Clinically Undetected Motor Neuron Disease in Pathologically Proven Frontotemporal Lobar Degeneration With Motor Neuron Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL CONTRIBUTION
Clinically Undetected Motor Neuron Disease
in Pathologically Proven Frontotemporal Lobar
Degeneration With Motor Neuron Disease
Keith A. Josephs, MST, MD; Joseph E. Parisi, MD; David S. Knopman, MD; Bradley F. Boeve, MD;
Ronald C. Petersen, MD, PhD; Dennis W. Dickson, MD
Background: Frontotemporal lobar degeneration with evidence of motor neuron disease. Semiquantitative
motor neuron disease (FTLD-MND) is a pathological analysis of motor and extramotor pathological findings
entity characterized by motor neuron degeneration and revealed a spectrum of pathological changes underlying
frontotemporal lobar degeneration. The ability to detect FTLD-MND. Hippocampal sclerosis, predominantly of
the clinical signs of dementia and motor neuron disease the subiculum, was a significantly more frequent occur-
in pathologically confirmed FTLD-MND has not been rence in the cases without clinical evidence of motor
assessed. neuron disease (P⬍.01). In addition, neuronal loss,
gliosis, and corticospinal tract degeneration were less
Objectives: To determine if all cases of pathologically severe in the other 3 cases without clinical evidence of
confirmed FTLD-MND have clinical evidence of fronto- motor neuron disease.
temporal dementia and motor neuron disease, and to de-
termine the possible reasons for misdiagnosis. Conclusions: Clinical diagnostic sensitivity for the el-
ements of FTLD-MND is modest and may be affected by
Method: Review of historical records and semiquantita- the fact that FTLD-MND represents a spectrum of patho-
tive analysis of the motor and extramotor pathological find- logical findings, rather than a single homogeneous en-
ings of all cases of pathologically confirmed FTLD-MND. tity. Detection of signs of clinical motor neuron disease
is also difficult when motor neuron degeneration is mild
Results: From a total of 17 cases of pathologically con- and in patients with hippocampal sclerosis.
firmed FTLD-MND, all had clinical evidence of fronto-
temporal dementia, while only 10 (59%) had clinical Arch Neurol. 2006;63:506-512
F
RONTOTEMPORAL DEMENTIA MND).4 Therefore, FTLD-MND currently
(FTD) is a clinical term ap- represents a distinct pathological entity.
plied to patients who pre- During the last decade, we and others
sent with progressive demen- have observed cases that at autopsy have
tia with an insidious onset, had histologic evidence of mixed fea-
prominent behavioral or language dysfunc- tures of FTLD and MND. Furthermore,
tion, or both. Motor neuron disease (MND) clinical studies have revealed an in-
is also a clinical term, but it is applied to creased frequency of MND in cases of
patients with clinical evidence of cortico- FTD,3 and an increased frequency of FTD
spinal tract involvement, evidence of brain- in cases of MND.2 Unfortunately, studies
stem or spinal cord anterior horn cell in- correlating the clinical signs of FTD-
volvement, or both. Recent studies have MND with the pathologic diagnosis of
revealed that clinical features of FTD and FTLD-MND are limited.5 We therefore set
MND (FTD-MND) can occur in the same out to assess the association of clinical fea-
patient and not infrequently.1-3 tures of FTD-MND and pathologically con-
firmed FTLD-MND.
Author Affiliations:
Departments of Neurology
For editorial comment
METHODS
(Drs Josephs, Knopman, Boeve, see page 489
and Petersen) and Laboratory
Medicine and Pathology CASE ASCERTAINMENT
As with the clinical syndrome of FTD-
(Dr Parisi), Mayo Clinic,
Rochester, Minn; Department of MND, pathologic studies have indepen- The Mayo Clinic (Rochester, Minn) pathologi-
Pathology and Neuroscience dently identified cases with frontotempo- cal database was searched to identify all cases
(Dr Dickson), Mayo Clinic, ral lobar degeneration and features of typical that were autopsied with a pathological diag-
Jacksonville, Fla. motor neuron degeneration (FTLD- nosis of Pick disease, FTLD-MND, or demen-
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
506
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015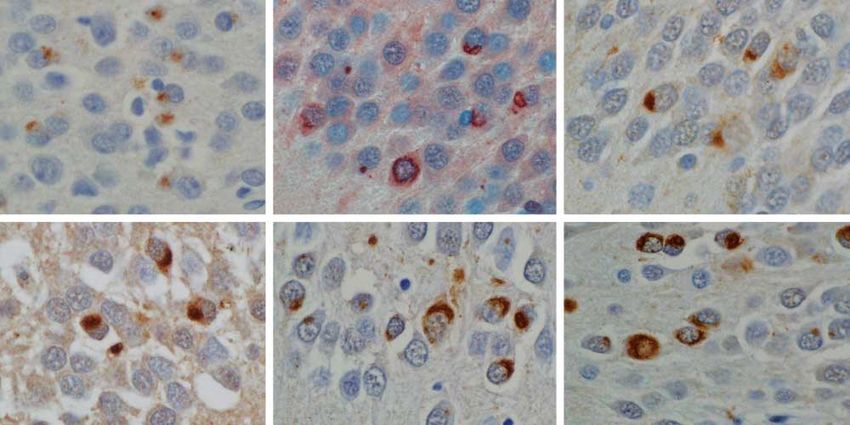
tia lacking distinctive histopathologic features. We also re- rons plus (1) shrunken residual motor neurons, (2) evidence
viewed our cases of FTLD, but none had pathologic evidence of neuronophagia, (3) Bunina bodies, or (4) ubiquitin-
of motor neuron degeneration.6 All identified cases were then immunoreactive intraneuronal inclusions, including Lewy body–
reexamined pathologically with modern neuropathologic stains. like hyaline inclusions, skeinlike inclusions, or pleomorphic
Only cases with a final diagnosis of FTLD-MND were retained cytoplasmic inclusions, which were grouped with skeinlike in-
for this study. clusions for the purpose of analysis. Evidence of frontotempo-
A retrospective review of the historical records of all cases ral lobar degeneration included the presence of superficial spon-
with final pathological diagnosis of FTLD-MND was under- giosis, neuronal loss, and astrogliosis affecting predominantly
taken. Special attention was paid to any sign or symptom sug- layer II of the cortex, with or without the presence of ubiquitin-
gestive of bulbar dysfunction, upper or lower motor neuron dis- immunoreactive neuronal cytoplasmic inclusions. Neuronal in-
ease (or both), and the treating physician’s diagnoses at onset tranuclear inclusions were not detected.
and throughout the disease course.
STATISTICAL ANALYSIS
PATHOLOGICAL ANALYSIS Statistical analyses were performed with SigmaStat software (Sy-
stat Software Inc, Point Richmond, Calif ). Univariate correla-
In all cases identified from the previously described electronic tions for analysis of clinical and pathologic factors used Spear-
search, slides of frontal, temporal, and parietal neocortex, hip- man rank order correlation analysis. A P value of less than .05
pocampus, basal ganglia, thalamus, midbrain, pons, medulla, was considered significant.
and cerebellum were reviewed. In all cases, sections were stud-
ied with hematoxylin-eosin (HE) and modified Bielschowsky
staining, as well as other stains needed for routine evaluation, RESULTS
including immunohistochemistry for markers of glial pathol-
ogy. Those stains include glial fibrillary acid protein for astro- We identified 18 cases that fulfilled pathological criteria
cytes and either CD68 or HLA-DR antigens for microglia. Neu- for FTLD-MND, including presence of ubiquitin-
ronal pathology was studied with antibodies to neurofilament immunoreactive neuronal inclusions in motor or extra-
protein, ubiquitin, ␣-synuclein, and phospho-tau. motor neuronal populations or both in all cases. The
In all cases, the hypoglossal nucleus and/or cervical spinal ubiquitin-positive inclusions were negative for tau,
anterior horn cells were reviewed for evidence of motor neu-
ron degeneration with HE and ubiquitin. In many cases, stains
␣-synuclein, and neurofilament.
for glial fibrillary acidic protein and macrophages were also avail- One case was removed from further analysis because
able. Neuronal loss and gliosis were assessed semiquantita- of a clinical diagnosis of multiple sclerosis 20 years prior
tively in the hypoglossal nucleus and the anterior horn cells of to death. The demographics of the other 17 cases are pre-
the spinal cord with a 4-point scale (0=none; 1⫹=focal neu- sented in Table 1. Of these, 13 (76%) were male. The
ronal loss and focal microgliosis; 2⫹=extensive neuronal loss mean age at onset and disease duration were 52 years and
with microgliosis and empty cell beds containing macro- 2.3 years, respectively.
phages; 3⫹=almost complete loss of motor neurons with at-
rophy and astrocytic fibrillar gliosis). The presence of Bunina CLINICAL FEATURES
bodies was assessed on HE staining in motor neurons of the
hypoglossal nucleus and spinal anterior horn cells. Lewy body–
like hyaline inclusions were assessed on HE staining and ubiq-
All patients had clinical features suggestive of fronto-
uitin stains. Skeinlike and pleomorphic cytoplasmic inclu- temporal dysfunction; however, only 10 cases carried a
sions were assessed on ubiquitin immunostains. The diagnosis of FTD-MND or a comparable diagnostic term
corticospinal tract was assessed for wallerian degeneration us- (such as amyotrophic lateral sclerosis–dementia or de-
ing HE (presence of atrophy with vacuolation and lipid-laden mentia with MND) prior to death. Of the other 7 cases,
macrophages), myelin stains (pallor on Luxol fast blue), or mac- 4 were diagnosed as FTD, 2 with a rapidly progressive
rophage stains (increased ameboid microglia) paying special dementing illness, and 1 as FTD vs Alzheimer disease.
attention to the pyramids in the medulla and the lateral fu- All 10 cases with a clinical diagnosis of FTD-MND had
niculi in the spinal cord. The severity of corticospinal tract de- evidence of motor neuron disease on clinical examina-
generation was assessed semiquantitatively on a 5-point scale tion, while the other 7 did not.
(0 = none, 1 ⫹ = very mild vacuolation and sparse macro-
phages; 2 ⫹ = vacuolation with many lipid-laden macro-
Two cases were initially diagnosed as FTD only (data
phages; 3⫹=many lipid-laden macrophages with myelin loss; not shown); however, they later developed signs of MND
4 ⫹ = myelinated fiber loss, tract atrophy and astrocytic glio- and were subsequently diagnosed as FTD-MND. One of
sis). Extramotor inclusions were assessed semiquantitatively these 2 cases (case 13) developed signs of MND approxi-
with ubiquitin immunostains with a 5-point grading scale mately 45 months after the onset of symptoms of FTD.
(0=none; 0-1⫹=isolated; 1⫹=sparse; 2⫹=moderate; 3⫹=fre- In addition to the features in keeping with a diagnosis
quent number). Histopathologic analysis was conducted by neu- of FTD, 5 cases (cases 2, 3, 15, 16, and 17) also had symp-
ropathologists with expertise in degenerative neuropathology toms of forgetfulness at initial examination. Memory im-
( J.E.P. and D.W.D.). Semiquantitative analysis was con- pairment was not severe or more prominent than the other
ducted by a neuropathologist (D.W.D.). presenting features in any of these 5 cases.
Frontotemporal lobar degeneration with motor neuron dis-
ease (Figure 1) was diagnosed if there was evidence of brain-
stem or spinal cord anterior horn cell degeneration or degen- PATHOLOGIC FINDINGS
eration of the corticospinal tract, or both, in addition to histologic
evidence of frontotemporal lobar degeneration. Histologic evi- Pathologic findings are presented in Table 2 and shown
dence of motor neuron degeneration included loss of large an- in Figure 1 and Figure 2. All cases met pathologic cri-
terior horn cells in the spinal cord or hypoglossal motor neu- teria for FTLD-MND.4,7 The hypoglossal nucleus was
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
507
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015A B C
D E F
G H I
J K L M
N O P Q R
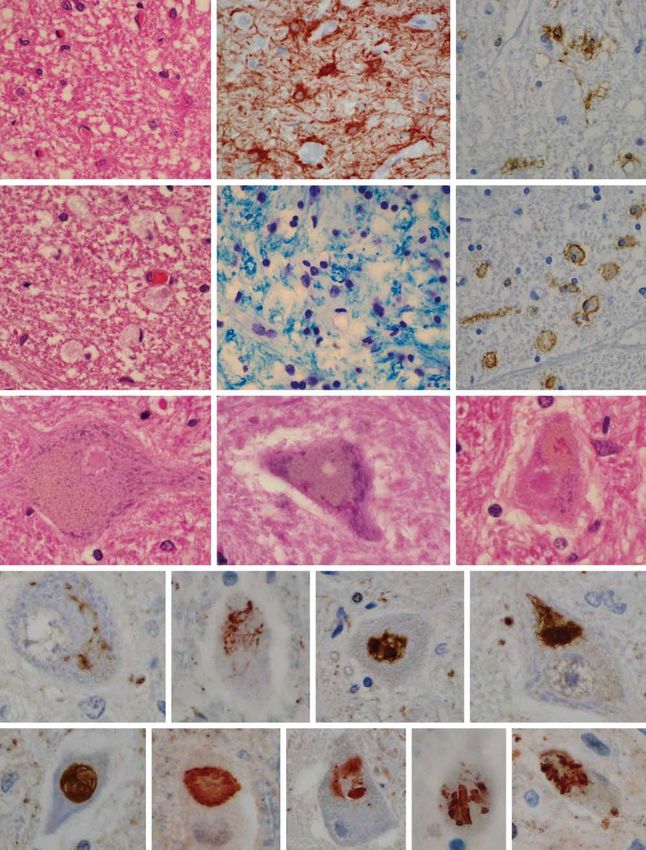
Figure 1. Motor neuronal loss and gliosis (A-C), corticospinal tract degeneration (D-F), and motor neuron inclusions with routine histology (G-I) and with ubiquitin
immunohistochemistry ( J-R). A, Anterior horn cell neuronal loss and gliosis. B, Anterior horn cell gliosis (glial fibrillary acidic protein). C, Hypoglossal nucleus
microgliosis (HLA-DR antigens). D, Pyramidal degeneration and lipid-laden macrophages (arrows). E, Pyramidal myelin loss (Luxol fast blue stain). F, Pyramidal
macrophages (HLA-DR antigens). G and I, Lewy body–like inclusions anterior horn cells (arrows). H and I, Bunina bodies (arrowheads). J-M, Skeinlike inclusions.
N and O, Lewy body–like inclusions. P-R, Pleomorphic inclusions (for all figures, hematoxylin-eosin stain was used unless otherwise noted, original magnification⫻400).
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
508
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015Table 1. Demographics of 17 Cases of FTLD-MND*
STMSS Prominent Symptoms Abnormal Cranial Nerve
Case, Age at Age at Disease on Initial Early in Disease Course, and Motor Neuron Final Clinical
No. /Sex Onset, y Death, y Duration, y Examination (Less Prominent Symptoms) Findings During Illness Diagnosis
1/F 66 70 4 21/38 Personality change, combative, None documented RPD
agitative
2/F 49 51 2 13/38 Personality change, socially None documented FTD
withdrawn, (forgetful)
3/F 47 49 2 NA Behavioral dyscontrol, paranoia, None documented FTD vs AD
pacing, and roaming, (forgetful)
4/M 32 34 2 NA Inappropriate behaviors, apathetic, None documented RP-FTD
(unusual spontaneous laughter)
5/M 55 57 6 35/38 Personality change, apathetic, None documented FTD
weight gain, inability to follow
through
6/M 58 60 2 33/38 Socially withdrawn, emotional None documented FTD
blunting, aphasia, easily
distracted
7/M 58 60 2 17/38 Behavioral dyscontrol, hyperorality, None documented FTD
visual hallucinations,
(incontinence of urine)
8/M 37 39 2 23/38 Personality change, tangentional Prominent fasciculations, Dementia/MND†
and circumstantial in language Babinski sign
9/M 56 58 2 26/38 Language difficulties, slowed Prominent fasciculations, Dementia/ALS†
speech, swallowing difficulties mixed spastic-flaccid
dysarthria, Babinski sign
10/M 49 51 2 28/38 Agitation, personality change, Babinski sign, infrequent FTD-MND
less interactive, rapid loss of fasciculations
verbal output
11/M 43 46 3 NT Emotional blunting, irritability, Spastic dysarthria, Dementia/ALS†
decline in communication fasciculations, tongue
weakness
12/F 51 52 1 23/38 Paranoia, difficulty with planning, Mixed spastic-flaccid FTD-MND
organizing, speaking, dysarthria
(swallowing)
13/M 43 50 7 29/38 Personality change, sexual Prominent fasciculations, FTD-MND
indiscretions, delusions muscle atrophy
involving bugs, lack of
spontaneity
14/M 40 41 1 20/38 Personality change, apathetic, Mixed spastic-flaccid FTD-MND
difficulty processing information dysarthria, prominent
fasciculations
15/M 70 72 2 34/38 Irritability, anomia, (forgetful), Prominent fasciculations, Dementia/MND†
spells of confusion, Babinski sign, muscle
1 hallucination seeing elves wasting
16/M 76 77 1 NA Language difficulties, slowed Prominent fasciculations, FTD-MND
speech, (forgetful) mild weakness, muscle
atrophy
17/M 56 58 2 NA Difficulty with speech, (forgetful), Spasticity, spastic FTD-MND
depression, difficulty performing dysarthria, Babinski sign,
job duties prominent fasciculations
Abbreviations: AD, Alzheimer disease; ALS, amyotrophic lateral sclerosis; FTD, frontotemporal dementia; FTLD-MND, frontotemporal lobar degeneration with
motor neuron disease; MND, motor neuron disease; NA, not able to be tested (either too severely affected or anarthric); NT, not tested (evaluated in 1986 before
publication of the STMSS); RPD, rapidly progressive dementia; RP-FTD, rapidly progressive frontotemporal dementia; STMSS, Short Test of Mental Status score.
*Group 1 (cases 1-7); group 2 (cases 8-17).
†These cases were clinically diagnosed between 1987 and 1991 and explain the older terminology.
available for review in 16 cases. In 14 cases, the cervical present in a number of cases including 2 cases with skel-
spinal cord, but more often multiple levels of spinal cord, etal muscle from the general autopsy; both had evi-
were available for study. Bunina bodies were found in 14 dence of group atrophy with small acutely angulated
cases and skeinlike inclusions, pleomorphic inclusions, fibers consistent with neurogeneic atrophy.
or Lewy body–like hyaline inclusions in motor neurons
were found in 11 cases. Extramotor ubiquitin-positive SEMIQUANTITATIVE RESULTS
neuronal inclusions were present in all cases, in the den-
tate fascia, neocortex, or both regions. Four cases had Semiquantitative results are presented in Table 2. Neu-
evidence of hippocampal sclerosis predominantly affect- ronal loss and gliosis of the hypoglossal nucleus and
ing the subiculum. Additional pathologic findings were spinal anterior horn cells were variable and ranged from
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
509
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015Table 2. Semiquantitative Data of Motor and Extramotor Neuron Pathologic Findings in FTLD-MND*
Motor Inclusions Extramotor Inclusions
Neuronal Loss and Gliosis† (Ubiquitin) (Ubiquitin)§
Additional
Case, Cranial Anterior Cranial Anterior CST Dentate Cortical Cortical Hippocampal Pathological
No. Nerve XII Horn Cell Nerve XII Horn Cell Degeneration‡ Fascia Inclusions Neurites Sclerosis Findings
1 0-1 ⫹ 1⫹ No No 4⫹ 3⫹ 1⫹ 1⫹ SUB Mild CAA and
senile changes
2 0 NA No NA 3⫹ 3⫹ 1⫹ 0-1 ⫹ SUB None
3 2 ⫹ (BB) 1 ⫹ (BB) No No 0 3⫹ 3⫹㛳 3⫹㛳 SUB Alzheimer disease
4 1 ⫹ (BB) NA Yes NA 2⫹ 1⫹ 0-1 ⫹ 0-1 ⫹ CA1, SUB None
5 1 ⫹ (BB; LBHI) 1 ⫹ (BB; LBHI) Yes No 1⫹ 1⫹ 0-1 ⫹ 0-1 ⫹ No None
6 1 ⫹ (BB) 2 ⫹ (BB) No Yes 1⫹ 1⫹ 0-1 ⫹ 0 No Muscle neurogenic
atrophy; none
7 1 ⫹ (BB) NA No NA 0 1⫹ 0 0 No None
8 2 ⫹ (BB; LBHI) 2 ⫹ (BB) Yes Yes 4⫹ 2⫹ 1⫹ 1⫹ No None
9 1 ⫹ (BB; LBHI) 1 ⫹ (BB) Yes Yes 4⫹ 1⫹ 1⫹ 1⫹ No Mild CAA
10 2 ⫹ (BB) 2 ⫹ (BB; LBHI) NA No 3⫹ 2⫹ 0-1 ⫹ 0-1 ⫹ No None
11 3 ⫹ (BB; LBHI) 2 ⫹ (BB; LBHI) Yes Yes 1⫹ 1⫹ 1⫹ 0-1 ⫹ No None
12 2 ⫹ (BB) 2 ⫹ (BB; LBHI) No Yes 1⫹ 2⫹ 1⫹ 0-1 ⫹ No None
13 2 ⫹ (BB) 1 ⫹ (BB; LBHI) Yes No 1⫹ 1⫹ 0-1 ⫹ 0-1 ⫹ No Muscle neurogenic
atrophy; none
14 1 ⫹ (BB; LBHI) 3 ⫹ (BB) No Yes 0 2⫹ 1⫹ 0 No None
15 1 ⫹ (LBHI) 2 ⫹ (LBHI) Yes Yes 0 0-1 ⫹ 0 0 No Acute hem infarct;
incidental Lewy
bodies
16 1 ⫹ (BB) 1 ⫹ (BB) No No 1⫹ 1⫹ 1⫹ 1⫹ No None
17 NA 1 ⫹ (BB) NA No 4⫹ 0-1 ⫹ 0-1 ⫹ 0-1 ⫹ No None
Abbreviations: BB, Bunina bodies; CA1, cornu ammonis 1; CAA, cerebral amyloid angiopathy; CST, corticospinal tract; FTLD-MND, frontotemporal lobar
degeneration with motor neuron disease; LBHI, Lewy body–like hyaline inclusions; NA, not able to evaluate; SUB, subiculum.
*Group 1 (cases 1-7); group 2 (cases 8-17).
†For neuronal loss and gliosis, 0 = none; 1 ⫹ = focal neuronal loss and focal microgliosis; 2 ⫹ = extensive neuronal loss with microgliosis and empty cell beds
containing macrophages; 3 ⫹ = almost complete loss of motor neurons with atrophy and astrocytic fibrillar gliosis.
‡For severity of corticospinal tract degeneration, 0 = none; 1 ⫹ = very mild vacuolation and sparse macrophages; 2 ⫹ = vacuolation with many lipid-laden
macrophages; 3 ⫹ = many lipid-laden macrophages with myelin loss; 4 ⫹ = myelinated fiber loss, tract atrophy, and astrocytic gliosis.
§For extramotor inclusions, 0 = none; 0-1 ⫹ = isolated; 1 ⫹ = sparse; 2 ⫹ = moderate; 3 ⫹ = frequent number.
㛳Difficult to exclude Alzheimer disease neurites and inclusions.
A B C
D E F
Figure 2. A range of ubiquitin-positive inclusions in the dentate fascia including granular inclusions that are polarized or circumferential (A-C), as well as
crescent-shaped inclusions (arrows), and round Pick body–like inclusions (arrowheads) (D-F). It should be emphasized that Pick body–like inclusions are the
minority in frontotemporal lobar degeneration with motor neuron disease and granular-type inclusions are the most common (for all figures, hematoxylin-eosin
stain was used unless otherwise noted, original magnification ⫻400).
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
510
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015absent to severe, and the severity of motor neuron patho- lar to amyotrophic lateral sclerosis, and the majority had
logic features tended to correlate with clinical evidence Bunina bodies, which are a histologic hallmark of amyo-
of motor neuron disease (r = 0.63, P⬍.05 for hypoglos- trophic lateral sclerosis. The severity of motor neuron de-
sal nucleus; r=0.57, P=.10 for anterior horn cells). Simi- generation was variable and ranged from absent to se-
larly, corticospinal tract degeneration ranged from ab- vere. We found that some cases had a predominance of
sent to severe. Severity of corticospinal tract degeneration corticospinal tract degeneration (cases 1, 2, 4, 8, 9, 10,
did not correlate with clinical signs of motor neuron dis- and 17), while others had no corticospinal tract degen-
ease or with severity of neuronal loss and gliosis in the eration (cases 3, 7, 14, and 15). Extramotor ubiquitin-
hypoglossal nucleus and spinal anterior horn cells. There positive pathologic findings were minimal overall and
was a weak correlation between severity of corticospi- mostly granular in all cases. Despite these differences, at
nal tract degeneration and cases with cortical ubiquitin- the present time there is no way to distinguish between
positive inclusions (r= 0.50, P⬍.05). Extramotor ubiq- cases on the basis of extramotor ubiquitin-positive patho-
uitin-positive inclusions were absent to sparse in all logic features or on the basis of predominant involve-
cortical regions (except case 3 for which it was difficult ment of upper or lower motor neurons. A larger sample
to exclude Alzheimer disease neurites and inclusions), size would be needed to address possible clinically use-
and absent to moderate in the dentate fascia of the hip- ful subtypes.
pocampus in almost all cases. In only 3 cases with hip- Four of the 7 cases without clinical evidence of mo-
pocampal sclerosis were there frequent inclusions in the tor neuron disease had hippocampal sclerosis, predomi-
dentate fascia. nantly of the subicular region. Hippocampal sclerosis is
a common feature of frontotemporal lobar degeneration
CLINICOPATHOLOGIC CORRELATION with ubiquitin-only immunoreactive changes. 8,9 In
addition, 3 of these 4 cases had frequent ubiquitin-
We divided the cases into the following 2 groups: group positive inclusions in the dentate fascia of the hippo-
1 consisted of those cases that were not clinically diag- campus, which is another common feature of fronto-
nosed as FTD-MND (cases 1-7) and group 2 consisted temporal lobar degeneration with ubiquitin-only
of those that were clinically diagnosed as FTD-MND (cases immunoreactive changes. We therefore argue that FTLD-
8-17). Four of the 7 cases from group 1, but none of the MND should be thought of as a spectrum of diseases and
10 cases from group 2, were found to have hippocampal include FTLD-MND with hippocampal sclerosis and
sclerosis (3 of which also had frequent inclusions in the FTLD-MND without hippocampal sclerosis. Frontotem-
dentate fascia). In addition, the other 3 cases from group poral lobar degeneration with motor neuron disease with
1 (those without hippocampal sclerosis) were found to hippocampal sclerosis seemed strikingly similar to other
have minimal neuronal loss in hypoglossal nucleus and frontotemporal lobar degenerations with some evi-
anterior horn cells as well as absent to minimal cortico- dence of MND, while FTLD-MND without hippocam-
spinal tract degeneration. In contrast, the cases from group pal sclerosis seemed strikingly similar to amyotrophic lat-
2 had moderate to severe neuronal loss in the hypoglos- eral sclerosis with some evidence of FTLD.
sal nucleus and anterior horn cells, moderate to severe Fibers from the subiculum serve as the major output
corticospinal tract degeneration, or a mixture of both. Only center for the hippocampus. Therefore, the cases with
case 16 from group 2 had minimal hypoglossal and an- hippocampal sclerosis predominantly affecting the su-
terior horn cell pathologic features. Spearman rank or- biculum were likely to be more amnestic and impaired,
der correlation confirmed our observations and demon- which may explain why features of motor neuron dis-
strated that cases from group 1 were significantly more ease were not clinically detected in these 4 cases with mod-
likely to have hippocampal sclerosis (r=0.70, P⬍.01). Pa- erate motor neuron degeneration. Two of these 4 cases
tients from group 1 also tended to be female (r = 0.44, were so impaired that a mental status examination was
P=.08) and hippocampal sclerosis was significantly cor- not possible, the third was severely demented with a score
related with female sex (r= 0.67, P⬍.01). of 13 out of 38 on the Short Test of Mental Status,10 and
the fourth was moderately to severely demented with a
score of 21 out of 38.
COMMENT Three of the 7 cases with clinically undetected motor
neuron disease, however, did not have hippocampal scle-
This study demonstrates many important features re- rosis. Semiquantitative analysis in these cases revealed
garding the co-occurrence of frontotemporal lobar de- very mild motor neuron pathological features. There-
generation and motor neuron disease. fore, another reason for inability to clinically detect mo-
As expected, all 17 cases had neuronal loss and gliosis tor neuron disease without the aid of detailed and spe-
affecting the frontal and temporal cortices in keeping with cialized electrophysiologic studies or muscle biopsy may
a diagnosis of frontotemporal lobar degeneration. In ad- be very mild subclincal motor neuron degeneration. Rou-
dition, all cases had pathologic evidence of one form of tine electromyography had been completed in 2 of the 7
motor neuron degeneration. Therefore, they were appro- cases without clinical detection of motor neuron dis-
priately categorized as FTLD-MND. Furthermore, all ease; in 1 case (case 7), electromyographic recordings had
17 cases met pathologic criteria for FTLD-MND.4,7 been taken 6 months prior to death and revealed nor-
The pathologic features of FTLD-MND were vari- mal findings.
able. Most cases had a mixture of lower motor neuron All 17 cases had clinical evidence of frontotemporal
degeneration and corticospinal tract degeneration, simi- impairment and met research criteria for a diagnosis of
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
511
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015FTD.11 Five of the cases also had symptoms of mild for- Institute on Aging, Bethesda, Md, and by the Robert H.
getfulness in addition to the more prominent behav- and Clarice Smith and Abigail Van Buren Alzheimer’s Dis-
ioral features. This is not surprising because memory loss ease Research Programs of the Mayo Foundation.
is not an uncommon symptom or sign in FTD.12 Acknowledgment: Phospho-tau was a gift from Peter Dav-
We also show in this study that when FTD and MND ies, PhD, Albert Einstein College of Medicine, Bronx, NY.
co-occur, signs of MND may not always be present early.
In 2 cases, only features of dementia were noted early in
the disease course and both initially carried a diagnosis REFERENCES
of FTD. Both cases later developed signs of MND. Sur-
prisingly, in 1 of the 2 cases (case 16), there was no evi- 1. Caselli RJ, Windebank AJ, Petersen RC, et al. Rapidly progressive aphasic de-
dence of MND until almost 4 years into the disease course. mentia and motor neuron disease. Ann Neurol. 1993;33:200-207.
Prior studies had suggested that MND typically post- 2. Lomen-Hoerth C, Murphy J, Langmore S, Kramer JH, Olney RK, Miller B. Are
amyotrophic lateral sclerosis patients cognitively normal? Neurology. 2003;
dates the onset of dementia by 6 to 26 months.13,14 This 60:1094-1097.
study extends this interval to approximately 45 months. 3. Lomen-Hoerth C, Anderson T, Miller B. The overlap of amyotrophic lateral scle-
We did not find any cases of spinal cord anterior horn rosis and frontotemporal dementia. Neurology. 2002;59:1077-1079.
cell degeneration without hypoglossal nucleus involve- 4. Lowe J, Rossor MN. Frontotemporal lobar degeneration. In: Dickson DW, ed.
ment and we do not know if such cases exist. Therefore, Neurodegeneration: The Molecular Pathology of Dementia and Movement Dis-
orders. Basel, Switzerland: ISN Neuropath Press; 2003:342-348.
spinal cord harvesting and analysis are of the utmost im- 5. Hodges JR, Davies RR, Xuereb JH, et al. Clinicopathological correlates in fron-
portance for future clinicopathologic studies in cases with totemporal dementia. Ann Neurol. 2004;56:399-406.
combined dementia and motor neuron disease. 6. Josephs KA, Petersen RC, Knopman DS, et al. Clinicopathologic analysis of
frontotemporal and corticobasal degenerations and PSP. Neurology. 2006;
66:41-48.
Accepted for Publication: August 31, 2005. 7. McKhann GM, Albert MS, Grossman M, et al. Clinical and pathological diagno-
Correspondence: Keith A. Josephs, MST, MD, Depart- sis of frontotemporal dementia: report of the Work Group on Frontotemporal De-
ment of Neurology, Mayo Clinic, 200 First St SW, Roch- mentia and Pick’s Disease. Arch Neurol. 2001;58:1803-1809.
ester, MN 55905 (josephs.keith@mayo.edu). 8. Josephs KA, Jones AG, Dickson DW. Hippocampal sclerosis and ubiquitin-
Author Contributions: Study concept and design: Jo- positive inclusions in dementia lacking distinctive histopathology. Dement Geri-
atr Cogn Disord. 2004;17:342-345.
sephs, Parisi, Knopman, Boeve, and Petersen. Acquisi- 9. Hatanpaa KJ, Blass DM, Pletnikova O, et al. Most cases of dementia with hippo-
tion of data: Josephs, Parisi, Knopman, Boeve, and Dick- campal sclerosis may represent frontotemporal dementia. Neurology. 2004;
son. Analysis and interpretation of data: Josephs, Parisi, 63:538-542.
Boeve, Petersen, and Dickson. Drafting of the manu- 10. Kokmen E, Naessens JM, Offord KP. A short test of mental status: description
and preliminary results. Mayo Clin Proc. 1987;62:281-288.
script: Josephs, Parisi, and Petersen. Critical revision of 11. Neary D, Snowden JS, Gustafson L, et al. Frontotemporal lobar degeneration: a
the manuscript for important intellectual content: Josephs, consensus on clinical diagnostic criteria. Neurology. 1998;51:1546-1554.
Parisi, Knopman, Boeve, and Dickson. Obtained fund- 12. Graham A, Davies R, Xuereb J, et al. Pathologically proven frontotemporal de-
ing: Petersen. Administrative, technical, and material sup- mentia presenting with severe amnesia. Brain. 2005;128:597-605.
port: Josephs, Parisi, Boeve, and Dickson. Study supervi- 13. Mitsuyama Y. Dementia with motor neuron disease. Neuropathology.
2000;20(Suppl):S79-S81.
sion: Parisi and Knopman. 14. Mitsuyama Y. Presenile dementia with motor neuron disease in Japan: clinico-
Funding/Support: This study was supported by grants pathological review of 26 cases. J Neurol Neurosurg Psychiatry. 1984;47:953-
P50-AG16574 and U01-AG06786 from the National 959.
Announcement
Visit www.archneurol.com. As an individual subscriber
to Archives of Neurology, you have full-text online access
to the journal from 1998 forward. In addition, you can
find abstracts to the journal as far back as 1975.
(REPRINTED) ARCH NEUROL / VOL 63, APR 2006 WWW.ARCHNEUROL.COM
512
©2006 American Medical Association. All rights reserved.
Downloaded From: http://www.jamafacial.com/ on 03/08/2015You can also read