Clinical Pharmacists in Oncology Practice - ASCO Journals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Best Practices in Practice
Clinical Pharmacists in Oncology Practice
Why do we need our own pharmacist? That’s what Barbara
McAneny, MD, wondered. As chief executive officer of New
Mexico Oncology Hematology Consultants in Albuquerque,
New Mexico, a practice that includes 10 medical oncologists
at five sites, she wasn’t sure such an addition could be
justified. After all, oncology nurses can mix chemotherapy
and the typical salary package of a clinical pharmacist
generally exceeds six figures.1 So, to determine the possible
impact a pharmacist might make on the practice, she
conducted an informal, internal, time-and-motion study. A
review of it led her to predict a “break-even” cost for the hire,
she recalls. Still, it confirmed that a clinical pharmacist was a
tangible idea—it wasn’t going to take money away from
the practice.
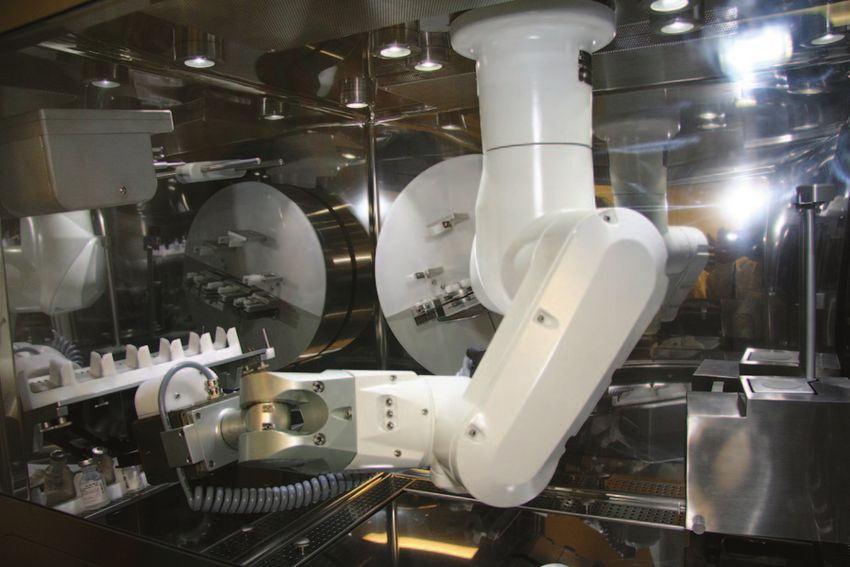
The group ran a local advertisement, listing some carefully A totally automated mixing system for chemotherapy
researched job requirements, including specifying an medications is making its debut at two American
oncology pharmacist. McAneny had high hopes for the new medical centers, with little fanfare but a lot of optimism
employee. She thought he might free up enough time from that this new way of compounding will benefit
the nursing staff to preclude the need to hire another nurse. cancer care.
“I have to admit I was wrong,” she says—and very happily so.
“He’s far more valuable than just that,” she adds. In fact, Michael Sanborn, RPH, MS, corporate vice president
McAneny now considers the practice’s clinical at Baylor Health System in Dallas, Texas, said oncology
pharmacist invaluable. has been the driving force behind a pilot program on
the system that is scheduled to begin there in May. He
Inventory no longer piles up, and it is so well managed that thinks the approach will be “better for patients, better
the possibility of drugs doing a disappearing act now seems for pharmacy operations.”
almost nonexistent. And the improvements in oversight don’t Testing already is underway by the pharmacy staff at
end there. From adding updates on evidence-based protocols the University of Colorado Hospital, just outside
in the electronic medical record (EMR) to keeping precise Denver, Colorado, says Nancy Stolpman, PharmD,
track of medications, the clinical pharmacist has lightened the PhD, the pharmacy director. A robotic workbench
load by providing in-service education on guideline revisions prepares chemotherapy regimens in a new kind of
and new drugs, and by implementing operational technology error-preventing way. “The robot has numerous
that makes that information available at the touch of a redundancies built in,” she says. A “picture library”
few keystrokes. contained in the technology, for example, validates that
the active ingredient is correct; bar code technology
“He’s so good at figuring out what we need,” she says. Under ensures that the mixture is the right drug, for the right
the pharmacist’s purview, two pharmacy technicians provide patient. The engineering involved also protects the
patient refills and help in patient-assistance programs for sterility of the compound, and uses specific gravity
securing free or low-cost medications for those who calculations to determine that the dose is
need them. precisely accurate.
The technology also will help protect pharmacy staff
At a time in which treatment regimens seem subject to near-
who now may be exposed to cytotoxic agents during
constant revision and in an era in which error prevention in
the course of manual mixing. “This robot is ideal
medicine has been made a national priority, the collaboration
because it pushes the exposure to zero for pharmacy
between oncologists and clinical pharmacists seems destined
personnel,” she says.
to grow, says James G. Stevenson, PharmD, director of
pharmacy services at the University of Michigan Health The system is designed to cut down on waste, to
System and associate dean for clinical sciences at the College promote patient safety, to increase the volume of
of Pharmacy. It benefits both oncologists and pharmacists, he admixture that can be mechanically produced, and to
suggests. The teamwork allows oncologists to focus on disease improve dosing accuracy.
eradication, while pharmacists help keep patients informed
172 JOURNAL OF ONCOLOGY PRACTICE • V O L . 4, I S S U E 4 Copyright © 2008 by American Society of Clinical Oncology
Downloaded from ascopubs.org by 46.4.80.155 on October 15, 2021 from 046.004.080.155
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.about the multiple-drug usage that often becomes a routine certain practice contracts are among the tasks now associated
part of life during treatment. with clinical pharmacists in oncology practices. One report
estimates that currently a majority of oncology practices that
The role of clinical pharmacist as health educator has grown. have eight or more oncologists on staff also have pharmacists
Now, many spend more time than ever in direct patient and pharmacy technicians.4 From efficient management of
contact, explaining treatment goals, possible adverse effects, drug inventory to effective use of the EMR, a clinical
and safe and successful use of medications. In fact, patients pharmacist can mean significant “charge capture” that keeps
with cancer often receive information about their cost-saving high and unnecessary expenditure low, D’Amato
chemotherapy regimen and supportive-therapy options from explains. And data routinely can be caught and analyzed, too,
a clinical pharmacist, he observes. “With this higher patient when clinical pharmacists are well versed in
contact, the field is drawing people into it who are more medical informatics.
patient-oriented,” Stevenson notes. Because the impact on
quality of life can be sudden and significant, the latter can be In the coming years, as the baby-boom population
particularly important to patients, who want to live as presumably increases the demand for cancer care, there will be
normally as possible after diagnosis. even more need for screening and prevention of potential
drug interactivity from both prescription and over-the-
Pharmacists also have played a big part in helping ensure safer counter medications, a knowledge niche that may be filled by
medication prescribing and dispensing practices at many clinical pharmacists.5
hospitals, by assisting in the implementation of electronic However, for practices with fewer than five oncologists, a
order-entry systems that prevent the kind of medical errors clinical pharmacist might not make as much financial sense,
highlighted nearly a decade ago, in the Institute of Medicine McAneny speculates. Clinical pharmacists typically do not
(IOM) report, “To Err is Human: Building a Safer Health bill directly for their services—although Medicare Part D
System.” Practice guidelines have flourished since the medication therapy management opens the door to some
publication of the IOM report, necessitating changes in direct billing.6
information technology (IT) to keep up with the frequent
growth and changes in such guides. In terms of the IT that One other aspect of the job that may become more important
helps prompt compliance with them, “a lot of pharmacists in the next few years is supervision of pharmacy technicians,
have been very active helping their hospitals to do this,” according to D’Amato. In the practice in which he works—
Stevenson says. four sites, 17 physicians—there are seven pharmacy
technicians. Because of growing reliance on such staffers,
Beyond the benefits of IT improvement, inventory flow, and states are now taking a hard look at the training and
protocol expertise, there are other reasons an oncologist might certification of them. “Nationally, this is starting to be
want to bring a pharmacist on board. Clinical pharmacy is a addressed,” he observes. One result will likely be more
field that has made pharmacogenics an increasingly important participation by clinical pharmacists in educating and
area of study, as research continues to show how individual managing these technicians.
genes may relate to drug metabolism and treatment response.2
And, in community practices, the inclusion of clinical How do clinical pharmacists like working side by side with
pharmacists has been shown to improve outcomes in chronic oncologists? Early anecdotal accounts in pharmacy journals
disease, particularly when they are directly involved in patient peg it almost as a match made in health care heaven. Being a
care. In one study, for example, pharmacist involvement clinical pharmacist in a busy practice is demanding, but also
resulted in substantial reductions of glycemia measures in very gratifying, affirms D’Amato. His profession often isn’t
patients with type 2 diabetes.3 just a critical member of the team, but also an integral part of
the leadership, he notes. As such, clinical pharmacists help
To be most cost saving and effective, a clinical pharmacist build practices, not just support them. “It’s been challenging
needs to have a strong relationship with all departments in an and fun,” he adds.
oncology practice, advises Steven D’Amato, RPh, BCOP, “This isn’t replacing what the physician does,” reiterates
clinical pharmacy specialist at the Maine Center for Cancer David Chen, RPh, MBA, director of the section of home,
Medicine in Scarborough, Maine. In many cases, a clinical ambulatory, and chronic care practitioners for the American
pharmacist makes sense for the practice— dollars and cents, Society of Health-System Pharmacists (ASHP) in Bethesda,
that is. “In private practices, there isn’t room to lose a dollar,” Maryland. But with the aging demographic, the pharmacist is
he explains. the right person to manage patients on complex drug
regimens, he stresses. However, for the most part, pharmacists
Keeping clinical regimens consistent with current guidelines, don’t bill directly for services. That is predicted to change.
staying abreast of the operational technology required for the
EMR, clinical education, oversight of research protocols, and A primary goal of the ASHP is to work with the Centers for
providing financial oversight of most coding procedures and Medicare and Medicaid Services to achieve provider status
Copyright © 2008 by American Society of Clinical Oncology J U L Y 2008 • jop.ascopubs.org 173
Downloaded from ascopubs.org by 46.4.80.155 on October 15, 2021 from 046.004.080.155
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.under Part B, so that these clinical services—which now have Buffington asserts. At CPT editorial panel hearings on coding
been formally labeled as medication therapy management changes, for example, oncologists have repeatedly expressed
(MTM)— can be made more broadly available to patients, support for the emerging role of the pharmacist in patient
Chen says. care, he observes. In oncology, the addition of a pharmacist
“is clearly associated with a strong return on investment from
Pharmacists already can receive direct compensation for a financial, liability, time efficiency and clinical perspectives,”
small percent of Medicare Part D beneficiaries who need he adds.
multiple drugs and have multiple disease states. And, in
certain parts of the country, there are provisions for direct Though the codes have yet to be given an official monetary
reimbursement by state-sanctioned programs for MTM in assignment, they are being utilized for billing—and paid
which the pharmacist may be a primary provider. These for— by insurers in many practices across the country, he
include states such Florida, Minnesota, and North Carolina. says. Typically, billing success begins with opening a dialogue
The latter is a state that has set aside appropriations for just between the practice and the payor to discern if MTM codes
such a purpose—a form of funding that may increase in the are covered and to discuss the anticipated fee schedule, he
coming years, Chen suggests. But, because pharmacists are says. In most cases, the MTM codes are yielding payment
not currently listed as providers on the CMS Medicare Part rates similar to those paid for mid- to high level evaluation
B, it’s currently left to the marketplace to determine the value and management cognitive service codes utilized by their
range for MTM service codes. physician counterparts, according to Buffington.
However, three new entries—99605, 99606, 99607—in the Pharmacists are positioned to be more of a “consultative
2008 coding manual of Current Procedural Terminology support role” to improve medication outcomes and support
(CPT) now describe the patient-care services provided by the prescriber in the management of patient, not a “primary
pharmacists, and they create a viable mechanism to bill care” role, he emphasizes. In fact, most states have enhanced
insurers, notes Dan Buffington, PharmD, MBA, president their pharmacy and medical practice acts to reinforce the
and chief executive officer of Clinical Pharmacology Services “collaborative” nature of pharmacist and physician
in Tampa, Florida. These codes were converted from relationships, Buffington says. “It is all about helping
temporary “Category III” codes to permanent “Category I” physicians to select, refine, and implement the most effective
codes within 2 years of approval for placement in the CPT medication regimens.”
manual. “This is a reflection of the rapid uptake in the health
care market based on both volume of use and value to After all, pharmacists “take a 10,000 foot view of a patient’s
insurers,” he says. However, receiving a nationally recognized medications,” adds Buffington—a perspective that helps
“valuation” or range-of-service rates will likely take longer to ensure safe medication usage and lighten the burden that can
establish, he cautions. overwhelm practitioners in a busy practice.
Clinching those recommended values is just a question of
time, though, and not a difficult professional challenge, DOI: 10.1200/JOP.0843001
References
1. Ukens C: Pharmacist salaries. Drug Topics, http://drugtopics.modern 4. News Report: Oncology practices recruit pharmacists for efficiency, savings.
medicine.com/drugtopics/Independent⫹Pharmacy/Pay-dirt-Pharmacist-salaries- Am J Health Syst Pharm 63:1774-1775, 2006
are-still-climbing-bu/ArticleStandard/Article/detail/408159?contextCategoryId⫽
6880&searchString⫽Pay%20dirt
5. De Lemos ML: Pharmacist’s role in meeting the psychosocial needs of cancer
2. Grabinski JL: Pharmacogenomics of anticancer agents: Implications for clinical
patients using complementary therapy. Psychooncology 14:204-210, 2005
pharmacy practice. J Pharm Pract 20:246-251, 2007
3. Clifford RM, Davis WA, Batty KT, Davis TME: Effect of a pharmaceutical care
program on vascular risk factors in type 2 diabetes. Diabetes Care 28:771-776, 6. Dole EJ, Murawski MM: Reimbursement for clinical services provided by phar-
2005 macists: What are we doing wrong? Am J Health Syst Pharm 64:104-106, 2007
PRACTICAL TIPS FOR THE ONCOLOGY PRACTICE
An essential reference tool, Practical Tips for the Oncology Practice is a comprehensive
manual answering the most frequently asked questions about coding, reimbursement
coverage, and regulatory policies specific to the oncology practice. Order your copy today
at asco.org/store!
174 JOURNAL OF ONCOLOGY PRACTICE • V O L . 4, I S S U E 4 Copyright © 2008 by American Society of Clinical Oncology
Downloaded from ascopubs.org by 46.4.80.155 on October 15, 2021 from 046.004.080.155
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.Journal of
Oncology
Practice http://jop.ascopubs.org
From the Editor’s Desk
The Time Has Come for National Insurance Cards
Therese M. Mulvey, MD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161
Original Research
Barriers to Enrollment of Elderly Adults in Early-Phase Cancer Clinical Trials
• Potential strategies to overcome barriers to enrollment of seniors into early-phase trials.
Michele Basche, MD, Anna E. Barón, PhD, S. Gail Eckhardt, MD, Lodovico Balducci, MD,
Martha Persky, RN, Adrah Levin, MPH, Nathaniel Jackson, MS, Chan Zeng, PhD, Pamela Vranas, MS,
and John F. Steiner, MD, MPH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162
Commentary: Overturning Barriers Will Take Heavy Lifting
Harvey Jay Cohen, MD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
Business of the Business
Practical Tips: Concurrent Infusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
• Clarification of the appropriate use of the concurrent drug administration code.
Best Practices in Practice
Clinical Pharmacists in Oncology Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
• The collaboration between oncologists and clinical pharmacists seems destined to grow.
Increased Use of Oral Chemotherapy Drugs Spurs Increased Attention to Patient Compliance . . . . 175
• Ensuring that patients with breast cancer are taking the oral aromatase inhibitors prescribed as follow-up
treatment to surgery is an ongoing concern for oncologists.
Feature Article
The 2007 National Practice Benchmark: Results of a National Survey of Oncology Practices
• Long-term trends in the cost of pharmaceutical goods purchased by community oncology practices seem to
have dramatically changed in 2007, potentially ending an era of practice growth built on the economic
engine of in-office chemotherapy provision.
Thomas R. Barr, MBA, Elaine L. Towle, CMPE, and William M. Jordan, DO . . . . . . . . . . . . . . . . . . . . . . . 178
The Voice of ASCO
ASCO’s Clinical Practice Committee
The Clinical Practice Committee: A Look Ahead
W. Charles Penley, MD. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
Clinical Research
ASCO Outlines Minimum Standards and Exemplary Attributes for Research Sites: Previews
Tools to Be Provided
• Encouraging community oncologists to consider how to enhance their research programs and also
to give practitioners not already involved in research a clearer understanding of what it involves. . . . . . . . . 185
For Your Patients
Cancer.Net Resources
Cancer.Net. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
Patient Advocate Corner
Planet Cancer: A Community of Young Adults With Cancer
Heidi Adams. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
Downloaded from ascopubs.org by 46.4.80.155 on October 15, 2021 from 046.004.080.155
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.Contents
Volume 4 Issue 4, July 2008
Focus on Quality
Geriatric Oncology: Past, Present, Future
• Efforts to integrate geriatric oncology principles in the training of all medical oncologists are underway.
Arati V. Rao, MD, Arti Hurria, MD, Gretchen Kimmick, MD, Sandro Pinheiro, PhD, and
Pearl H. Seo, MD, MPH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
Commentary: Caring for the Elderly Cancer Patient: Training the Next Generation of Oncologists
Gary H. Lyman, MD, MPH, FRCP(Edin) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193
Strategies for Career Success
Financial Management in Oncology Practice, Part 2: Billing and Collections . . . . . . . . . . . . . . . . . 195
• It pays off to learn how to code accurately and how to make sure that what you legitimately earned
is billed correctly and collected on time.
Technology and Innovation
Personal Health Records: An Emerging Trend . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200
• While today PHRs seem far from the world of working oncology offices, that may change soon.
IT Help Desk
Principles of Safe Practice Using an Oncology EHR System for Chemotherapy Ordering,
Preparation, and Administration, Part 1 of 2
• An outline of broad principles that should be considered when integrating an electronic health record, and
in particular, a chemotherapy ordering module, into practice.
Lawrence N. Shulman, MD, Robert S. Miller, MD, Edward P. Ambinder, MD, Peter Paul Yu, MD, and
John V. Cox, DO, MBA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
Current Clinical Issues
When Doctors and Patients Disagree About Medical Futility
• Factors that may help physicians determine when additional treatment is medically futile, and what
physicians can do to encourage patients to explore more appropriate care options.
Mary S. McCabe, RN, and Courtney Storm, JD, MBE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207
Letter to the Editor
Including Oncological Image Data From CD-ROMs Into the Normal Workflow
Peter M.A. van Ooijen, MSc, PhD, and André Broekema, BSc . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 210
Errata . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 211
Journal of Oncology Practice (ISSN 1554-7477) is published bimonthly (January, March, May, July, September, November) by American Society of Clinical
Oncology, 1900 Duke St, Suite 200, Alexandria, VA 22314. Periodicals postage pending at Alexandria, VA, and at additional mailing offices. Publication Mail
Agreement Number pending. Editorial correspondence should be addressed to Douglas W. Blayney, MD, Journal of Oncology Practice, 330 John Carlyle St, Suite
300, Alexandria, VA 22314; telephone, 703-797-1900; fax, 703-684-8720; e-mail, jopsubmissions@asco.org.
POSTMASTER: Send change of address to Journal of Oncology Practice, American Society of Clinical Oncology, 1900 Duke St, Suite 200, Alexandria, VA 22314.
Nonmembers send change of address to Journal of Oncology Practice, Customer Service, 330 John Carlyle St, Suite 300, Alexandria, VA 22314.
Annual subscription rates (effective through August 31, 2007): United States and possessions: ASCO active-allied, $50; ASCO affiliate, $50; nonmember individual
US, $125; nonmember individual international, $145; in-training US, $65; in-training international, $75; institutional US, $200; institutional international, $250; single
issue US, $25; single issue international, $35.
To receive in-training rate, orders must be accompanied by name of affiliated institution, date of term, and the signature of program/residency coordinator on
institution letterhead. Orders will be billed at individual rate until proof of status is received. Current prices are in effect for back volumes and back issues. Back issues
sold in conjunction with a subscription rate on a prorated basis. Subscriptions are accepted on a calendar-year basis. Prices are subject to change without notice.
Single issues, both current and back, exist in limited quantities, and are offered for sale subject to availability.
Downloaded from ascopubs.org by 46.4.80.155 on October 15, 2021 from 046.004.080.155
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.You can also read