CLIMATIC HAZARDS, HEALTH RISK AND RESPONSE CASE STUDY 3: CHIHUAHUA, MEXICO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research Report
CLIMATIC HAZARDS, HEALTH RISK
AND RESPONSE
CASE STUDY 3: CHIHUAHUA, MEXICO
January 2008
Teresa E. Cueva-Luna
El Colegio de la Frontera Norte, Matamoros Tamaulipas, Mexico
Roger Few
School of Development Studies, University of East Anglia (UEA), Norwich, UK
Alfonso Mercado, Boris Graizbord
El Colegio de Mexico, Mexico City
A research programme funded by
UK Economic and Social Research CouncilContents
1 Introduction 2
2 Methods 4
3 Study sites 10
4 Health impacts of climatic hazards: perceptions of risk 24
5 Risk factors and responses to health risks 32
6 Synthesis 46
Appendix 1: National organizations consulted in the Mexico studies 56
Appendix 2: Secondary sources consulted in the Mexico studies 57
Please reference this report as:
Cueva-Luna, T. E., Few, R., Mercado, A. and Graizbord, B. (2008). ‘Climatic
hazards, health risk and response. Case study 3: Chihuahua, Mexico.’
Research report, University of East Anglia, Norwich, UK.
11 Introduction
This document reports on a research project carried out in the Sierra Tarahumara of
south-west Chihuahua from December 2006 - April 2007, as part of an international
research programme on preparedness and response to the health risks that result from
weather extremes. The project is a collaboration between: the Overseas Development
Group/School of Development Studies, University of East Anglia (UEA), UK; El Colegio
de Mexico, Mexico City; and El Colegio de la Frontera Norte, Matamoros Tamaulipas,
Mexico. It is funded by the UK Economic and Social Research Council (ESRC).
The project entails primarily qualitative research on perceptions of health risk and
analysis of household coping mechanisms, with a spatial focus on three communities in
different zones of the Sierra region: San Jose del Pinal/El Durazno, Choguita/Capochi
and Wacareachi. The household-level research was complemented by interviews with
local key informants, as well as state-level and national-level investigation and collation
of secondary data.
The project is one of two field studies in Mexico, the second taking place in Yucatan
where the focus is on health sector response to risks from tropical cyclones and other
hazards. The overall research programme also includes institutional and household level
research projects in Vietnam, another highly hazard-prone country. Though funding
limitations mean that all these studies are relatively small-scale, they provide a first
opportunity to target research on this theme.
Rationale for the research
Different climatic hazards (flood, drought, thermal extremes and storm events) affect
most regions of the globe and in many their impacts are likely to be exacerbated by the
effects of climate change. The prospect of changes in the extent, magnitude and
distribution of climatic hazards compounds an already severe socio-environmental
problem in many regions, especially in developing countries where the state’s capacity
to provide widespread protection measures is often limited and where poverty and
vulnerability to hazards may have a cyclical relationship. Vulnerability to hazard is now
broadly recognized as a function not just of physical environment but, crucially, of social
and political context. A key component of this social dimension is resilience: the
capability of reducing risks through coping strategies and adaptive behaviour. This, in
turn, is shaped by differential access and entitlement to economic, social and political
resources.
One of the most complex and widespread impacts of hazards is on health. Climatic
hazards bring both short and long term, direct and indirect health risks, including
accident and injury, psychosocial disturbance, changes in exposure to vectors and
pathogens, impacts on food supply and impacts on health care services. These risks are
especially evident in lower-income settings, where mortality and morbidity outcomes are
often concentrated among the poor and marginalized. Yet health aspects of hazards
tend to be under-researched and, other than short-term deaths and injury, under-
reported.
2Though much remains to be achieved, research on the potential public health impacts of
climate change is now gaining momentum, through a combination of epidemiological
research on current hazards and geographical modelling of changes in disease burden
and hazard occurrence. Yet there is at present very little work analyzing response to
health risks by people and institutions, and in particular the constraints and opportunities
that shape capacity to adapt to the health challenges.
Mexico is among the most hazard-prone countries of the world, facing annual risks from
tropical cyclones (storms and hurricanes), floods, droughts and other weather-related
hazards such as coldwaves, heatwaves and forest fires. Our review of previous research
in Mexico suggests there has been little work to date on perceptions and coping
strategies relating to the health risks from weather extremes. The study reported in this
document continues the process of addressing that important research gap.
32 Methods
The principal data collection method was semi-structured interviews with households.
This was complemented by group interviews and interviews with local and state-level
key informant. Background inputs to the research also included national-level interviews
(with governmental institutions, health care providers, non-governmental organizations
and academics), and secondary data (studies, reports, papers, policy documents) –
these are listed in the Appendices.
Field research in the Sierra Tarahumara is challenging for a number of reasons (difficult
terrain and transportation, physical remoteness, social access to communities and
households, language and cultural barriers), and this was reflected in the progress of the
data collection and the mix of methods used with households. In practice, data collection
to large extent had to be opportunistic: reliant on occasions when social access to
households was possible, and responsive to what was feasible within the fieldwork time
constraints. The approach was to establish planned targets for data collection and then
make the best use of opportunities that could be arranged to meet those targets.
Interview notes from households and key informants were annotated through a system
of open coding. Compiling and comparing these different coded sources enabled the
researchers to build qualitative insights into the process of vulnerability and response to
health risks. Further insights and opportunities for triangulation of data were obtained by
cross-reference with secondary data sources.
Household interviews
Interviews were conducted with a total of 31 households across the three study sites: 15
in the village of El Durazno in San Jose del Pinal (plus two shorter discussions); 10 in
Wacareachi; and 6 in the village of Capochi in Choguita. The initial target for the
research was to conduct an equal number of interviews in the sites, but for reasons of
access the work in Choguita had to be curtailed and an additional set of households was
selected in the final site visited (San Jose del Pinal). In consultation with local key
informants, the field researcher (Dr Cueva-Luna) then sketched maps of the sites, with
an indication of household locations. She then randomly selected households to visit,
with an element of purposive sampling to ensure sufficient respondents were selected
from different sections of each site. If a household member was unavailable on either of
two occasions a replacement household was selected.
Interviews were conducted with one or more adult representatives of each household
(both men and women) at the homes of the interviewees. In total, the interviews included
19 women and 20 men, although the gender mix from location to location was quite
different, depending on the circumstances and timing of access to households (see also
section on Group Interviews below). Table 1 provides a breakdown of the household
interviews completed for each site, together with codenames. In the chapters that follow,
references to interview material are provided using these codenames. Actual names of
interviewees have not been used in the report, in order to preserve the anonymity of
respondents.
4Table 1 Household interviews
site description interview codename
San Jose del Pinal 1 man Sjp1
1 woman Sjp2
1 woman Sjp3
1 man Sjp4
1 woman and 1 man Sjp5
1 man Sjp6
1 man Sjp7
1 woman and 1 man Sjp8
1 man Sjp9
1 man Sjp10
1 man Sjp11
1 man Sjp12
1 man Sjp13
1 man Sjp14
1 man Sjp15
Wacareachi 1 woman and 1 man Wac1
1 man Wac2
1 woman Wac3
1 woman Wac4
1 woman Wac5
1 woman Wac6
1 woman Wac7
1 woman Wac8
1 woman Wac9
1 man Wac10
Choguita 2 women Cho1
1 woman Cho2
2 women and 2 men Cho3
1 woman Cho4
1 man Cho5
1 woman and 1 man Cho6
All interviews were semi-structured, guided by a flexible question schedule, designed to
elicit qualitative information on interviewees’ perceptions of climatic hazards and
attendant health risks and information about the forms of coping response at both
household and communal level. The question schedule was based on the following list
(initially devised in English, revised in Spanish and then back-translated):
1) Describa como afectan a esta comunidad el clima extremo: sequías (periodos
prolongados de falta de lluvia y nieve), o fríos extremos en el invierno, calores extremos,
incendios forestales.
1a) ¿Cómo han cambiado estos problemas del clima en el tiempo en que usted
guarda memoria?
1b) ¿Ha cambiado su estilo de vida (rutinas diarias) por esa razón? En qué y cómo?
51) Describe how extreme climatic conditions can affect this community: e.g. droughts
(prolonged periods of lack of rain and snow), extreme cold in the winter, extreme heat,
forest fires.
1a) How have they these problems of the climate changed within your living
memory?
1b) Has your way of life changed (daily routines) for that reason? What and how?
2) ¿Cuáles son los principales riesgos para la salud de la gente en la comunidad
debido a estos fenómenos naturales y como han ocurrido? (ej. Escasez de agua para
beber, lavarse y bañarse, contacto con agua contaminada, enfermedades transmitidas
por insectos, enfermedades respiratorias, estrés, desnutrición).
2a) ¿Cuáles son los riesgos más serios?
2b) ¿Podría dar un ejemplo de un riesgo serio? ¿Una experiencia de algún miembro
de su familia o de algún conocido?
2) Which are the main risks for the health of the people in the community due to these
natural phenomena and how have they occurred? (e.g. Shortage of water for drinking,
washing and bathing, contact with contaminated water, illnesses transmitted by insects,
respiratory illnesses, stress, malnutrition).
2a) Which are the most serious risks?
2b) Can you give an example of a serious risk? An experience of some member of
your family or of some acquaintance?
3) ¿Quienes son los más afectados por estos problemas, los que más sufren en esta
comunidad y porqué?
3) Who are most affected by these problems, the ones that suffer most in this community,
and why?
4) ¿Qué hace usted para prevenir enfermedades o riesgos a la salud ocasionados por
estos fenómenos naturales?
4a) ¿Qué se ha hecho en su familia? ¿Qué se ha hecho en la comunidad? Identificar
quienes lo han hecho.
4) What do you do to prevent illnesses or risks to health caused by these natural
phenomena?
4a) ¿What has your family done? What has been done in the community? Identify
who has done this.
5) Cuando hay una enfermedad en su hogar ocasionada por estos fenómenos, ¿qué
hace usted para afrontarlo, para encontrar un tratamiento y una cura?
5a) ¿Qué es lo que hace la comunidad en estos casos?
5) When there is an illness in your home caused by these phenomena, what do you do to
confront it, to find a treatment and a cure?
5a) ¿What does the community do in these cases?
6) ¿Qué le gustaría hacer para proteger más su salud ante estos fenómenos?
6) What would you like to do more to protect health against these phenomena?
7) ¿Porqué usted no ha podido hacer esto hasta ahora? ¿Que es lo que se lo impide
(barreras)?
7) Why you have not been able to do this up to now? What is it that stops you (barriers)?
8) ¿Qué ayuda ha conseguido usted de parte de los servicios de salud (privados /
públicos / ONGs) para afrontar de la mejor manera estos problemas? (Por ejemplo,
conocer mejor los riesgos, prevenir contagios, tener acceso a medicamentos o
tratamientos)
68) What help have you obtained from the health services (private / public / NGOs) to
confront these problems in a better way? (For example, to know the risks better, to
prevent contagion, to have access to medicines or treatment)
9) ¿Cuál cree que seria la forma mas importante para mejorar la protección de la salud
ante estos riesgos en la comunidad?
9a) En este sentido, ¿cuales son las prioridades para el futuro?
9) What do you believe would be the most important way to improve protection of health
against these risks in the community?
9a) In this sense, what are the priorities for the future?
Most interviews were conducted in the indigenous language with the aid of a translator,
although some were possible for the researcher to conduct directly in Spanish. The
interview method was piloted and refined during initial investigations in the field.
Interview notes were subsequently translated into English.
Group interviews
In addition to the individual household interviews, a total of 5 group interviews also took
place with local people in the study areas. One of these was organized opportunistically
(ChoGr1), when the fieldworker encountered a group of men waiting for a meeting at the
mission in Choguita. The remaining 4 group interviews were pre-planned, in order both
to maximize access to certain social groups in the sites that had been hard to reach
during first rounds of interviewing (especially women in El Durazno and men in
Wacareachi), and as an alternative interview method to help elicit responses via the
different question/answer dynamics in action within during a group setting. Table 2 lists
these meetings.
Table 2 Group interviews
site description codename
San Jose del Pinal Assistants in local PESA programmes + SjpGr1
SJdP governor, SJdP police chief (10 men)
San Jose del Pinal Women of El Durazno (11 women) SjpGr2
Wacareachi Men of Wacareachi (6 men) WacGr
Choguita Assistants in mission activities (6 men) ChoGr1
Choguita Indigenous health promoters (6 women, 1 ChoGr2
man)
Questions posed to groups were based on similar themes as to those covered in
household interviews. In one case (SjpGr2), a group interview with women followed a
specially devised format, intended to increase women’s willingness to discuss potential
health problems by using a depersonalized vignette (story-telling) approach (see Box 1).
Assistance in facilitating the group interviews was provided by local key informants.
7Box 1 Format of group interview with women of El Durazno
Following a round of household interviews in the village of El Durazno, it was
decided to host a further group interview with women from the village. The
interview took place at the community’s meeting place on a hilltop site within the
valley, where villagers were already assembling for a traditional fiesta that was
due to take place that night. During the preparations for the fiesta 11 women of
varying ages were asked to gather in a group at the edge of the meeting place.
Some women had children with them.
As a method to help the women talk about health issues associated with
weather-related hazards, they were first told the beginning of a storyline and then
were asked to continue constructing it through subsequent questions. The initial
storyline ran as follows:
There is a woman, Maria, who lives with her husband and his children. It is a dry
year, in April. She is very young and she has two children. The older one is 3
years old. The second is a year old.
1. The older boy becomes ill. He is crying. He says that his belly hurts.
2. The boy begins to have fever.
3. The boy is sleepy. Now his diarrhea has a little blood.
At each stage 1-3, the women were asked about the mother’s concerns and how
she and the father react to the child’s illness. They were then asked questions
about causes, prevention and treatment based on the following:
Why did the boy become ill? Remember that it is the month of April, dry. What
was the water he drank like? Where did he drink it from?
Is there something that you can make to avoid the diarrhea? Do they do it?
Would it be good doing what the promoter-the mothers says on washing the
hands, plates, boiling the water? Do people do it?
Which is the best way to take care of the children so that they do not become ill?
The method was quite effective in allowing women to articulate issues and
provided useful perspectives, although several of those in the group remained
reluctant to contribute despite careful efforts to coax them into participating. In
hindsight, it may have been most effective as a research tool to have the
storyline exploration of ideas as a group held first, and then to have followed this
up with household interviews to capture individual experiences (once the group
interview had sensitized people to issues/approach).
Key informant interviews
The third main element of primary data collection was a series of semi-structured
interviews with local and state-level key informants. These interviews followed a similar
procedure as those at the household level, but with a modifiable question schedule
designed to develop an understanding of local hazard, health risk, socio-economic and
8policy contexts, with question themes tailored to the expertise and role of the
interviewee. These meetings took place at each of the three sites, at nearby urban
centres in the Sierra Tarahumara, and within the state capital of Chihuahua City.
Table 3 gives a breakdown by scale and sector for the 13 interviews (18 people in all)
that provided input to the study (NB as already noted, names of the interviewees and
details of their staff positions are not disclosed in this report). Some of the interviews
were group meetings with two or more informants.
Table 3 Key informant interviews
level institution/sector/location codename
Chihuahua 2 (4 people) Junta Central de Agua y Sanamiento Ki1, Ki6
state (water/sanitation sector) Chihuahua City
1 (3 people) Instituto Chihuahuense de Salud (health Ki7
sector) Chihuahua City
2 Centro de Desarrollo Alternativo Indígena CEDAIN Ki5, Ki8
(development NGO) Chihuahua City
1 (2 people) Centro de Investigacion Sobre Sequia, Ki2
Instituto de Ecologia (research institute) Ciudad Aldama
Field sites and 1 Health brigades programme coordinator El Fuerte Ki9
local urban 1 Health brigades programme coordinator Carichi Ki10
centres 1 Tarahumara Diocese health commission Guachochi Ki3
1 Local NGO for Tarahumara development Creel Ki4
1 Health centre doctor Carichi WacKi1
1 Missionary to Tarahumara Cerokawi SjpKi1
1 CEDAIN field worker San Jose del Pinal SjpKi2
Key informants at state level were selected purposively according to their professional
role and expertise. Access to local key informants had to be more ad hoc, because of
the difficulties of access and communication in the mountain region, and the limitations
on fieldwork time. Apart from the health sector staff, they formed part of the network of
contacts that then allowed initial access into the communities. Though it was not feasible
to organize equivalent sets of local key informant interviews for all three sites, we are
confident that the combined findings from these interviewees represents a good range of
perspectives on the issues of hazard and health that arise in the region.
Finally, it is important to note that in order to gain access to the study sites the principal
field researcher (Dr Cueva-Luna) developed working relationships with key individuals in
each community who acted in a ‘gatekeeper’ role. These included indigenous community
leaders, volunteer workers and members of religious groups. Three of these
gatekeepers were not formally interviewed, but informal conversations with them also
yielded important insights, and they are referred to in this report under the codenames
SjpGk, WacGk and ChoGk.
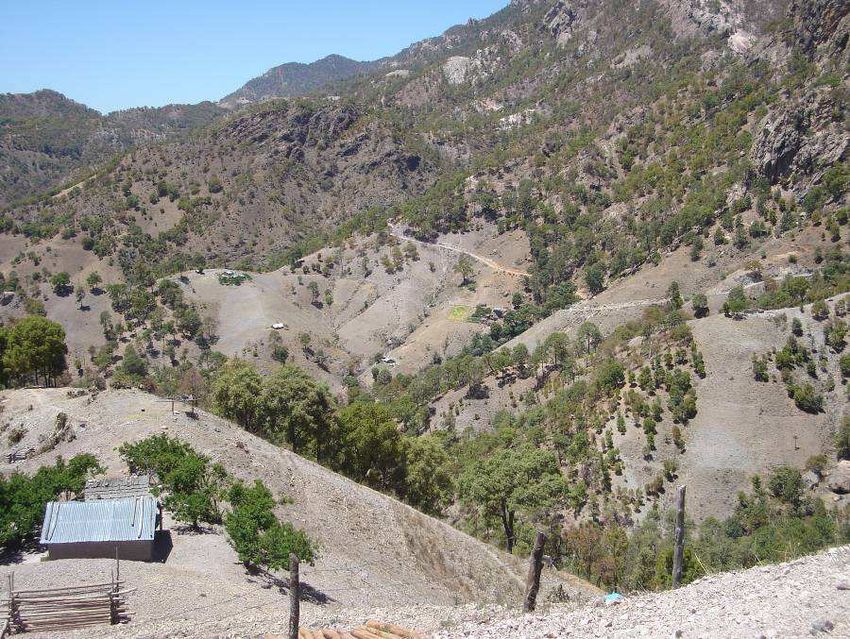
93 Study sites
Located in the interior uplands of north-west Mexico, Chihuahua is the largest of all the
Mexican states in area, and had a population in 2005 of more than 3,400,000. The state
has a predominantly dry climate, in which periodic droughts can be intense. The high
elevation also mean that the state is subject to cold winter extremes. The south-west of
the state is dominated topographically by the northern section of the Sierra Madre
Occidental, with mountains rising to over 2600m. This rugged landscape is home to the
majority of the state’s indigenous population, including the Raramuri people – whose
alternative name of Tarahumara gives the region its popular title the Sierra
Tarahumara. Because the region faces harsh climatic hazards and has northern
Mexico’s most marked concentration of economic marginalization, it was selected as a
case study area for the research programme on climatic hazards, health risks and
responses under conditions of poverty. Within the Sierra region, three sites with differing
physical characteristics were chosen for detailed study: San Jose del Pinal/El Durazno,
Choguita/Capochi and Wacareachi (see Figure 1).
Figure 1 Study sites in the Sierra Tarahumara, Chihuahua
10Physical/social context
The Sierra Tarahumara is a highland region covering just under 60,000 sq km (CEDAIN,
2006a). It occupies the south-west of Chihuahua up to the borders with the Mexican
States of Sinaloa and Sonora. Most of the region lies above 2000m elevation, with some
human settlements above 2400m and the highest mountains rising to over 2600m. The
land gently rises through the drier eastern flanks of the Sierra, typified by open
grassland, to the high central zone, where pine and oak woodland occupies much of the
landscape. West of the continental divide, the terrain is characterized by steep slopes
and deep canyons or ‘barrancas’, incised by rivers descending toward the Pacific (this
includes the area known as the ‘Copper Canyons’, which is one of the prime tourism
areas in northern Mexico). Some of the canyons are sufficiently deep that subtropical
vegetation grows on the valley floor.
A regional study by CEDAIN (2006a) records the population of the Sierra region as
approximately 270,000, spread across 17 municipalities. Urban centres are few and the
majority of the population lives in small rural settlements, with agriculture as the principle
livelihood. Many of the settlements are physically isolated from main communication
routes, and suffer high levels of poverty. The Sierra Tarahumara stands out as a
concentration of poverty on national poverty maps, with income levels equivalent to
many of Mexico’s poorest areas in the south of the country. The region includes the
most marginalized municipalities in Chihuahua state, characterized, according to the
state’s health programme, by inadequate levels of education, health, employment,
nutrition, communications and housing (Secretaria de Fomento Social, undated).
This is consistent with data on the human poverty index (HPI-1)1. As estimated by the
United Nations using data up to 2005, the HPI-1 for Mexico is 6.8. It ranks 10th among
the 108 developing countries for which the index has been calculated (UNDP, 2007).
Though the data we have for Chihuahua is from 2000, it gives a less favoured image of
human poverty for the three municipalities in Chihuahua in which the study sites are
located. The HDI-1 is ranked between 47.29 for Urique and 44.3 for Carichi, while
Guachochi has an intermediate position (Gobierno del Estado, 2007). According to this
estimation, Urique is the third most marginalized municipality in the state, followed by
Guachochi in fourth and Carichi in fifth position.
Alternative indices compiled by CONAPO (2005)2 indicate that the three study sites are
evaluated as municipalities with ‘very high’ marginalization and lie within the six most
marginalized municipalities in the state of Chihuahua: Carichi is ranked as the third most
marginalized, while Urique and Guachochi are in fourth and sixth rankings (see Table 4).
These three municipalities have very poor education conditions, like Carichi, where 39%
of its people (of 15 years and older) are illiterate and 65% have not finished their primary
education. Sanitary conditions are also very poor; for example, 62% of the houses in
1
The HPI-1 combines measures of: proportion of people who are not expected to survive age 40; the adult
illiteracy rate; the unweighted average of people without access to an improved water source; and the
proportion of children under age 5 who are underweight.
2
This index of marginalization takes into account various socio-economic data of households, including % of
illiterate population, access to drainage or sanitation services, access to electrical energy and running water,
and the % of occupied population with poor income (up to 2 minimum wages).
11Carichi do not have running water and 58% do not have electricity, while in Urique, 67%
of inhabitants live in houses with just soil floor. The economic level is very low, especially
in Carichi, where 59% of the occupied population earned up to the equivalent of only two
minimum salaries (up to approximately $4 per day).
Table 4 Chihuahua: Marginalization Indices in 2005
State of
Chihuahua Carichí Guachochi Urique
Total population 3 241 444 8 377 45 881 19 566
% Illiterate population (15 years old or
older) 4.42 39.29 31.11 35.25
% Population without complete primary
school (15 years old or older) 18.81 65.07 54.87 60.56
% Occupants in houses without drainage
nor sanitary service 3.29 44.35 41.47 34.17
% Occupants in houses without electrical
energy 4.28 51.30 57.61 45.48
% Occupants in houses without running
water 6.45 46.74 62.42 55.90
% Occupants in houses with soil floor 6.45 51.83 61.93 66.72
% Population in localities with less than
5000 inhabitants 17.54 100.00 73.01 100.00
% Occupied population with revenue of
up to 2 minimum wages 27.25 58.93 43.79 50.65
Marginalization Index 1.95372 1.92281 1.93383
Very
Degree of Marginalization High Very High Very High
Marginalization ranking in the state of
Chihuahua 3 6 4
82 89 86
Marginalization ranking in Mexico
Source: CONAPO, 2005, Annex B, "Índices de marginación por municipio, 2005", Table B.8, pp.
108-109. Calculations by CONAPO based on the II Conteo de Población y Vivienda 2005, and
Encuesta Nacional de Ocupación y Empleo (ENOE) 2005, IV Trimestre.
Just under a third of the population of this micro-region belongs to indigenous ethnic
groups. By far the largest of these groups is the Raramuri or Tarahumara people. With a
current population estimated at 75,000 (in 2005, INEGI registered 72,461 Tarahumaras
of 5 years old and over), the Tarahumara represent 77% of the total indigenous
population in Chihuahua (see Table 5). Income poverty is high among the Tarahumara,
many of whom are poorly integrated into the market economy, have poor access to
services and are relatively marginalized from wider Mexican society. Official figures
reveal a rather low rate of economic activity for indigenous people in Chihuahua (46% in
2000), lower still than the low average for indigenous people across Mexico, and with an
extremely low rate for women (27%) (see Table 6). Similarly, indigenous people in
Chihuahua have had a relatively low educational attainment (3.2 years of education in
2005), which has just slightly increased in recent years, and which is again worse in the
case of women (2.9 years) (see Table 7). In recent decades, outmigration has become
common among the Tarahumara, with seasonal or permanent migration to nearby urban
centres such as Cuauhtemoc and Chihuahua City, as well as to other parts of Mexico
12and to the United States (CEDAIN, 2006a). Box 1 provides further information on the
Tarahumara people.
Table 5 Chihuahua: indian population (5 years old and over) by language, 2005
Language Total Distribution %
Indigenous population (5 years old and
over) 93,709 100.0
a
Tarahumara 72,461 77.3
Chihuahua's Tepehuano 6,797 7.3
Mixteca languages 1,199 1.3
Náhuatl 1,042 1.1
Chinanteca languages 838 0.9
Mazahua 730 0.8
Guarijio 605 0.6
Zapoteca languages 589 0.6
Other indigenous languages 1,975 2.1
Not specified 7,473 8.0
a
This population represents 2.48% of the total population in Chihuahua.
Source: INEGI, 2006.
Table 6 Percentage of indigenous population of 12 and more years old that is
economically active, 2000
Total Men Women
MEXICO 58.6 85.0 33.1
Chihuahua state 46.4 64.8 26.9
Source: INEGI, 2000
Table 7 Average educational attainment of indigenous population (15 and more
years old)
(Years of education)
2000 2005
Total Men Women Total Men Women
MEXICO 4 4.6 3.4 4.5 5.1 3.9
Chihuahua state 3 3.4 2.6 3.2 3.6 2.9
Source: INEGI, 2006
13Box 1 The Tarahumara people
Tarahumara people are internationally known for their ability to walk and run long
distances, either for normal social interaction or for special competitive events.
They have been portrayed as nomads because they move about from place to
place, usually seasonally. If in the past these movements followed either routes
or circuits according to the state of the pasturage or food supply within a
subsistence farming system, nowadays they tend to involve movement to and
from cities in order to gain income (in part, at least, to make up for shortages of
food in the subsistence system).
As Tarahumaras have tended to live in remote places within the Sierra, often
within ravines and canyons, they have been isolated for centuries and this has
helped them maintain old traditions and a simple way of life. Despite this,
Tarahumara people have been exposed to the influence of Catholic missionaries,
especially Jesuits, who early set up missions within their territory. One benefit of
the missions is that they have often provided health services. Catholic influence
in Tarahumara life has been major, yet some of the indigenous customs remain
alive.
Tarahumaras have tended to retain an organization in each community partially
based on leaders (governors) elected every three years on average. In the most
organized communities, people meet every Sunday so that the authorities can
give a speech about current issues that affect them in some way. An important
domestic institution they have been able to keep is the tesguinada, which is a
corn-beer party where people of the community or their surroundings come to
socialize and to learn what is happening in the communities. A tesguinada may
have the purpose of returning favours as the Tarahumara have a strong system
of mutual assistance. It may also have a religious purpose associated with
benefit for a person individual (who wishes to be cured) or a communal benefit
(to get rain from God). Anthropologist John Kennedy estimated that each adult
spent about 100 days out of each year in this sort of celebration, considering time
for ‘preparation, consumption, and recovery from the effects’ (cited in Fontana
and Schaefer, 1997, p46). This institution is so important in Tarahumara life that
Carl Lumholtz, one of the first anthropologists to visit the region, said: ‘Rain can
not be obtained without tesguino; and corn cannot grow without rain. This in a
nutshell is the Tarahumaras´ view of life’ (Lumholtz, 1902, p255).
The three study sites in this research project are all predominantly Tarahumara
communities, with high levels of poverty and all located at least one hour’s drive on dirt
roads from the nearest small town. They differ principally in their location within the
Sierra region, with one in the barranca zone, one in the high mountain zone and one in
the lower upland zone to the east. (Though located along an imaginary transect line
across the centre of the region, there is no direct communication between these three
sites and transport between each of them takes at least one full day.)
14Site 1 San Jose del Pinal/El Durazno
The first site of San Jose del Pinal is located in the central part of the municipality of
Urique, a few kilometres from the region’s deepest canyon, the Barranca de Urique. The
only vehicle access is via a narrow and rock-strewn dirt road that connects with the
larger settlement of Piedras Verdes, to the north-west. The main village of San Jose del
Pinal (103 inhabitants in 2006) stands on a table-like mountain-top at an altitude of
2100m, and has a church, a school, an assembly room, a CONASUPO (government)
shop, and a clinic run by local nuns (CEDAIN 2006b). It forms the central settlement for
a group of ‘neighbouring’ communities located in the surrounding high mountains,
valleys and deep in the nearby barrancas (up to 5 hrs walk downhill – and 8 walk hours
uphill). Access between these communities is mainly by walking. Local-scale
governance is based on a traditional Tarahumara system led by ‘gobernadores’ – with a
head governor in San Jose del Pinal and further governors and officials in other
communities. San Jose del Pinal in turn is part of the ejido of Piedras Verdes (CEDAIN
2006b). The area retains strong Tarahumara cultural traditions, and the indigenous
language is mainly spoken (people’s Spanish language skills vary from minimal to
fluent). CEDAIN, a non-governmental organization supporting community development
in the Sierra Tarahumara, has a base in the settlement. It has responsibility for
organizing projects under the national PESA programme in fields such as agriculture,
nutrition and education, and has enrolled a number of indigenous community members
as PESA promoters to help implement these projects.
Household interviews in the site focussed on the community of El Durazno (meaning
‘peach’). El Durazno occupies a deep, bowl-shaped valley descending steeply below
San Jose del Pinal and the access road. In 2006, the community had 66 people in 14
households (CEDAIN 2006c), scattered through the valley at various altitudes and with
distances between houses typically measured in hundreds of metres. All households
farm the land, typically growing maize, beans and other crops including squash and
peaches and keeping animals such as chickens, goats and some pigs, asses and cattle.
It seems that most of the farming is for subsistence (or possibly for barter). However,
one important cash crop in the area is cannabis, which appeared to be grown by many
households at the time of the research. Our understanding was that the illicit crop was
promoted by and supplied to external intermediaries. All houses are of simple
construction with adobe walls and, usually two rooms (CEDAIN 2006c). Water supplies
are largely springs and streams in the surrounding slopes from which water can be
collected directly or piped by gravity to households (some of which have storage tanks).
According to one key informant the promotion of cannabis production has stimulated
households to purchase, organise and lay a system of water pipes - for the primary
purpose of irrigation, although the water is also then used for domestic needs [Ki5].
None of the households have latrines.
Site 2 Wacareachi
The second site Wacareachi is located near the south-eastern border of Carichi
municipality, in the eastern margins of the Sierra Tarahumara (Gobierno del Estado,
2007). It lies roughly halfway between the settlements of Tecubichi and Betebachi, and
the main vehicle access is via a steep and rocky side-road connecting to a long-distance
dirt road running north-south. The nearest major town is Nonoava, about one hour’s
drive away in a neighbouring municipality (Wacareachi is remote from the town of
15Carichi). The surrounding landscape is a mountainous semi-desert, with low shrubs,
grassland and bare rock surfaces.
Wacareachi is a small, isolated community or ‘rancheria‘, with an estimated population of
around 100, separated from neighbouring settlements by the rugged terrain and long
distances/journey times. It stands in a valley where two river courses or ‘arroyos‘ meet,
at an altitude around 2000m. These rivers are seasonal, and by the end of our research
(April) had completely dried up except for a few shallow pools, possibly fed by
subterranean water (a well dug in the river bed had water up to about one metre below
the surface). During the rains, however, there can be strong flash flows along these
watercourses (indeed, one in the previous year had swept away a water pump system
put in place by the state water authority).
Some 22 households comprise the settlement (although four houses were unoccupied at
the time of the study). These are scattered through the valley bottoms (at intervals often
hundreds of metres apart), generally standing near the arroyos but on higher ground.
Houses are mostly two-roomed, built from large stones and have neighbouring plots
planted with beans, corn, pumpkin and potato. In the central area of the settlement stand
a small church, school, CONASUPO shop, and a building set aside for meetings and
visits by the local Tarahumara ‘coordinator’. Farming is the principal livelihood in the
area: as well as their crops most households have chickens, goats and sometimes pigs,
and a few people also have horses. The main water sources for the community are the
arroyos and underground water from wells that are dug when the arroyos run dry..The
community has experienced much temporary (e.g. dry season) or permanent
outmigration, with economically active adults seeking income-earning opportunities
elsewhere, including the major urban centres of Cuauhtemoc and Chihuahua City;
however, transportation to and from these cities remains difficult. Apart from the
household running the shop, the local priest and a group of volunteer workers, all
members of the community are Tarahumara.
Site 3 Choguita/Capochi
The third site Choguita lies in the north of the municipality of Guachochi, in the high
mountain zone of the Sierra region. It is about three hours drive from the main town of
Guachochi to the south (via the small town of Norogachi), and three hours from the town
of Creel to the north, in neighbouring Bocoyna municipality. At Creel, connection can be
made both with the paved highway system of the state and with the Chihuahua-Pacific
railroad. The area is high-altitude (much of the municipality stands at over 2400m), with
a landscape broken by the upper tracts of the barrancas that continue west. There are
extensive woodlands (Gobierno del Estado, 2007), and in Choguita a forest industry has
developed , providing a source of work for men.
Choguita is the central settlement of 14 rancherias: which together form an ejido
(communal territory by presidential decree). It is estimated that 280 ejidatarios live in
Choguita and that the total population is 1,500 inhabitants (Velador-Delgado 2006).
Several activities are developed in the central settlement of Choguita, so people from
different rancherias, including Capochi, meet there daily. The settlement has a long strip
of agricultural plots between houses, and there is no well-defined centre: the different
institutions are scattered along the roadway, including a school, a house for ejidatarios,
a clinic run by a non-catholic Christian group, a Catholic nunnery and two houses for
handicraft workers.
16Although research could not be fully completed at this site, the household interviews that
did take place focussed on the rancheria of Capochi (while the group interviews were
formed by women and men of the ejido in Choguita). Capochi is located about half an
hour’s walking distance from the central settlement of Choguita, a distance which is
considered negligible by the Tarahumara and people will make the journey several times
a day if needed. There are 20 households in the rancheria, and a total of over 120
inhabitants, but no common buildings. The layout of the community is fairly rounded,
with a small hill within its terrain and an arroyo that surrounds it. Although some people
have access to mechanical water pumps, there are others, like those who live in the
lower land, who obtain water directly from their arroyos. In dry periods, especially May,
the water supply from the pumps is insufficient in the evenings so people need to
conserve water strategically or travel far away to get it. According to some men in
Choguita, Capochi is one of the communities within the ejido that has suffered most
severely from droughts [ChoGr1].
Health and health care provision
Chihuahua as a whole performs relatively well on key health indicators compared with
the rest of Mexico. According to state health programme document for 2005-2010, the
state has higher life expectancy and lower rates of infant mortality than the national
average and recent years have seen significant advances (Secretaria de Fomento
Social, undated). The document points to a 43% decline in infant mortality between 1990
and 2003, and most strikingly to a steep decline in infant deaths associated with
infectious intestinal diseases from 178 in 1990 to 33 in 2003. Recent data also continues
an epidemiological transition trend taking place for the population as a whole, showing
proportions of deaths due to infectious diseases steadily declining, with intestinal
diseases again highlighting the trend by falling from eighth to nineteenth among the
leading causes of death from 1990 to 2003 (Secretaria de Fomento Social, undated).
However, despite these changes problems remain in tackling preventable conditions,
including rising levels of maternal deaths and persistent child malnutrition. Maternal
mortality was over 50% higher in 2002 than in 1990, and in 2004 the state health
services reported more than 3000 children suffering from malnutrition. As for Mexico as
a whole, though the number of severe cases may have declined, morbidity from
intestinal/diarrheal infections and respiratory diseases remains high. Acute respiratory
infections accounted for 56% of all cases seen by doctors during 2004, followed by
intestinal infections with 14%, and among infants ‘nine out of every 10 cases originate
from these two causes’ (Secretaria de Fomento Social, undated, p23).
Within the state, the Sierra Tarahumara region tends to record the highest levels of
disease risk. According to CEDAIN (2006a) just over 2000 of those malnutrition cases
reported above were concentrated in the Sierra region; and a more recent report
disseminated in La Jornada (2006) indicates that 5000 cases of child malnutrition were
detected in the region by the state system Desarollo Integral de la Familia. The CEDAIN
(2006a) document also claims that the reported infection rate for acute respiratory
infection in the mountain region in 2004 was 63% higher than the average for the state,
and the rate for intestinal infections was 10% higher. For the more marginalized
municipalities the disparity can be still higher: the rate of intestinal infection in Urique
17was reportedly more than 80% higher than the state average. One key informant from
the health system in Carichi underlined how the prevalence of malnutrition compounds
the susceptibility of children to disease: he believed not only that the statistics
significantly under-estimated the malnutrition burden among the Tarahumara but that the
child mortality rate is extremely high and poorly reported [WackKi1].
Key informants from the state’s health system described how acute respiratory cases
are most prevalent during the colder winter months (beginning and end of the year),
while diarrhea cases tend to peak in the warmer months around April-May, according to
some key informants [Ki7, Ki9, WacKi1], and in the early weeks of the rainy season
starting end of June, according to other key informants [SjpKi1, ChoGk]. The point of
view of the last group of key informants is consistent with the official statistics of
Chihuahua health sector in two of the study sites. Health service data available for two of
the study areas for the period 2000-2007 indicate that both acute respiratory diseases
and acute intestinal diseases occur year-round, but tend to rise on the seasonal basis
described above (Servicios de Salud de Chihuahua, 2007a, 2007b). Table 8 draws on
this data for the health administration unit of Urique I, which includes San Jose del Pinal
and has a total population of 4453 people, and Table 9 shows information for the health
administration unit of Carichi III, which includes Wacareachi and has 778 people.
Analysis of such data has to be treated with caution, but the seasonal pattern is evident,
and it is also appears that in some years the burden of reported disease from these
causes can be high, with up to 5% of the population reporting within a single week.
According to several key informants, dermatitis caused by contact with polluted water is
another very common disease [Ki7, Ki9, WacKi1].
Table 8 Seasonal disease incidence: reported cases for Urique I unit
acute intestinal infections acute respiratory infections
Weeks of the year with highest week 33: 5 cases week 3: 19 cases
3
median number of reported week 37: 3 cases week 11: 17 cases
cases, 2000-2007 week 38: 3 cases week 49: 16 cases
Week with maximum number week 33, 2006: 111 cases week 46, 2005: 193 cases
of reported cases week 25, 2006: 82 cases week 50, 2005: 182 cases
week 38, 2006: 61 cases week 7, 2006: 169 cases
Source: Servicios de Salud de Chihuahua, 2007a.
Table 9 Seasonal disease incidence: reported cases for Carichi III unit
acute intestinal infections acute respiratory infections
Weeks of the year with highest week 33: 4 cases week 3: 21 cases
median number of reported week 37: 4 cases week 2: 8 cases
cases, 2000-2007 week 25: 2 cases week 6: 6 cases
Week with maximum number week 33, 2003: 13 cases week 2, 2005: 42 cases
of reported cases week 4, 2000: 12 cases week 16, 2002: 39 cases
week 36, 2005: 11 cases week 3, 2002: 36 cases
Source: Servicios de Salud de Chihuahua, 2007b.
3
Median was used in the original data source rather than mean, because the presence of occasional extreme
values relating to specific short-term disease outbreaks would otherwise have skewed the data.
18The public health system in Chihuahua operates through diverse institutions: those
people with social insurance are served by the Instituto Mexicano del Seguro Social
(IMSS) and other employment-based schemes (e.g. ISSSTE, SEDENA); those who
have no social insurance are served either by the Chihuahua health services (Servicios
de Salud de Chihuahua) or by the scheme IMSS-Oportunidades. It is these last two that
are mostly utilized by low-income groups in the Sierra Tarahumara.
None of the study sites themselves are home to public medical facilities. In order to
access primary or secondary level facilities residents face a journey by vehicle of several
hours at least, and such facilities are seldom utilized except for severe cases. For San
Jose del Pinal, the nearest is a small SSC medical unit in Piedras Verdes, but there is a
larger SSC clinic in Cerocahui, an IMSS-Oportunidades unit in Cienguita, and at several
hours distance an IMSS-Oportunidades facility capable of dealing with emergency cases
[Ki7, Ki9, SjuPKi2]. For people in Wacareachi the nearest health unit is in Nonoava, but
many appear to reserve attending a medical unit only in severe cases, in which case
they may travel to one of the secondary level facilities in the large urban centres of
Cuauhtemoc or Chihuahua [Ki7, Wac1]. For residents of Choguita the nearest facility is
the IMSS-Oportunidades unit in the town of Guachochi [Ki7, Cho4].
In the last 10 years, the state health system has initiated an itinerant service in order to
reach the remote communities in the Sierra region. These ‘brigades’ are medical teams
with a vehicle that visit defined areas within the mountains (Urique municipality, for
example, has three such administrative areas, with San Jose del Pinal part of the area
Urique I). Every brigade is made up of one doctor, one nurse and one auxiliary worker
(who also acts as driver). The brigade visits: (1) the central site of its area; (2) sub-
centres that exist in that area; and, in addition, (3) some communities that have access
by road. The first two of these have some facilities which belong to the health system
and are located in strategically important points of the area. The brigade can stay two or
three days in each place, depending on the number of communities that they have to
visit. Hence, personnel distribution and the time they remain in each community in the
area is based on the demographic density and access criteria.
In conjunction with the brigades, the health system has also recently set up a network of
community health workers referred to as ‘Cocs’ (which means in Spanish Coordinador
de salud Comunitaria). Cocs´ work is coordinated by the head of the brigade in each
municipality, and they are trained in the same way as the brigade auxiliary workers [Ki9].
They have responsibility to access the most remotes communities in the area: those that
cannot be reached by the brigades. Each brigade and its cocs leave their centre
together every month and make rounds for a period of 19 days. As the brigade arrives at
each stop, the cocs then make their own way to visit the outlying communities (often on
foot).
The brigade and the cocs provide preventive health services under the Oportunidades
Programme, provide some curative care, and refer more seriously ill patients to second
level facilities. In theory the health system provides attention and medicine free of
charge for the majority of the Tarahumara population. However, it was stated by some of
the households that only those who attend preventive health talks are those who
become enrolled in the Oportunidades Programme [SjpGr2].
19In the study sites themselves, very few people have access to private sector medical
practitioners, although religious groups, volunteers and traditional healers have long
played an important role. San Jose del Pinal has a clinic run by the local nuns that
provides free advice, medicines and some traditional remedies for the local population,
including residents of El Durazno (CEDAIN 2006c) [SjpKi2]. According to CEDAIN
(2006b), the clinic pays special attention to child health, with weight/height checks and
free milk provided for the under fives. The nuns have also established a network of
indigenous health promoters within the local communities. In the local area there are
also three traditional healers (‘curanderos’ or ‘owirúames’), who dispense spiritual
services as well as herbal remedies (CEDAIN 2006b). Communities in Wacareachi and
Choguita also have access to simple medical assistance provided by religious groups or
volunteers, and similarly make use of traditional healers and herbal medicines [Wac2,
Cho1]. Choguita also has relatively easy access to well-equipped clinics run by nuns in
Norogachi and Creel. Table 10 provides further details on the different types of health
workers who provide services in the study sites.
Table 10 Health workers in the Tarahumara communities
function/training presence in the communities
1. Nurses Trained by schools. They either External actors who work in the
have a job in the public health communities. We distinguish nuns
system (eg in the brigades) or and missionary workers. Nuns
work in other institutions or who are nurses were working in
groups, mainly associated with San Jose del Pinal. Missionary
churches. volunteers with nursing training
were working in Wacareachi.
2. Volunteer Volunteers without formal They are residents of the
community nursing training when communities. Wacarechi has a
nurses commencing their services; health worker in this category,
they learn through experience. whose role is now informally
They may later receive training incorporated within the health
through informal participation in system.
health system.
3. Cocs Auxiliary health workers (or Their function is to travel to the
possibly nurses) who have farthest communities by foot or on
training via the health system. animals.
They visit those communities
that cannot be reached directly
by the brigades.
4. Indigenous Indigenous people organized by Members of the local
health religious groups to assist with communities organized by nuns in
promoters health promotion. They may San Jose del Pinal and Choguita.
already have knowledge on
home remedies, and are willing
to learn more about health from
people in the Church. They
eventually might learn to use
medicine for basic treatments.
5. Traditional Indigenous people who have Individuals with this role are
healers or specialist knowledge of present in each of the study
curanderos traditional healing. They cure areas.
with medicinal herbs and rituals
20Climatic hazards
Most of the Sierra Tarahumara has a semi-humid climate, with warm summers and cold
winters, although the barrancas in the extreme west are low enough in elevation that
temperatures are subtropical in character (Gobierno del Estado, 2007). Annual rainfall
across the region tends to be higher than for the state as a whole, although in the drier
months (the main dry season is typically March to June) precipitation is commonly just a
few millimeters. Mean annual temperatures tend to be lower than the state average,
especially in the higher mountain zones, and in the coldest winter months (November to
February) minimum temperatures often drop below freezing in the higher settlements
(JCAS, 2005).
Unfortunately, weather data available for the region is of poor spatial resolution because
there are few functioning weather stations [Ki2]. Table 11 provides indicative data for the
municipalities in which the study sites are located, and provides figures for the state as a
whole for comparison. However, because of complex topography and altitude
differences, this can only approximate to conditions in the sites themselves, especially in
terms of temperature. In particular, El Durazno is likely to experience cooler
temperatures than those recorded for the low-lying main town of Urique. El Durazno lies
in a climatic zone intermediate between the subtropical barrancas and the high
mountains (CEDAIN 2006c).
Table 11 Mean climatic conditions for the municipal towns of Urique, Guachochi
and Carichi
Urique Guachochi Carichi Chihuahua
state
altitude (m) 549 2400 2038 -
mean annual 22.4 13.7 16.4 17.4 (2005)
temperature
(degrees C)
mean annual rainfall 782 540 497 445 (2005)
(mm)
Source: Gobierno del Estado, 2007; JCAS, 2005.
The principal climatic hazards that affect the Sierra region are extreme cold weather
and, especially, prolonged drought. According to CENAPRED (2001), the Sierra
Tarahumara is one of the regions of Mexico most prone to cold winter spells, with the
high mountain zone averaging more than 100 days per year of ‘heladas’ (when
temperature falls below 0 degrees for more than 12 hours). In 2005, for example, the
town of Creel (2353m altitude) had 146 days during October to March with temperature
falling below zero, and a minimum recorded temperature of -11 degrees (JCAS, 2005).
The lowest temperature recorded at Carichi is -12.3 degrees and at Guachochi is -15
degrees (Gobierno del Estado, 2007). Cold spells can be a particular problem in this
region. Despite acclimatization to cold conditions, the more vulnerable members of poor
21communities may be especially at risk from exposure outdoors and from inadequate
heating in the home [SjpKi2]. Chihuahua has experienced at least five severe cold wave
periods since the 1980s, including a phase spanning three months in 1992/93 when
temperatures dropped to -19 degrees in the Sierra region and 44 people died within the
state (CENAPRED 2001).
Periodic snowfalls also affect the region in winter, but according to many interviewees
these are generally welcomed because of the belief that snow reduces agricultural pests
in the subsequent growing season and may also reduce the prevalence of respiratory
pathogens [Ki3, Ki4, SjpKi2, ChoGr1]. Indeed absence of snowfall in winter is perceived
as one negative consequence of prolonged droughts, in terms of nutrition and disease.
According to CENAPRED (2001), Chihuahua is the Mexican state most severely
affected by droughts or ‘sequías’. The state is characterized by relatively low rainfall, but
periodically undergoes phases of exceptionally low precipitation, including the historic
periods 1948-54, 1960-64 and 1970-78, when drought was prolonged and severe
(CENAPRED, 2001). At the time of the research, the region had recently experienced a
very prolonged phase of lower than average rainfall: one that had continued since 1992
(JCAS, 2005). Rainfall across most of the state for 2005 was 60-70% the national
average (JCAS, 2005), and for much of 2006 extreme drought conditions affected many
parts of the state, including the Sierra region. The North American Drought Monitor
service introduced an ‘extreme drought category’ for south-western Chihuahua in
February 2006 (NADM, 2007), and a series of precipitation maps produced by the
Chihuahua Instituto de Ecologia for the first half of 2006 record categories of ‘severe’,
‘extreme’ or ‘exceptional’ drought affecting each of the study sites. The category
‘extreme’ implies widespread water shortages and major damage to crops and pasture.
By early 2007, when the field research took place, the drought appeared to have eased
in the study sites, with more normal patterns of rain and snow for several months
(NADM, 2007) [SjpKi1, SjpKi2, WacGr]. Nevertheless water shortages were still a major
issue for the communities.
Many interviewees (both key informants and householders) spoke of severe problems of
water supply in recent years, with associated crop losses and shortages of water for
domestic uses [Ki3, Ki4, Sjp6, Sjp7, Cho1/2, Wac 1]. One key informant stated: ‘there
hasn’t been a normal seasonal cycle for many years; people have lost faith in
agriculture’ (interview Ki4, Creel). In some cases whole crops had been ruined – in
Wacareachi many people said that this had happened to the previous harvest [Wac2,
Wac7, Wac8, WacGr]. In San Jose del Pinal water was reportedly in such short supply
during April 2006 that there was only enough water for preparing meals and people had
to stop bathing and washing clothes [SjpKi2]. For all the study communities the bulk of
their domestic water normally comes from sources rapidly affected by seasonal
changes: from rivers and mountain springs.
The long duration of the recent drought begs the question of whether the region itself is
undergoing climatic change. As Box 2 shows many interviewees described a pattern of
change. However, whether that perception has arisen simply because the recent drought
was an exceptionally long anomaly or because there is a long-term directional shift in
climate is impossible to ascertain. There is not yet conclusive scientific evidence that
global-scale climate change is affecting the region, but neither is there conclusive proof
otherwise. Moreover, four of the interviewees specifically argued that a drying trend had
been caused over recent decades because of local-scale environmental change –
22You can also read