Cognitive behaviour therapy using the Clark & Wells model: a case study of a Japanese social anxiety disorder patient
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Cognitive Behaviour Therapist: e3, page 1 of 13 PRACTICE ARTICLE
doi:10.1017/S1754470X13000081
Cognitive behaviour therapy using the Clark & Wells model:
a case study of a Japanese social anxiety disorder patient
Naoki Yoshinaga ∗ , Osamu Kobori , Masaomi Iyo and Eiji Shimizu
1 2 3 1
1
Department of Cognitive Behavioral Physiology, Chiba University Graduate School of Medicine,
Chiba, Japan
2
Center for Forensic Mental Health, Chiba University, Chiba, Japan
3
Department of Psychiatry, Chiba University Graduate School of Medicine, Chiba, Japan
Received 12 November 2012; Accepted 12 May 2013
Abstract. Cognitive behaviour therapy (CBT) is widely regarded as an effective
treatment for social anxiety disorder (SAD) in Europe and North America. The
theoretical orientations underlying CBT models and treatment interventions developed
in Western cultures were typically constrained by Western conceptualizations of
SAD. This case study reports on the use of CBT for Japanese SAD, demonstrating
the successful implementation of cognitive techniques grounded in the Clark &
Wells model. The patient was a Japanese female with excessively high standards
for workplace social performance. Therapy mainly comprised case formulation,
behavioural experiments, and opinion surveying based on the Clark & Wells model.
These techniques allowed the patient to reduce the strength of maladaptive cognitions
and lower her excessively high standards for social performance. CBT treatment using
the Clark & Wells model was effective and suitable for Japanese SAD, at least in the
present case. We also discuss the cross-cultural differences of SAD and adaptation of
CBT.
Key words: Cognitive therapy, Japan, single case experimental study, social anxiety
disorder.
Theoretical and research basis for therapy
Cognitive behaviour therapy (CBT) is widely regarded as an effective treatment for social
anxiety disorder (SAD) in Europe and North America (Hofmann & Smits, 2008). CBT was
introduced into Japanese psychiatry in the late 1980s, and awareness of the effectiveness of
CBT has spread, not only among professionals and academics but also among the general
public (Ono et al. 2011). Nevertheless, the number of facilities offering CBT is still limited;
as of 2012, selective serotonin re-uptake inhibitors (SSRIs; fluvoxamine and paroxetine) are
the only treatments covered by insurance for Japanese patients with SAD.
∗ Authorfor correspondence: Dr N. Yoshinaga, Department of Cognitive Behavioral Physiology, Chiba University
Graduate School of Medicine, 1-8-1 Inohana, Chuouku, Chiba, Japan (email: nao@chiba-u.jp).
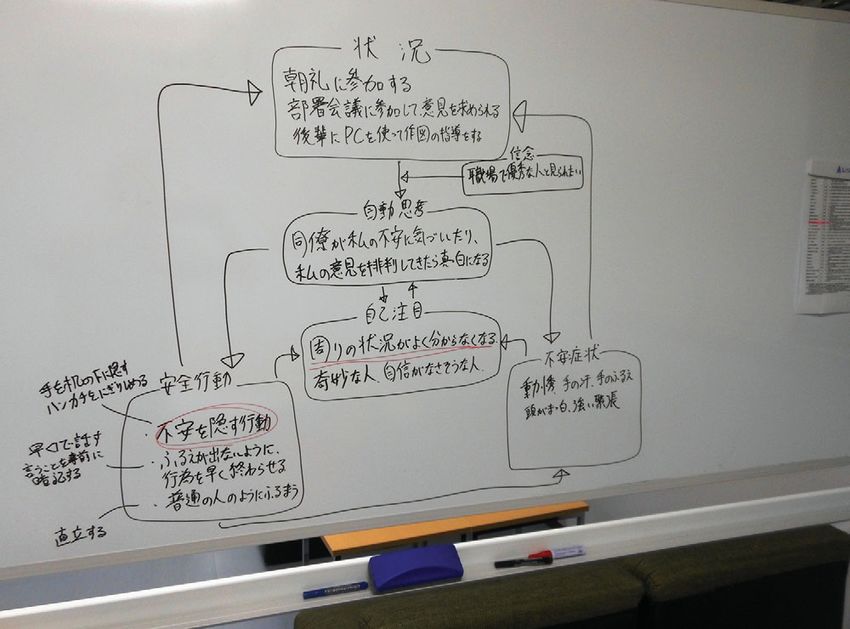
© British Association for Behavioural and Cognitive Psychotherapies 20132 N. Yoshinaga et al. Reports regarding the effectiveness of CBT come mostly from Europe and North America, with theoretical orientations underlying CBT models and treatment interventions typically constrained by Western conceptualizations of SAD. This is problematical, as cultural factors may be especially relevant to SAD pathology. For example, taijin-kyofu-sho (in Japanese, taijin means ‘interpersonal’, kyofu means ‘fear’, and sho means ‘syndrome’), is listed in the appendix to DSM-IV-TR as a ‘culture-bound syndrome’ unique to East Asia. However, fear of interpersonal relationships (e.g. Kleinknecht et al. 1997) can also be classified under existing DSM-IV-TR categories (e.g. Hofmann et al. 2010), and the conceptualization of fear of interpersonal relationships as purely culture-bound does not always hold true. Further, there is little difference between Asian and Western manifestations of SAD; despite differences between the conceptualizations of SAD and taijin-kyofu-sho, SAD patients in different parts of the world have many features in common (Stein, 2009). This paper presents a case study wherein CBT based on the Clark & Wells (1995) model was successfully employed for a Japanese SAD patient. Case summary and main presenting problem The patient, Mika (not the patient’s real name), was a 42-year-old unmarried Japanese woman. She had suffered from social anxiety for 5 years and panic for 10 years. Her presenting problem was ‘I got stage fright performing in front of co-workers’ (e.g. in the monthly depart- mental meeting and daily morning plenary meetings). She experienced a haunting fear that co- workers would notice signs of her anxiety, resulting in a heightened sensitivity to evaluation by co-workers. Although Mika had opinions that she wanted to share in departmental meetings, she avoided any behaviour that might attract attention, simply stating ‘I agree’. In addition, she could not use public transport to come to our hospital because of panic symptoms. Treatment goals included disagreeing and engaging in negotiation without excessive anxiety. She wanted to be able to speak in front of large groups; a concrete goal was to make a speech at a friend’s wedding. Mika also had an unrelated inability to use public transport such as crowded buses or trains, experiencing shortness of breath and stomach discomfort. Treatment consisted of 14 weekly 90-min individual therapy sessions, based on the Clark & Wells model. Sessions were audiotaped, and Mika was encouraged to listen to these recordings as homework. Follow-up sessions were offered 1 month and 6 months after the fourteenth session. Therapy was conducted both inside and outside of the treatment room, and between-session homework was designed in collaboration with the patient. In order to reduce Mika’s self-consciousness and summarize discussions, notes were made on a whiteboard during all sessions (Fig. 1). History At the age of 32, Mika suddenly began to experience intense nausea whenever she boarded the bus. She was referred to a psychiatric clinic and diagnosed with panic disorder. Although she was prescribed paroxetine, she stopped taking it due to nausea. Five years later, while presiding at morning meeting, she suddenly experienced an uncontrollable shaking of her hands so serious that she was unable to hold her notes. She tried various SSRIs and serotonin norepinephrine reuptake inhibitors (SNRIs) but continued to experience severe workplace social anxiety. She experienced heart palpitations and her hands shook just from participating
CBT for Japanese SAD 3
Fig. 1. Using a whiteboard to develop case formulation.
in both departmental and plenary meetings. At this time, she was diagnosed with SAD by her
general practitioner, and was referred to our hospital.
Case assessment
After referral to our hospital, Mika was again diagnosed with SAD and panic disorder by
an experienced psychiatrist, using the Structured Clinical Interview for Axis I Disorders
(SCID-I). She had no comorbid Axis II disorders before starting therapy. She had previously
been treated with duloxetine at 20 mg/day and clonazepam at 1.5 mg/day, and this regimen
remained stable throughout CBT treatment.
Mika had been working for a prestigious construction company as an assistant architect
for 10 years (involved mainly in the design and supervision of the construction of small
buildings). Her highest academic qualification was secondary school. She had experience in
sales for a major automotive company and as a temporary office worker for various companies.
She lived on her own near her office. Her hobbies included reading novels and socializing
with friends. Mika presented no serious social or economic problems at the beginning of
therapy.4 N. Yoshinaga et al.
Fig. 2. Case formulation demonstrating how maladaptive behaviours and cognitions maintain and
exacerbate social anxiety.
Therapist details and supervisory arrangements
The therapist was a Japanese psychiatric nurse, in the first year of a CBT training programme
at Chiba University (Chiba – IAPT training course). The therapist attended weekly group
supervision (60 min) and fortnightly individual supervision (30 min) sessions with the authors.
Multiple supervisors and other trainees supported and assisted in planning sessions.
Formulation
Case formulation was collaboratively developed (see Fig. 2). Typical triggering situations for
anxiety were (a) presiding over or participating in plenary meetings, (b) stating her opinion
or participating in departmental meetings, and (c) instructing junior staff about drawing using
PCs.
In these situations, Mika had automatic thoughts such as ‘I will go blank if co-workers
notice my anxiety, or if they roundly criticize my opinions’. Her belief ‘I always need to look
competent to [my] co-workers’ activated these automatic thoughts.
Automatic thoughts generated somatic symptoms such as heart palpitations and shaking
hands. She also experienced cognitive symptoms; her mind went blank and it was extremely
distressing for her to tolerate the situation.
In response to these symptoms, Mika had the following safety behaviours:
(a) Hiding her anxiety: she would hide her hands under her desk, clench her handkerchief,
and stand upright without touching anything on the desk.CBT for Japanese SAD 5
(b) Finishing performances quickly before her hands could begin to shake: she would speak
quickly, rehearse her words in order to deliver them as briefly as possible, and sympathize
with others’ opinions.
(c) Trying to look normal: she would act as if she was not experiencing anxiety by keeping
an erect posture, keeping her head up, looking around, and smiling.
While desperately deploying safety behaviours, Mika’s attention became increasingly self-
focused, with thoughts such as ‘I cannot understand what is going on around me’. Mika
generated self-impressions such as ‘I imagine that I look suspicious or strange’.
Mika understood the vicious cycle of these safety behaviours: ‘I knew that I had to listen
to others’ opinions in order to give accurate opinions, but I could not pay attention because
I was so wrapped up in performing my safety behaviours . . . Thinking about my panic and
paying attention to myself may be strengthening my bodily symptoms of panic. For example,
while chatting with my friend on the bus, I did not worry about possible stomach discomfort.’
Here, case formulation relating to panic was intentionally left undeveloped in order to avoid
confusion with Mika’s social anxiety. Mika’s worst fear when stomach discomfort occurred
on public transport was that she would ‘faint and collapse’; she would experience this fear
even when there were no people around her. Therefore, the therapist acted on the assumption
that her stomach discomfort was not directly related to SAD.
Mika understood that her safety behaviours were increasing her self-focused attention
and reducing awareness of social cues, such as other people’s responses. She was also
aware that her self-monitoring of somatic sensations could increase perceived intensity of
symptoms.
Course of therapy and assessment of progress
Training in external focusing and attention shifting
Although her stomach discomfort was not directly related to SAD, Mika had to use public
transport to attend treatment. Therefore, the therapist prioritized her panic problems during the
first session. Mika was encouraged to alternate between an internal and external focus while in
the session room. Outside of social situations, this could be accomplished using all five senses.
Following initial training, she reflected on the role that attention may have played in her panic
using public transport: ‘Self-focused attention would better enable someone to notice small
changes in sensation, such as heart palpitations and shaking hands’. After practising in the
safety of the session room, Mika practised maintaining an external focus in anxiety-producing
situations, such as the bus. Exercises in maintaining an external focus prevented her from
focusing on her own somatic sensations, helping her to avoid generating heart palpitations,
stomach discomfort, or strong anxiety. Homework assignments were collaboratively planned
to practice maintaining an external focus in feared situations (e.g. the bus, the train, morning
meetings). Mika was gradually able to use the bus and train to come to the hospital for
her sessions, but was unable to prevent self-focused attention and strong anxiety during
morning meetings. Central issues related to managing social anxiety produced by the self-
image generated by self-focused attention were not discussed at this stage of treatment. This
attentional training was intended as an intervention for her panic problems, not as part of her
treatment for social anxiety under the Clark & Wells model.6 N. Yoshinaga et al.
Behavioural experiments: safety behaviours and videotaped feedback
Role-plays depicting realistic hypothetical situations, in which she was chairing plenary
meetings, stating her opinion in a departmental meeting, instructing junior staff about drawing
using PCs, etc., were performed, both with and without Mika engaging in safety behaviours
and self-focused attention. Through this role-playing, Mika understood that ‘I felt unexpect-
edly worse when I performed safety behaviours and engaged in self-focused attention’. Mika
speculated that safety behaviours might actually make her appear stranger to colleagues.
During the following session, Mika watched a video of the previous session, and compared
how she expected that she would appear with how she actually appeared. As she had
speculated during the previous session, safety behaviours (such as standing ramrod straight)
made her appear even more anxious than she actually felt. Mika confirmed that her safety
behaviours had the opposite effect than what was intended. Mika expressed interest in further
experimentation, and was curious to know ‘How do I look on video when I feel as if my
hands are shaking violently?’ Mika demonstrated her most extreme hand shaking, expecting
this to appear as violent spasms in the video. However, neither she nor her therapist noticed
her hands shaking at all. On the basis of these discoveries, homework assignments were as
follows:
(a) Observe whether anyone noticed her hands shaking at lunch.
(b) Observe whether her supervisor noticed her hands shaking when she handed in
documents.
Results of homework (a) are presented in Table 1. Only her friend, who knew she had
SAD, whispered ‘Are you OK?’ but few co-workers commented. As for homework (b), her
superior just accepted her documents and ignored the fact that her hands were shaking. Mika
learned that fewer people noticed her anxiety than she had expected, modifying her negative
assumptions to match reality. However, Mika worried that people were just not saying what
was on their minds, and that this experiment did not reveal the true extent of their judgmental
thoughts, limiting the value of this behavioural experiment.
Behavioural experiments: stating different opinions
As Mika always agreed with co-workers’ opinions to avoid criticism or attention, she and the
therapist agreed that it was premature to practice role-playing disagreeing in feared situations.
Instead, the therapist encouraged Mika to disagree on neutral topics such as favourite foods.
Through this role-play, Mika realized that both social and business conversations are more
animated when people have differing opinions, and that agreeing with the other person
feels boring. Mika also realized that she did not endanger relationships by changing prior
opinions. Maladaptive cognitions were progressively refuted through behavioural experiments
and homework, becoming more aligned with consensus reality.
Opinion survey to follow-up behavioural experiment
Mika completed an opinion survey to directly test negative predictions about what other
people thought of her behaviours. Mika and the therapist collaboratively designed the
following original questionnaire:CBT for Japanese SAD 7
Table 1. Example sheet from a behavioural experiment
Situation
• When I had lunch with co-workers, I showed symptoms of anxiety during conversation
Prediction
• Co-workers will notice and point out my anxiety (Belief: 70%)
• If co-workers notice my anxiety, they will make fun of me (Belief: 30%)
Experiment
• Lift a bottle to my lips while my hands are shaking
• Note the direction of co-workers’ eyes and how they respond
Outcome
• The only response was that my friend whispered, ‘Are you all right?’
• The other co-workers neither watched my hands nor pointed out that they were shaking – they just
continued to enjoy chatting
What I learned
• My friend was the only person who was aware that my hands were shaking; this was only because
she knew that I had social anxiety and was more attuned to my symptoms than other people (Belief:
80%)
• Fewer people are able to notice my anxiety symptoms than I think (Belief: 60%)
• Co-workers actually noticed my anxiety, but they decided not to say anything. (Belief: 50%)
‘Belief: 70%’ indicates that the patient was 70% certain of the accuracy of this belief.
(a) When you notice someone experiencing anxiety or becoming nervous, what do you think
about him/her?
(b) If someone who is a good worker and an excellent public speaker seems to be anxious
one day, what do you think about him/her?
Survey results helped Mika realize that most people do not pay attention to others’ anxiety,
nor do they judge others’ professional abilities based on anxiety. Most people do not have
critical thoughts, but sympathetic and supportive ones, and if a competent person looked
anxious, this did not damage others’ opinions of him/her. This led Mika to a breakthrough
in understanding: it is impossible to know what others really think, and attempts at mind
reading are just tiring and never accomplish anything useful. Thus, the opinion survey was
able to address points that the behavioural experiment was not able to accomplish.
The opinion survey modified Mika’s maladaptive belief ‘If I do not conceal my anxiety,
I will be evaluated poorly by my colleagues’. Further discussion modified her excessively
high standards for social performance, transforming ‘I have to maintain my image of being an
expert at all times’ to ‘I do not mind being considered incompetent by my colleagues’ and ‘I
can now accept my inability to be perfect and show my real self’.
Discussion about excessively high standards for social performance
The therapist and Mika discussed how her excessively high standards for social performance
(e.g. ‘I have to maintain my impression of being a competent at all times’) had developed.
Mika listed the following possible causes:
(a) Feeling inferior about her lack of academic achievements compared with co-workers of
the same age.8 N. Yoshinaga et al.
Fig. 3. Scores on (a) the Liebowitz Social Anxiety Scale (LSAS), and (b) the Panic Disorder Severity
Scale (PDSS).
(b) Belief that she should perform much better than other newcomers due to her previous
architectural experience. This belief was compounded by the fact that she was older than
other co-workers who had entered the company at the same time as she had.
Mika and her therapist discussed the gap between traditional Japanese social norms,
which emphasize educational background, age, and seniority, and modern social norms in
prestigious companies, which increasingly value meritocracy over seniority. Mika and her
therapist talked about her professional experience and what values she held about meritocracy
and seniority. Through these discussions, she discovered the following perspectives, which
directly contradicted her grounds for feeling inferior:
(a) Not all workers with prestigious educational backgrounds perform better than others;
Mika had earned several awards for outstanding performance, even though she did not
have a prestigious background.
(b) Most workers placed little emphasis on their colleagues’ age or how many years they had
worked for the company.
This session demonstrated the ways in which the traditional social norms held by Mika
differed from more salient modern social norms, modifying her maladaptive beliefs and
helping her to transcend her shame regarding her academic background, age, and seniority.
Mika was able to accept herself despite her imperfections, realizing that the strain of always
acting supremely competent and confident was exhausting.
Treatment outcome
Self-reported symptoms of social anxiety were measured using the Liebowitz Social Anxiety
Scale (LSAS; Liebowitz, 1987) and severity of panic was measured using the Panic Disorder
Severity Scale (PDSS; Shear et al. 1997). Over a period of 14 sessions, total LSAS scores
decreased from 86 to 30 and the PDSS total score decreased from 11 to 0 (Fig. 3a, b).
Through CBT, Mika realized that
(a) It is more difficult for observers to detect her anxiety than she thought.CBT for Japanese SAD 9
(b) Most people neither paid attention to others’ anxiety nor judged others for experiencing
anxiety.
(c) Conversations are more animated when participants state differing opinions, and immedi-
ately agreeing with the other person makes the conversation boring.
(d) Not every worker with a prestigious educational background performs a highly skilled
function.
(e) Nobody is perfect.
Mika also made the decision to enrol in a class at her local gym, even if it involved a fitness
recital. Since she could once again use public transport, her range of activity was expanded
and her social life became richer (e.g. she visited a friend who lived far away).
Complications or innovations in therapy
First, as SAD is directly linked to culturally dependent social standards and role expectations
(Draguns & Tanaka-Matsumi, 2003), therapists sometimes need to challenge social norms in
order to address patients’ maladaptive beliefs. For instance, until well after the Second World
War, Japanese companies had a norm of lifetime employment, with promotion tied entirely
to seniority. However, following the collapse of the economic bubble in the 1990s, many
companies replaced seniority with meritocracy, causing a radical shift in professional social
norms. Some workers in Japan, such as Mika, are caught in a dilemma between these two
norms, uncertain about how to reconcile conflicting expectations. This conflict is heightened
by social anxiety and always trying hard to meet group standards.
Second, in the behavioural experiments, the therapist encouraged Mika to observe only
others’ immediate reactions. Our behavioural experiments should have been designed so
as to observe not only immediate reactions, but also long-term reactions or relationships,
since patients sometimes cannot detect clear responses from others in the short term. This
is exacerbated by the fact that Japanese people are less likely than Westerners to express
themselves directly, tending to employ vague expressions (e.g. Klopf & Cambra, 1979) and
to conceal their true thoughts and feelings. Thus, even in the absence of the feared response
(e.g. criticism or disgust) in the behavioural experiment, patients might conclude that the
other person was simply hiding these feelings. For this reason, Mika reported that the opinion
survey was a more useful tool for reducing maladaptive assumptions and beliefs. This may
suggest that the opinion survey is a more useful option if patients predict that the feared
consequence will take a long time to manifest, such as a slowly spreading rumour or negative
opinion of their character.
Case management considerations
As of 2012, 70% of medical expenses are covered by national health insurance in Japan.
In April 2010, CBT for mood disorders was approved by the Japanese national health
insurance authorities, but many important issues remain to be addressed. Only clinicians
are able to provide CBT, and they can provide CBT only for mood disorders; other mental
health problems, such as SAD, are not covered. This makes it difficult for middle-class or
working-class SAD patients to receive intensive psychotherapy. Mika received CBT free of
charge as she was a participant in our clinical trial, and she did not require additional case10 N. Yoshinaga et al. management such as coordination with community mental health services, health insurance, or other supportive services. Follow-up Two 10-min follow-up sessions were held at 1 and 6 months following treatment. Follow-up sessions confirmed that social anxiety and panic had not recurred. Mika expanded her range of activity and her social life became more enjoyable – she was able to attend meetings without feeling too anxious, and even attended a pop concert. Self-reported LSAS and PDSS scores remained low at 1- and 6-month follow-up intervals (Fig. 3a, b). Therapy implications of the case This case presentation offered in-depth examples of case formulation and treatment tech- niques, including understanding and manipulating safety behaviours, self-focused attention, and negative self-image; planning and conducting behavioural experiments; and conducting an opinion survey. CBT was demonstrated to be effective for a Japanese SAD patient in reducing fear of social censure by reducing the strength of maladaptive cognitions and modifying excessively high standards for social performance. Moreover, a comorbid panic problem that arose when the patient used public transport was successfully alleviated through training in maintaining an external focus during the first session. Similar assessments and treatments for typical SAD have been utilized worldwide. Multiple assessments for SAD severity developed in Western cultures have been translated and standardized for use in Japan (e.g. LSAS, Social Phobia and Anxiety Inventory, Social Phobia Scale, Social Interaction Anxiety Scale). Additionally, clinical trials have indicated that individual and group CBT, originally developed in Western countries, could significantly reduce SAD severity in Japanese patients (Watanabe et al. 2010; Yoshinaga et al. 2013). Recommendations to therapists Current case presentation This case study presented a detailed argument that CBT developed in Western cultures may be effective for Japanese SAD patients. Although we presented this point in a Japanese context, our study has the following important implication for an international audience: behavioural experiments and opinion surveys for use in any culture need to be designed more carefully, particularly when patients worry that others are concealing their true feelings and thoughts. Offensive-subtype SAD Offensive-subtype SAD (most notably taijin-kyofu-sho), a variety of SAD more frequently seen in collectivist cultures such Asia, South America, the Pacific Islands, and Southern European countries, needs more attention. In collectivist cultures, harmony within the group is a higher priority than fulfilling individual goals, and norms and role expectations have a considerable impact on behaviour. Although SAD and taijin-kyofu-sho have many features in common (Stein, 2009), offensive-subtype SAD is concerned primarily with offending or
CBT for Japanese SAD 11 embarrassing another person, or otherwise disturbing the group atmosphere, and not with em- barrassing one’s self. A case can be made for interpreting this stronger fear of offending others in terms of culturally determined child-rearing practices and the early childhood environment in Japan. Japanese parents often say things like ‘Look around before you act’ and ‘care about others’ feelings and put them first’. They emphasize the importance of empathy, obligation, and meeting others’ expectations. Therefore, Japanese children tend to be discouraged from making their wishes known; instead, they rely on others to sense and meet their needs (Roland, 1988). Offending fear may, therefore, be easily provoked by Japanese collectivism and child- rearing culture. Offensive-subtype SAD patients often struggle to determine the right things to say, when to say it, and whose opinion they should not disagree with; they excessively fear diverging from group norms or disrupting the group atmosphere. When planning a behavioural experiment, therapists may want to ask what the worst-case scenario would be if the patient diverged from the group norms or disrupted the group atmosphere. In our clinical experience, patients often say something like ‘I know other people may not respond negatively and our relationship may not change even if I do something that separates me from group norms or disrupts the group atmosphere, but I would feel guilty and like a bad person if I did’. If the patient expresses such guilty or depressed feelings rather than fear or anxiety, therapists might consider employing cognitive restructuring techniques, in order to reconsider how bad it would be for them to be different and/or to act differently. Further clinical research and case presentations need to explore how to design behavioural experiments and adapt CBT for offensive-subtype SAD so as to better serve patients from collectivist societies. Therapeutic relationship with Japanese patients Finally, we describe differences in the patient–therapist relationship between Western countries and Japan. The expected role and view of the therapist varies by culture (Jenkins, 1990): in the UK, the basic assumption is that although a therapist may form a therapeutic alliance with patients or their families, patients and therapists remain separate individual entities. The therapist is basically regarded as a supporter, assisting patients in solving their own problems. In contrast, Japanese patients tend to view the therapist as an authority figure who directs them in the right way, and they tend to deify the therapist. For example, Japanese patients usually address therapists not by their first names, but by their surnames and/or the honorific sensei (a title of respect widely used for teachers, doctors, lawyers, and members of parliament). The therapist is basically regarded as a director; and therapists are expected to solve patients’ problems using therapeutic interventions. Culturally, Japanese patients often depend excessively on their therapists, and tend to entrust treatment-related decisions to their therapists and psychiatrists (Munekata, 1986; Higuchi, 1992). This Japanese conceptualization of the therapist–patient relationship has some advantages. It sets a clear boundary in the therapeutic relationship, preventing the patient and therapist from becoming too close; it also makes the therapist’s advice more authoritative, making it easier for patients to try challenging tasks such as behavioural experiments in feared situations, and motivating patients to attend sessions. However, it also has disadvantages, a major one being that patients tend to remain passive in their treatment, and may be afraid to express what is on their minds. They feel strong pressure not to inconvenience their therapists or make them uncomfortable; for example, patients may attend sessions even when they are feeling very ill. In our clinical experience, patients sometimes appeal to administrative staff
12 N. Yoshinaga et al. such as, ‘My therapist does not understand how I feel. I have difficulty with the homework, but I can’t tell my therapist because it might make therapist uncomfortable or embarrassed’. If patients in treatment for SAD deify their therapists, those patients may become afraid of their therapists and conceal their feelings; offensive-subtype SAD sets the stage for an especially strong fear of displeasing or disappointing the therapist. For these reasons, therapists must be aware of tendencies in the therapeutic alliance, especially when working with native Japanese patients. Declaration of Interest None. Recommended follow-up reading Hofmann SG, Anu Asnaani MA, Hinton DE (2010). Cultural aspects in social anxiety and social anxiety disorder. Depression and Anxiety 27, 1117–1127. Stein DJ (2009). Social anxiety disorder in the West and in the East. Annals of Clinical Psychiatry 21, 109–117. References Clark DM, Wells A (1995). Social Phobia: Diagnosis, Assessment, and Treatment. New York: Guilford Press. Draguns JG, Tanaka-Matsumi J (2003). Assessment of psychopathology across and within cultures: issues and findings. Behaviour Research and Therapy 41, 755–776. Higuchi N (1992). The patient’s right to know of a cancer diagnosis: a comparison of Japanese paternalism and American self-determination. Washburn Law Journal 31, 455–473 Hofmann SG, Asnaani A, Hinton DE (2010). Cultural aspects in social anxiety and social anxiety disorder. Depression and Anxiety 27, 1117–1127. Hofmann SG, Smits JAJ (2008). Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. Journal of Clinical Psychiatry 69, 621– 632. Jenkins H (1990) Csalad therapia: family therapy training in Hungary. Association for Child Psychology and Psychiatry Newsletter 12, 9–13. Kleinknecht RA, Dinnel DL, Kleinknecht EE, Hiruma N, Harada N (1997). Cultural factors in social anxiety: a comparison of social phobia symptoms and Taijin kyofusho. Journal of Anxiety Disorders 11, 157–177. Klopf DW, Cambra RE (1979). Communication apprehension among college students in America, Australia, Japan, and Korea. Journal of Psychology 102, 27–31. doi:10.1080/00223980.1979. 9915091 Liebowitz MR (1987). Social phobia. Modern Problems of Pharmacopsychiatry 22, 141–173. Munekata T (1986). Japanese attitudes toward mental illness and mental health care. In: Japanese culture and behavior. (ed. T. Lebra T & W. Lebra), pp. 369–378. Honolulu: University of Hawaii Press. Ono Y, Furukawa TA, Shimizu E, Okamoto Y, Nakagawa A, Fujisawa D, Nakagawa A, Ishii T, Nakajima S (2011). Current status of research on cognitive therapy/cognitive behavior therapy in Japan. Psychiatry and Clinical Neurosciences 65, 121–129.
CBT for Japanese SAD 13
Roland A (1988). In Search of Self in India and Japan: Toward a Cross-cultural Psychology. New
Jersey: Princeton University Press.
Shear MK, Brown TA, Barlow DH, Money R, Sholomskas DE, Woods SW, Gorman JM, Papp LA
(1997). Multicenter collaborative panic disorder severity scale. American Journal of Psychiatry 154,
1571–1575.
Stein DJ (2009). Social anxiety disorder in the West and in the East. Annals of Clinical Psychiatry 21,
109–117.
Watanabe N, Furukawa TA, Chen J, Kinoshita Y, Nakano Y, Ogawa S, Funayama T, Ietsugu T,
Noda Y (2010). Change in quality of life and their predictors in the long-term follow-up after group
cognitive behavioral therapy for social anxiety disorder: a prospective cohort study. BMC Psychiatry
10, 81.
Yoshinaga N, Ohshima F, Matsuki S, Tanaka M, Kobayashi T, Ibuki H, Asano K, Kobori O,
Shiraishi T, Ito E, Nakazato M, Nakagawa A, Iyo M, Shimizu E (2013). A preliminary study
of individual cognitive behavior therapy for social anxiety disorder in Japanese clinical settings: a
single-arm, uncontrolled trial. BMC Research Notes 6, 74.
Learning objectives
(1) CBT developed in Western cultures may be effective for Japanese SAD patients.
(2) Behavioural experiments and opinion surveys need to be designed more carefully
for Japanese persons, as they are less likely to express themselves directly; rather,
they tend to employ vague expressions and to conceal their true thoughts and
feelings.
(3) Further clinical research and case presentation are needed to clarify how to design
behavioural experiments and adapt CBT especially for offensive-subtype SAD.
(4) Therapists must be aware of tendencies in the therapeutic alliance, especially when
working with native Japanese patients.You can also read