Complete Remission of Widely Metastatic Melanoma: A Case Report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Complete Remission of Widely Metastatic
Melanoma: A Case Report
Mitchell Gaynor, MD, et. al.*
Melanoma has the potential to metastasize to any organ in the body.
Patients with metastatic melanoma usually have a median survival of
6-9 months. A complete response was achieved when low dose IL-2 and GM-CSF
were combined with high doses of intravenous vitamin C and
glutathione, low doses of Temodar administered on a metronomic schedule, with
magnolia extract. The clinical, radiological and histopathological features are
discussed.
Melanoma has the potential to metas- pain. On physical exam, the patient ap- patient had another large metastatic lesion
tasize to any organ in the body Patients peared toxic and was febrile. There was a in her left leg. She underwent a biopsy and
with metastatic melanoma usually have a 5x7cm, multilobulated, exophytic tumor debulking of a metastatic melanoma in the
median survival of 6-9 months. We report with necrosis overlying the skin of the left superficial dermis with clear margins. She
a complete remission in an 80-year-old anterior tibial region. A number of smaller had a CT scan of the chest, abdomen and
patient with malignant melanoma. The cutaneous metastases were present proxi- pelvis in September 2010 that revealed a
patient presented with pulmonary metasta- mally (Figure 1). 7x9 mm nodule at the right lung base con-
ses and a history of multiple resections for She had inguinal lymphadenopathy and sistent with new metastasis (Figure 2).
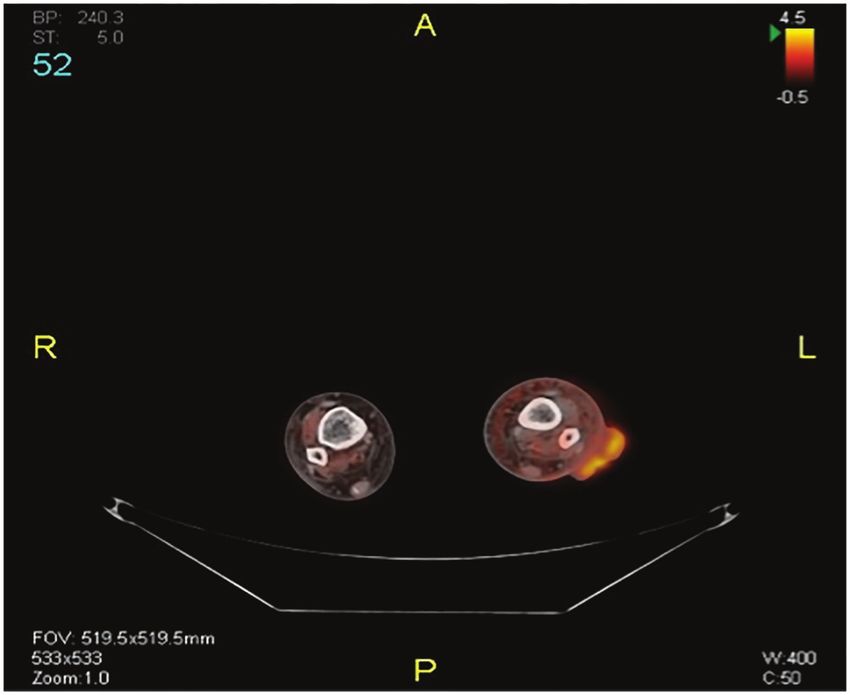
local recurrence and in-transit metastasis. 4+ edema of the left lower extremity. The MRI of the left calf showed several new
The following case seems worthy of a re- tumor was inflamed with exudative weep- subcutaneous tumor deposits consistent
port because of a CR (complete response) ing along with erythema and swelling in with in-transit metastasis (Figure3).
when low dose IL-2 and GM-CSF were the surrounding area. After refusing ipilimumab because of po-
combined with high doses of Intravenous The patient’s relevant medical history tential side effects, the patient presented at
vitamin C and glutathione, low doses of dates from 2006 when she noted a lump our integrative clinic to discuss treatment
Temodar administered on a metronomic in her left leg near the heel. She initially options for the progression of her disease.
schedule, with magnolia extract. The clini- deferred evaluation of this, but eventually She was initially started on antibiotics (Cef-
cal, radiological and histopathological fea- presented to a dermatologist where on Oc- triaxone and Levofloxacin for severe left
tures are discussed. tober 2006, she had a biopsy of the lesion lower extremity cellulitis). A week later,
that showed invasive melanoma. Subse- leukine (250 mcg SQ twice weekly), vi-
Case Presentation quently, she underwent a surgical consul- tamin C (50 grams IV weekly), proleukin
An 80-year old female with a past medi- tation and later a wider excision with a (1million units SQ twice weekly), temozol-
cal history of stage IV melanoma meta- sentinel node biopsy. The pathology report amide (20 mg 5 days per week), acitretin
static from a left foot primary with multiple from the heel specimen described residual (25mg orally three times per week) and
prior resections of in-transit metastasis and malignant invasive melanoma in situ and Magnolia extract 200 mg (containing 90%
right lung metastasis presented to the clinic invasive to a Breslow depth of 2.4 mm of honokiol and magrolol) daily by mouth,
on Dec 2011. She complained of extreme thickness, Clark level IV. Surgical margins were added to her treatment regimen. The
weakness, pruritus, rashes and left heel were clear, and the tumor was noted to be patient slowly improved over a few weeks
present throughout the cicatrix. The sen- as her cellulitis resolved. The vitamin C
Figure 1 tinel node biopsies from the left inguinal was given weekly for one year and con-
5x7 cm. exophytic, fungating, necrotic mass
over the left anterior tibial area prior to
area were negative for metastatic disease. tinued every other week since September
therapy. The patient had no evidence of disease 2010. Glutathione 3000 mg. was given IV
over the next 2 years. By Novem- weekly for one year and continued every
ber 2008, she underwent an FNA other week since September 2010. The
biopsy of a left heel nodule near leukine and proleukin were continued
her initial resection site that con- twice weekly since September 2010. After
firmed metastatic melanoma. On 3months of treatment, the patient under-
December 2008, she underwent went PET- CT of the body and extremities
a left heel excision of a recurrent in April 2012 that demonstrated significant
melanoma lesion. The patient 6 resolution of previous metastatic lung le-
months later developed in-transit sion (Figure 4) and complete resolution of
metastases, which led to mul- the subcutaneous and superficial lesions in
tiple small subcutaneous nodules her left leg (Figure 5).
along the left anterior shin for Follow up PET-CT on October 2012 re-
which she had a biopsy that also vealed no evidence of metastatic disease.
confirmed metastatic malignant There has been complete regression of
melanoma. In February 2010, the the metastatic melanoma lesions in the
Reprint - Cancer Strategies Journal - Spring 2014 - www.cancerstrategiesjournal.com 1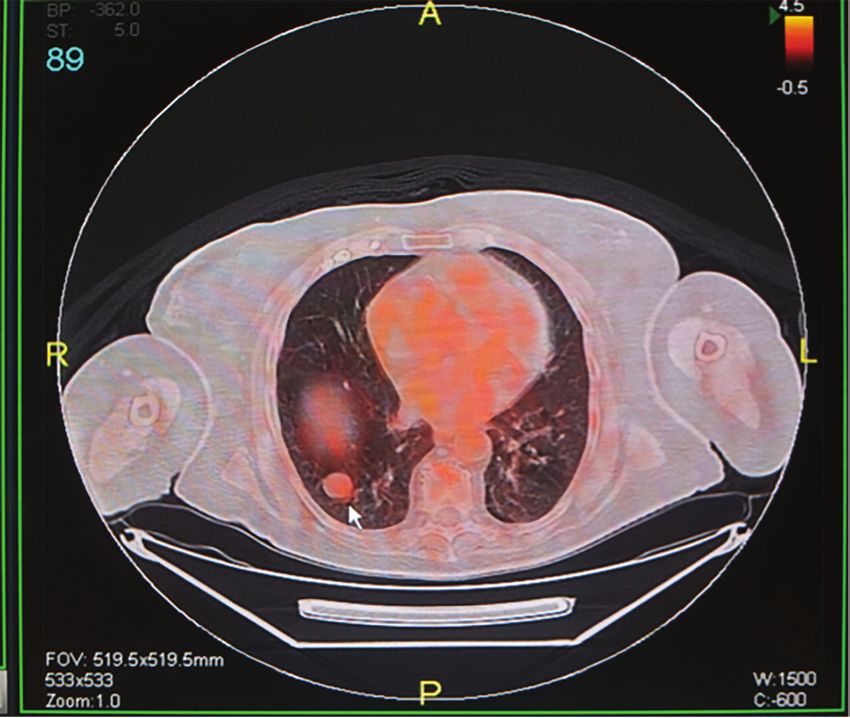
stage IV disease, the sites of cancer cell types are killed only at con-
metastasis and level of lac- centrations approaching Mm range.13 As
tate dehydrogenase are the established by seminal studies by Chen et
most important predictors of al, vitamin C in concentrations higher than
survival. Patients with distant 1Mm can cause build up of hydrogen per-
skin or subcutaneous sites or oxide (H2O2) which is preferentially toxic
distant lymph nodes have towards tumor cells.14 Though the mys-
1year survival rate of 59%. tery of cytotoxicity to cancer cells remain
Patients with lung metastasis unsolved, possibilities include stimulatory
have a 10-year survival rate effects on apoptotic pathways, accelerated
of less than 47%, whereas pro oxidant damage that cannot be re-
patients with metastasis to paired by tumor cells and increased oxida-
other visceral sites like the tion of ascorbic acid at high concentration
brain have a 10 year survival in plasma to unstable metabolite dehydro-
rate of < 30%.5 Cutane- ascorbate which can be toxic. Overexpres-
ous melanoma metastasizes sion of COX2, VEGF (a potent angiogenic
more commonly to the lungs. factor) and type I insulin like growth factor
Figure 2 A single focus of pulmonary (IGF) receptor are important for prolifera-
Chest CT scan showing 7x9 mm. pulmonary metastasis is associated with a better sur- tion and protection from apoptosis in ma-
nodule (shown by arrow) at right lung base sus-
picious for potential metastasis from primary vival than presence of multiple foci. Treat- lignancies.15,16 When vitamin C is used in
melanoma in the left lower leg. ment of melanoma in its early stages is the treatment of malignant melanoma, it
predominantly surgical and consists of ex- suppresses proliferation of melanoma cell
left lower leg (Figure 6). Currently, the pa- cision of primary tumor with a 1-2 cm mar- line SK MEL2 via down regulation of IGF
tient’s clinical status remains excellent as gin and radical lymphadenectomy if the expression, inhibition of COX2 expression
she continues in complete remission. sentinel lymph nodes harbor metastasis. and therefore suppression of VEGF pro-
Ipilimumab is a biologic response modifier duction. There have been several reports
Discussion which blocks cytoxic T-lymphocyte antigen of clinical evidence that has shown benefits
Malignant melanoma (MM) is a fatal cu- 4 has an overall response rate of 11% and of combining Ascorbate with chemothera-
taneous neoplasm, arising from the pig- improved median overall survival from 6.4 py.17
ment producing cells (melanocytes) of the months to 10.1 months for patients with Glutathione is an abundant natural tri-
epidermis. Of the seven most common metastatic melanoma.6 Patients with meta- peptide found within almost all cells. It is
cancers in the US, melanoma is the only static disease with BRAF V600E mutation an important antioxidant that prevents
one whose incidence is increasing. Be- have an average progression free response damage to important cellular component
tween 2000 and 2009, incidence climbed (PFS) of 6.7 months, compared to 2.9 caused by reactive oxygen species such
1.9 percent annually.1 Melanoma accounts months in controls7,8 and a 50% response as free radicals and peroxides. It is also
for less than five percent of skin cancer rate utilizing BRAF mutation specific inhib- involved in the modulation of immune re-
cases, but the vast majority of skin cancer itors such as vemurafenib and dabrafanib. sponse and detoxification of xenobiotics. In
deaths.2 It is usually described as an ir- Regarding its role in cancer treatment, healthy living cells and tissues, more than
regular dark skin lesion that may have ar- vitamin C has been debated for many 90% of total glutathione is in the reduced
eas of varying color in sun-exposed areas years. Emerging evidence indicates that state (GSH) and less than 10% exists in di-
or in unexposed areas. Early diagnosis is ascorbic acid in cancer treatment deserves sulfide form (GSSG). An increase in GSSG
crucial, as metastatic or advanced disease re-examination. Cameron and Pauling re-
is associated with poorer prognosis. The ported in 1976 and 1978 that high dose Figure 3
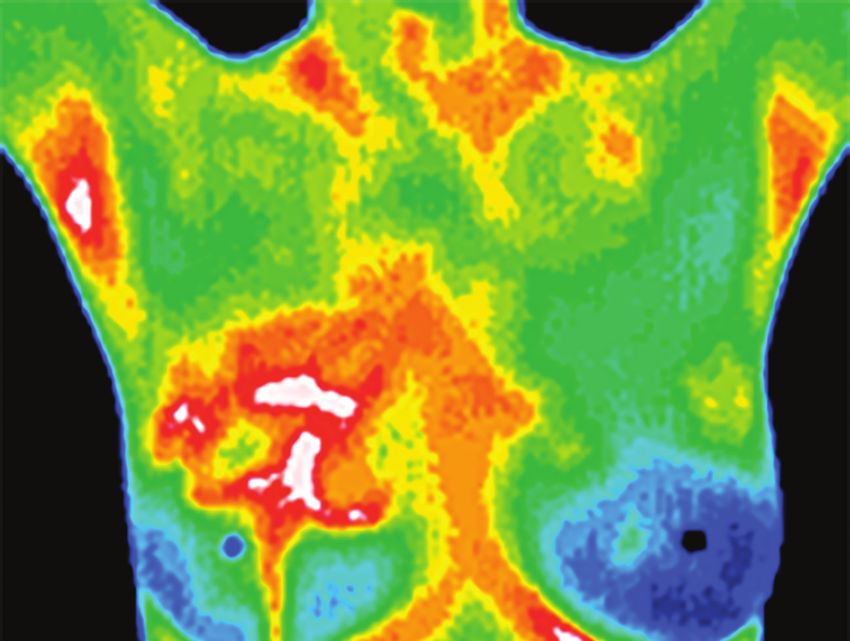
MRI combined with PET-CT of the extremities
commonest site of presentation for men vitamin C (typically 10gms/day by IV in- showing in-transit metastasis of melanoma in
tends to be the trunk, and for women is the fusion for about 10days and thereafter the left lower leg represented by
lower limb.3 orally) increased the average survival of hyper-metabolic yellow areas.
The most common cause of death in advanced cancer patients
melanoma is widespread metastasis.4 Stag- and for a small group of
ing in melanoma is based on primary tu- responders, survival was
mor thickness, ulceration, lymph node and increased up to 20 times
distant metastasis. The American Joint longer than controls.9 Cam-
Commission on Cancer (AJCC) TNM eron and Pauling suggested
system is the most commonly used mela- that Vitamin C increased
noma staging system. Stage I and II of this extracellular collagen and
system are comprised of patients without strengthened the extracel-
regional or distant metastasis. Stage III pa- lular matrix, thus walling in
tients have metastasis either in the regional tumors.10 Laboratory data
lymph nodes or intra-lymphatic sites. Stage show that ascorbic acid is
IV patients have visceral metastasis in dis- toxic to a variety of cancer
tant sites. The thickness and ulceration of cell lines.11,12 Extracellular
melanoma are important in criteria assess- concentrations as low as
ing survival in patients with localized dis- 100-200µM are toxic to
ease (Stage I and Stage II). In patients with some cell lines, but many
2 Reprint - Cancer Strategies Journal - Spring 2014 - www.cancerstrategiesjournal.com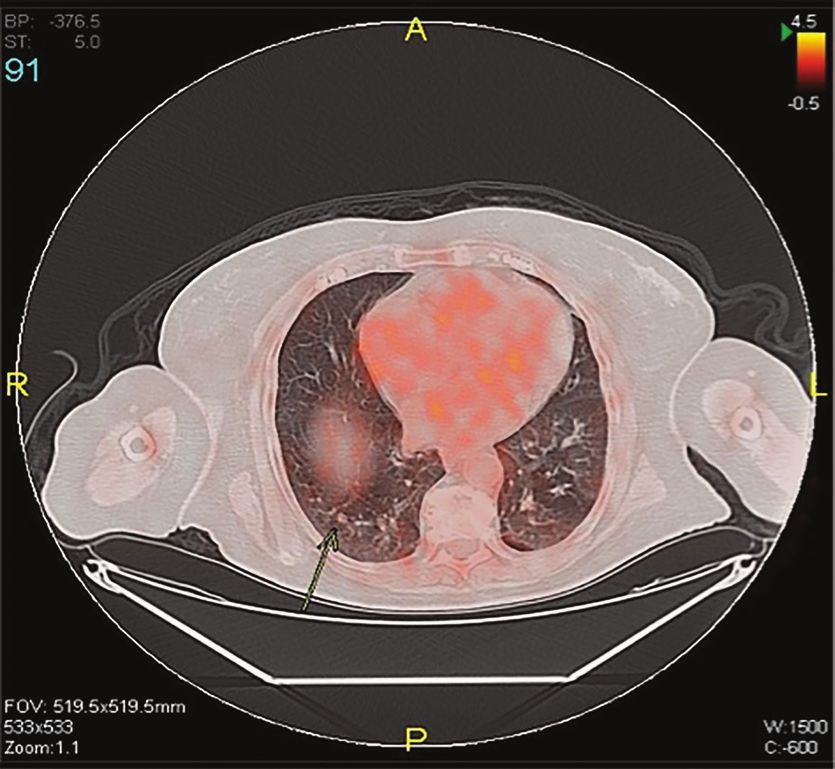
to GSH ratio is considered oxidative stress, (MMP-9), vascular endothelial
which is implicated in cancer progression.18 growth factor (VEGF), and cell
The intracellular depletion of glutathione cycle regulatory genes (cy-
leading to cell death has been extensively clin D1 and c-myc). Honokiol
researched for decades. GSH levels in hu- downregulates the expres-
man tissue normally range from 0.1mM, sion of the abovementioned
most concentrated in liver, spleen, kidney, products and thus prevents
lens, erythrocytes and leucocytes. Oxida- proliferation and metastasis of
tive stressors that can deplete GSH include cancer.26,27,28 It also potentiates
ultraviolet rays and other radiation, viral apoptosis induced by TNF and
infections, environmental toxins, heavy chemotherapeutic agents.29
metals, surgery, inflammation, burns, sep- In patients with advanced
tic shock, and dietary deficiencies of GSH melanoma, treatment with te-
precursors.19,20 The immune system func- mozolomide is associated with
tion is dependent upon the lymphoid cells greater improvements in over-
having a delicately balanced, adequate all survival.30 Temozolomide is
level of glutathione. Certain functions a novel oral alkylating agent, Figure 5
MRI combined with PET-CT of the extremi-
such as orderly DNA synthesis are exqui- which appears to exert its therapeutic ben- ties showing complete resolution of in-transit
sitely sensitive to reactive oxygen species efit through DNA methylation and there- metastasis seen in the left lower extremity of
and therefore improved by high levels of fore triggering the death of neoplastic cells. previous scan.
antioxidant glutathione. Certain signaling Its acceptable safety profile and predictable
pathways, in contrast, are enhanced by pharmacokinetics make temozolomide an
oxidative conditions and favored by low excellent candidate for inclusion in combi- centrations, the normal melanocytes were
glutathione levels. IL-2 dependent func- nation therapies for advanced metastatic not affected. EGCG treatment of the mela-
tions including T-cell proliferation, cytotox- melanoma. Temozolomide, which is 100% noma cell lines resulted in decreased cell
ic T-cell activity, lymphokine activated killer orally bioavailable, allows for outpatient proliferation and induction of apoptosis via
cells and natural killer cells are particularly treatment. This is particularly desirable downmodulation of anti-apoptotic protein
sensitive to glutathione depletion.23 It has for patients with advanced melanoma, a Bcl2, upregulation of proapoptotic Bax and
been demonstrated that exogenous, extra group with a short life expectancy and a activation of caspases.39 EGCG also causes
cellular glutathione induces apoptosis in low rate of response to treatment. In clini- significant induction of cell cycle arrest via
ovarian cancer cell lines by inducing ex- cal studies, temozolomide was well toler- modulations in the cki-cyclin-cdk network.
pression of the P53 and P21 tumor sup- ated and demonstrated rapidly reversible, Thus, EGCG, alone or in conjunction with
pressor genes.24 mild to moderate myelosuppression.31 current therapies, could be useful for the
Honokiol and magnolol (isomer of Ho- However given this patient’s concurrent management of melanoma. Sinecatechine
nokiol) have shown to inhibit skin tumor infection and advanced age, conventional (trade name Veregen) is an ointment of
growth and invasion.25 The nuclear tran- dosing of temozolamide was contraindicat- catechins (55% epigallocatechin gallate)
scription factor nuclear factor (NF-Kb) is ed. Metronomic dose chemotherapy has extracted from green tea and other com-
involved in the expression of several genes been found to be well tolerated,32 and have ponents. It was the first botanical prescrip-
whose products are involved in tumori- both pro-apoptopic33 and anti-angiogenic tion drug approved by the US Food and
genesis. These include antiapoptotic genes effects34 in multiple tumor types. Drug Administration, for treatment of geni-
(survivin, TRAF, Bcl-2, bcl-xl), cyclooxy- Based on several clinical studies, vitamin tal warts caused by the Human Papilloma
genase (COX-2), matrix metalloproteinase A has been observed to interfere with the Virus.40
carcinogenic process in different ways.
Figure 4 Inhibition of malignant melanoma cell Conclusion
Chest CT scan showing virtual resolution of proliferation through Fas death receptor Late presentation of metastatic mela-
previously seen metastatic right
pulmonary lesion
pathway mediated cell apoptosis,35 inhibi- noma is common, and should be remem-
tion of proliferation of melanoma bered in patients with a distant history of
cells through cell cycle arrest36 ap- melanoma. Follow-up is necessary in or-
pear to be some of the proposed der to diagnose potential dissemination or
mechanisms of vitamin A against secondary sites of the disease. In stage-IV
malignant melanoma. melanoma, Temodar, IL-2 therapy com-
Natural plant extracts, such as bined with retinoic acid, vitamin C, topical
polyphenolic antioxidants found sinecatechin, magnolol, glutathione and
in green tea and grape seed, have sargramostim demonstrates a promising al-
been shown to inhibit tumor angio- ternative/complementary regimen to stan-
genesis and tumor growth through dard regimens for treatment of metastatic
a number of mechanisms.37 Epigal- melanoma. Temodar was added on met-
locatechin-3-gallate (EGCG), the ronomic schedule for its broadspectrum
major catechin (flavonol) in green antitumor activity via promoting apoptosis
tea was found to result in a dose- and inhibiting angiogenesis with limited
dependent decrease in the viability side effects. Magnolol, vitamin C, vitamin
and growth of melanoma cells.38 A, and topical sinecatechin were included
Interestingly, at similar EGCG con- because of their proapoptotic properties
Reprint - Cancer Strategies Journal - Spring 2014 - www.cancerstrategiesjournal.com 3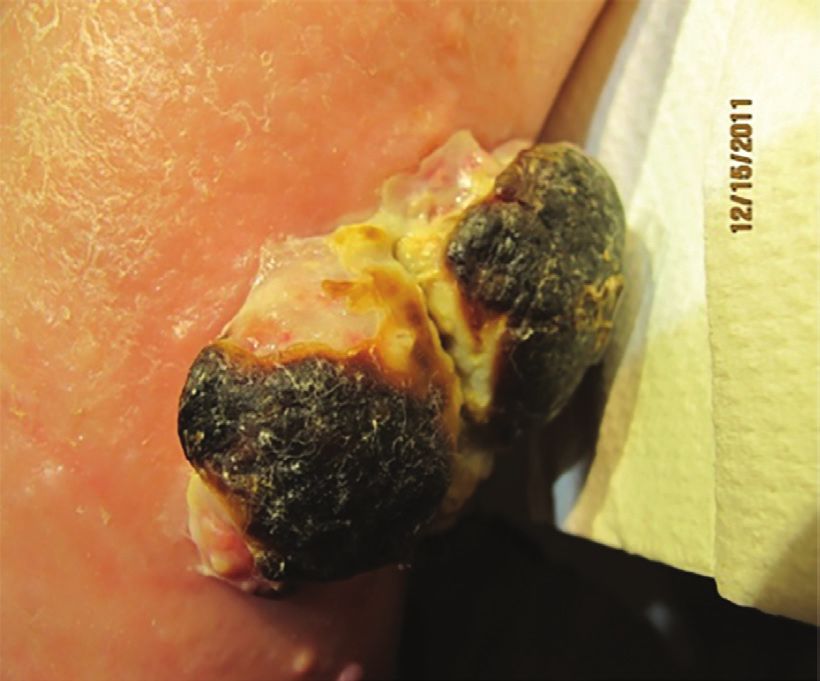
*Authors: Gaynor, Mitchell L., Gopal- References for this article may be found at at
http://www.cancerstrategiesjournal.com/
arathinam, Rajesh., Kline, Mitchell.
ReferencesVolume2Issue2.pdf
Figures and artwork included by permission of the authors.
Mitchell L. Gaynor, MD
Mitchell L. Gaynor MD is Founder and President of Gaynor Integrative Oncology (www.
dr.gaynor.com). Assistant Attending Physician at New York Presbyterian Hospital/Weill Cor-
nell Medical Center, and Clinical assistant Professor of Medicine at Weill Medical College.
He has held the position of Director of Medical Oncology at The Strang Cancer Prevention
Center where he still serves as a consultant. He is also former Medical Director and Direc-
tor of Medical Oncology at the Weill Cornell Medical Center Institute for Complementary
Figure 6 and Integrative Medicine. He has served on the Executive Review Panel at the Department
There was complete resolution of the
melanoma lesion seen initially on the of Defense – Alternative Medicine for Breast Cancer Sector and the Smithsonian Institute’s
left anterior tibia area. Symposium on New Frontier in Breast Cancer and the Environment. He is a frequent speak-
er and lecturer at hospitals, conferences, and universities throughout American and abroad.
against melanoma cells. IL-2 even in low Dr. Gaynor is the best selling author of four books and a CD focusing on healing, health, the
doses regulates cellular immune response. environment, and cancer prevention.
Glutathione has immune-stimulating and Dr. Gaynor has been consecutively listed in The Best Doctors in New York since 1997
pro-apoptopic effects. Sargramostim stim- and has served on the Board of Advisors for Healthy Living Magazine, the Sass Medical
ulates the bone marrow to produce natural Foundation, as well as the Editorial board of Integrative Cancer Therapies. After receiving
killer cells. This patient has remained in his medical degree from the University of Texas – Southwestern Medical School in Dallas,
complete remission for 25 months and is TX, he was a clinical fellow in hematology-oncology at the New York Hospital-Cornell Medi-
tolerating the regimen without side effects. cal Center and a post-doctorate fellow in molecular biology at Rockefeller University. He is
Further investigation of this combination board certified in medical oncology, hematology and internal medicine. He is a member of
of low dose immune modulating agents, the American Society of Clinical Oncology, the American College of Physicians and the New
chemotherapy and bioactive nutrients is York Academy of Sciences.
warranted.
Advertise in the Cancer Strategies Journal
Take Advantage of Rates that are low
until the end of 2014. An ad
m
nal.co adver vertising r
g i e sjour h us. t a
cerst
ra t e
n ad w
i t www. ising cont te sheet a
@can to place a c r
t e v e reque
st. Who Should Advertise With Us? adver ancerstra act may b nd an
a c n d o n tising te e
n t
Co estions a
etting
u p • Product Manufacturers and/or .htm. giesjourn found at
types al.com
for qu p l e Distrbutors /
o si m
We d • Service Providers
• Cancer Centers
• Individual Practitioners
• Someone who has something to
offer to the field of Integrative
Cancer Medicine
Momentum has been strong in the growth of our subscriber base in our
first year of publication. Most of our readers have re-subscribed and
our subscriber base grows daily. You can be part of that momentum by
advertising with us and growing with us. Our advertisers tell us that
they are receiving calls from our subscribers about their products.
4 Reprint - Cancer Strategies Journal - Spring 2014 - www.cancerstrategiesjournal.com
Imagine having a copy of the Cancer Strategies
Journal next to you on your desk as an
effective guide in your work with cancer.
Featured in Each Issue:
• Articles with information about botanicals, nutrition, food and dietary
supplements, mistletoe, IV Vitamin C, expanded lab interpretations,
research, helpful pharmaceuticals, off-label drugs in cancer medicine,
modern cancer medicine (chemotherapeutic, surgical, radiation and
diagnostic)
• Cancer treatment and prevention, with new, up to date thinking on can-
cer care and successful outcomes research, how primary care physicians
can become more knowledgeable and participatory with local oncologists
and be supportive to their patients therapeutically, and in preventing
cancer, social and economic aspects in cancer care
Subscription Options
• Ways to educate your patients who are wavering on their choice of care, One Year: $75
or who are fearful of not following the one-size-fits-all model of modern
Two Years: $130 (You may opt to receive the entire
medical oncology, insights and tools to help your patients with cancer first year and pick up with our current second year, if you
resolve the hidden conflicts underlying their cancers, giving the body choose)
permission to heal, psychological/stress-related issues in cancer care Reprints: $7 per reprint plus postage (bulk discounts are
available)
• Clinical pearls, clinical applications and the thinking behind them, pro-
Individual Issues: $20/issue plus postage
found outcomes even in serious cases of cancer, and the combination of
good science and heartfelt spiritual involvement If international subscription, foreign postage
will be added (per issue). Subscription price:
• Integrative Medicine Perspectives, Naturopathic Medicine Perspectives, Canada: $92.40 per year, includes postage
Oriental Medicine Perspectives, Anthroposophical Medicine Perspectives, Mexico: $105.40 per year, includes postage
Ayurvedic Medicine Perspectives, Energy Medicine Perspectives
Overseas: $113.80 per year, includes postage
and more
A PEER-REVIEWED JOURNAL
STAY ON TOP OF THE ONGOING METAMORPHOSIS IN INTEGRATIVE CANCER MEDICINE *
PRACTICAL CLINICAL APPROACHES *
SIGNIFICANTLY ENHANCE YOUR RESULTS WITH PATIENTS *
ORDER FORM - SUBSCRIPTION - CANCER STRATEGIES JOURNAL
Name______________________________________________________ Email ____________________________________
Mailing Address____________________________________________________________Tel. No. _____________________
City, State, Zip__________________________________________________ Form of Payment: Credit Card Check
Credit Card # (NO AMEX): _______________________________________________Exp. Date______________________
3-Digit Code__________ Please circle: One Year $75 Two Years $130 If international, foreign postage will be added.
Billing address if different from mailing address: ____________________________________________________________
Please email to eve@cancerstrategiesjournal.com, fax to (303) 499-0102 or
mail to 4650 Talbot Drive, Boulder, CO 80303. Make checks payable to Healthy Medicine Academy.
For more subscription options, advertising information, manuscript information, and
To order online, www.cancerstrategiesjournal.com.
Making Cancer Treatment More Effective with Integrative Oncology
Cancer Strategies
Journal
Advances in Integrative Cancer
Medicine and Research
Using Digital Infrared Thermal Imaging (DITI) Adjunctively in the Prevention and
Treatment of Cancer
Complete Remission of Widely
Metastatic Melanoma
Onco-Immunology
Cancer and Coagulation
Mistletoe Therapy in Cancer
Treatment
Clinical Pearls
Addressing the Miasm in Cancer
Treatment
Glycemic Restriction in Cancer Patients: A Controlled Interventional Study
A PEER-REVIEWED JOURNAL
PRACTICAL CLINICAL APPROACHES *
SIGNIFICANTLY ENHANCE YOUR RESULTS WITH PATIENTS *
STAY ON TOP OF THE ONGOING METAMORPHOSIS IN INTEGRATIVE CANCER MEDICINE *
Spring 2014
Volume 11, Issue 2


You can also read

















































