespread and diffuse interstitial lung pattern with varying degrees of bronchial
involvement. Histopathological changes included thickened alveolar septa, interstitial fibrosis, and
pneumocyte hyperplasia. Based on the clinical, radiographic, and histopathological changes, a
diagnosis of idiopathic pulmonary fibrosis was made. Idiopathic pulmonary fibrosis is a chronic dis-
ease characterized by inflammation and fibrosis of the pulmonary interstitium and peripheral air-
spaces, which has been poorly characterized in the dog. J Am Anim Hosp Assoc 2001;37:119–127.
Remo G. Lobetti, MMedVet (Med), Introduction
Diplomate ECVIM Interstitial lung disease is a heterogeneous group of disorders of the lower
Rowan Milner, MMedVet (Med), respiratory tract characterized by derangements of the alveolar walls and
Diplomate ECVIM loss of functional alveolar capillary units.1–3 Many forms of pulmonary
injury can cause interstitial pneumonia, and in humans over 130 different
Emily Lane, BVSc, MPhil causes are known to induce interstitial lung disease.4 However, in over
50% of cases, no cause can be identified.2–4 Commonly recognized
causes include inhalation of toxic substances or organic antigens, adverse
drug reactions, and diseases such as sarcoidosis, collagen-vascular disor-
C ders, and unusual granulomatous diseases such as Wegener’s granulo-
matosis or eosinophilic granuloma.3,4 In animals, most of the recognized
causes of spontaneous interstitial pneumonia are infectious diseases, para-
sitic agents, or toxins. Potential known causes in the dog are infectious
diseases (e.g., distemper, toxoplasmosis, lungworms or migrating ascarid
larvae, pneumocystosis, fungi, or bacteria), pneumoconiosis, hypersensi-
tivity reactions, neoplasia, inhaled gases or toxins, irradiation, and sys-
temic lupus erythematosus.3,5 Since the clinicopathological picture of
interstitial pneumonia is often nonspecific, many cases are not identified
by a specific cause and likely go unreported.5 In the dog, the interstitial
lung diseases are a poorly characterized group of respiratory conditions,
and little is known of their prevalence, incidence, or etiopathogenesis.6
Acute and chronic interstitial pneumonia of unknown cause, termed
From the Departments of Companion Animal idiopathic pulmonary fibrosis (IPF), is encountered in all species. Idio-
Medicine (Lobetti, Milner) and pathic pulmonary fibrosis is characterized by inflammation and fibrosis of
Pathology (Lane), the pulmonary interstitium and peripheral airspaces.7 Idiopathic pul-
Faculty of Veterinary Science,
monary fibrosis should, however, not be considered a specific disease as it
University of Pretoria,
Private Bag X04, may have varying etiologies, including underlying connective-tissue dis-
Onderstepoort, 0110, eases, organic dust or other exposures, and prior acute lung injury. Less
South Africa. often, IPF may reflect a nonrepresentative biopsy of another process.8
The lack of a completely satisfactory morphological designation embrac-
Address all correspondence to Dr. Lobetti,
ing the variants of interstitial pulmonary disease has resulted in a confus-
Bryanston Veterinary Hospital,
P.O. Box 67092, ing array of terms.3,5 Two terms commonly used are interstitial
Bryanston, 2021, pneumonia and diffuse fibrosing alveolitis. The former term is preferred,
South Africa. as it covers the broad range of morphological, etiological, and pathogenic
JOURNAL of the American Animal Hospital Association 119120 JOURNAL of the American Animal Hospital Association March/April 2001, Vol. 37
aspects. Other terms used are chronic diffuse infiltrative lung
disease and diffuse interstitial pulmonary fibrosis.5 In A
humans, IPF is a specific syndrome characterized by a com-
bination of clinical, physiological, morphological, lavage,
and scintigraphic features.9 Diagnosis of IPF in humans
depends on histopathological analysis of open-chest lung
biopsy samples. The findings are consistent with an active
inflammatory disease resulting in progressive fibrosis and
end-stage honeycombing of the lung. The alveolitis involves
accumulation of monocytes (particularly macrophages),
thickening of the alveolar septa with edema, fibrinous exu-
date, fibroblast proliferation, and deposition of excess quan-
tities of collagen (fibrosing alveolitis).3,9
Although IPF is a distinct clinical entity, the literature deal-
ing with IPF is confusing, as it is referred to by different
names (e.g., lone cryptogenic fibrosing alveolitis, desquama-
tive interstitial pneumonia, usual interstitial pneumonia, and
giant-cell interstitial pneumonia).1,3,10 In the dog, this disease
entity is poorly characterized, and the lack of data is partly
due to the difficulty of accurate diagnosis and the lack of
biopsy or postmortem material from these cases.6,11 There are
widespread anecdotal accounts of a chronic respiratory condi-
tion in dogs characterized by severe radiographic changes
consistent with lung fibrosis and inspiratory crackles,11,12
with some resemblance to IPF in humans.6 The condition has
been described primarily in middle- to old-aged terrier breeds,
most notably the West Highland white. These dogs present
with a chronic and progressive illness characterized by cough-
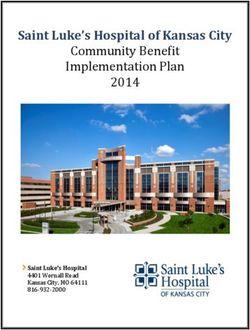
ing, dyspnea, exercise intolerance, and significant inspiratory Figures 1A, 1B—Thoracic radiographs in a six-year-old
crackles on auscultation, and an interstitial pattern is shown on schipperke (case no. 1) with chronic idiopathic pulmonary
radiography. Histopathological changes are consistent with a fibrosis. (A) Ventrodorsal thoracic radiograph showing an
chronic proliferative epithelial response,11 which has a simi- advanced interstitial pattern involving all the lung lobes.
(B) Lateral thoracic radiograph showing an advanced intersti-
larity to the clinical entity of IPF in humans. tial lung pattern tending to be bronchial to nodular and involv-
ing all lung fields.
Case Reports
B
Case No. 1
A six-year-old, fully vaccinated, female schipperke was
referred to the Onderstepoort Veterinary Academic Hospital
(OVAH) with a two-month history of progressive dyspnea,
exercise intolerance, and syncope. There was no history of
coughing. On clinical examination, polypnea and inspiratory
and expiratory dyspnea were evident. On thoracic ausculta-
tion, crackles were audible throughout the lung fields. Com-
plete blood count (CBC) and urine and fecal analyses all
were within reference ranges. Survey thoracic radiographs
showed an advanced interstitial lung pattern tending to be
bronchial to nodular and involving all lung fields [Figure 1].
Right heart enlargement was also evident and was attributed
to cor pulmonale. The only abnormality on transtracheal
aspirate (TTA) cytopathology was an increased amount of areas of bullous emphysema. Histopathology of a biopsy
mucus. Transtracheal aspirate culture was negative for both section showed severe, focally extensive to diffuse, subacute
bacterial and fungal growth. Fine-needle aspiration (FNA) to chronic, proliferative interstitial pneumonia. The pneumo-
cytopathology of the lung yielded no respiratory epithelial nia was characterized by the presence of a moderate number
cells. Antinuclear antibody (ANA) titer was negative. of mixed-type inflammatory cells within thickened alveolar
During the open-chest lung biopsy procedure, the lungs walls; proliferation of and occasional filling of alveoli by
appeared fibrosed, showed poor compliance, and had two alveolar macrophages with marked microvesicular cytoplas-March/April 2001, Vol. 37 Pulmonary Fibrosis 121
Figure 2—Histopathological
section of an open-chest biopsy
from the dog in Figure 1, show-
ing a mature, fibrous
connective tissue tract infiltrated
with lymphoplasmacytic inflam-
matory cells (large arrowhead)
and protein-rich fluid
in alveoli (small arrowhead)
(Hematoxylin and eosin stain,
10X; bar=130 µm).
Figure 3—Histopathological
section of an open-chest lung
biopsy from a three-year-old
Staffordshire bull terrier (case
no. 2), showing irregularly
thickened alveolar walls, oblit-
eration of most alveolar
spaces, and patchy hyperpla-
sia of type II pneumocytes
(arrowhead) (Hematoxylin and
eosin stain, 10X; bar=130 µm).
mic change; variable type II pneumocyte hyperplasia; patchy pleural cells, and marked subpleural lymphatic dilatation
alveolar filling with protein-rich, deeply hyaline fluid; mod- were also evident. Special stains for infectious agents (i.e.,
erate multifocal alveolar emphysema; moderate peribronchi- periodic acid-Schiff, Ziehl-Neelsen, Gram) were all negative.
olar and perivascular edema; and moderate hyperplasia of Due to the poor prognosis, the owners opted for euthana-
the smooth muscle around the terminal bronchioles. In addi- sia. No postmortem examination was performed.
tion, coalescing foci and fibrous tracts were present, mainly
beneath the pleura, where the alveoli were replaced by Case No. 2
mature, fibrous connective tissue and were infiltrated with a A three-year-old, fully vaccinated, female Staffordshire bull
moderate number of lymphoplasmacytic inflammatory cells. terrier was referred to the OVAH for chronic, progressive
Remaining bronchioles were collapsed, lined by hyperplastic dyspnea and exercise intolerance over a three-month period.
and often bizarrely shaped epithelial cells, and surrounded On clinical examination, cyanotic mucous membranes,
by loose lymphoplasmacytic cuffs [Figure 2]. Moderate sub- severe polypnea, and inspiratory dyspnea were present. On
pleural fibrosis, moderate hyperplasia of the mesothelial thoracic auscultation, inspiratory crackles were audible,122 JOURNAL of the American Animal Hospital Association March/April 2001, Vol. 37
Figure 4—Histopathological
section from an autopsy from
case no. 3, showing thickening
of alveolar walls and marked,
often bizarre hyperplasia of type
II pneumocytes (arrowhead)
(Hematoxylin and eosin stain,
10X; bar=130 µm).
especially over the caudoventral lung lobes. Complete blood discharge, the dyspnea was unchanged. Three months later,
count showed absolute polycythemia (hematocrit, 71%; ref- the owners opted for euthanasia. No autopsy was performed.
erence range, 37% to 55%; red blood cell count [RBC],
10.44 x1012/L; reference range, 5.5 to 8.5 x1012/L), with
Case No. 3
albumin within reference ranges.
Survey thoracic radiographs showed a severe, generalized, A three-year-old, fully vaccinated, male bull terrier was
mixed-bronchial and interstitial pattern and pleural thicken- referred to OVAH with a four-month history of lethargy as
ing. On TTA cytopathology, mucus, few macrophages, and well as panting and cyanotic mucous membranes when
alveolar epithelial cells were evident. Culture of a TTA speci- excited. Clinical evaluation showed mildly elevated body
men was negative for bacterial and fungal growth. Fine-nee- temperature, polypnea, inspiratory and expiratory dyspnea,
dle aspirate of the lung showed fibroblasts, macrophages, and cyanotic mucous membranes. The only abnormality on
and plaques of alveolar epithelial cells. An ANA titer was CBC was a mature neutrophilia (12.01 x109/L; reference
negative. range, 3.0 to 11.5 x109/L). Serum biochemistry and urine
An open-chest lung biopsy was done. Macroscopically, and fecal analyses all were within reference ranges. Survey
there was lung fibrosis with decreased compliance. radiographs of the thorax showed a bronchoalveolar to inter-
Histopathology showed severe, focally extensive, subacute to stitial pattern, affecting both lung fields. Transtracheal aspi-
chronic, proliferative interstitial pneumonia characterized by rate, bronchial lavage, and FNA of the lung were all
the presence of a small number of mixed-type inflammatory cytopathologically unrewarding, with few cells seen. Bacte-
cells; mature, fibrous connective tissue in irregularly thick- rial and fungal cultures from all three specimens were nega-
ened alveolar walls; and mild, patchy hyperplasia of type II tive. An ANA titer was negative.
pneumocytes. In scattered foci, often associated with bron- An open-chest biopsy was done. During the biopsy proce-
chioles, alveolar wall thickening virtually obliterated alveo- dure, the dog underwent cardiac arrest and died. On autopsy,
lar spaces [Figure 3]. Alveolar spaces, where present, were the lungs were incompletely collapsed, firm, mottled cream-
either overdistended or variably filled with protein-rich gray and red, and exuded small amounts of foam from cut
edema fluid and macrophages with abundant, finely vacuolar surfaces. On histopathology, there was severe, focally exten-
cytoplasm. Peribronchiolar smooth muscle was moderately sive to diffuse, subacute to chronic, proliferative interstitial
hyperplastic, as was the bronchiolar epithelium of terminal pneumonia characterized by moderate to marked alveolar
bronchioles. Special stains for infectious agents (i.e., peri- wall thickening by mature, fibrous connective tissue, infiltra-
odic acid-Schiff, Ziehl-Neelsen, Gram) were negative. tion of a small number of mixed-type inflammatory cells, and
The animal was treated with prednisolone (2 mg/kg body marked, often bizarre hyperplasia of type II pneumocytes
weight, q 24 hrs and tapered over a two-month period to 0.5 [Figure 4]. The remaining alveolar spaces contained protein-
mg/kg body weight, alternate days) and the antifibrotic drug, rich fluid and, often, small numbers of necrotic inflammatory
colchicine (0.03 mg/kg body weight, q 24 hrs), to possibly cells, fibrin, and alveolar macrophages. Greatly enlarged
aid in slowing progression of the disease. Six weeks after macrophages with abundant, finely vacuolar cytoplasm filledMarch/April 2001, Vol. 37 Pulmonary Fibrosis 123
many of the subpleural alveoli. Moderate perivascular
edema, mild to moderate hyperplasia of the smooth muscle A
surrounding bronchioles, and a few, scattered, loose lympho-
plasmacytic foci were also present. Special stains for infec-
tious agents (i.e., periodic acid-Schiff, Ziehl-Neelsen, Gram)
were negative.
Case No. 4
A five-year-old, female, fully vaccinated Staffordshire bull
terrier was referred to the OVAH for chronic respiratory dis-
ease. On clinical examination, a dry, hacking cough could
be easily elicited on tracheal palpation, and polypnea was
detected. A full CBC, serum biochemistry profile, urinaly-
sis, and ANA titer were all within reference ranges. Survey
thoracic radiographs showed possible cardiomegaly and an
interstitial to bronchial lung pattern [Figure 5]. Echocardiog-
raphy and electrocardiogram (EKG) tracings showed no
cardiac abnormalities. Transtracheal aspirate, tracheobron-
choscopy, and bronchoalveolar lavage were all within refer-
ence ranges. Based on the above findings, a diagnosis of
chronic, interstitial pneumonia was made. The dog was dis-
charged on supportive therapy consisting of nebulization, an
antitussive (codeine, 1 mg/kg body weight, q 12 hrs), and
prednisolone (2 mg/kg body weight, q 24 hrs and tapered
down over a two-month period to 0.5 mg/kg body weight,
alternate days). The dog progressively deteriorated and was
readmitted four months later. At this point, she showed inspi-
ratory dyspnea with no cough. Survey radiographs of the
thorax showed a severe, diffuse, interstitial lung pattern [Fig-
ure 6]. Transtracheal aspirate was within reference ranges.
Two days after being admitted, the dog went into respiratory Figures 5A, 5B—Thoracic radiographs in a five-year-old
arrest and died. Staffordshire bull terrier (case no. 4) with chronic idiopathic
At autopsy, the lungs did not collapse on opening the tho- pulmonary fibrosis. (A) Dorsoventral thoracic radiograph
racic cavity and showed areas of consolidation and hepatiza- showing an early diffuse interstitial pattern involving all the
lung lobes. (B) Lateral thoracic radiograph showing an early
tion with multifocal, whitish-gray, peribronchiolar areas that diffuse interstitial lung pattern.
felt firm and exuded foam on cut surface. Histopathological
examination revealed chronic and proliferative interstitial
pneumonia throughout the parenchyma with marked alveolar
wall thickening due to proliferation of type II pneumocytes,
fibrous connective tissue, and various inflammatory cells.
The latter consisted predominately of macrophages, some
giant cells, and lesser numbers of lymphocytes and plasma
cells [Figure 7]. A similar inflammatory cell infiltrate and
fibrin filled the alveolar spaces. There was marked bronchio-
lar epithelial hyperplasia and peribronchiolar smooth-muscle
hyperplasia and fibrosis.
Case No. 5
A three-year-old, fully vaccinated, female Staffordshire bull B
terrier was referred to the OVAH for chronic, progressive
dyspnea over a 12-month period. On clinical examination,
cyanotic mucous membranes, severe polypnea, and dyspnea moderate, generalized alveolar pattern. Before any further
were present. On thoracic auscultation, inspiratory crackles diagnostic tests could be done, the dog died.
were audible throughout the lung fields. Complete blood At autopsy, the lungs were congested, failed to collapse
count showed absolute polycythemia (hematocrit, 72%; on opening the thoracic cavity, and were markedly increased
RBC, 11.50 x1012/L) and an albumin of 36 g/L (reference in consistency. Histopathology showed severe, extensive,
range, 27 to 35 g/L). Survey thoracic radiographs showed a multifocal to coalescing pulmonary fibrosis; mixed-type124 JOURNAL of the American Animal Hospital Association March/April 2001, Vol. 37
Idiopathic pulmonary fibrosis is thought to occur secondary
A to any lower respiratory tract insult in which the inflamma-
tory response to the insult cannot be controlled.1 Interstitial
fibrosis is seen in the lung in response to a variety of insults
and often appears stereotypical in terms of its clinical and
pathological features. However, exposure to a known etio-
logical factor does not always lead to fibrosis. In humans, the
etiopathogenesis of idiopathic pulmonary fibrosis is not
known, but a possible role for immune complexes (i.e.,
unidentified antigens), which are chemotactic for polymor-
phonuclear leukocytes and active macrophages, has been
postulated.11
Pulmonary fibrosis resulting from an interstitial pneumo-
nia may either be attributable to acute damage or to chronic
inflammatory conditions involving a proliferative cellular
response.13 During the acute phase, the most dramatic fea-
tures of the lesion are the flooding of alveoli with serofibrin-
ous exudate and the congestion and edema of alveolar
walls.5 Replacement of degenerative type I pneumocytes
takes place on intact basement membranes by proliferation
of type II pneumocytes. This resultant epithelialization of the
alveoli is a common feature of subacute to chronic intersti-
tial pneumonia.5 Proliferation of alveolar type II pneumo-
cytes marks the shift from the exudative to the proliferative
stage of interstitial pneumonia. Onset of fibrosis is a critical
feature of the proliferative phase, because it is irreversible.5
Stimulation or up-regulation of fibroblast proliferation and
Figures 6A, 6B—Thoracic radiographs in a five-year-old collagen synthesis is induced by macrophage-derived
Staffordshire bull terrier (case no. 4) with chronic idiopathic cytokines.5
pulmonary fibrosis, taken four months after initial Alveoli are lined by two types of epithelial cells: type I
presentation. (A) Ventrodorsal thoracic radiograph showing and II pneumocytes. Type I pneumocytes have a large sur-
progression of the interstitial lung pattern. (B) Thoracic lateral
radiograph showing progression of the interstitial lung
face-to-volume ratio and cover a large area of the alveolar
pattern. wall. The morphological features of these cells make them
highly sensitive to injury, whereas type II pneumocytes are
more compact and are thus less vulnerable. When alveolar
injury occurs following an acute exudative phase of inflam-
mation, type II pneumocytes proliferate to fill denuded areas
of alveoli. If inflammation abates and scarring is not severe,
type II pneumocytes can later be transformed into type I
pneumocytes.5 Acute pulmonary injury, whether toxic, meta-
bolic, or infectious in origin, causes damage principally to
alveolar endothelial cells and type I pneumocytes.5 Whether
the endothelium or epithelium is damaged first is dependent
on the nature, portal of entry, and intensity of the insult and,
to some extent, the species affected.5
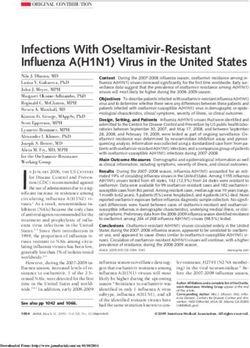
Several parts of the alveolar structure are affected in IPF,
B including the alveolar walls lined with type I and type II
pneumocytes, and the interstitial supporting structure com-
posed of fibroblasts, myofibroblasts, collagen, adhesive pro-
inflammatory cells; mature, fibrous connective tissue within teoglycans, and capillary endothelium3 [Figure 8]. In the
irregularly thickened alveolar walls; and mild, patchy hyper- early stage of the disorder, there is patchy alveolitis with
plasia of type II pneumocytes. A lung sample was negative mild to moderate thickening of the alveolar walls.9,14 As the
for bacterial and fungal growth. disease progresses, the inflammation persists, and progres-
sive derangement of the alveolar structures occurs, including
Discussion loss of type I pneumocytes, proliferation of type II pneumo-
The five dogs described in this report showed clinical, radio- cytes, migration of bronchoalveolar epithelial cells to the
graphic, and histopathological changes compatible with IPF. alveoli, loss of capillaries, and thickening of the walls of theMarch/April 2001, Vol. 37 Pulmonary Fibrosis 125
Figure 7—Histopatho-
logical section from an
autopsy from case no. 4,
showing marked conges-
tion and alveolar wall
thickening due to prolif-
eration of type II pneu-
mocytes and the
presence of mainly his-
tiocytic inflammatory
cells (Hematoxylin and
eosin stain, 10X;
bar=130 µm).
small airways and arteries. The interstitial matrix is
expanded with large numbers of fibroblasts, myofibroblasts,
smooth-muscle cells, and masses of twisted, deranged fibers
(particularly type I collagen).14 These histopathological
changes were evident in the lung sections from all five dogs.
Idiopathic pulmonary fibrosis is thought to represent a
stereotyped inflammatory response of the alveolar wall to
injuries of different types, durations, and intensities.15 In
humans, detailed evaluations for a specific etiology have
been fruitless.9 Studies have also shown that T-lymphocytes
from patients with this disorder proliferate in response to a
variety of “self” components, including type I pneumocytes,
collagen, and deoxyribonucleic acid (DNA).16 There is evi-
dence that proliferating type II pneumocytes in regenerating
alveolar epithelium are implicated in the pathogenesis of this
disorder.17 Several studies in humans have suggested a
genetic link for IPF, but definitive evidence is lacking.1,3,18
No obvious clinical or historical cause could be identified in
these five cases. Although the dogs in this report were not
related, four of the dogs were bull terrier-type dogs, and the Figure 8—Schematic representation of the pathogenic
one case reported in the veterinary literature was a dog of a mechanisms within the alveolar space, alveolar walls, and
similar breed.6 Therefore, it is possible that bull terrier pulmonary interstitium that can lead to inflammation and
breeds are at an increased risk for the development of IPF. eventual fibrosis. The focus is the pulmonary macrophage
that is activated by inhaled antigens (Ag), circulating immune
In humans, all age groups can be affected with IPF; how-
complexes, or circulating antigens (Cf). The net result is that
ever, it is more common between the ages of 20 to 40 the macrophage, through mediators such as chemotaxins,
years.3,7 This correlates to the age group of these dogs, as attracts inflammatory cells from the circulation into the alveo-
their ages ranged from three to six years. In humans, an irri- lar space, as well as stimulates fibrogenesis and muscle cell
tative, nonproductive cough is present in approximately 15% proliferation. Interstitial fibrosis may result. (Reproduced with
permission from: Reynolds HY. Interstitial lung diseases. In:
of patients.3 An interstitial pneumonia is not usually associ- Isselbacher KJ, Braunwald E, Wilson JD, Martin JB, Fauer
ated with a cough, and manifestations of this disease would AS, Kasper DL, eds. Harrison’s principles of internal medi-
not be expected until pulmonary gas exchange has already cine. 13th ed. New York: McGraw-Hill, 1994:1206–11).126 JOURNAL of the American Animal Hospital Association March/April 2001, Vol. 37
been severely compromised.3,10,13 One dog was initially pre- present in all five cases of this report. These result from both
sented with a cough, whereas the other four did not have a an increased alveolar-arterial oxygen gradient and increased
history of coughing. dead-space ventilation.3,7,9,10
In humans, the physical examination may be entirely nor- A lung biopsy is necessary to confirm the diagnosis and
mal. Loud, dry, and basilar, so-called velcro crackles are vir- to determine prognosis. An open-lung biopsy is preferred
tually diagnostic in advanced disease. A patient with because of the ability to obtain a greater amount of tissue
end-stage IPF presents with the physical findings of cor pul- and the opportunity for the surgeon to select areas of obvious
monale.3,7 Clinical findings in these dogs were limited to the involvement. It is well known that while some areas of the
respiratory system and consisted of polypnea, dyspnea, and lung may demonstrate fibrosis, other areas may show an
inspiratory crackles. Cyanosis was present in two cases. active process.7 Histopathology of the lung from humans
In humans, typical chest radiographic changes demon- affected with IPF typically showed severe, chronic, intersti-
strate diffuse reticular or reticulonodular infiltrates that have tial pneumonia; marked fibrosis; lymphoplasmacytic and
lower-zone predominance. In the advanced stages of IPF, a macrophage infiltration; epithelialization; patchy alveolar
fine honeycombing (i.e., small, cystic spaces) and reduced edema; and hypertrophy/hyperplastic type II pneumocytes.
lung volume are evident.1 Radiographically, interstitial lung These changes are similar to the changes present in the lungs
disease in the dog may appear as a diffuse increase in over- of the dogs described in this report and to what has been
all pulmonary density; indistinct, smaller, pulmonary vascu- reported in another affected dog.6
lar structures; indistinct linear or reticular densities; or as a The principal therapy for IPF is corticosteroids.3 In
combination of short linear and small nodular (i.e., reticulo- approximately 20% of human cases, corticosteroid therapy
nodular) densities throughout the lung.19 However, unstruc- not only provides symptomatic relief but also increases sur-
tured increases in interstitial density may reflect past or vival in these diseases. In humans, another guide to the
current disease.19 An increased interstitial opacity on tho- effectiveness of corticosteroid therapy appears to be the
histopathological findings: if dense fibrosis with honey-
racic radiographs is usually the only indication that intersti-
combed lung is present, the results of therapy are likely to
tial disease exists, but this type of pattern is associated with
be minimal; however, if examination reveals an active cel-
a disparate group of thoracic conditions including acute
lular process (neutrophils and macrophages), then benefi-
fibrosing alveolitis, cardiogenic and noncardiogenic pul-
cial results from corticosteroid therapy can be expected.10
monary edema, infection, pulmonary infiltration with
Symptomatology, chest radiographs, and lung function
eosinophilia, certain infiltrative neoplasms, exposure to tox-
studies can judge improvement. Maintenance therapy with
ins such as paraquat, and certain systemic illnesses. Most of
corticosteroids after the first two to four weeks should be
these conditions have a rapid clinical onset (hours to days)
titrated to the lowest dose that maintains clinical benefits.
and rarely have a slow, chronic-progressive course.6,11 Sur-
Should the disease not respond or be progressive, immuno-
vey thoracic radiographs in these dogs showed an interstitial
suppression with cyclophosphamide or azothioprine should
lung pattern tending to be bronchial to nodular and involving be considered.3 Other antifibrotic or immunosuppressive
all lung fields. agents such as colchicine, penicillamine, and cyclosporine
In humans affected with IPF, changes in CBC, routine have not been thoroughly evaluated in humans.3,7,10 In the
serum biochemistry, and urinalysis are not seen.3,7 Approxi- literature, it has been reported that a proportion of canine
mately 40% of human patients with IPF have positive cases show good clinical response to corticosteroid therapy,
rheumatoid or antinuclear factors. These findings suggest but the condition eventually results in respiratory failure.6
that an immunopathogenetic mechanism may be operative in Concurrent use of azothioprine may be of additional bene-
some cases of IPF. Some cases of IPF may, in fact, represent fit.11 Two of the dogs in this report did not respond to corti-
a limited connective-tissue disease of the lung.3,7,10 Antinu- costeroids.
clear antibody was negative in four of the dogs tested in this Although oxygen administration may improve clinical
report, thus reducing the possibility of an immune-mediated signs, it may in fact worsen the pulmonary lesions. Oxygen
collagen-vascular disorder. toxicity is emerging as an important form of inhaled injury,
Classically in human patients, spirometry demonstrates a as concentrations over 50% can produce damage in already
reduction of the total lung capacity that is a restrictive venti- compromised lungs after two to three days of exposure.5
latory defect.3 The flow rates are usually preserved, provided Proliferating type II pneumocytes are sensitive to the toxic
the patient does not have a complicating airway problem.3,10 effects of oxygen.13
The diffusing capacity for carbon monoxide is reduced,
especially after exercise.3 The compliance of the lung (i.e., Conclusion
elastic recoil) is also reduced. Although not specifically Although not a common disease, IPF should be considered
measured, decreased lung compliance was evident macro- in all dogs with chronic dyspnea and radiographic changes
scopically during thoracotomy in the dogs of this report. The suggestive of interstitial pneumonia. Evaluation of lung tis-
most important and probably the earliest pathophysiological sue, obtained either antemortally (via thoracotomy or thora-
derangements are hypoxemia and hyperventilation, made coscopy) or postmortally, is necessary to further elucidate
worse by exercise. Exercise intolerance and polypnea were this disease in the dog.March/April 2001, Vol. 37 Pulmonary Fibrosis 127
Acknowledgments 19. Crystal RG, Fulmer JD, Roberts WC, Moss ML, Line BR, Reynolds
HY. Idiopathic pulmonary fibrosis: clinical, histologic, radiographic,
The authors wish to thank Professor Kirberger for the radio- physiologic scintigraphic, cytologic, and biochemical aspects. Ann Int
graphic assessment of these cases; Dr. A. Sigobodhla for the Med 1976;85:769–88.
autopsy and histopathology of case no. 4; Dr. E. Dvir for 10. Schwarz MI. Interstitial pneumonia. In: Mitchell RS, ed. Synopsis of
providing case no. 5; and Professor N. Duncan for the clinical pulmonary disease. 2nd ed. St Louis: Mosby, 1978:241–47.
11. Corcoran BM. Idiopathic pulmonary fibrosis: an emerging disease in
autopsy and histopathology of case no 5. dogs. In: Congress synopses: 22nd World Sm Anim Vet Assoc Con-
gress, 1997:42.
12. Martin MWS. Progressive lung disease with pulmonary crackles in 18
References terrier breed dogs. In: Congress synopses: Brit Sm Anim Vet Con-
11. Crystal RG, Bitterman PB, Rennard SI, Hance AJ, Keogh BA. Intersti- gress, 1998:287.
tial lung diseases of unknown cause. N Engl J Med 1984;310:154–66. 13. Cogan DC, Carpenter JL. Diffuse alveolar injury in two dogs. J Am
12. Buergelt CD, Hines SA, Cantler G, Stirk A, Wilson JH. A retrospec- Vet Med Assoc 1989;194:527–30.
tive study of proliferative interstitial lung disease of horses in Florida. 14. Madri JA, Furthmayr H. Collagen polymorphism in the lung: an
Vet Path 1986;23:750–56. immunochemical study of pulmonary fibrosis. Human Path
13. Reynolds HY. Interstitial lung diseases. In: Isselbacher E, Braunwald 1980;11:353–66.
JD, Wilson JB, Martin AS, Fauer DL, Kasper KJ, eds. Harrison’s prin- 15. Cotran RS, Tumar V, Robbins SL. Robbins pathologic basis of disease.
ciples of internal medicine. 13th ed. New York: McGraw-Hill, 5th ed. Philadelphia: WB Saunders, 1994:714–15.
1994:1206–11. 16. Krawis TC, Ahmed A, Brown TE, Fulmer JD, Crystal RG. Pathogenic
14. Dungworth DL. Interstitial pulmonary disease. Adv Vet Sci Comp mechanisms in pulmonary fibrosis: collagen-induced migration inhibi-
Med 1982;26:173–200. tion factor production and cytotoxicity mediated by lymphocytes. J
15. Dungworth DL. The respiratory system. In: Zubb PC, Kennedy N, Clin Inves 1976;58:1223–32.
Palmer KVF, eds. Pathology of domestic animals. 4th ed. San Diego: 17. Corrin B, Dewar A. Pathogenesis of idiopathic interstitial pulmonary
Academic Press, 1993:598–607. fibrosis. Ultrastructural Path 1996;20:369–71.
16. Corcoran BM, Dukes-McEwan J, Rhind S, French A. Idiopathic pul- 18. Marshall RP, Mcanulty RJ, Laurent GJ. The pathogenesis of pul-
monary fibrosis in a Staffordshire bull terrier with hypothyroidism. J monary fibrosis: is there a fibrosis gene? Intl J Biochem Cell Biol
Sm Anim Pract 1999;40:185–88. 1997;29:107–20.
17. Du Bios RM. Idiopathic pulmonary fibrosis. Ann Rev Med 19. Myer W. Radiography review: the interstitial pattern of pulmonary dis-
1993;44:441–50. ease. Vet Rad 1980;21:18–23.
18. Katzenstein AL, Fiorelli RF. Non specific interstitial pneumonia/fibro-
sis: histiologic features and clinical significance. Am J Surg Path
1994;18:136–47.You can also read