Current Status of Liver Transplantation for Cholangiocarcinoma - USA Health System
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
REVIEW ARTICLE GOLDARACENA, GORGEN, AND SAPISOCHIN
Current Status of Liver Transplantation
for Cholangiocarcinoma
Nicolas Goldaracena, Andre Gorgen, and Gonzalo Sapisochin
Multi-Organ Transplant, Division of General Surgery, Department of Surgery, University Health Network, University of Toronto,
Toronto, Ontario, Canada
Cholangiocarcinoma (CCA) is the second most common liver cancer, and it is associated with a poor prognosis. CCA can
be divided into intrahepatic, hilar, and distal. Despite the subtype, the median survival is 12-24 months without treatment.
Liver transplantation (LT) is recognized worldwide as a curative option for hepatocellular carcinoma. On the other hand,
the initial results for LT for CCA were very poor mainly due to a lack of adequate patient selection. In the last 2 decades,
improvements have been made in the management of unresectable hilar CCA, and the results of LT after neoadjuvant
chemoradiation have been shown to be promising. This has prompted a consideration of hilar CCA as an indication for
LT in some centers. Furthermore, some recent research has shown promising results after LT for patients with early
stages of intrahepatic CCA. A better understanding of the best tools to prognosticate the outcomes of LT for CCA is still
needed. Here, we aimed to review the role of LT for the treatment of patients with perihilar and intrahepatic CCA. Also,
we will discuss the most recent advances in the field and the future direction of the management of this disease in an era
of transplantation oncology.
Liver Transplantation 24 294–303 2018 AASLD.
Received July 18, 2017; accepted October 1, 2017.
Since the establishment of liver transplantation (LT) stage liver disease, its indication to treat tumors con-
as the best treatment option for patients with end- fined to the liver has grown substantially.(1,2)
Hepatocellular carcinoma (HCC) is the most fre-
quent liver cancer, and LT is the best treatment option
in selected patients because it removes both the cancer
Abbreviations: BILCAP, Adjuvant capecitabine for biliary tract can-
cer; CA19-9, carbohydrate antigen 19-9; CCA, cholangiocarcinoma; (with the widest possible margins) and the underlying
ELITA, European Liver and Intestine Transplant Association; liver disease.(3-5) However, as the understanding of
HCC, hepatocellular carcinoma; hCCA, hilar cholangiocarcinoma; tumor biology and multidisciplinary oncological treat-
HCC-CCA, mixed hepato-cholangiocarcinoma; HCV, hepatitis C
virus; iCCA, intrahepatic cholangiocarcinoma; iCCA1HCC, concom- ments improve, the indication of LT to treat other
itant intrahepatic cholangiocarcinoma and hepatocellular carcinoma in unresectable tumors confined to the liver (ie, cholangio-
the explant; iCCA-HCC, mixed hepatocellular cholangiocarcinoma;
carcinoma [CCA], metastatic neuroendocrine tumors)
LT, liver transplantation; MELD, Model for End-Stage Liver Dis-
ease; OS, overall survival; PSC, primary sclerosing cholangitis; has expanded.(6-10) LT has therefore gained momen-
TRANSPHILL, Liver Resection Versus Radio-Chemotherapy- tum as a treatment for patients with cancer. Because of
Transplantation for Hilar Cholangiocarcinoma; UCLA, University
of California, Los Angeles; UNOS, United Network for Organ Shar-
organ shortages, the main concern when offering a
ing; VEGF, vascular endothelial growth factor. transplant to these patients is the impact on other
Address reprint requests to Gonzalo Sapisochin, M.D., Multi-
patients on the waiting list.(11) With recent advances in
Organ Transplant, Division of General Surgery, Department of the treatment of hepatitis C virus (HCV), there seems
Surgery, University Health Network, University of Toronto, 585 to be a decrease in the number of patients in need of a
University Avenue, 11PMB184, Toronto, M5G 2N2, ON
Canada. Telephone: 1 1-416-340-5230; FAX: 1 1-416-340-
LT because of HCV, resulting in a potential increase in
5242; Email: gonzalo.sapisochin@uhn.ca the organ pool.(12) However, in some regions (such as
Copyright V
C 2017 by the American Association for the Study of Liver
North America), the increase in the incidence of
Diseases. patients with cirrhosis with nonalcoholic steatohepatitis
View this article online at wileyonlinelibrary.com.
may result in no change in the organ pool.(13) Further-
more, living donor LT may be another excellent option
DOI 10.1002/lt.24955
to provide access to LT to those patients with cancer.
Potential conflict of interest: Nothing to report. In this regard, the use of LT for the treatment of
CCA has become a focus of interest around the
294 | REVIEW ARTICLELIVER TRANSPLANTATION, Vol. 24, No. 2, 2018 GOLDARACENA, GORGEN, AND SAPISOCHIN
world.(14-16) This type of tumor arising from the bile
duct epithelium is very aggressive, and its prognosis is
mainly dependent on its location along the biliary tree
and its chance of being completely resected with nega-
tive margins.(17)
The role of LT to treat patients with CCA has been
explored in some centers for those patients presenting
with an unresectable tumor confined to the hepatic
hilum (ie, perihilar CCA/Klatskin tumor)(18-21) and
more recently for patients with “very early” (single tumor
2 cm) intrahepatic cholangiocarcinomas (iCCAs).(8)
So far, only these 2 locations of CCA are the ones
where patients can potentially benefit from LT.
Here we aimed to review the role of LT for the treat-
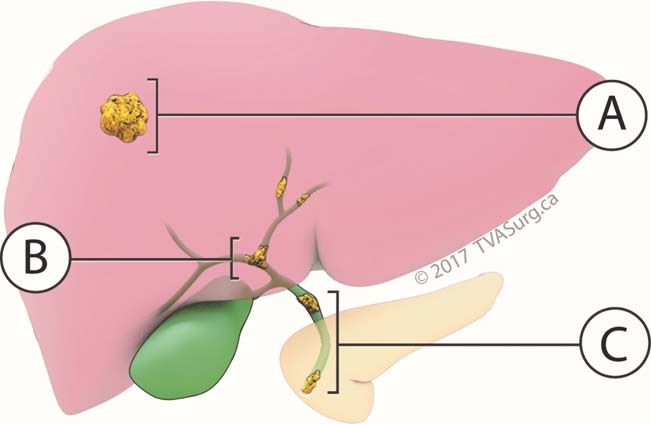
ment of patients with perihilar CCA and iCCA. Also, FIG. 1. CCA locations. (A) Intrahepatic (iCCA). (B) Hilar
we will discuss the most recent advances in the field and (hCCA). (C) Distal.
the future direction of the management of this disease.
CCA Classification approach was first attempted in the late 1990s and
failed to show any promising results because the 5-year
CCA is a malignant tumor of the biliary system that survival rate was reported to be approximately 18%
stands as the second most common primary liver can- (Table 1).(33) However, this was a retrospective analysis
cer after HCC.(22) More than 95% of the time, it con- of a small series where patients did not undergo any
sists of an adenocarcinoma that depending on its type of protocolized neoadjuvant or adjuvant
locations on the biliary tree, can be classified as iCCA treatment.
or extrahepatic CCA.(23) In turn, the extrahepatic
CCA can be subclassified into hilar (Klatskin tumor)
or distal CCA (mid third and lower third bile duct
THE “MAYO CLINIC” PROTOCOL
lesions; Fig. 1).(24) In the year 2000, the Mayo Clinic group reported their
preliminary experience with a protocol of neoadjuvant
Hilar CCA therapy followed by LT.(41) The neoadjuvant protocol
consisted of the combination of external beam and
The incidence of hilar cholangiocarcinoma (hCCA; transcatheter radiation with intravenous 5-fluorouracil.
Klatskin tumor) is approximately 7000 cases per year A total of 11 out of the initial 19 patients who were
in North America, representing around two-thirds of found to be eligible for the study completed the proto-
all cases of CCA.(25) Unfortunately, the overall survival col and underwent LT, showing encouraging
(OS) for patients suffering from an hCCA is detri- results.(18) In 2004, the previous series was updated
mental, ranging between 12 and 24 months.(26) and an 82% 5-year survival rate was reported for 24
It is well-known that the most important prognostic patients undergoing the “Mayo protocol.”(35,42) In
factor is to achieve a complete resection with negative 2005, the same group published their experience of
oncological margins, but unfortunately, this is only neoadjuvant chemoradiation followed by LT. In this
achieved in 25%-40% of the patients.(27-29) The cur- study, they compared those patients undergoing a
rent 5-year survival rate after surgery, even in select resection approach alone against those who underwent
patients, rarely exceeds 40%.(30-32) From this low sur- neoadjuvant therapy in addition to LT.(10) The LT
vival after resection derives the concept of treating this group with neoadjuvant chemoradiation (38 patients)
patient population with a LT. This concept allows a achieved better OS at 1 year (92% versus 82%), 3 years
complete resection with good negative margins in (82% versus 48%), and 5 years (82% versus 21%) when
patients who have tumors that are locally unresectable compared with the resection group (26 patients). Also,
due to the invasion of major vessels, bilobar tumor the LT group experienced lower posttransplant recur-
involvement, or insufficient hepatic reserve. This rence (13% versus 27%).(10) Importantly, all the
REVIEW ARTICLE | 295GOLDARACENA, GORGEN, AND SAPISOCHIN LIVER TRANSPLANTATION, February 2018
TABLE 1. Patient Survival and Disease-Free Survival of Patients Transplanted With hCCA
Neoadjuvant
Number of Chemotherapy
Total Patients 1- With or
Number Who Year 5-Year Without
of Underwent OS 3-Year OS Radiation
References Center Study Type Patients LT (%) (%) OS (%) (%) Therapy Comments
Iwatsuki et al.(34) University of Retrospective 72 38 (53) 60 32 25 61% 37 (51%) disease free
(1998) Pittsburgh comparing of patients at 3 years
resection to LT
Sudan et al.(18) University of Retrospective 17 11 (65) — — — Yes Median survival
(2002) Nebraska 11 months
Rea et al.(10) Mayo Clinic Retrospective 71 38 (54) 79 61 58 Yes —
(2005) comparing
resection to LT
Heimbach et al.(35) Mayo Clinic Retrospective 106 65 (61) 91 — 76 Yes Median time
(2004) to recurrence
22 months
Rosen et al.(36) Mayo Clinic Retrospective 148 90 (61) 82 63 55 Yes —
(2008)
Kaiser et al.(37) Germany Retrospective 47 47 (100) 61 31 22 No —
(2008) Multicenter
Darwish et al.(38) United States Retrospective 287 216 (75) — 68 (2 years) 53 Yes 65% 5-year
(2012) Multicenter disease-free
survival
Welling et al.(20) University of Retrospective 12 6 (50) 83 — — Yes —
(2014) Michigan
Marchan et al.(39) Emory Retrospective 10 8 (80) 80 67% (2 years) — Yes —
(2016)
Mantel et al.(40) ELITA database Retrospective 173 28 (16)* — — 59* Yes This article compared
(2016) Multicenter 77 (45)† 21† patient selection within
“Mayo protocol” to
beyond that protocol.
*Within Mayo protocol.
†
Beyond Mayo protocol.
patients who underwent LT were deemed to be livers.(44) In 2012, a multicenter study of 12 US centers
unresectable. including patients with hCCA who were treated with
On the basis of their experience, the Mayo clinic neoadjuvant therapy followed up by LT reported a
group described the risk factors for dropout of the LT 65% 5-year recurrence-free survival and an 11.5%
waiting list due to disease progression.(43) These were dropout rate after 3.5 months of therapy.(38) This
found to be as follows: carbohydrate antigen 19-9 study validated the hypothesis that it is appropriate for
(CA19-9) 500 U/mL, a mass 3 cm, malignant selected patients with hCCA to receive the proposed
brushing or biopsy, and a Model for End-Stage Liver MELD exception points and therefore have a faster
Disease (MELD) score 20. Likewise, factors found access to transplant.
to be predictors of recurrence after LT were as follows:
an elevated CA19-9, the presence of an encased portal LIVER RESECTION VERSUS LT
vein, and the evidence of a residual tumor on FOR hCCA
explant.(43)
Since the establishment of the Mayo protocol, sev- Other groups have also assessed the role of resection
eral other groups reported their experience with the versus transplantation for hCCA.(34,45) In 2011, Hong
same or similar protocols. In 2006, based on the expe- et al. found in a 24-year experience that surgical resec-
riences of the Mayo Clinic and the University of tion was a predictor of worse survival outcome when
Nebraska, Gores et al. proposed that patients with compared with transplantation.(9,46) However, data of
unresectable hilar CCA arising in the setting of pri- this study might be misleading because it included
mary sclerosing cholangitis (PSC) should receive a iCCA and hCCA as well as patients with and without
MELD score exception points for better allocation of liver cirrhosis. Also, numbers in the hCCA group were
296 | REVIEW ARTICLELIVER TRANSPLANTATION, Vol. 24, No. 2, 2018 GOLDARACENA, GORGEN, AND SAPISOCHIN
low (13 patients in the LT group versus 7 in the resec- (HCC-CCA) in the explant pathology.(62) Moreover,
tion group). It is important to note that this was not a a German series of 10 patients who underwent LT
randomized controlled trial and therefore patients in with a preoperative diagnosis of iCCA demonstrated a
the LT group were unresectable and likely had more 5-year survival of 33%.(63) The results of these studies
advanced disease. Therefore, there is a need for ran- showed a poor and likely unacceptable 5-year survival
domized controlled trials that can better compare the for LT in the current era of organ shortage.
outcome of resectable (with similar disease stage) In 2011, the University of California, Los Angeles
hCCA between LT and resection. (UCLA) group published a series comparing LT and
To date, until randomized controlled trials show resection using neoadjuvant chemotherapy associating
otherwise, LT after aggressive neoadjuvant therapy radiotherapy in some patients.(9) In this 24-year expe-
including external beam and transluminal radiation, as rience with a total of 132 CCAs, they performed LT
well as systemic chemotherapy, seems like an adequate in 38 patients (25 of those were iCCA). The 5-year
treatment for both unresectable hCCA, as well as survival after LT was 32%. Unfortunately, the OS was
hCCA arising in the setting of PSC.(25) However, calculated for both iCCA and hCCA, and the data on
these transplants should be conducted in large aca- each type of cancer were not available.(9) In a subse-
demic centers with both a transplant and surgical quent publication, the same group reported a multivar-
oncology expertise. iate analysis identifying predictors of tumor recurrence.
Multifocal tumors, perineural invasion, infiltrative sub-
type, and lack of neoadjuvant and adjuvant therapies
Intrahepatic CCA were found to be associated with a poor prognosis.(46)
Intrahepatic cholangiocarcinoma (iCCA) corresponds On the other hand, tumor size failed to be found as a
to 5%-10% of all CCAs.(47) The incidence of iCCA is predictor of tumor recurrence. However, this study was
0.6-1.0/100,000 new cases per year in the United a retrospective analysis where only 13 patients had
States and its incidence is increasing.(48) This increase received neoadjuvant treatment with chemotherapy
seems to be greater in groups with risk factors for plus radiation therapy, making the results difficult to
HCC as cirrhosis, chronic viral hepatitis, and nonalco- interpret.(46)
holic steatohepatitis.(49,50) Several retrospective series were conducted to review
the outcomes after LT for patients with incidental
iCCA. A Canadian multicenter study found 10
LT FOR iCCA
patients who underwent LT for other indications and
Currently, iCCA is a contraindication for LT in most were found to have CCA features in the explant. The
LT centers around the world.(15,51) This is probably 3-year OS in this series was 30%.(60) Also, Facciuto
related to the very poor outcomes in the early experi- et al. studied the explanted specimens and found 32
ence of LT for this disease.(52-54) The results of initial patients with intrahepatic biliary differentiation and
experiences were difficult to interpret as most series cirrhosis. Interestingly, they conducted a matched
included patients with both iCCA and hCCA as well analysis of this CCA population with HCC control
as patients with and without liver cirrhosis. It is well- patients. When patients were stratified by Milan crite-
known that iCCA and hCCA are different entities ria, those within Milan had similar OS between groups
that may present with different outcomes, and we also (78% for CCA versus 79% for only HCC; P 5 0.61).
know from the HCC literature that tumors arising In the same way, patients outside Milan criteria had a
from healthy versus cirrhotic livers may also present lower 5-year OS compared with those within Milan
with different outcomes.(55) criteria, but it was not different between CCA and
In 2004, Robles et al. published a retrospective anal- HCC groups (48% for CCA versus 53% for only
ysis of a multicenter experience with 23 patients who HCC; P 5 0.12).(64) In 2016, Vilchez et al. conducted
underwent LT for iCCA (Table 2).(56) Notably, in 10 a retrospective analysis using the United Network for
of their patients, the tumor was diagnosed incidentally Organ Sharing (UNOS) database. They analyzed 4049
after LT. The overall 5-year survival was reported to patients, of whom 440 had an iCCA diagnosis. The 5-
be 42%. Likewise, in 2011, Sapisochin et al. reported a year OS for patients with iCCA in the explant was
47% 5-year survival for patients who underwent trans- 47%, but no subgroup analysis according to the size of
plantation with preoperative diagnosis of HCC but the tumor was conducted. A population-based study
had either iCCA or mixed hepato-cholangiocarcinoma from the United States found a worse OS when
REVIEW ARTICLE | 297GOLDARACENA, GORGEN, AND SAPISOCHIN LIVER TRANSPLANTATION, February 2018
TABLE 2. Patient Survival and Disease-Free Survival From Studies Including Patients Transplanted for Both iCCA
and hCCA
Neoadjuvant
Chemotherapy
With or
Total Without
Number 1-Year 3-Year 5-Year Radiation
References Center Study Type of Patients OS (%) OS (%) OS (%) Therapy Comments
O’Grady et al.(52) King’s College Retrospective 13 hCCA 38 10 10 No —
(1988) 13 iCCA
Yokoyama et al.(57) University of Retrospective 19 hCCA 24 24 0 No —
(1990) Pittsburgh 2 iCCA 50 0 —
Meyer et al.(58) Cincinnati Retrospective 207 72 48 23 No 10% had adjuvant therapy.
(2000) Transplant Multicenter 84% disease-free survival
Tumor Registry in 25 months
Shimoda et al.(59) UCLA Retrospective 9 hCCA 86 31 — 4 patients 8 patients with iCCA-HCC
(2001) 16 iCCA 62 39 5-year disease-free survival 57%
for patients with hCCA and 35% for
those with iCCA
Robles et al.(56) Spain Retrospective 36 hCCA 82 53 30 No 2-year disease-free survival
(2004) Multicenter 23 iCCA 77 65 42 52% for hCCA
and 35% for iCCA
Ghali et al.(60) Canada Retrospective 10 — 30 — No 1 patient had iCCA-HCC
(2005) Multicenter
Hong et al.(9) UCLA Retrospective 132 — 38 32 Yes LT for 25 iCCA
(2011) comparing LT for 13 hCCA
resection 3 LT 29% patients underwent LT
Panjala et al.(61) Mayo Retrospective 22 90 63 — Yes —
(2012)
Duignan et al.(19) Dublin Retrospective 27 73 73 61 (4 years) Yes 74% patients underwent LT.
(2014) Median time to recurrence
37 months
compared with HCC (hazard ratio, 1.1; 95% confi- series, patients with “very early” iCCA (2 cm) did
dence interval, 1.1-1.2) for patients with iCCA. not present tumor recurrence, and their longterm sur-
Unfortunately, only 2.2% of iCCA patients were vival at 5 years was 73%. Instead, patients with tumors
treated with LT, so it is difficult to extrapolate these >2 cm or with multifocal disease did much worse with
worse results to the transplant field.(65) a 40% 5-year survival. These promising results sug-
gested that patients with “very early” iCCA should
NEW INSIGHTS maybe be considered as a formal indication for LT.
However, the number of patients on that study was
In the last few years, efforts have been made to analyze limited, and their conclusions needed validation.(69)
homogeneous cohorts (Table 3). A multicenter study Hence, in 2016, Sapisochin et al. conducted a multi-
of LT centers in Spain published in 2014 their experi- center international study with the aim of validating
ence with LT for patients found to have iCCA and the previous findings. A total of 48 (59%) out of 81
mixed HCC-CCA in the explant pathology.(67) These patients with iCCA features at the explant pathology
results were compared with a control group of patients were found have only iCCA. Among them, 31% (15
transplanted for HCC. The OS was 50% at 5 years for patients) constituted the “very early” iCCA group.
those patients with exclusively iCCA. Interestingly, This group of patients was then compared with 33
this large series found tumor size (>2 cm) and multi- (69%) patients with “advanced” disease (single tumor
nodularity as risk factors for tumor recurrence and >2 cm or multifocal disease). The 5-year actuarial sur-
worse outcomes when compared with similar HCCs. vival rates were 65% in the “very early” iCCA group
On the other hand, patients with small single tumors versus 45% in the advanced group. The cumulative risk
had similar results to those of patients with HCC. Fol- of recurrence at 5 years was 18% versus 61%, respec-
lowing that study, the same Spanish consortium tively. These data support the previous findings that
reported a series of 29 patients who were found to have “very early” iCCA (2 cm) should formally be consid-
exclusively iCCA in their explant pathology. In this ered as candidates for LT.(8) Notably, all of these
298 | REVIEW ARTICLELIVER TRANSPLANTATION, Vol. 24, No. 2, 2018 GOLDARACENA, GORGEN, AND SAPISOCHIN
TABLE 3. Survival and Disease-Free Survival of Patients Transplanted With iCCA
Total 5-Year
Number of 1-Year 3-Year 5-Year Disease-Free
References Center Study Type Patients OS (%) OS (%) OS (%) Survival (%)
(63)
Sotiropoulos et al. Mainz Retrospective 10 70 50 33 —
(2008)
Vallin et al.(66) France Retrospective 10 80 60 24 —
(2013) Multicenter
Sapisochin et al.(67) Spain Retrospective 27 78 66 51 36
(2014) Multicenter
Facciuto et al.(64) Mont Sinai Retrospective 7 iCCA 71 — 57 44
(2015) Medical Center 9 iCCA1HCC
16 iCCA-HCC
Vilchez et al.(68) UNOS database Retrospective 440 79 58 47 —
(2016) Multicenter
Sapisochin et al.(8) Canada Retrospective 15 iCCA single 2 cm 93 84 65 18
(2016) Multicenter 33 iCCA multiple or > 2 cm 79 50 45 61
NOTE: All articles included patients without neoadjuvant chemoradiation.
studies were conducted in patients who were either Asian centers, arterial resection and reconstruction in
transplanted with the suspicion of HCC and were some cases of bilateral arterial involvement may be
found to have iCCA in the explant (misdiagnosis) or considered as an alternative to LT, and this treatment
underwent transplantation due to decompensated cir- strategy should be further investigated in the
rhosis and were incidentally diagnosed with an iCCA. future.(71)
Certainly, this is the main caveat of these encourag- For iCCA, the encouraging results from retrospec-
ing results, and the outcomes of patients with known tive studies opens a new door when considering LT
iCCA before transplant is still to be investigated and for patients with “very early” iCCA. Indeed, given
will need to be evaluated prospectively. Also, it is that the radiological features of iCCA (especially in
important to mention that the first treatment option cirrhosis) have yet to be established, a tumor biopsy in
for patients with iCCA should be liver resection if pos- patients considered for LT with a nodule without typ-
sible.(51) As with HCC, LT for early stages of iCCA ical HCC features will need to be performed. In this
should be reserved for patients where liver resection is regard, a prospective trial (NCT02878473)(72) aiming
not an option (ie, portal hypertension). All patients to transplant patients with “very early” iCCA will be
evaluated in previous studies analyzing LT for “very recruiting in the near future to prospectively confirm
early” iCCA only included patients who were not can- that these patients can benefit from this treatment
didates for liver resection.(8,56,69) and to open a new indication for LT. The main caveat
for such a protocol will be the difficulty of precisely
diagnosing these tumors in patients where a tumor
Future Perspectives biopsy cannot be performed. One of the unanswered
questions is if as with hCCA and the Mayo protocol,
Prospective trials should allow the identification of these patients will require neoadjuvant chemoradia-
hCCA patients who would benefit from either LT or tion. Also, it is unclear if by using chemoradiation
surgical resection. To answer this question, there is protocols LT could be offered to patients with a
currently 1 prospective, randomized, multicenter >2 cm iCCA. These unanswered questions will need
study (Liver Resection Versus Radio-Chemotherapy- to be studied in the near future to better understand
Transplantation for Hilar Cholangiocarcinoma and improve the management of patients with cirrho-
[TRANSPHILL] study NCT02232932) comparing sis diagnosed with CCA.
LT preceded by neoadjuvant radiochemotherapy ver- To date, available data on systemic therapy for
sus standard of care liver and bile duct resection. The CCA have demonstrated limited therapeutic efficacy.
primary outcome for this study is OS.(70) Hopefully Data from the Adjuvant capecitabine for biliary tract
in the future, we will have some insights if LT is a cancer (BILCAP) randomized trial, presented recently
better treatment than LR in resectable patients. On at the American Society of Clinical Oncology, showed
the other hand, due to encouraging results from some encouraging results of capecitabine as adjuvant therapy
REVIEW ARTICLE | 299GOLDARACENA, GORGEN, AND SAPISOCHIN LIVER TRANSPLANTATION, February 2018
after resection of biliary cancers. The OS in the capeci- these genomic classes will predict the outcomes of
tabine group was 15 months longer compared with iCCA after LT.
observation.(73) The applicability of this in the trans-
plant setting is unknown and probably difficult to
extrapolate, but it should be explored in the future
Conclusion
under research protocols aiming to increase the survival The era of “Transplant Oncology”(6) is happening now
of transplant recipients with CCA. and is likely to advance further in the next decade.
Certainly, target therapies in the context of LT for Selected patients with CCA can benefit from a radical
CCA will also need to be better assessed. Genetic treatment such as LT to achieve a cure. However, fur-
aberrations such as KRAS mutation, fibroblast growth ther research to better define inclusion criteria and
factor receptor 2 gene fusions, and somatic mutations neoadjuvant and adjuvant treatments is needed. The
in IDH1/2 are common in CAA and potentially can- hCCA should be an indication for LT under a strict
didates to targeted therapies.(74,75) In the same way, neoadjuvant chemoradiation protocol, and patients
vascular endothelial growth factor (VEGF) expression must be carefully followed while listed to identify
is reported in up to 40% of CCA.(76) However, the tumor progression and avoid posttransplant recurrence.
results with VEGF blockers in CCA are disappoint- Posttransplant analysis suggests patients with cirrhosis
ing. Although sorafenib failed to prove beneficial in with very early iCCA may achieve excellent OS. In
phase 2 studies, bevacizumab associated with gemcita- this regard, it is possible that patients diagnosed preop-
bine and oxaliplatin has shown a median progression- eratively of a “very early” iCCA may achieve the same
free survival of 7 months in a single-arm phase 2 results after LT. Further prospective research is needed
study.(77,78) Immune checkpoints have also been to confirm these encouraging results.
proven to be dysregulated in CCA resected tissue.(79)
However, the clinical experience in immunotherapy for
CCA is incipient with 2 phase 2 trials that are ongoing REFERENCES
(NCT02628067 and NCT02268825).(80,81) The 1) Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A,
results of these trials will hopefully provide a better Bozzetti F, et al. Liver transplantation for the treatment of small
hepatocellular carcinomas in patients with cirrhosis. N Engl J
understanding of the role of these new therapies in
Med 1996;334:693-699.
patients with CCA. 2) Eghtesad B, Aucejo F. Liver transplantation for malignancies.
Another possible consideration is if genomic fea- J Gastrointest Cancer 2014;45:353-362.
tures can play a role in identifying adequate candi- 3) Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet
2012;379:1245-1255.
dates with iCCA for LT. Recent studies have 4) Sapisochin G, Bruix J. Liver transplantation for hepatocellular
identified messenger RNA and noncoding RNA carcinoma: outcomes and novel surgical approaches. Nat Rev
expression associated with iCCA outcomes. Sia et al. Gastroenterol Hepatol 2017;14:203-217.
5) Clavien PA, Lesurtel M, Bossuyt PM, Gores GJ, Langer B,
analyzed the gene expression profile using samples of Perrier A; for OLT for HCC Consensus Group. Recommenda-
149 patients and identified 2 main biological classes tions for liver transplantation for hepatocellular carcinoma: an
of iCCA: international consensus conference report. Lancet Oncol 2012;13:
e11-22.
1. The inflammation class, characterized by activa- 6) Hibi T, Itano O, Shinoda M, Kitagawa Y. Liver transplantation
tion of inflammatory signaling pathways, overex- for hepatobiliary malignancies: a new era of “Transplant
Oncology” has begun. Surg Today 2017;47:403-415.
pression of cytokines, and signal transducer and 7) Hagness M, Foss A, Line PD, Scholz T, Jørgensen PF, Fosby
activator of transcription 3 (STAT3) oncogene B, et al. Liver transplantation for nonresectable liver metastases
activation. from colorectal cancer. Ann Surg 2013;257:800-806.
8) Sapisochin G, Facciuto M, Rubbia-Brandt L, Marti J, Mehta N,
2. The proliferation class characterized by activation Yao FY, et al.; for iCCA International Consortium. Liver trans-
of oncogenic signaling pathways (including RAS, plantation for “very early” intrahepatic cholangiocarcinoma: inter-
mitogen-activated protein kinase, and MET), national retrospective study supporting a prospective assessment.
DNA amplifications at 11q13.2, deletions at Hepatology 2016;64:1178-1188.
9) Hong JC, Jones CM, Duffy JP, Petrowsky H, Farmer DG,
14q22.1, mutations in KRAS and BRAF, and French S, et al. Comparative analysis of resection and liver trans-
gene expression signatures previously associated plantation for intrahepatic and hilar cholangiocarcinoma: a 24-
with poor outcomes for patients with HCC.(82) year experience in a single center. Arch Surg 2011;146:683-689.
10) Rea DJ, Heimbach JK, Rosen CB, Haddock MG, Alberts SR,
Unfortunately, there is still limited understanding of Kremers WK, et al. Liver transplantation with neoadjuvant
genomics abnormalities in iCCA, and it is unclear if
300 | REVIEW ARTICLELIVER TRANSPLANTATION, Vol. 24, No. 2, 2018 GOLDARACENA, GORGEN, AND SAPISOCHIN
chemoradiation is more effective than resection for hilar cholan- one-year experience with 564 patients at a single institution. Ann
giocarcinoma. Ann Surg 2005;242:451-458. Surg 2007;245:755-762.
11) Mazzaferro V. Squaring the circle of selection and allocation in 29) Kimura N, Young AL, Toyoki Y, Wyatt JI, Toogood GJ,
liver transplantation for HCC: an adaptive approach. Hepatology Hidalgo E, et al. Radical operation for hilar cholangiocarcinoma
2016;63:1707-1717. in comparable Eastern and Western centers: outcome analysis
12) Belli LS, Berenguer M, Cortesi PA, Strazzabosco M, and prognostic factors. Surgery 2017;162:500-514.
Rockenschaub SR, Martini S, et al.; for European Liver and 30) Hasegawa S, Ikai I, Fujii H, Hatano E, Shimahara Y. Surgical
Intestine Association (ELITA). Delisting of liver transplant can- resection of hilar cholangiocarcinoma: analysis of survival and
didates with chronic hepatitis C after viral eradication: a Euro- postoperative complications. World J Surg 2007;31:1256-1263.
pean study. J Hepatol 2016;65:524-531. 31) Groot Koerkamp B, Wiggers JK, Gonen M, Doussot A, Allen
13) Parikh ND, Marrero WJ, Wang J, Steuer J, Tapper EB, PJ, Besselink MG, et al. Survival after resection of perihilar
Konerman M, et al. Projected increase in obesity and non- cholangiocarcinoma-development and external validation of a
alcoholic steatohepatitis-related liver transplantation waitlist addi- prognostic nomogram. Ann Oncol 2015;26:1930-1935.
tions in the United States. Hepatology 2017;doi: 10.1002/ 32) Klempnauer J, Ridder GJ, von Wasielewski R, Werner M,
hep.29473. Weimann A, Pichlmayr R. Resectional surgery of hilar cholan-
14) Robles R, Sanchez-Bueno F, Ramırez P, Brusadin R, Parrilla P. giocarcinoma: a multivariate analysis of prognostic factors. J Clin
Liver transplantation for hilar cholangiocarcinoma. World J Gas- Oncol 1997;15:947-954.
troenterol 2013;19:9209-9215. 33) Pichlmayr R, Weimann A, Tusch G, Schlitt HJ. Indications and
15) Razumilava N, Gores GJ. Cholangiocarcinoma. Lancet 2014; role of liver transplantation for malignant tumors. Oncologist
383:2168-2179. 1997;2:164-170.
16) Gu J, Bai J, Shi X, Zhou J, Qiu Y, Wu Y, et al. Efficacy and 34) Iwatsuki S, Todo S, Marsh JW, Madariaga JR, Lee RG,
safety of liver transplantation in patients with cholangiocarci- Dvorchik I, et al. Treatment of hilar cholangiocarcinoma (Klat-
noma: a systematic review and meta-analysis. Int J Cancer 2012; skin tumors) with hepatic resection or transplantation. J Am Coll
130:2155-2163. Surg 1998;187:358-364.
17) Sia D, Villanueva A, Friedman SL, Llovet JM. Liver cancer cell 35) Heimbach JK, Gores GJ, Haddock MG, Alberts SR, Nyberg SL,
of origin, molecular class, and effects on patient prognosis. Gas- Ishitani MB, Rosen CB. Liver transplantation for unresectable
troenterology 2017;152:745-761. perihilar cholangiocarcinoma. Semin Liver Dis 2004;24:201-207.
18) Sudan D, DeRoover A, Chinnakotla S, Fox I, Shaw B Jr, 36) Rosen CB, Heimbach JK, Gores GJ. Surgery for cholangiocarci-
McCashland T, et al. Radiochemotherapy and transplantation noma: the role of liver transplantation. HPB (Oxford) 2008;10:
allow long-term survival for nonresectable hilar cholangiocarci- 186-189.
noma. Am J Transplant 2002;2:774-779. 37) Kaiser GM, Sotiropoulos GC, Jauch KW, L€ohe F, Hirner A,
19) Duignan S, Maguire D, Ravichand CS, Geoghegan J, Hoti E, Kalff JC, et al. Liver transplantation for hilar cholangiocarci-
Fennelly D, et al. Neoadjuvant chemoradiotherapy followed by noma: a German survey. Transplant Proc 2008;40:3191-3193.
liver transplantation for unresectable cholangiocarcinoma: a 38) Darwish Murad S, Kim WR, Harnois DM, Douglas DD,
single-centre national experience. HPB (Oxford) 2014;16:91-98. Burton J, Kulik LM, et al. Efficacy of neoadjuvant chemoradia-
20) Welling TH, Feng M, Wan S, Hwang SY, Volk ML, Lawrence tion, followed by liver transplantation, for perihilar cholangiocar-
TS, et al. Neoadjuvant stereotactic body radiation therapy, cape- cinoma at 12 US centers. Gastroenterology 2012;143:88-98.
citabine, and liver transplantation for unresectable hilar cholan- 39) Marchan EM, Landry JC. Neoadjuvant chemoradiation followed
giocarcinoma. Liver Transpl 2014;20:81-88. by orthotopic liver transplantation in cholangiocarcinomas: the
21) Hassoun Z, Gores GJ, Rosen CB. Preliminary experience with emory experience. J Gastrointest Oncol 2016;7:248-254.
liver transplantation in selected patients with unresectable hilar 40) Mantel HT, Westerkamp AC, Adam R, Bennet WF, Seehofer
cholangiocarcinoma. Surg Oncol Clin N Am 2002;11:909-921. D, Settmacher U, et al.; for European Liver and Intestine Trans-
22) Bergquist A, von Seth E. Epidemiology of cholangiocarcinoma. plant Association (ELITA). Strict selection alone of patients
Best Pract Res Clin Gastroenterol 2015;29:221-232. undergoing liver transplantation for hilar cholangiocarcinoma is
23) Razumilava N, Gores GJ. Classification, diagnosis, and manage- associated with improved survival. PLoS One 2016;11:e0156127.
ment of cholangiocarcinoma. Clin Gastroenterol Hepatol 2013; 41) De Vreede I, Steers JL, Burch PA, Rosen CB, Gunderson LL,
11:13-21. Haddock MG, et al. Prolonged disease-free survival after ortho-
24) Oliveira IS, Kilcoyne A, Everett JM, Mino-Kenudson M, topic liver transplantation plus adjuvant chemoirradiation for
Harisinghani MG, Ganesan K. Cholangiocarcinoma: classifica- cholangiocarcinoma. Liver Transpl 2000;6:309-316.
tion, diagnosis, staging, imaging features, and management. 42) Gores GJ, Darwish Murad S, Heimbach JK, Rosen CB. Liver
Abdom Radiol (NY) 2017;42:1637-1649. transplantation for perihilar cholangiocarcinoma. Dig Dis 2013;
25) Mansour JC, Aloia TA, Crane CH, Heimbach JK, Nagino M, 31:126-129.
Vauthey JN. Hilar cholangiocarcinoma: expert consensus state- 43) Darwish Murad S, Kim WR, Therneau T, Gores GJ, Rosen
ment. HPB (Oxford) 2015;17:691-699. CB, Martenson JA, et al. Predictors of pretransplant dropout
26) Hu HJ, Mao H, Shrestha A, Tan YQ, Ma WJ, Yang Q, et al. and posttransplant recurrence in patients with perihilar cholan-
Prognostic factors and long-term outcomes of hilar cholangiocar- giocarcinoma. Hepatology 2012;56:972-981.
cinoma: a single-institution experience in China. World J Gas- 44) Gores GJ, Gish RG, Sudan D, Rosen CB; for MELD Excep-
troenterol 2016;22:2601-2610. tion Study Group. Model for end-stage liver disease (MELD)
27) Jarnagin WR, Fong Y, DeMatteo RP, Gonen M, Burke EC, exception for cholangiocarcinoma or biliary dysplasia. Liver
Bodniewicz BS J, et al. Staging, resectability, and outcome in Transpl 2006;12(suppl 3):S95-S97.
225 patients with hilar cholangiocarcinoma. Ann Surg 2001;234: 45) Kaiser GM, Sotiropoulos GC, Sgourakis G, Bleck J, Baba HA,
507-517. Beckebaumr Sn, et al. Surgical treatment of Klatskin tumor: liver
28) DeOliveira ML, Cunningham SC, Cameron JL, Kamangar F, resection versus transplantation. Hepatogastroenterology 2010;57:
Winter JM, Lillemoe KD, et al. Cholangiocarcinoma: thirty- 1337-1340.
REVIEW ARTICLE | 301GOLDARACENA, GORGEN, AND SAPISOCHIN LIVER TRANSPLANTATION, February 2018
46) Hong JC, Kaldas FM, Kositamongkol P, Petrowsky H, Farmer 65) Bergquist JR, Groeschl RT, Ivanics T, Shubert CR, Habermann
DG, Markovic D, et al. Predictive index for long-term survival after EB, Kendrick ML, et al. Mixed hepatocellular and cholangiocar-
retransplantation of the liver in adult recipients: analysis of a 26- cinoma: a rare tumor with a mix of parent phenotypic character-
year experience in a single center. Ann Surg 2011;254:444-448. istics. HPB (Oxford) 2016;18:886-892.
47) Gupta A, Dixon E. Epidemiology and risk factors: intrahepatic 66) Vallin M, Sturm N, Lamblin G, Guillaud O, Hilleret MN,
cholangiocarcinoma. Hepatobiliary Surg Nutr 2017;6:101-104. Hervieu V, et al. Unrecognized intrahepatic cholangiocarcinoma:
48) Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. an analysis of 993 adult cirrhotic liver explants. Clin Transplant
Semin Liver Dis 2004;24:115-125. 2013;27:403-409.
49) Ariizumi S, Yamamoto M. Intrahepatic cholangiocarcinoma and 67) Sapisochin G, de Lope CR, Gastaca M, de Urbina JO, Lopez-
cholangiolocellular carcinoma in cirrhosis and chronic viral hepa- Andujar R, Palacios F, et al. Intrahepatic cholangiocarcinoma or
titis. Surg Today 2015;45:682-687. mixed hepatocellular-cholangiocarcinoma in patients undergoing
50) Palmer WC, Patel T. Are common factors involved in the path- liver transplantation: a Spanish matched cohort multicenter study.
ogenesis of primary liver cancers? a meta-analysis of risk factors Ann Surg 2014;259:944-952.
for intrahepatic cholangiocarcinoma. J Hepatol 2012;57:69-76. 68) Vilchez V, Shah MB, Daily MF, Pena L, Tzeng CW,
51) Bridgewater J, Galle PR, Khan SA, Llovet JM, Park JW, Patel Davenport D, et al. Long-term outcome of patients undergoing
T, et al. Guidelines for the diagnosis and management of intra- liver transplantation for mixed hepatocellular carcinoma and chol-
hepatic cholangiocarcinoma. J Hepatol 2014;60:1268-1289. angiocarcinoma: an analysis of the UNOS database. HPB
52) O’Grady JG, Polson RJ, Rolles K, Calne RY, Williams R. Liver (Oxford) 2016;18:29-34.
transplantation for malignant disease. results in 93 consecutive 69) Sapisochin G, Rodrıguez de Lope C, Gastaca M, Ortiz de
patients. Ann Surg 1988;207:373-379. Urbina J, Suarez MA, Santoyo J, et al. “Very early” intrahepatic
53) Ringe B, Wittekind C, Bechstein WO, Bunzendahl H, cholangiocarcinoma in cirrhotic patients: should liver transplanta-
Pichlmayr R. The role of liver transplantation in hepatobiliary tion be reconsidered in these patients? Am J Transplant 2014;14:
malignancy. a retrospective analysis of 95 patients with particular 660-667.
regard to tumor stage and recurrence. Ann Surg 1989;209:88-98. 70) Vimbert E. Randomized prospective multicentric study: radio-
54) Goldstein RM, Stone M, Tillery GW, Senzer N, Levy M, chemotherapy and liver transplantation versus liver resection to
Husberg BS, et al. Is liver transplantation indicated for cholan- treat respectable hilar cholangiocarcinoma. https://clinicaltrials.gov/
giocarcinoma? Am J Surg 1993;166:768-771. ct2/show/NCT02232932?term=TRANSPHIL&rank=1. Accessed
55) Wu ZF, Wu XY, Zhu N, Xu Z, Li WS, Zhang HB, et al. Prognosis November 14, 2017.
after resection for hepatitis B virus-associated intrahepatic cholan- 71) Matsuyama R, Mori R, Ota Y, Homma Y, Kumamoto T,
giocarcinoma. World J Gastroenterol 2015;21:935-943. Takeda K, et al. Significance of vascular resection and reconstruc-
56) Robles R, Figueras J, Turrion VS, Margarit C, Moya A, Varo E, tion in surgery for hilar cholangiocarcinoma: with special refer-
et al. Spanish experience in liver transplantation for hilar and ence to hepatic arterial resection and reconstruction. Ann Surg
peripheral cholangiocarcinoma. Ann Surg 2004;239:265-271. Oncol 2016;23(suppl 4):475-484.
57) Yokoyama I, Todo S, Iwatsuki S, Starzl TE. Liver transplanta- 72) Sapisochin G. Liver transplantation for early intrahepatic cholangio-
tion in the treatment of primary liver cancer. Hepatogastroenter- carcinoma. https://clinicaltrials.gov/ct2/show/NCT02878473?term=
ology 1990;37:188-193. sapisochin&rank=3. Accessed November 14, 2017.
58) Meyer CG, Penn I, James L. Liver transplantation for cholan- 73) Primrose JN, Fox R, Palmer DH, Prasad R, Mirza D,
giocarcinoma: results in 207 patients. Transplantation 2000;69: Anthoney DA, et al. Adjuvant capecitabine for biliary tract can-
1633-1637. cer: The BILCAP randomized study. J Clin Oncol 2017;
59) Shimoda M, Farmer DG, Colquhoun SD, Rosove M, Ghobrial 35(suppl):4006.
RM, Yersiz H, et al. Liver transplantation for cholangiocellular 74) Rizvi S, Gores GJ. Emerging molecular therapeutic targets for
carcinoma: analysis of a single-center experience and review of cholangiocarcinoma. J Hepatol 2017;67:632-644.
the literature. Liver Transpl 2001;7:1023-1033. 75) Kayhanian H, Smyth EC, Braconi C. Emerging molecular tar-
60) Ghali P, Marotta PJ, Yoshida EM, Bain VG, Marleau D, gets and therapy for cholangiocarcinoma. World J Gastrointest
Peltekian K, et al. Liver transplantation for incidental cholangio- Oncol 2017;9:268-280.
carcinoma: analysis of the Canadian experience. Liver Transpl 76) Park KW, Kim SJ, Oh SY. Clinicopathologic significance of
2005;11:1412-1416. nuclear factor-jB and vascular endothelial growth factor expres-
61) Panjala C, Nguyen JH, Al-Hajjaj AN, Rosser BA, Nakhleh RE, sion in advanced gastric cancer patients. Oncol Res Treat 2014;
Bridges MD, et al. Impact of neoadjuvant chemoradiation on the 37:183-190.
tumor burden before liver transplantation for unresectable cholan- 77) Zhu AX, Meyerhardt JA, Blaszkowsky LS, Kambadakone AR,
giocarcinoma. Liver Transpl 2012;18:594-601. Muzikansky A, Zheng H, et al. Efficacy and safety of gemcita-
62) Sapisochin G, Fidelman N, Roberts JP, Yao FY. Mixed hepato- bine, oxaliplatin, and bevacizumab in advanced biliary-tract can-
cellular cholangiocarcinoma and intrahepatic cholangiocarcinoma cers and correlation of changes in 18-fluorodeoxyglucose PET
in patients undergoing transplantation for hepatocellular carci- with clinical outcome: a phase 2 study. Lancet Oncol 2010;11:
noma. Liver Transpl 2011;17:934-942. 48-54.
63) Sotiropoulos GC, Kaiser GM, Lang H, Molmenti EP, 78) El-Khoueiry AB, Rankin C, Siegel AB, Iqbal S, Gong IY,
Beckebaum S, Fouzas I, et al. Liver transplantation as a primary Micetich KC, et al. S0941: a phase 2 SWOG study of sora-
indication for intrahepatic cholangiocarcinoma: a single-center fenib and erlotinib in patients with advanced gallbladder car-
experience. Transplant Proc 2008;40:3194-3195. cinoma or cholangiocarcinoma. Br J Cancer 2014;110:882-
64) Facciuto ME, Singh MK, Lubezky N, Selim MA, Robinson D, 887.
Kim-Schluger L, et al. Tumors with intrahepatic bile duct differ- 79) Nakamura H, Arai Y, Totoki Y, Shirota T, Elzawahry A, Kato
entiation in cirrhosis: implications on outcomes after liver trans- M, et al. Genomic spectra of biliary tract cancer. Nat Genet
plantation. Transplantation 2015;99:151-157. 2015;47:1003-1010.
302 | REVIEW ARTICLELIVER TRANSPLANTATION, Vol. 24, No. 2, 2018 GOLDARACENA, GORGEN, AND SAPISOCHIN
80) Merck Sharp and Dohme Corp. Study of pembrolizumab (MK- GI cancers (MK-3475 GI). https://clinicaltrials.gov/ct2/show/
3475) in participants with advanced solid tumors (MK-3475-158/ NCT02268825?term=NCT&rank=1. Accessed November 14, 2017
KEYNOTE-158). https://clinicaltrials.gov/ct2/show/NCT02628067? 82) Sia D, Hoshida Y, Villanueva A, Roayaie S, Ferrer J, Tabak B,
term=NCT&rank=1. Accessed November 14, 2017. et al. Integrative molecular analysis of intrahepatic cholangiocarci-
81) University of Utah. Phase I Study of MK-3475 in combination with noma reveals 2 classes that have different outcomes. Gastroenter-
chemotherapy and supplemental celecoxib in patients with advanced ology 2013;144:829-840.
REVIEW ARTICLE | 303GASTROENTEROLOGY ARTICLE OF THE WEEK
September 13, 2018
Goldaracena N, Gorgen A, Sapisochin G. Current status of liver transplantation for
cholangiocarcinoma. Liver Transplantation 2018;24:294‐303.
1. Patients with CCA that are likely to have a poor prognosis include
a. CA19‐9 > 500 U/mL
b. Mass >2cm
c. MELD >20
d. Malignancy found on brushing or biopsy
True of False
2. Patients with PSC and hilar cholangiocarcinoma are not eligible for liver transplantation
3. Intrahepatic CCA has a better prognosis after resection than HCC
4. Sorafenib, an effective treatment for HCC appears promising in iCCA
5. Very early iCCA (2cm in diameter and multinodularity are risk factors for poor prognosis after
transplant
9. The first choice of therapy for patients with iCCA should be resection
10. The prevalence of iCAA is increasing due to an increase in PSC casesYou can also read