Condom use adoption and continuation: a transtheoretical approach
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
HEALTH EDUCATION RESEARCH Vol.12 no.l 1997
Theory & Practice Pages 61-75
Condom use adoption and continuation:
a transtheoretical approach
Diane M. Grimley1, Gabrielle E. Prochaska and James O. Prochaska
Abstract States with serious health consequences for thou-
sands of children and adults (Roper et al., 1993).
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
The use of latex condoms can reduce the risks of Specifically, 86% of all STDs occur among indi-
sexually transmitted diseases (STDs), including viduals between the ages of 15 and 29 (Centers
the human immunodeficiency virus (HIV) that for Disease Control and Prevention, 1991). Some
can lead to the acquired immunodeficiency syn- individuals are infected repeatedly with many hav-
drome (AIDS). Yet, most intervention programs ing more than one infection simultaneously (Aral
have demonstrated little effect on overall con- and Holmes, 1990). Moreover, sexually active
dom use. The major limitation of many tradi- individuals today have to deal with the real threat
tional behavioral change programs is that they of infection from the human immunodeficiency
are based on an action paradigm which impli- virus (HIV) that can lead to the acquired immuno-
citly or explicitly views behavior change as a deficiency syndrome (AIDS). The consistent use
dramatic and discrete movement (e.g. going of latex condoms can reduce the risks of infection
from 'never' using condoms to 'always' using or transmission of STDs/HTV (Centers for Disease
condoms). The Transtheoretical Model of Control and Prevention, 1988; Coates, 1990; Roper
Change (TMC) offers an alternative concep- et al., 1993); yet, most intervention programs have
tualization of the structure of change, a stage demonstrated little effect on overall condom use
paradigm, that defines behavior change as an (Catania et al., 1994). It would appear that tradi-
incremental process through a series of stages. tional behavior change technology is being put to
This paper offers a summary of how measures the scientific test and the limits of this approach
and models of condom use based on the TMC are acutely evident (Chesney, 1993).
have been developed and continue to be refined,
offers some preliminary findings with diverse The major limitation of traditional behavior
populations, and describes intervention applica- change technology is that it is implicitly or expli-
tions of a stage paradigm approach to condom citly based on an action paradigm. Action-oriented
use adoption and continuation. approaches to behavior change view condom use
adoption as a dramatic and discrete movement
Introduction from 'never' using condoms to 'always' using
condoms. Most intervention programs are
An estimated 12 million cases of sexually transmit- developed for small groups of individuals motiv-
ted diseases (STDs) occur each year in the United ated enough to seek help (Chesney, 1993; Kelly
et al., 1993). The problem is, a number of studies
using different populations (see Table II) point out
Cancer Prevention Research Center, University of Rhode that only about one-third of individuals at risk for
Island, Kingston, RI 02881-0808 and •School of Public STDs/HI V are prepared to take action for consistent
Health, Department of Health Behavior, University of
Alabama at Birmingham, Birmingham, AL 35294-0022,
and correct condom use (Prochaska et al., 1990;
USA Fishbein et al., 1993; Bowen and Trotter, 1995;
© Oxford University Press 61D. M. Grimley et al.
Galavotti et al, 1995; Grimley et al, 1993a, 1988; Marcus et al, 1992; Wilcox et al, 1985).
1995b). Action-oriented programs are missing two- At a minimum, these static factors are not under
thirds of the population at greatest risk because the potential control of professionals trying to
these individuals are less likely to respond to facilitate change nor are they under the immediate
public health messages or to sign up for our control of individuals who need to change
intervention programs. (Prochaska, 1989).
Many researchers and practitioners in the area Since the TMC is a 'template' of sorts that is
of STD/HIV prevention are beginning to recognize translated or redefined across different health-
that a single intervention approach may not be related behaviors (Grimley et al, 1994), the general
appropriate for all individuals who are engaging constructs of the model (i.e. stages of change,
in unprotected sex. As with other health-related processes of change, decisional balance and self-
problems, change agents are shifting the focus of efficacy) have been adapted to the measurement
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
their efforts toward identifying the 'best fit' of condom use by making their content specific to
between an individual's characteristics and inter- condom use in order to operationalize the con-
vention strategies. The Transtheoretical Model of structs. In the initial measurement study conducted
Change (TMC; Prochaska and DiClemente, 1983, in collaboration with the Centers for Disease Con-
1984) offers promise for this endeavor by providing trol and Prevention's Division of STD/HTV
a framework—or paradigm—for understanding (Prochaska et al, 1990), one of the goals was to
condom use behavior (Centers for Disease Control investigate the dimensional complexity of condom
and Prevention, 1992; Galavotti et al, 1995; use. Specifically, is it necessary to distinguish
Grimley and Lee, 1996; Grimley et al, 1993a,b, between type of sexual partner (primary versus
1995a-c, 1996; Prochaska et al, 1990). This paper non-primary) and type of sexual intercourse
offers a summary of how measures and models of (vaginal versus anal) when examining condom
condom use behavior based on the TMC were use? Individuals from a community sample at risk
developed and continue to be refined. The paper for HTV (e.g. IV drug users, prostitutes, at-risk
also provides some preliminary findings with street youth, gay or bisexual men, etc.) were
diverse populations and describes some interven- assessed separately on each of the model's key
tion applications of the stage paradigm approach constructs with both types of partners and types of
to condom use adoption and continuation. sexual activities. Conceptual model testing results
demonstrated that it is necessary to model condom
use behavior separately based on partner type as
The TMC
well as specific intercourse activities.
The TMC has been postulated as an integrative Assessing an individual's condom use separately
and comprehensive model of behavior change. with primary versus non-primary partners results
Research has provided strong support for the in more explained variance with this behavior
reliability and validity of core constructs from the as compared with more global measures. The
model such as the stages of change (McConnaughy distinction between partner type is a pervasive
et al, 1983, 1989), the processes of change finding that has been replicated with a number of
(Prochaska et al, 1988), decisional balance different populations such as STD clinic patients
(Prochaska et al, 1994; Velicer et al, 1985) (Fishbein et al, 1993), women at high risk for
and self-efficacy (Velicer et al, 1990). Numerous HIV infection and unintended pregnancy (Galavotti
studies have demonstrated the predictive validity etal, 1995; Grimley et al, 1992), college students
of the TMC's dynamic variables as compared with (Grimley et al, 1995b) and a random state-wide
demographic variables such as age, gender or sample of women (Grimley et al, 1995c). Accord-
ethnicity which are imposed on us for the most ing to Aggleton et al (1994), as the TMC is further
part rather than determined by us (Lam et al.. refined for application to HIV/AIDS, 'its use to
62Condom use adoption and continuation
guide intervention development and evaluation of Itoble L Algorithm of condom use for vaginal intercourse with
a main partner
intervention effects is becoming better appreciated'
(p. 343). Ql. Do you have a main partner of the opposite sex?
Stages of change 1) No (Skip to OTHER Partner)
2) Yes
A comprehensive model needs to cover the full Q2. When you have vaginal sex with your main partner, how
course of change, from the time an individual often do you use a condom?
becomes aware that engaging in unprotected sex 1) Every time (Go on to Q3)
is a problem to the point at which consistent 2) Almost every time (Skip to Q4)
condom use is maintained. There are many steps 3) Sometimes (Skip to Q4)
4) Almost never (Skip to Q4)
that precede and follow a person taking action
5) Never (Skip to Q4)
for consistent condom use. In contrast to action-
Q3. How long have you been using condoms every time you
oriented approaches to behavior change, the TMC
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
have vaginal sex with your main partner?
offers an alternative conceptualization of the struc- 1) Less than 6 months
ture of change by defining behavior change as an 2) More than 6 months
incremental and dynamic process. Thus, acquisition (Skip to OTHER partner section)
of condom use behavior is the endpoint of a Q4. Axe you seriously thinking about using condoms every
process that involves motivational and decision- time you have vaginal sex with your main partner in the next
making interventions as individuals progress 6 months'!
1) No (Skip to OTHER partner section)
through a sequence of discrete stages.
2) Yes
Similar to cessation behaviors (e.g. smoking), Q5. Are you seriously thinking about using condoms every
acquisition of health-enhancing behaviors such as time you have vaginal sex with your main partner in the next
condom use involves the progression through five 30 days?
stages of change of which 'action' is only one. l)No
These stages include: (1) precontemplation, (2) 2) Yes
(Go on to OTHER partner section)
contemplation, (3) preparation, (4) action and (5)
maintenance.
Sample items employed to assess condom use condoms 'sometimes' or 'almost always'
with a primary (main) partner are given in Table with their main partner. The preparation
I. The following classification scheme results from stage, therefore, consists of both intention
the assessment of condom use for individuals plus some behavioral 'steps' toward consist-
engaging in vaginal intercourse with a main ent condom use.
partner: (4) Action includes individuals who are using
condoms 'every time' for vaginal sex, but
(1) Precontemplation includes individuals who
have been doing so for less than 6 months.
are not currently using condoms 'every time'
(5) Maintenance includes individuals who are
for vagina] sex with their main partner and
using condoms with their main partner 'every
have no intention to start doing so in the
time' for vaginal sex for more than 6 months.
foreseeable future (i.e. in the next 6 months).
(2) Contemplation includes persons who are not Progression through the stages is often not linear
currently using condoms 'every time' for because many individuals regress or recycle back
vaginal sex with their main partner, but through earlier stages. Individuals may cycle
intend to start doing so sometime in the next through the stages several times before they reach
6 months. the action criterion of using condoms 'every time'
(3) Preparation consists of individuals who they engage in intercourse. Within the framework
intend to start using condoms 'every time' of the TMC, relapse is viewed as a normal part of
within the next month and are currently using the change process as opposed to a failure. It
63D. M. Grimley et al.
simply reinforces the notion that change is difficult from diseases they can contract from having inter-
and it is unrealistic to expect people to modify course with an infected partner.
unhealthy behaviors without having any 'slips.' To date, men and women have been shown to
The stages of change represent a temporal be evenly distributed across the stages of readiness
dimension that provides information regarding for using condoms in a college population (Grimley
when a particular shift in condom use attitudes, et al, 1995b), with a community sample (Prochaska
intention and behaviors may occur. The notion that et al, 1990), and with not-in-treatment IV drug
behavior change occurs in stages is not unique to users and crack cocaine smokers (Bowen and
the TMC; similar concepts have been postulated Trotter, 1995). Sex differences across the stages
by others (e.g. Horn, 1976; Weinstein, 1993). of change for using condoms have been reported
The utility of the stages of change for classifying in only one study with STD clinic patients. Fishbein
individuals on their condom use intentions and et al (1993) found that men were more likely than
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
behaviors has been examined with a number of women to be in the precontemplation stage for
populations (Prochaska et al., 1990; O'Reilly and using condoms within primary relationships. Male
Higgins, 1991; Grimley et al, 1992, 1993a,b, STD clients remain an understudied population
1995b,c; Fishbein et al, 1993; Galavotti et al, in urgent need of further intervention research
1995; Grimley and Lee, 1997), supporting the designed to reduce the adverse health consequences
validity of the construct with this behavior. Table of sexual risk behaviors.
II shows stage distributions from five independent Ethnicity of individuals as a function of stage
samples that classify individuals into the stages of has also been reported in one study. Bowen and
change for condom use for vaginal intercourse Trotter (1995) found that with main partners, White
with the two types of partners. With the exception participants were more likely to be in the action
of male STD patients, individuals were more likely stage and less likely to be in the contemplation
to be using condoms with non-primary (other) as stage as compared with African-Americans,
compared with primary (main) partners. In all four whereas those who were Hispanic were more likely
studies, individuals were more resistant to using to be in the contemplation stage than African-
condoms with a main partner (i.e. more likely to Americans. These preliminary findings for ethnic
be in the precontemplation stage), as compared difference across the stages of change support the
with other partners. These observations are consist- contention that in order to increase adoption and
ent with previous research reporting condom use continuation of condom use, assessments and inter-
frequencies (e.g. Rosenberg and Weiner, 1988; ventions of specific attitudes sensitive to condom
Armstrong et al, 1991; Soskolne et al, 1991; use across cultural groups are important considera-
Dorfman et al, 1992, 1993). Table II also shows tions when targeting condom use (e.g. Amaro,
that about half of the college students, as well 1995).
as the community high-risk sample, were using Age differences as a significant predictor of
condoms with non-primary partners. All other stage is beginning to emerge as a more stable
stage distributions indicate that 63-92% of the finding, with younger individuals being in the later
individuals were not using condoms consistently, stages of action and maintenance and older persons
with the majority of non-users being in the two being in the earlier stages of precontemplation and
earlier stages of readiness—precontemplation and contemplation for consistent condom use (Bowen
contemplation. These observations point out that and Trotter, 1995; Grimley et al, 1995c). These
interventions which are based on the assumption observations may reflect the fact that younger
that people are prepared to change (i.e. action- individuals are becoming better educated regarding
oriented) may not be sensitive to the specific needs their need for safety, may have more positive
of many people who are not protecting themselves attitudes regarding condom use, or perhaps possess
64Condom use adoption and continuation
Table II. Percentages of individuals across the stages of change for using condoms with primary versus non-primary partners
Sample N Partner type PC (9b) C (%) />(%) A (9b) M (%)
Community sample1-1'
(Prochaska et al., 1990)
218 primary 55 19 — 9 17
193 non-primary 21 26 — 9 44
STD clinic patients0
(Fishbein et al., 1993)
men 268 primary1 43 18 25 8 6
women 233 primary 32 37 24 8 4
men 200 non-primary 15 55 35 2 7
IV drug users and crack cocaine smoker*
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
(Bowen and Trotter, 1995)
166 primary 49 8 31 4 8
99 non-primaryf 22 4 38 9 26
Women at high risk8
(Galavotti et al., 1995)
233 primary 46 11 15 7 21
122 non-primary 26 12 25 9 27
University students*-*
(Grimley et al., 1995)
134 primary^ 23 16 33 13 16
78 non-primary 6 19 24 21 30
•Sex differences across stages were not reported.
'This study was conducted before the consistent emergence of the preparatjon stage; therefore, only four stages were assessed.
c
Percentages were estimated from a graph in Fishbein et al. (1993).
d
Data from women with non-primary partners were too few for meaningful analysis.
e
No significant sex differences were found for stage of change with either primary or non-primary partners.
f
May not equal 100% due to rounding errors.
g
The preparation stage included both intention and a behavioral component (i.e. currently using condoms 'sometimes' or 'almost
always'). Other studies assessed future intention only, without taking any behavioral steps toward consistent condom use into
account.
awareness that they are having more sexual partners in specific stages of change (Prochaska et al.,
(Bowen and Trotter, 1995). 1985; DiClemente et al., 1991).
The processes of change as applied to condom
Processes of change use acquisition and maintenance have received
The second dimension of the model, the processes little attention by researchers as compared with
of change, provides information on how people other constructs from the model. To date, only
change. The processes represent both covert and two cross-sectional studies have been conducted
overt activities individuals use to alter their experi- (Grimley et al., 1992, 1994a). Yet, due to the
ences and/or environments in order to affect urgency of assisting individuals at risk for HIV to
behavior, cognitions or relationships. The processes adopt condom use, behavior scientists at the Cen-
of change have been found to integrate empirically ters for Disease Control and Prevention have
within the stage dimension of change (Prochaska moved forward and are currently conducting an
and DiClemente, 1983) showing that these pro- ongoing intervention study based on general
cesses are emphasized differentially by individuals assumptions of the model regarding process use
65D. M. Grimley et al.
(Cabral et al., 1996). Although tentative, some emerged with exercise, another acquisition
conclusions can be made based on findings from behavior. These findings suggest that although
these preliminary efforts. individuals in the maintenance stage for condom
Although 10 processes of change have been use may feel more confident using condoms and
found with smoking cessation, 11 processes thus less tempted to engage in unprotected sex, they still
far have emerged with condom use. Assertiveness have to work at strengthening their commitment to
for condom use is the additional process of change using condoms and have to continue to have
individuals utilize in order to adopt and maintain condoms with them, so as to maintain behavior
consistent condom use (Grimley et al., 1993b; change. Also, women have been found to rely
Bowen and Trotter, 1995). This additional process heavily on the process of helping relationships
of change reflects the interpersonal aspect of sexual with both types of partners, perhaps because
behavior compared with more individual behaviors women depend on their partner to 'have' condoms
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
like smoking, exercise, etc. When integrated with available for intercourse. Sacco et al. (1993) note
the stages, condom use assertiveness increases that despite women's more favorable opinions
almost linearly across the stages with assertiveness regarding condom use, they rely on their partners
being the lowest in the precontemplation stage and to buy condoms and make them available during
the highest in the action or maintenance stage. sex. These observations are supported by the fact
Consistent with model-based research that the only process of change men have been
(Prochaska et al., 1988), the 11 processes of found to utilize more than women is stimulus
change represent two hierarchical factors labeled control (e.g. having condoms with them).
'experiential' and 'behavioral'. These two latent Utilization of the experiential processes of
factors include consciousness raising, self-reevalu- change as applied to condom use acquisition has
ation, dramatic relief, environmental reevaluation also been shown to differ from that found with
and social liberation (experiential processes); self- cessation behavior. In a process evaluation of an
liberation, counter conditioning, stimulus control, ongoing intervention study in which stage of
reinforcement management, helping relationships change counseling is provided to high-risk women
and assertiveness (behavioral processes). Defini- (Cabral et al., 1996) more emotional and cognitive
tions and sample items for the processes of change factors were being addressed with women in the
for condom use are shown in Table III. action and maintenance stages for condom use
Some external validity for the measure repres- with primary partners than would be expected
enting the processes of change has been established based on the TMC. These preliminary findings
by examining standardized process mean scores' have some support with college women. Grimley
across the stages of change for using condoms et al. (1994a) found that not only were women
with main and other partners (Grimley et al., 1992, using consciousness raising and dramatic relief
1994a). Precontemplators were found to use fewer (experiential processes) more than men, they con-
processes than those further along in the stages of tinued to do so in the action and maintenance
change, as the model predicts. The relationships stages.
between the processes and the stage of change for Overall, these findings suggest that, in general,
condom use appear to be similar to other problem maintaining condom use within important sexual
behaviors with process use increasing after the relationships may require more continued cognit-
precontemplation stage. However, preliminary ive/emotional effort than may be required with
findings indicate that, contrary to cessation non-primary partners or for the maintenance of
behaviors where the behavioral processes tend to other behaviors examined with the model. The fact
level off in the maintenance stage, the behavioral that men have the final say regarding whether or
processes for condom use continue to climb well not a condom is used makes consistent condom
into the maintenance stage. Similar findings have use more difficult for women. One implication for
66Condom use adoption and continuation
Table III. Titles, definitions and sample items of the processes of change for condom use
Process Definitions: sample items
Consciousness raising Increasing information about condom use and awareness regarding one's risk for STDs/HIV
(e.g. 'You remember what people have told you about how condoms can help keep you from
getting STDs/HIV).
Self-reevaluation Assessing how one feels and thinks about oneself with respect to his/her lack of condom use
(e.g. 'You feel more responsible when you use condoms').
Self-liberation Choosing and committing to act or belief in one's ability to use condoms (e.g. 'You tell yourself
you can choose to have sex with a condom').
Counter conditioning Substituting low risk sexual behaviors for high-risk sexual behaviors (e.g. 'When you want to
have sex but don't have a condom, you find other sexual ways to satisfy yourself and your
partner').
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
Stimulus control Avoiding people, places, or situations that could result in unprotected sex (e.g. 'You carry
condoms when you go out').
Reinforcement management Rewarding one's self or being rewarded by others for engaging in safer sex (e.g. 'You reward
yourself when you use condoms for sex').
Helping relationships Having someone to talk with, share feelings with, and get feedback from regarding one's
experiences with using condoms (e.g. 'You have someone you can count on when you're having
a hard time using condoms').
Dramatic relief Experiencing and expressing feelings associated with not protecting oneselfs from STDs/HIV
(e.g. 'You get scared when you hear about people getting STDs/HIV because they didn't use
condoms').
Environmental reevaluation Assessing how one's not using condoms could affect the health and lives of others ('You stop to
think that using a condom protects your partner, as well as yourself).
Social liberation Changing social norms ('You notice it's getting easier to find partners who don't mind using
condoms').
Assertiveness Perception of one's ability to assert the use of condoms in a variety of sexual situations ('If a
partner doesn't want to use a condom, you refuse to have sex').
future research is to consider targeting couples as order to predict advancement to the next stage and
a unit in order to modify high-risk sexual behaviors. to predict relapse.
With smoking cessation, for instance, if one spouse
quits and the other does not, the chances of success Decisional balance and self-efficacy
are slim.
Although these examinations of the processes In addition to the stages and the processes of
of change in conjunction with condom use behavior change, the TMC incorporates two other core
represent important preparatory efforts, future stud- constructs: decisional balance (Velicer et ai, 1985;
ies will offer stronger evidence of the measure's Prochaska et al., 1994) based on the decision
predictive ability. Further measurement develop- making theory of Janis and Mann (1977), and
ment and model testing of the processes of change self-efficacy, which Bandura (1977, 1982, 1986)
for condom use could potentially offer interven- considers as the most important construct in social
tionists the ability to conduct much needed process learning theory.
to outcome evaluations. Such evaluations as Cabral Decisional balance, simply stated, involves
et fl/.'s (1996), when completed, will help to weighing the advantages (pros) against the disad-
determine the extent to which a particular process vantages (cons) of using condoms, e.g. the potential
needs to be emphasized at a particular stage in benefits of using condoms for protection from
67D. M. Grimley et al.
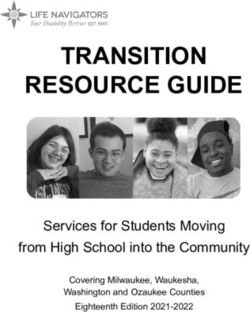
Pros and Cons of Condom Use-Main Partner
STDs/HTV infection or transmission must be bal-
anced against the perceived costs. Item content of
the positive aspects of using condoms within the
, •
TMC includes protection from pregnancy and/or
•—•
diseases, availability, personal responsibility, low —•—Pros
50
cost, and protection for a partner, as well as oneself. —•—Con*
An example of a positive item is, 'I would be safer -—•
from disease'.
1 1 1 j —i
The content covered for the negative aspects of
PC C P A M
using condoms within the TMC includes hassles, Stages of Change
decreased sexual enjoyment, the anticipation of a
partner's disapproval, as well as having to rely on
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
Pros and Cons of Condom Use-Other Partner
a partner's cooperation. A sample item of a negative
item is, 'My partner would be angry'. Individuals
are asked to rate 'how important' each statement
is to his or her decision whether or not to use
condoms. -Pro*
Figure 1 displays the pros and cons of condom -Cons
use with main and other partners across their
corresponding stage dimensions for college men
and women (Grimley et al., 1995b). Comparing
individuals across the stages of change on their C P A M
pros and cons for using condoms has resulted in Stages of Change
some highly predictable patterns. For example, the
cons of using condoms always outweigh the pros Fig. 1. Standardized mean scores (M = 50, SD = 10) for the
pros and cons of condom use with MAIN and OTHER
for individuals in the precontemplation stage. The partners across the five stages of change: precontemplation
opposite is true for those in the maintenance stage. (PC), contemplation (Q, preparation (P), action (A) and
From precontemplation to contemplation the pros maintenance (M).
of using condoms always increase, but there are
no consistent pattern in the cons. The cross-over across the stages of change tends to be more
of the pros and cons occurs before action takes characteristic of acquisition behaviors (e.g. exercise
place. To date, the functional relationship between adoption), rather than cessation behaviors, because
the pros and cons and the stages has been replicated continual effort is required to maintain the behavior
for condom use adoption and continuation with a change (Marcus et al., 1992). The results found
high-risk community sample (Prochaska et al., with condom use are more consistent with the
1990), women at risk for HIV infection or transmis- behavioral adoption pattern than with the pattern
sion (Grimley et al., 1992; Galavotti et al., 1995), of cessation behaviors (Galavotti et al., 1995).
and two independent college samples. (Grimley Thus, even if individuals adopt the use of condoms,
et al., 1993a, 1995b). the potential for discontinuing condom use remains
Although the characteristic cross-over pattern of high, unless the perceived negative aspects are
the pros and cons of condom use for vaginal diminished. This circumstance may pose a signi-
intercourse is similar to that found with at least 12 ficant challenge to intervention efforts (Galavotti
other health-related behaviors (Prochaska et al., et al., 1995). Moreover, the cons of condom use
1994), the cons of condom use do not decrease are relatively stable across the stages, particularly
significantly with further movement through the with non-primary partners (Bowen and Trotter,
stages. A less pronounced decrease in the cons 1995; Galavotti etal., 1995; Grimley etal., 1995b).
68Condom use adoption and continuation
Bowen and Trotter (1995) speculate that the inactive teens reported that they were 'seriously
stability of the cons with non-primary partners thinking about having intercourse' for the first time
may reflect an increased likelihood of relapse as within the next six months (Grimley and Lee,
compared with primary partners because of the 1997). Helping teens weigh the subjective advant-
overall smaller change in decisional balance. ages and disadvantages of becoming sexually act-
Another alternative is that an increase in the pros ive could assist them in the decision-making
of condom use with non-primary partners may be process of whether or not becoming sexually active
all that is necessary. is right for them. Such action could potentially
The basic pattern found for the pros and cons of result in the identification of ways in which con-
condom use adoption has implications for applied tinued abstinence may be more advantageous and
interventions. In order to assist individuals in compatible with an adolescent's personal values
precontemplation to move to the contemplation and long-term goals. Individuals who make an
stage, programs must increase people's perceptions informed decision to engage in intercourse could
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
of the benefits of using condoms. These observa- be provided with information regarding the impor-
tions point out that the expensive media campaigns tance of using condoms in order to protect oneself
that focus on the negative consequences of from STDs, as well as unintended pregnancy.
unplanned pregnancies and infection from STDs Self-efficacy is defined as the conviction that
might be more effective if public policy permitted one can successfully execute the behavior required
them to stress the advantages and safety of contra- to produce desired outcomes (Bandura, 1982,
ceptives as well (Zabin et al., 1993). Information 1986). Perceived self-efficacy has been shown to
channels such as sex education courses and public affect whether individuals consider changing their
health messages may also need to be revised (Bryne behavior, the degree of effort they invest in chan-
et al., 1993). Modification techniques should deal ging, and long-term maintenance of behavioral
directly with making the pros of condom use more change (Velicer et al., 1990; Bandura, 1982, 1986;
salient for individuals (e.g. 'Using condoms tells O'Leary, 1985). The potential usefulness of indi-
your partners that you care about them'). Once a vidual self-efficacy ratings in predicting health
person has progressed from precontemplation to behavior change has been well documented in such
the contemplation stage, and is at least thinking areas as smoking, weight control, contraception,
about change, interventions need to focus on alcohol abuse, pain management, recovery from
decreasing the cons of condom use which should myocardial infarction and adherence to exercise
lead to further progress from contemplation to programs (Strecher et al., 1986; Marcus et al.,
action. 1992; Velicer et al, 1990).
Males have been found to evaluate the disadvant- Within the TMC framework, the construct of
ages of using condoms as higher than the advant- self-efficacy represents an integration of the model
ages of their use with primary partners (Grimley of self-efficacy proposed by Bandura (1982) and
et al., 1995b). To date, no sex differences on the the coping models of relapse and maintenance
pros and cons for using condoms with non-primary described by Shiffman (1986). When examining
partners have been found, suggesting that males condom use adoption, the measure of self-efficacy
and females may share similar attitudes regarding assesses the degree of situational pull that might
condom use in less psychologically intimate sexual exist that could induce an individual to choose to
situations. have intercourse without the use of condoms. Some
Alternatively, the pros and cons can be integrated example items include: 'How confident are you
with the stages of readiness for sexual acquisition that you would use a condom ... When you have
behavior among adolescents. In a random sample been using alcohol or other drugs? When you're
of 235 heterosexual female adolescents between already using another method for birth control?'
the ages of 15 and 19 years, 18% of the sexually The content domain of self-efficacy within the
69D. M. Grimley et al.
Confidence of Condom Use-Main Partner
TMC also includes biological and partner-related
issues. Similar to physical urges to smoke experi-
enced with quitting smoking, self-efficacy for using
condoms can be effected by fundamental biological
circumstances such as states of high sexual arousal.
What is unique to condom use, as compared to -Confidence
other behaviors examined by the model, is the
interpersonal or relational aspect inherent to con-
dom use. Despite the fact that the male condom
was endorsed as the most acceptable method of
contraception by over 2000 women at high risk of PC C P A M
HTV infection (Galavotti etal., 1994), lowest levels
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
of confidence for using condoms were reported in Confidence of Condom Use-Other Partners)
situations where the partner might become angry
or upset. Yet, in another study with college-age
men and women (Grimley et al., 1995c), females
reported higher levels of self-efficacy for using
condoms with someone other than a main partner,
-Confidence
whereas no sex differences in efficacy ratings were
found for condom use within primary relationships.
In fact, both college-age men and women and
women at risk for HTV and unintended pregnancy
reported lower levels of confidence for using C P
condoms when engaging in vaginal intercourse Stages of Change
with primary, as compared with non-primary part-
Fig. 2. Standardized mean scores (M = 50, SD = 10) for self-
ners (Galavotti et al., 1995; Grimley et al., 1995b, efficacy for condom use with MAIN and OTHER partners across
1996). These observations suggest that such inter- the five stages of change: precontemplation (PC), contemplation
personal factors as fidelity, commitment and con- (C), preparation (P), action (A) and maintenance (M).
flict may inhibit the use of condoms within
important intimate relationships, not just for
with the basic premise of the Information-Motiva-
women (e.g. Morrill, 1994; Amaro, 1995), but for
tion-Behavioral Skills (1MB) model of AIDS-
some men as well.
preventive behaviors postulated by Fisher and
Figure 2 shows self-efficacy for using condoms Fisher (1992) and Fisher et al. (1994). The 1MB
with main and other partners across the five stages model assumes that different levels of information
of change. Efficacy scores are the lowest for and motivation may characterize individuals at
individuals in the precontemplation stage and different stages of the change process. Fisher et al.
increase almost linearly for those further along in (1994) contend that individuals in the precontem-
the stages of change for condom use (Prochaska plation stage may be informed about STDs/HIV,
et al., 1990; Galavotti et al, 1995; Grimley et al., but are not yet motivated to change their unsafe
1995c). Ratings of self-efficacy are not strong sexual practices; those contemplating change may
predictors of outcome before an individual reaches be informed and somewhat motivated but may still
action, but have been shown to be related to not possess the requisite behavioral skills necessary
utilization of the processes of change (Prochaska to engage in consistent condom use; yet, individuals
and DiClemente, 1992). actually enacting change must generally possess the
These findings based on the stages of readiness requisite information, motivation and behavioral
and self-efficacy for using condoms are consistent skills associated with condom use.
70Condom use adoption and continuation
regards to condom use intention and behaviors.
Putting theory into practice Each assessment is separated into distinct sections
based on the model's constructs. After each section,
Nearly 15 years of research on how people change participants will receive immediate, personalized
on their own and in intervention studies has lead feedback based on their individual responses
to the development of a TMC expert system regarding their current stage of change for using
intervention (Prochaska et al., 1993; Velicer et al., condoms; the change processes which they may
1993). Expert systems are computerized interven- not be using, or perhaps using too much; where
tions that are based on a person's own responses they stand in the decision-making process for using
to questionnaires that are scored and then inter- condoms based on their pros and cons scores; what
preted by expert computer technology which then ideas they need to think more about in order to
generates a unique report. The reports include motivate them to move to the next stage of change;
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
feedback on: the individual's stage of change, and alerts them to specific sexual situations they
decisional balance regarding the pros and cons, will need to avoid to maintain consistent condom
the processes of change that the individual may be use. This feedback will appear 'on screen' and
underutilizing, overutilizing or is utilizing appro- win also be vocalized through the use of a headset.
priately, and self-efficacy across a variety of situ- At the end of each session, each participant and
ations, and points out potentially problematic her assigned counselor will be provided with a
situations that need to be targeted to prevent computer generated printed report reflecting the
relapse. key issues that need to be addressed in order to
At baseline, each person's scores on all TMC promote advancement tiirough the stages. Coun-
variables are compared to a normative data base selors will then reinforce the computerized feed-
(data from individuals from the same population; back with each individual. Teens in the usual
same age group, etc., who have successfully pro- care condition will receive generic feedback plus
gressed through the stages for a specific behavior). counselor support.
At follow-up, ipsative feedback (compared to self The second system is home-based as opposed
over time) is also provided on TMC variables to the above clinic-based intervention. This expert
that are most important for progressing from one system is being designed to increase compliance
particular stage to the next. Expert systems are with oral contraceptive use and to promote condom
theory driven and lead to more scientific and use with women whose sexual behavior, or their
accurate diagnoses of specific problem behaviors. partner's behavior, may place them at risk for
It is important to emphasize that each report STDs.
generated by the system is truly matched to the This expert system will involve a pencil-and-
individual based on his or her responses to the paper survey that is filled out by women when a
TMC assessment instrument. prescription for oral contraceptives is given, or
Two systems are currently being developed in completed at home and returned in a postage-paid
the area of high-risk sexual behavior change. The envelope. Proactive phone calls will be made to
first is a multi-media expert system that targets women who do not return the completed question-
condom use with inner city females 14-17 years naire with 2 weeks in order to have each study
old. The overall focus of the study is to prevent participant's data. Survey's will then be scanned
cervical cancer and will be provided in several into a database and a unique report generated,
family planning clinics in the Philadelphia area. which will then be mailed out to each participant as
Females will be randomly assigned to the TMC quickly as possible. In addition to giving feedback
condition or the usual care condition. Participants based on all constructs of the model regarding
in the TMC intervention will sit at a computer and adherence to pill-taking directions, women who
answer questions by clicking on a 'mouse' in are having intercourse with more than one partner,
71D. M. Grimley et al.
or with a high-risk partner, will receive feedback ling them to reach and assist large numbers of
on the importance of using condoms along with the individuals who are in the earlier stages of change
pill for disease protection. Such stage-matched to progress more quickly through the stages. In
interventions have the ability to reach the vast addition, they possess knowledge of the cultural
majority of populations at risk by providing inter- barriers that may exist in their particular commun-
ventions which are sensitive to the specific needs ity and can make referrals to other community
of individuals in the earlier stages and not just organizations when needed.
those who are motivated to change. When used in
combination with proactive recruitment methods, Conclusion
stage-matched computer-based expert systems can
provide effective standardized, individualized, and Many existing behavior change programs offer the
interactive interventions while impacting large per- best action-oriented strategies available, but seem
centages of the population (Velicer and DiCle-
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
to be failing. This is due, in part, to providing
mente, 1993). 'one-size-fits-air interventions without considering
A stage-based intervention2 is currently being a person's readiness to follow such advice (e.g.
employed with women at high-risk for both unin- Prochaska, 1994b). Interventions targeting condom
tended pregnancy and HTV infection or transmis- use adoption and continuation based on the TMC
sion (Cabral et al., 1996) funded by the Division have the potential of combining not only the
of Reproductive Health at the Centers for Disease individualization and intensity of the clinical inter-
Control and Prevention. This comprehensive AIDS vention, but also the high participation rates of the
and reproductive health education study (Project public health approach, resulting in high-impact
CARES) has generated a guide based on the TMC interventions. When we integrate individual and
for advocates to utilize when counseling women public health approaches, the treatment goal must
(Project CARES: Advocates' Guide to Stage of be to accelerate stage movement to action prior
Change Counseling, January 1994). The interven- to providing action-oriented treatments (Abrams,
tion study focuses on women who are less likely 1993). In other words, we need to move away
to come into family planning centers and have from the old action-oriented paradigm of behavior
been recruited through drug treatment centers, change to a stage-matched approach if we are to
homeless shelters, an HTV clinic, and street out- meet the needs of all individuals at risk for STDs/
reach in high-risk neighborhoods. Participants are HIV and not just the relatively small percentage
assessed on their readiness to change by paraprofes- of individuals prepared to take action.
sional peer advocates who assist women to engage
in stage-based strategies in order to facilitate pro- Acknowledgements
gress toward action for the consistent use of
condoms and other contraceptives. This type of This paper was supported in part by grants
stage-based guide has recently been developed for CA27821 and CA50087 from the National Cancer
utilization with heterosexual men who are STD Institute and CSA-92-109 from the Centers for
patients in order to increase condom use (Grimley Disease Control and Prevention, and funding pro-
and Prochaska, 1996). vided from Ortho Pharmaceutical, Inc.
Another potential application of the TMC when
modifying STD/HIV risk behaviors could be to Notes
utilize community outreach workers or street edu-
cators who have already developed credibility 1. In order to provide a standard metric, data on all TMC
and rapport with community members. Outreach constructs are converted from raw scores to 7"-scores (M =
50, SD = 10) when integrated with the stages of change.
workers familiar with the TMC can have a much 2. Stage-based interventions are designed based on a person's
greater impact on the overall community by enab- current stage of change only.
72Condom use adoption and continuation
References The processes of smoking cessation: an analysis of
precontemplation, contemplation, and preparation stages of
change. Journal of Consulting and Clinical Psychology,
Abrams, D. B. (1993) Treatment issues: towards a stepped- 59, 295-304.
care model. Tobacco Control, 2 (suppl.), S17-S37.
Dorfman, L. E., Derish, P. A. and Cohen, J. B. (1992) Hey
Aggleton, P., O'Reilly, K., Slutkin, G. and Davies, P. (1994)
girlfriend: an evaluation of AIDS prevention among women
Risking everything? Risk behavior, behavior change, and
in the sex industry. Health Education Quarterly, 19, 25-40.
AIDS. Science, 265, 341-345.
Amaro, H. (1995) Love, sex, and power considering women's Hshbein, M., Douglas, J. M., Rhodes, F., Hananel, L. D.
and Napolitano, E. (1993) Distribution of STD clinic
realities in HIV prevention. American Psychologist, SO,
patients along a stages-of-change continuum: selected sites,
437^(47.
Aral, S. O. and Holmes, K. K. (1990) Epidemiology of 1993. Mortality and Morbidity Weekly Report, 42, 880-883.
sexual behavior and sexually transmitted diseases. In Fisher, J. D. and Fisher, W. A. (1992) Changing AIDS-
Holmes, K. K., et al. (eds), Sexually Transmitted Diseases, related risk behavior. Psychological Bulletin, 111, 455-474.
2nd edn. McGraw-Hill, New York. Fisher, J. D., Fisher, W. A., Williams, S. S. and Malloy,
Armstrong, K. A., Kenen, R. and Samost, L. (1991) Barriers T. E. (1994) Empirical tests of an information—motivation-
to family planning services among patients in drug behavioral skills model of ATDS-preventive behavior with
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
treatment programs. Family Planning Perspectives, 23, gay men and heterosexual university students. Health
264-271. Psychology, 13, 238-250.
Bandura, A. (1977) Self-efficacy: toward a unifying theory Galavotti, C , Grimley, D. M., Cabral, R., the CDC Perinatal
of behavior change. Psychological Review, 84, 191-215. HTV Prevention and Education Demonstration Activities
Bandura, A. (1982) Self-efficacy mechanism in human agency. (PHREDDA), and the CDC Prevention of HTV in
American Psychologist, 37, 122-147. Women and Infants Demonstration Projects (1994) Condom
Bandura, A. (1986) Social Foundations of Thought and Action: acceptability among women at high risk of HIV infection.
A Social Cognitive Theory. Prentice-Hall, Englewood Cliffs, Paper presented at the Society of Behavioral Medicine,
NJ. Boston, MA.
Bowen, A. M. and Trotter, R., II (1995) HIV risk in Galavotti, C , Cabral, R., Lansky, A., Grimley, D. M., Riley,
intravenous drug users and crack cocaine smokers: G. E. and Prochaska, J. O. (1995) Validation of measures
predicting stage of change for condom use. Journal of of condom and other contraceptive use among women at
Consulting and Clinical Psychology, 63, 238-248. high risk for HIV infection and unintended pregnancy.
Bryne, D., Kelley, K. and Fisher, W. A. (1993) Unwanted Health Psychology, 14, 570-578.
pregnancies: incidence, interpretation, and intervention. Grimley, D. M. and Lee, P. A. (1997) Condom and other
Applied and Preventive Psychology, 2, 101-113. contraceptive use among a random sample of female
Cabral, R. J., Galavotti, C , Gargiullo, P. M., Armstrong, K., adolescents: A snap-shot in time. Adolescence, in press.
Cohen, A., Gielen, A. C. and Watkinson, L. (1996) Grimley, D. M., Prochaska, G. E. and Prochaska, J. O.
Paraprofessional delivery of a theory-based HIV prevention (1993a) Condom use assertiveness and the stages of
counseling intervention for women. Public Health Reports, change with main and other partners. Journal of Applied
3, 75-82. Biobehavioral Research, 1, 152-173.
Catania, J. A., Coates, T. J., Golden, E., Dolcini, M. M., Grimley, D. M., Riley, G. E., Bellis, J. M. and Prochaska,
Peterson, J., Kegeles, S., Siegel, D. and Fullilove, M. T. J. O. (1993b) Assessing the stages of change and decision-
(1994) Correlates of condom use among black, hispanic, making for contraceptive use for the prevention of
and white heterosexuals in San Francisco: the AMEN pregnancies, STDs, and AIDS. Health Education Quarterly,
longitudinal survey. AIDS Education and Prevention, 6, 20, 455-470.
12-26.
Grimley, D. M., Riley, G. E., Prochaska, J. O., Redding, C.
Centers for Disease Control and Prevention (1988) Condoms
A., Ruggiero, L., Velicer, W. F. and Rossi, J. S.
for the prevention of sexually transmitted diseases.
(1992) The application of the transtheoretical model to
Morbidity and Mortality Weekly Report, 37, 133-137.
contraceptive and condom use in high-risk women.
Centers for Disease Control and Prevention (1991) Division
Technical Report to the Centers for Disease Control and
of STD/HIV Prevention Annual Report. US Department of
Prevention (contract grant CSA-92-109).
Health and Human Services, Atlanta, GA.
Centers for Disease Control and Prevention (1992) A Grimley, D. M., Prochaska, G. E. and Prochaska, J. O.
conceptual framework for evaluating behavior change. (1994a) The stages and the processes of change for
HIV/AIDS Prevention Newsletter, 3, 2-3. condom use with main and other partners. Unpublished
Chesney, M. A. (1993) Health psychology in the 21st century: manuscript. Cancer Prevention Research Center, University
acquired immunodeficiency syndrome as a harbinger of of Rhode Island, Kingston.
things to come. Health Psychology, 12, 259-268. Grimley, D. M., Prochaska, J. O., Velicer, W. F , Blais, L.
Coates, T. J. (1990) Strategies for modifying sexual behavior M. and DiClemente, C. C. (1994b) The transtheoretical
for primary and secondary prevention of HIV disease. model of change. In Brinthaupt, T. M. and Lipka, R. P.
Journal of Consulting and Clinical Psychology, 58, 57-69. (eds). Changing the Self: Philosophies, Techniques, and
DiClemente, C. C , Prochaska, J. O., Fairhurst, S., Velicer, Experiences. State University of New York Press. Albany,
W. F., Velasquez, M. M. and Rossi J. S. (1991) NY, pp. 201-227.
73D. M. Grimley et al.
Grimley, D. M., DiClemente, R. J., Prochaska, J. O. and Unmet Needs. American Cancer Society, Atlanta, GA, pp.
Prochaska, G. E. (1995a) Preventing adolescent pregnancy, 30-34.
STDs, and HIV: a promising new approach. Family Life Prochaska, J. O. (1994) Helping patients at every stage of
Educator. 13, 7-15. change. Behavioral Approaches to Addiction, 3, 2-7.
Grimley, D. M., Prochaska, J. 0., Velicer, W. F. and Prochaska, J. O. and DiClemente, C. C. (1983) Stages and
Prochaska, G. E. (1995b) Contraceptive and condom use processes of self-change in smoking: toward an integrative
adoption and maintenance: a stage paradigm approach. model of change. Journal of Consulting and Clinical
Health Education Quarterly, 22, 20-35. Psychology, 5, 390-395.
Grimley, D. M., Willey, C , Johnson, S., Lee, P., Prochaska, Prochaska, J. O. and DiClemente, C. C. (1984) The
J. O. and Redding, C. A. (1995c) Stages of change for translheorelical approach: Crossing the traditional
contraceptive and condom use: A random state-wide boundaries of therapy. Dow Jones/Irwin, Homewood, IL.
sample. Paper presented at the Annual Meeting of the Prochaska, J. O. and DiClemente, C. C. (1992) Stages of
Society of Behavioral Medicine, San Diego, CA change in the modification of problem behaviors. In
Grimley, D. M , Prochaska, G. E., Prochaska, J. O., Velicer, Herson, M., Eisler, R. M.and Miller, P. M. (eds),
W. E, Galavotti, C , Cabral, R. J. and Lansky, A. (1996) Progress in Behavior Modification. Sycamore Publishing,
Cross-validation of measures assessing decisions] balance Sycamore, IL.
Prochaska, J. O., DiClemente, C. C , Velicer, W. E, Ginpil,
Downloaded from http://her.oxfordjournals.org/ by guest on May 21, 2015
and self-efficacy for condom use. American Journal of
Health Behavior, 20, 406-416. S. E. and Norcross, J. C. (1985) Predicting change in
Horn, D. (1976) A model for the study of personal choice smoking status for self-changers. Addictive behaviors, 10,
health behavior. International Journal of Addiction, 19, 395-406.
179-185. Prochaska, J. O., Velicer, W. E, DiClemente, C. C. and
Janis, I. L. and Mann, L. (1977) Decision Making: A Fava, J. (1988) Measuring processes of change: Applications
Psychological Analysis of Conflict, Choice, And to the cessation of smoking. Journal of Consulting and
Commitment. Cassel and Collier Macmillan, London: Clinical Psychology, 56, 520-528.
Kelly, J. A., Murphy, D. A., Sikkema, K. J. and Kalichman, Prochaska, J. O., DiClemente, C. C , Velicer, W. F. and
S. C. (1993) Psychological interventions to prevent HIV Rossi, J. S. (1993) Standardized, individualized, interactive,
infection are urgently needed: new priorities for behavioral and personalized self-help programs for smoking cessation.
Health Psychology, 12, 399-405.
research in the second decade of AIDS. American
Psychologist, 10, 1023-1034. Prochaska, J. O., Harlow, L. L., Redding, C. A., Snow, M. G.,
Rossi, J. S. and Velicer, W. E (1990) Stages of change, self-
Lam, C. S., McMahon, B. T., Priddy, D. A. and Gehred-
efficacy, and decisional balance for condom use with a high-
Schultz, A. (1988) Deficit awareness and treatment risk sample. Centers for Disease Control and Prevention,
performance among traumatic head injury adults. Brain Atlanta, GA (contract grant 0-415-002).
Injury, 2, 235-242.
Prochaska, J. O., Rossi, J. S. and Wilcox, N. S. (1991) Change
Marcus, B. H., Rakowski, W. and Rossi, J. S. (1992) processes and psychotherapy outcome in integrative case
Assessing motivational readiness and decision making for research. Journal of Psychotherapy Integration, 1, 103-120.
exercise. Health Psychology, 11, 257-261. Prochaska, J. O., Velicer, W. E, Rossi, J. S., Goldstein, M. G.,
Marcus, B. H., Rossi, J. S., Selby, V. C , Niaura, R. S. and Marcus, B. H., Rakowski, W., Fiore, C , Harlow, L. L.,
Abrams, D. B. (1992) The stages and processes of exercise Redding, C , Rosenbloom, D. and Rossi, S. R. (1994)
adoption and maintenance in a worksite sample. Health Stages of change and decisional balance for twelve problem
Psychology, 11, 257-261. behaviors. Health Psychology, 13, 39-46.
McConnaughy, E. A., DiClemente, C. C , Prochaska, J. O. Project CARES Working Group. (1994, Revised) Project
and Velicer. W. F. (1989) Stages of change in psychotherapy: CARES: Advocates' Guide to Stage of Change Counseling
a follow-up report. Psychotherapy: Theory, Research, and (Draft manual). Division of Reproductive Health, National
Practice, 4, 494-503. Center for Chronic Disease Prevention and Health Promotion,
McConnaughy, E. A., Prochaska, J. O. and Velicer. W. F. Centers for Disease Control and Prevention.
(1983) Stages of change in psychotherapy: measurement Roper, W. L., Peterson, H. B. and Curran, J. W. (1993) Condoms
and sample profiles. Psychotherapy: Theory, Research, and and HIV/STD prevention: clarifying the message. American
Practice, 20, 368-375. Journal of Public Health, 83, 501-503.
Morrill, A. C. (1994) An interpersonal model of HIV risk Rosenberg, M. J. and Weiner, J. M. (1988) Prostitutes and
for heterosexual women. Paper presented at the American AIDS: a health department priority? American Journal of
Psychological Association Conference: Psychological and Public Health, 78, 418-423.
Behavioral Factors in Women, Washington, DC. Sacco, W. P., Rickman, R. L., Thompson, K., Levine, B. and
O'Leary, A. (1985) Self-efficacy and health. Behavioral Reed, D. L. (1993) Gender differences in AIDS-relevant
Research and Therapy, 23, 437- 451. condom attitudes and condom use. AIDS Education and
O'Reilly, K. R. and Higgins, D. L. (1991) AIDS community Prevention, 5, 311-326.
demonstration projects for HTV prevention among hard- Shiftman, S. (1986) A cluster analytic classification of smoking
to-reach groups. Public Health Reports, 106, 714-720. relapse episodes. Addictive Behaviors, 11, 295-307.
Prochaska, J. O. (1989) What causes people to change from Soskolne, V, Aral, S. O., Magder, L. S., Reed, D. S. and
unhealthy to health enhancing behavior? In Cummings, Bowen, G. S. (1991) Condom use with regular and casual
C. C. and Floyd, J. D. (eds), Human Behavior and Cancer partners among women attending family planning clinics.
Risk Reduction: Overview and Report of a Conference on Family Planning Perspectives, 23, 222-225.
74You can also read