(CFF) Consolidated Funding Framework 2018-2019 Support Pack
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Consolidated Funding Framework
(CFF)
2018-2019 Support Pack
1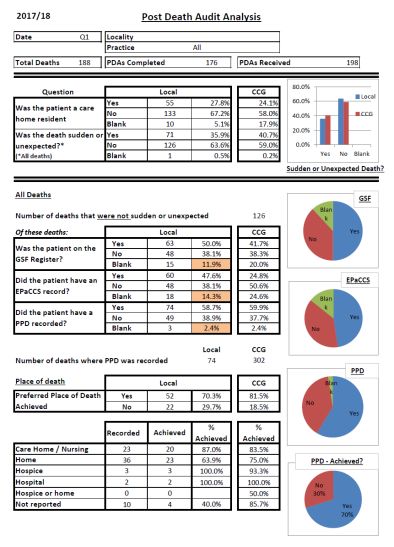
This page left intentionally blank
2
Contents
This support pack is intended to be printed as a whole on both sides, so some pages have been left
intentionally blank. Individual copies of each item are available on the CCG website and can be found at
the following link http://www.enhertsccg.nhs.uk/consolidated-funding-framework-year-2-201819
Item Item Details Page
A1 Foreword 5-6
A2 CFF Sign-up Sheet 18-19 7-8
Financial Balance
B1 Financial Balance – Guidance 9
Engagement
Engagement Guidance: Clinical Representation , PPG Engagement and
C1 Patient Communication, Collaborative working and Workforce and skills data. 11-12
C2 PPG Engagement Plan Template 13
C3 PPG Engagement Progress Report Template 14
C4 Collaborative Working Project Plan Template 15
C5 Collaborative Working Progress Report Template 16
C6 Collaborative Working Project Evaluation Template 17
Frailty and Care Management
D1 Care Planning Guidance 19-22
D2 Catheter Register Guidelines 23-26
D3 GSF/MDT Guidelines 28-31
D4 GSF/MDT Meeting Template 32
D5 Post Death Audit Guidance 34-36
D6 Post Death Audit Report Tool 38-39
D7 Post Death Audit Report access and guidance 40
D8 Mental Health Dementia Care Planning Guidance 42-44
Mental Health Physical Health Check for Serious Mental Health (SMI)
D9 Patients 46-50
Diabetes and Diabetes Prevention Guidance and Improvement Plan
D10 Template 52-56
Cancer
E1 Cancer Guidance 58-59
E2 Cancer Campaign Timetable 60
E3 Practice Cancer Plan Template 62-63
E4 Locality Cancer Plan Template 64
E5 Cancer Quarterly Return Template 66-67
E6 Breast Screening Letter Template 68
Planned Care
F1 CCG Pathway and Thresholds Assessment Guidance 70
F2 Medicines Optimisation Guidance 72-76
3This page left intentionally blank
4Item A1 - Foreword
East and North Herts CCG:
Consolidated Funding Framework (CFF) 2018-19
Foreword:
Aim and Purpose – This is the second year of the CFF, which is an investment of nearly £6m into
primary care and general practice by the CCG Governing Body. The main aim of CFF funding is to
give extra capacity to primary care operating in an integrated and collaborative way in order to
help address the ever increasing demand and workload on primary care.
CFF 2017-18 – This has been reviewed with practices and key changes made to the 2018-19 CFF
include, simplification – from 17 clinical sections to 12, simplified reporting and monitoring to
reduce practice workload and limited changes/new items. Some areas have been dropped
completely such as Children’s A+E frequent attendees.
CFF 2018-19 – has been jointly developed during January and February with practice
representatives’ patient groups and LMC input. There are limited new elements such as PPG and
Locality controlled collaborative working funds. We have tried to build on the successful elements
of the 2017-18 CFF and amended funding and monitoring especially where it was not clear what
metrics were being used to trigger payments.
The CFF has 5 sections: 2 non Clinical (25%) and 3 Clinical (75%) TOTAL £10.10 per patient.
Non Clinical Clinical
Financial Balance Engagement Frailty/Care Planning Cancer Planned Care
£1.50 £1.0 (4 elements) £4.75 (6 elements) £1.75 (3 elements) £1.10 (3 elements)
LCC per practice CARE Plans Awareness Practice pathway
PPG engagement New and review Training compliance
Workforce returns Mental health Screening Practice threshold
Locality Dementia Improvement and referral
Collaboration SMI Health Checks Breast compliance
Funds Diabetes Cervical Medicines
NDPP Bowel Management
8 Care Processes Case Review and
MDT/GSF Support Pathway/patient
Catheter Register experience
Post Death Audits improvement
Mandatory Elements – The 2 mandatory elements remain the same as in 2017/18 namely.
Pseudonymised data extraction to improve risk stratification and system data integration
Record sharing by consent. Practices to ask patients for consent to share as part of care
planning process and record number of patients who decline to allow sharing.
Proper safe record sharing is key to enabling safe integrated working for the benefits of complex
comorbidity patients. We are trying to move to a single system care record for the patient and the
CFF is attempting to support this major system wide objective.
5New Localities Structure – The CCG Governing Body and the STP are moving towards an
integrated care system (ICS) and the Governing Body has re-organised GP leadership roles to
enable primary care to lead on this and achieving a more sustainable primary care, as well as
integrated place based care linked to the primary care home model.
There will be a two tier meeting system from April 2018 for Localities to support the delivery of
CCG and system objectives as set out in the CCG Operating Plan for 2018-19. The CFF is
supporting practice engagement in each Locality Commissioning Committee which is accountable
to the Governing Body for improving the health of their population and ensuring Integrate Care
Delivery Boards (ICDB) deliver local service transformation and service performance targets as
part of the NHS Constitution and Mandate.
Locality Commissioning Committees (LCC) – are formally committees of the Governing Body and
will have their own Local Commissioning Plan and priorities for which the local Integrated Care
Delivery Board (ICDB) will be the vehicle for delivery. The CFF is intended to empower the LCC
and the LCC will be where practices can make a case for exceptionality or special circumstances
where CFF payments are concerned. Each LCC will have an oversight role on the CFF and where
there are any obvious conflicts of interest issues then the problem will be escalated to the CCG
and the Primary Care Committee (PCC) which will act on behalf of the Governing Body on GMS
delegation and Locally Enhanced Services including the CFF. It is expected that all practices will
be part of their local LCC and attend at least 6 of the 7 planned meetings over the year.
Integrated Care Delivery Boards (ICDB) and other GP/Clinical support – The expectation is that
Locality practices will agree locally who will represent practices/general practice on the ICDB. The
expectation is that between 2 and 4 members will be representing their Locality practices as all
practices are not needed at ICDB meetings as well as LCC meetings. A Federation for example
may be selected to represent all practices in one ICDB, or practices could chose to attend by town
or rural representation. The ICDB is linked to the STP Place Based Care Delivery Board system
as well as the CCG – LCC accountability line.
CFF 2018-19 – Aligns the incentives for practices with developments in primary care and the
GPFV especially the extended access agenda and we hope further innovation and change across
the health and social care system will benefit patients such as more MDT working and moving to
30-40 minute appointments for complex frail patients.
Monitoring and Reporting – will be done through new Locality Information Packs at each LCC and
there will be CCG – wide commissioning workshops to share best practice as well as address
problems and issues raised during implementation.
Quarterly Submission Dates – Practices to report back to the CCG on a quarterly basis. The
submission dates are as follows:
Q1 – Monday 16th July 2018
Q2 – Monday 15th October 2018
Q3 – Monday 14th January 2019
Q4 – Monday 15th April 2019
6Item A2 – CFF Sign-up Sheet 2018-2019
Consolidated Funding Framework (CFF) 2017-19
Year 2 – 2018-2019
Practice sign up form
Practice Name
Practice Number
Locality
Practice Declarations
As part of the CFF, practices are asked to identify a Lead for the below areas:
Please provide the appropriate information, and if during the CFF these positions
change within the practices, practices will need to alert the CCG Commissioning
team on Enhccg.localities1@nhs.net and advise of the same information for the new
lead.
Lead role: GSF Co-ordinator
Lead Name
Position in Practice
Contact email
Contact Telephone number
Lead role: Diabetes Lead
Lead Name
Position in Practice
Contact email
Contact Telephone number
Lead role: Cancer Champion
Lead Name
Position in Practice
Contact email
Contact Telephone number
7I confirm that the practice named overleaf signs up to the Consolidated Funding
Framework for 2018/19, and will comply with the core requirements set put in the
CFF metrics for 2018/19. The authorised signatory will be the dedicated CFF lead
for the practice.
I confirm that the practice representatives identified overleaf will comply with the
positions and roles assigned to them on behalf of the practice.
This declaration confirms that the practice will promote early presentation activities
for the Cancer element of the CFF as per the guidance provided. The practice will
work with the CCG to promote national and regional cancer campaigns, including Be
Clear on cancer, will take part in the cancer case analysis, case reviews and 6
months reviews and education and training throughout the year.
The practice will engage with the PPG to help promote and support the campaigns
and have a program of activity
This declaration confirms that the practice will comply with the CCG Pathways and
Implement Thresholds Assessment elements of the Planned Care Section of the
CFF Metrics and guidance documentation.
Any elements of the CFF the practice will not be signing up to are declared in the
table below:
Element Reason for abstaining
Authorised Signatory
Name (print)
Signature
Date
Contact number
Email
Note: No upfront payment will be provided to practices until they have confirmed their sign up to
the CFF including the compulsory element of the metrics
***Please return to the CCG on Enhccg.localities1@nhs.net by 30th April 2018***
8Item B1 – Financial Balance Guidance
Financial Balance Guidance
As stated in the 2018 – 2019 CFF Metrics, the remuneration for the financial balance section is
£1.50 (per registered patient). At the end of the financial year, the overall locality spending is to be
no greater than its agreed budget measured at the end of year when the Accounts are approved in
June 2019.
If a Locality achieves financial balance in 2018/19 (based on assessment by the CCG finance
team following submission of end of year accounts), the Locality will be awarded £1.50 per
registered patient.
If a locality fails to achieve financial balance in 2018/19, the Locality can be awarded up to 50p per
registered patient if it is overspend is less than that recorded in 2017/18.
The funding distribution by Practice will be decided and agreed by the Locality Commissioning
Committee.
Financial balance will be monitored and measured by the CCG and reported on following approval
of the CCG’s Accounts in June 2019. The locality finance reports will provide an indication
throughout the year on how localities are performing.
END
9This page left intentionally blank
10Item C1 – Engagement Guidance
Engagement Guidance
This guidance is designed to be read in tandem with the detail provided in the Metrics. The aim of
the engagement section of the CFF is summarised in the metrics. Meeting attendance per se is an
inexact measure for assessing engagement, and so while attendance at meetings is important, it
is important that other measures of engagements are also covered in this section.
Meeting Attendance
The CCG Localities workshops are new meetings, and will be an opportunity to tackle areas which
are of relevance to the entire CCG. The topic areas may cover areas such as diabetes, GDPR,
extended access or others, with an aim of sharing best practice either locally or nationally, and
enabling learning across the CCG.
Localities may choose to arrange Task and Finish groups to undertake specific agreed pieces of
work, for which locality management funds may be used to appropriately reimburse clinical time,
as approved by the relevant Locality Commissioning Committee. The Locality Commissioning
Committee may choose to approve the funding of locality management funds for agreed Task and
Finish Groups through a virtual meeting process (held via conference call facilities with formal
recording of the funding request and the decision and approval) should approval be required within
a more rapid time frame.
Metrics and other guidance is provided in the Metrics section. All meeting attendance will be
monitored via meeting minutes and/or records of attendance.
PPG Engagement and Patient Communication
Practices to improve PPG engagement and encourage use of the ‘building better participation’
toolkit developed by NAPP (the national association for patient participation) which can be found
at the below link.
http://www.napp.org.uk/
Practices are to use the range of resources available including planning sheets and self-
assessments. Building better participation is designed for use by a PPG working alongside its GP
practice.
You are not expected to work through all four Areas and all their Goals.
This tool is designed for you to pick and mix from the Goals, as is appropriate to your PPG and
your practice. You may decide to focus on several Goals within some Areas, while not looking at
others.
If the PPG wants to make use of the four Areas of Building better participation we recommend
that, initially, you review them with some PPG members and your practice together. We suggest
you concentrate at first on the Goals that are most relevant to your PPG.
Things you might discuss with your PPG and practice:
• Which Goals are relevant to you to work on?
• How you might show you are meeting each Goal?
• How you would use the Goals to help set action plans for the year ahead?
11Practices are to complete the PPG engagement plan template based on locality and practice
clinical priority areas and submit a copy of the plan at the end of Q1 2018. Practices will then
provide evidence of progress in implementing at least 2 key actions at the end of Q4.
An engagement plan template and progress report template will be provided by the CCG.
Collaborative Working
This is not to be used for a service that is already funded from another source. The localities may
choose to combine the resources from this section of the CFF with other funding sources if
appropriate to enable the delivery of the project.
A written project proposal (Item C4) will be submitted to and formally approved by the Locality
Commissioning Committee by the end of Q1. Localities may choose to use another template
should they prefer, or to submit additional information, but all key areas contained within the
template plan must be addressed in the project plan. Planning and implementation will comply with
the CCG policy on remuneration (if relevant to the locality plan).
The project needs to be duration of a minimum of six months and a maximum of 12 months.
A further template is provided (Item C5) for monitoring progress, which localities may use should
they find this helpful. An evaluation template (Item C6) is provided which must be used and
submitted to the Locality Commissioning Committee at the completion of the project.
Workforce and Skills Data
Practices are to complete the workforce data template, and workforce skills/training needs
template as sent out by the Primary Care workforce and Education team directly. These will be
sent to practices each quarter, with no fixed template as they will be standardising workforce and
skills data collection across the STP so the template may change during the year.
END
12Item C2 – PPG Engagement Plan
13Item C3 – PPG Engagement process Report
14Item C4 – Collaborative Working Project Plan
15Item C5 – Collaborative working – Progress Report
16Item C6 – Collaborative working – Evaluation Report
17This page left intentionally blank
18Item D1 Care Planning Guidance
Frailty and Care Planning
Care Planning in Primary Care - CFF 18/19
Background
Care and support planning with people with long term conditions (LTC’s) is about better
conversations - emphasising the importance of the care and support planning process itself in
achieving outcomes, rather than the written care plan that may emerge at the end.
This guidance provides details on which care plan should be used and where to find it. The
documents in this guidance are all patient held documents and there is an expectation that
these will be given to the patient. In addition, the professional care plan requirements will be met
by the use of templates, sharing of information and details of both are provided below.
What do I need to do?
1) Identify your cohort of patients
1.1 Identify the total number of patients that are in need of a care plan as per the list below:
Patients who are or are at risk of:
Frequent attendance at A and E or Ambulatory Care
Pneumonia / LRTI (Lower Respiratory Tract Infections) or regular COPD exacerbation
End stage Long Term Conditions:
o CHF (Congestive Heart Failure) NYHA (New York Heart Association) Stage 3/4
or
o COPD MRC(Medical Research Council) stage 4/5 or O2 therapy or
o CKD (Chronic Kidney Disease) Stage 4/5 or rapidly declining neurological
conditions)
o Those that exacerbate frequently
Frequent admissions (greater than or equal to 2 admissions per annum)
End of Life (within the last 12 months of life) or graded as moderately or severely frail
Carers who support very vulnerable patients
Some patients may fall into more than one category - please only count them once.
1.2 From that list of patients confirm how many already have a care plan
This will provide your baseline figures
Total number of patients Number with a care plan Number without a care
plan
X Y Z
Target numbers are
a. New care plans = 70%
b. Review of care plans = 30%
19Example
Total number of patients Number with a care plan Number without a care
plan
100 20 80
a. New care plans = 70% (of 80) = 56 care plans
b. Review of care plans = 30% (of 20)= 6 care plans
2) Completing Care Plans
2.1 Which Care Plan?
SystmOne - Ardens Users SystmOne - Non Ardens EMIS Web
Users
Use the relevant condition Continue to use the Continue to use the same
specific templates to capture key same Personal Care Personal Care Plan that
information. Plan that you used for you used for 17/18 and
17/18 and have used in have used in previous
Use the LTC review template to previous years as part of years as part of the
help you identify which condition the avoiding unplanned avoiding unplanned
specific plans the patient needs. admissions DES. admissions DES.
- Click on future care planning
- Click on Generic Care Plan Ensure patients are Ensure patients are
(This is the foundation correctly coded with a correctly coded with a GSF
document) - make sure you GSF stage / Frailty code, stage / Frailty code, where
select the code from the drop where appropriate. appropriate.
down box
- Click on Specific Care plan - Signpost patients (where Signpost patients (where
this will take you to the self- appropriate) to self- appropriate) to self-
management plans for management support on management support on
specific conditions the Health in Herts the Health in Herts
webpages. webpages.
Signpost patients (where
appropriate) to self-management For end of life patients: For end of life patients: Ask
support on the Health in Herts Ask for consent to add for consent to add
webpages information to the information to the summary
summary care record. care record. Use the
For end of life patients: Ask for Use the EPaCCS leaflet EPaCCS leaflet
consent to add information to the to explain how this works
summary care record. Use the
EPaCCS leaflet
Further step by step guidance
can be on the CCG website
20Read Codes CTV3 (e.g. EMIS
SystmOne)
Personal Care Plan offered XaRB3 9NS5.
Offer of Personal Care Plan accepted XaRB2 8CMF.
or Personal Care Plan completed
Personal Care Plan declined XaRB0 8IAe
Review of Personal Care Plan XaRB1 8CMC
3) Next Steps
3.1 Sharing the Care Plan
Once you have identified your cohort and completed the care plans, you need to ask for consent
from the patient to share information.
With the patient:
Print or email the documents to the patient
With other professionals
With the permission of the patient, practices can add additional information about specific
conditions to the summary care record to make it an enhanced summary care record.
Once you have selected this read code and saved the record, there is nothing further for
you to do as the system will automatically upload the information.
Patients at S1 practices can consent to having their whole record shared with other S1
users e.g. hospices and this will give a more in depth picture to other health care
professionals
More information can be found here: http://www.hblict.nhs.uk/scr/#toggle-id-8
The sharing of patient records and care plans/treatment plans is part of the wider “My Care
Record” project
For patients identified with severe frailty, promotion of the summary care record and
activation of this is part of the GMS contract (see section 4.2)
Ardens users can use the “Sharing Records” template to record patient consent - look for
this icon on any of the templates.
3.2 GSF Register
Patients who are end of life or severely frail should be added to the GSF register
These patients should be discussed at the GSF meetings (where appropriate)
4) Payments
Payments will be made as follows:
a. New care plans = £150
b. Review of care plans = £50
214.1 Change from Previous Year
Payments for severe frailty care plans in 2017/18 was £200 as not only was a care plan required,
but as part of the care planning process, these patients should have been discussed in the GSF
meetings.
The difference of £50 for severe frailty care plans has been moved to support GSF meetings.
4.2 Review of care plans
Payment will be made for each review of a care plan. Therefore if a patient is reviewed twice in the
year (if required) then the total payment for review will be £100 for the year.
For patients who are identified as severe frailty, the GMS contract for 2017/18 states:
7.1 LEVEL OF SKILL
7.7AA.3 Where the Contractor identifies a patient aged 65 or over who is living with severe
frailty, the Contractor will:
7.7AA.3.1 Undertake a clinical review in respect of the patient which includes:
(a) An annual review of the patient's medication; and
(b) Where appropriate, a discussion with the patient about whether the patient has fallen in the last
12 months.
7.7AA.3.2 provide the patient with any other clinically appropriate interventions; and
7.7AA.3.3 where the patient does not have an enriched Summary Care Record, advise the
patient about the benefits of having an enriched Summary Care Record and activate that record at
the patient's request.
Care planning for patients identified as severe frailty is technically covered under GMS contract as
a care plan is a clinically appropriate intervention. However, for the CFF for this year we are not
excluding these patients and the allocations for both new care plans and reviews is intended to
support practices with any additional work required.
END
22Item D2 – Catheter Register Guidance
Catheter Registers (Adults >18 years)
Through the Best Practice UTI & Urinary Catheter Care Forum, there have been reports of
patients with long-term catheters that have not been referred for appropriate follow-up. The
introduction of ‘catheter registers’, which are to be maintained by individual GP practices, will
ensure that all patients discharged from hospital with a catheter have the appropriate plans in
place for ongoing management and support.
Baseline Submission
To initiate this metric, GP practices should identify all existing catheter patients from their clinical
systems. A clinical report (for SystmOne and EMIS) has already been published to support this,
and further guidance can be made available if required. Practices should also check to see if any
of the long term catheter patients identified have been referred to the community services (and
complete a referral if not).
In addition to forming the basis of a catheter register, this will ensure that any existing long term
catheter patients are receiving the appropriate level of support. For consistency, practices may
choose to re-code existing catheter patients using the codes below.
At the end of quarter one (and in addition to the standard reporting outlined below), practices will
need to submit the following baseline figures:
Number of patients with existing catheters (identified from clinical systems);
Number of referrals to the community as a result of initial review.
Register Management (from April 2018)
GP practices should utilise hospital discharge summaries to identify patients that have left hospital
with a catheter in situ. The following clinical codes should then be used to ensure these individuals
are captured on practice registers:
SystmOne Code SNOMED CT Code
Table 1
(CTV3) (Concept IDs)
*Indwelling Catheter XE0iD 266737003
(Indwelling urethral catheter) (Indwelling urethral catheter)
- Urethral catheter Xa3du 34759008
(Urethral catheter) (Urethral catheter)
- Suprapubic catheter Xa3dh 286861005
(Suprapubic catheter) (Suprapubic catheter)
23EMIS Web Code SNOMED CT Code
Table 2
(Read V2) (Concept IDs)
*Indwelling Catheter 8D74. 266737003
(Indwelling urethral catheter) (Indwelling urethral catheter)
7B2Bz 410021007
- Urethral catheter (Urethral catheterisation of bladder
(Urethral catheterisation)
NOS)
- Suprapubic catheter 8D76. 440311000
(Suprapubic catheter in situ) (Suprapubic catheter in situ)
*Where the catheter type (i.e. urethral or suprapubic) is not clearly referenced in the discharge summary, practices
can opt to use the top level code (‘Indwelling urethral catheter’).
*Using the codes above will enable GP practices to report on the number of patients added to their catheter register
during a specified period (e.g. quarter 1).
*The codes in the blue columns will automatically map to SNOMED CT codes (although it should be noted that the
current mapping is subject to change).
*Note on coding: practices can opt to continue using existing codes, as opposed to the ones above (which have
been included in this guidance to support practices to maintain a simple catheter register). However, it should be
noted that this metric may include random practice audits across the year, hence it is important to implement a clear
system.
In addition to the above, practices will also need to record (as free text or using existing read
codes) whether patients have been:
supplied with an escalation plan;
supplied with a catheter passport;
provided with catheter equipment;
referred to TWOC clinic;
referred to Hertfordshire Community Trust (HCT).
The date and reason for catheter insertion should also be recorded in patient notes. This will
enable the community services to manage patients more effectively (including providing a
catheter passport where required).
Any instances where the information above (including catheter type) has not been captured in a
discharge summary should be reported to the CCG GP Hotline for escalation. When reporting an
issue, practices will need to supply the following details:
patient NHS number;
hospital discharged from (including ward if possible);
summary of missing information (as per the checklist above).
It is recommended that GP practices maintain a simple log of all escalations to the CCG (including
date, reason for escalation, etc.). This will enable them to complete the quarterly returns
spreadsheet.
In addition to maintaining an electronic catheter register, GP practices will need to refer all long
term catheter patients to HCT (as per the existing Integrated Community Team referral process).
This will ensure that no patients are lost to follow-up.
24*Note: it should be evident, from a discharge summary, whether the catheter is long or short term.
If this information is not included, the CCG should be notified as per the process above.
*Note: because SystmOne and EMIS Web are not currently interoperable, EMIS practices will
need to ensure that the ICT referral form is populated with sufficient information before referring
(e.g. date of catheter insertion, reason for insertion, etc.).
If a patient presents for a consultation with a previously un-documented catheter (i.e. there is no
record of the practice being informed that the patient was discharged from hospital with a catheter
in situ), GP practices will need to add a code to their record and refer to HCT if required. In
addition, practices should notify the CCG (via the GP Hotline) of any such cases so they can be
raised as a clinical incident. For quarterly reporting purposes, it is recommended that practices
utilise the log discussed above to record any such escalations.
Repeat dispensing of catheter equipment (e.g. leg bags) should also be used as an opportunity to
identify, code and report previously un-documented catheters still in situ.
Information required for escalation by CCG:
patient NHS number;
Notification that practice was not informed of catheter insertion;
Assumed place of discharge with catheter.
GP practices will also need to document catheter removals (e.g. after a successful TWOC in the
community). This can be achieved by using the following clinical codes (and supporting free text
where required):
SystmOne Code SNOMED CT Code
Table 3
(CTV3) (Concept IDs)
*Indwelling catheter removed XE0it 266768004
(Indwelling catheter removed) (Indwelling catheter removed)
- Removal of urethral catheter 7B2B2 55449009
(Removal of urethral catheter) (Removal of urethral catheter)
- Removal of suprapubic 7B2C2 75325006
catheter (Removal of suprapubic catheter) (Removal of suprapubic catheter)
EMIS Web Code SNOMED CT Code
Table 4
(Read V2) (Concept IDs)
- Removal of urethral catheter 7B2B2 55449009
(Removal of urethral catheter) (Removal of urethral catheter)
- Removal of suprapubic 7B2C2 75325006
catheter (Removal of suprapubic catheter) (Removal of suprapubic catheter)
*Note on coding: practices can opt to continue using existing codes, as opposed to the one above (which has been
included in this guidance to support practices to maintain a simple and reportable catheter register). However, it
should be noted that this metric may include random practice audits across the year, hence it is important to
implement a clear system.
In order to support GP practices to achieve this aspect of the metric, local provides (including
HCT) will be instructed to provide clear, physical confirmation (e.g. discharge summaries) when a
25catheter has been removed. This will enable practices to monitor and report on catheter removals
on a quarterly basis.
Sharing patient records will provision HCT with the ability to directly update patient records
(SystmOne only). In turn, this will enable community teams to code when a catheter has been
removed (using the tables above). However, HCT will still be expected to provide physical
confirmation that a catheter has been removed, and that the appropriate codes have been applied
to the patients record. This will enable SystmOne practices to confirm that records have been
updated appropriately. It will also ensure consistency across the CCG.
The vast majority of short term catheters will be removed in a TWOC clinic shortly after insertion.
Both SystmOne and EMIS Web practices will therefore need to review clinic letters to identify
catheter removals, and then code appropriately using the tables above (if required). This will
ensure that registers are kept up to date (regardless of whether catheters are short or long term).
Any issues relating to catheter removal notifications should be escalated to the GP Hotline for
resolution.
CCG and Local Providers
In addition to ensuring that directly affected providers understand the requirements of this scheme,
the CCG will be working with local hospitals to improve discharge processes. It is therefore
anticipated that the number of cases requiring escalation to the CCG will reduce significantly over
the next twelve months.
The CCG is also prepared to respond to any issues identified by practices, and provide further
guidance where requested.
Quarterly Reporting
The following metrics will need to be reported on a regular basis:
Metric Reporting Frequency Measurement
Register list size at end of quarter
Quarterly Count
(accounting for additions and removals).
Number of patients added to register
Quarterly Count
during quarter.
Number of patients removed from register
Quarterly Count
during quarter.
Number of escalations to CCG for
Quarterly Count
incomplete discharge summaries.
Number of escalations to CCG for
Quarterly Count
previously un-documented catheters.
Note on coding: the objectives of this metric do not include changing the way GP practices code catheter activity. If
practices already have systems in place, they can continue to utilise these for the duration of the 18/19 CFF
(assuming they fulfil the reporting requirement’s outlined above). However, it should be noted that this metric may
include random practice audits across the year, hence it is important to implement a clear system.
END
26Item D3 – GSF/MDT Guidance
GSF Meetings - CFF 18/19
Background
On average 0.75% of your practice population will die each year.
Most of these deaths can be predicted.
Identifying patients thought to be in their last years of life enables earlier discussion of their wishes
and improved care at the end of life.
A proactive team approach to the shared care of frail elderly people with multiple co-morbidities,
including cancer, becomes more possible.
Well run meetings support individual clinicians to not only care for their patients better, but to also
care for themselves.
‘Branding’ the meetings as supportive and ensuring the name of your register includes the term
‘supportive’ can make earlier conversations easier.
What do I need to do?
1) Set up the meetings
Identify and train a committed lead administrator with IT and organisational skills. If a GP cannot
attend, the administrator will share important information.
Involve your team – district nurses, community matrons, GPs, GP trainees, clinical nurse specialists,
practice nurses, community specialist palliative care nurses, palliative care consultants, etc.
Agree to set up a regular team meeting at least every 4-6 weeks lasting at least 60 minutes (it will
vary depending on practice size).
2) Identify your cohort of patients
2.1 SystmOne Practices
Ardens have set up a report on S1 that will pull through all the relevant information you need for your GSF
meeting. Even if you are not using the templates, you can still access the report by following these steps:
Go to Clinical Reporting > Ardens > Meetings > End of Life.
Right click the ‘End of Life Registers’ report > show patients.
Click on Select Output > Pre-defined report output > End of Life > Ok
Right > table > open as CSV
27This will provide you with a table that looks like this:
NHS Number
Name SCR-AI Consent GSF Status TEP DNACPR Anticipatory PrescribingPreffered Place of Care Preffered Place of Death
1244 Mrs L On gold standards palliative care framework
1245 Mrs M On gold standards palliative care framework
1246 Mrs N On gold standards palliative care framework
1250 Mr R On gold standards palliative care framework For resuscitation
1257 Miss Y On gold standards palliative care framework Not for attempted CPR (cardiopulmonary resuscitation)
1258 Mrs Z On gold standards palliative care framework Not for attempted CPR (cardiopulmonary resuscitation)Preferred place of care - home
Preferred place of death: pt unable to express prefere
1259 Colonel Mustard On gold standards palliative care framework Not for attempted CPR (cardiopulmonary resuscitation)
1275 Mr C Bing GSF prognostic indicator stage C (yellow) - weeks prognosis
Not for attempted CPR (cardiopulmonary
Issue of palliative
resuscitation)
care anticipatory
Preferred place
medication
of care -box
home
Preferred place of death: home
1276 Mrs M Gellar GSF prognostic indicator stage C (yellow) - weeks prognosis
Not for resuscitation Issue of palliative care anticipatory
Preferred place
medication
of care -box
care
Preferred
home place of death: nursing home (first choice)
1277 Miss R Green GSF prognostic indicator stage C (yellow)
Treatment
- weeks
Escalation
prognosis
Not
Plan
for resuscitation Prescription of anticipatory
Preferred
care medication
place of care
not- appropriate
care
Preferred
home place of death: nursing home (first choice)
1242 Mr J GSF prognostic indicator stage B (green) - months prognosis
1243 Mr K GSF prognostic indicator stage B (green) - months prognosis
1249 Miss Q GSF prognostic indicator stage B (green) - months prognosis
For attempted cardiopulmonary resuscitation Preferred place of care - home
Preferred place of death: home
1256 Miss X GSF prognostic indicator stage B (green) - months prognosis
Not for attempted CPR (cardiopulmonary resuscitation)Preferred place of care - care
Preferred
home place of death: care home
1270 Mr Dibble GSF prognostic indicator stage B (green) - months prognosis
Not for resuscitation
1273 Mr Bolt Express consent forGSF
coreprognostic
and additional
indicator
SCR stage
dataset
B (green)
upload
Treatment
- months
Escalation
prognosis
Not
Plan
for resuscitation Preferred place of care - home
Preferred place of death: home (first choice)
1279 Mr J Tribiani GSF prognostic indicator stage B (green) - months prognosis
Not for resuscitation Prescription of palliativePreferred
care anticipatory
place of medication
care - care
Preferred
home place of death: nursing home
1255 Mr W GSF prognostic indicator stage A (blue) - yr plus prognosis
Not for attempted CPR (cardiopulmonary resuscitation)Preferred place care - patient
Preferred
unableplace
to express
of death:
preference
pt unable to express prefere
You can then sort patients by GSF status to help you prioritise the patients to discuss and see what
discussions need to take place with the patient e.g. Treatment Escalation Plans, Preferred Place of death.
2.2 EMIS Practices
HBLICT have set up a template for EMIS Practices that will pull through all the relevant information you
need for your GSF meeting. Guidance for this can be found at the following link:
D3a - EMIS GSF Report Guidance (HBLICT to provide April 2018)
283) during the meeting
3.1 Prioritising Patients
Needs based RAG coding helps you to organise your meetings, an option is shown here, but others
exist:
1) Red – last days of life
2) Amber – last weeks of life or increasing decline
3) Green – last months of life or advancing disease
4) Blue – incurable condition but could live for years, e.g. dementia or frailty.
Use your own and other staff’s knowledge of the patient and their health status/closeness to death,
prioritise the most unwell.
Use your prioritisation code as a guide to who to discuss first e.g. patients coded red.
You will not need to discuss every patient on the list at every meeting e.g. stable patients coded
green and blue.
Include new additions since the last meeting and anyone else any team member has concerns
about.
Discuss all deaths since the last meeting including deaths of patients who were not on the register
and sudden or unexpected deaths – consider bereavement care needs.
3.2 Agenda
Plan the meeting; use the agenda as a tool, e.g.:
1) Introductions
2) Red patients (15 mins – include discussion of physical, social, psychological and spiritual
dimensions)
3) Amber patients (30 mins)
4) Green/Blue ‘changing’ patients
5) Review of deaths – celebrating good care and identifying areas to improve
6) Review of relevant admissions/discharges
7) New patients to the register (It is important to record the RAG code at the point of joining the
register).
8) AOB – such as educational points or Significant Event Analysis (SEA, see tip 3.4)
9) Summarise and plan date for next meeting
3.3 Running the meeting
Chair and run the meeting in a positive and supportive way, the issues dealt with can be
challenging, but keep control of time.
Invite the lead/administrator to ensure GP notes are up to date and accurate, and highlight key
areas – especially actions and accountabilities.
Open the patient record when they are being discussed and add any notes as you go through the
list
Follow up agreed actions and responsibilities – plan the next meeting
3.4 Significant Event Analysis
Review outcomes for patients:
Highlight good practice from ‘good deaths’
Patients who died in hospital – was this the preferred place of death?
If not, could the admission have been prevented?
Identify any barriers that prevented a ‘good death’.
• Patients not on the register who died – could they have been identified?
• Encourage a culture of trust and learning from each other.
• Identify training needs of the team, perhaps formalise SEA every six months to highlight
important issues
294) After the meeting
Complete the “GSF meeting record sheet”
Remove the Patient Identifiable data from the spreadsheet (Column A & B)
Send both to the CCG mailbox: ENHCCG.localities1@nhs.net
5) Payments
Practices will be paid on completion of the minimum number of meetings held and subject to
documentation as requested being submitted to the CCG.
30Item D4 – GSF/MDT Meeting Template
GSF Meeting Record Sheet
Date of meeting________________________
Meeting number /8 (you must conduct at least 8 evenly spaced meetings in 12 months.
Name of Surgery _______________________ Named GP Lead
_____________________________
Staff present: (initials and job roles)
No. of patients discussed ____________________________
Actions:
Provider issues that need addressing:
Further comments:
Please send a copy of this completed sheet to ENHCCG.localities1@nhs.net along with the
quarterly submissions.
31This page left intentionally blank
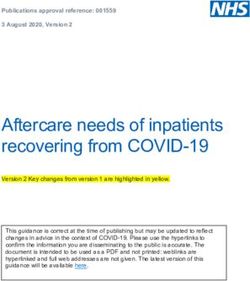
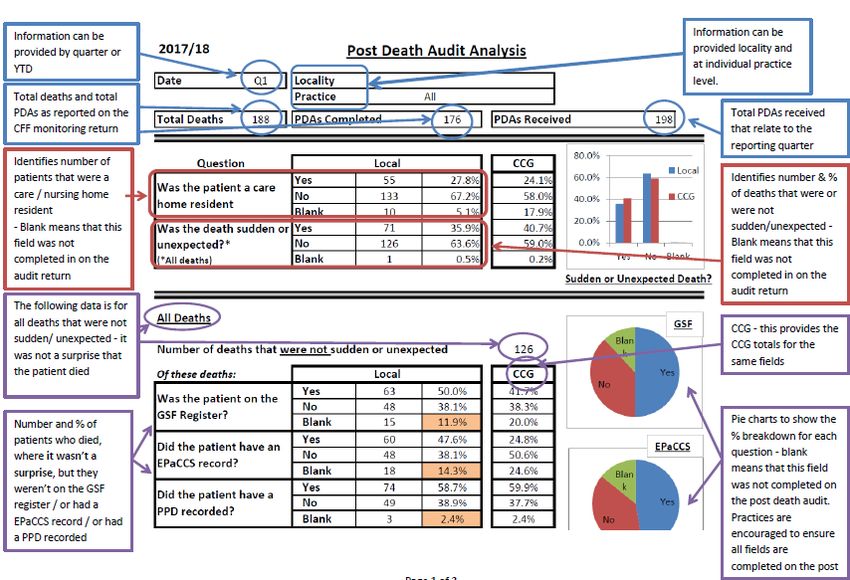
32Item D5 – Post Death Audit Guidance
Post Death Audits Primary Care - CFF 18/19
Background
Post Death Audits (PDA) support the CCG to identify where gaps exist in the palliative and end of
life care pathway. They provide the CCG with a snapshot of issues with current provision and
areas for improvement. This helps to improve the quality of services for patients.
In 2017/18 practices were asked to identify if the patient was a care home / nursing home resident
and which care home this was. This has enabled us to identify care homes that were sending
residents to hospital when they were end of life rather than keeping them at the home. We have
then been able to work with these homes and provide training on end of life care. As a result we
have seen an increase in the numbers of patients achieving their preferred place of death (PPD).
Changes to the Post Death Audit for 2018/19
1) Reporting
The CCG have developed a summary report that will be sent to practices on a quarterly basis.
This will collate the results of the audit at a CCG, practice and locality level. Practices will then
be able to see where they are performing well and where improvements may be made to the
end of life care provided.
Separate guidance has been developed to help practices understand the Post Death Audit
Reports.
2) Changes to / additional questions
2.1 Care Planning
This year we have added the option for practices to state that treatment escalation plans /
DNACPR / addition of information to Summary Care Record has been offered but declined by
the patient. This will allow for a more accurate reporting of those with and without these
elements of an advance care plan.
2.2 GSF register
A priority for the CCG is the early identification of palliative and end of life patients. For this
reason we have added to the PDA “date the patient was added to the GSF register and RAG
33code at that time”. This will enable us to provide you with a breakdown of how long before death
the patient was identified as end of life.
2.3 Preferred Place of Death (PPD)
To enable more accurate recording of the patients PPD, this is no longer a free text box.
Instead this will be either a tick box or drop down box (depending on clinical system) and relate
to the Read codes within the EoL template.
2.4 PPD - not achieved
Again, to enable more accurate recording, PPD not achieved is no longer a free text box.
Instead this will be either a tick box or drop down box (depending on clinical system). This will
allow the CCG to see where there are issues in the pathways that are stopping patients from
achieving their PPD.
3) Completing the Post Death Audits
SystmOne EMIS Web
No change from 2017/18 No change from 2017/18
4) Submitting the Post Death Audits
4.1 SystmOne
Please run the report (no change from 2017/18) and send to: ENHCCG.localities1@nhs.net
4.2 Emis
Please send the completed forms to: ENHCCG.localities1@nhs.net
5) Re-occurring issues from previous years
5.1 Patient identifiable information
Please ensure that any submissions you make do not contain NHS numbers or patient names.
Instead practices should number each one by creating an identifier consisting of:
Practice code
Financial Year
Consecutive number
For example: A12345-17/18-1
For practices that submit the PDA as a word document, please use this format to save/name the
document and not patient names or initials.
345.2 Correct S1 reports
On some occasions practices have submitted the wrong reports. This could be due to the way in
which the reports are being run and practices experiencing issues should contact the HBLICT
helpdesk.
The report should have the headings and look like this:
Did the If the discharge from
Was the patient a patient have Was preferred place of If Yes, did the patient What was the What was the main Were hospital was related to
residential / nursing care If YES, name of residential Was the death an advance Was the patient on Did the patient have an death (PPD) recorded in die in the preferred What was the If PPD recorded but not date of What was the diagnosis for these End of Life, was a clear Was the admission
home resident? / nursing care home Date of death? unexpected? care plan? the GSF register? EPaCCS record? the notes? place of death? PPD? achieved, please indicate why? discharge? cause of death? admission? related? End of Life Plan in the potentially avoidable?
Yes The home 01/04/2018 No Yes Yes Yes Yes Care Home
Yes The home 01/04/2018 No No No Yes Yes Nursing home
No 21/06/2018 Yes No No bed in hospice 15/06/2018 Pneumonia Pneumonia Yes Yes No
No 26/06/2018 No Yes Yes Yes Yes Home Unavoidable admission 10/06/2018 Pneumonia Pneumonia Yes Yes No
6) Payments
Practices payment based on completed quarterly submissions reviewed by End of Life Working
Group. Practices to provide number of deaths and number of post death audits for each month
within the quarterly submissions. Practice to analyse the data quarterly and report on the themes
and any changes to practice procedures, record of date discussed at the MDT/GSF meetings and
agreed actions, time frames and named owner of actions.
35This page left intentionally blank
36Item D6 – Post Death Audit Tool
Post Death Audit Tool
Reference: DoB:
Was the patient a residential / Yes No Date of
nursing care home resident? death:
If YES, name of residential / nursing
care home
Was the death unexpected? Yes No
If No:
Was the patient on the GSF register? Yes No
Date added to the GSF register
RAG code when added to the GSF Register (e.g. red,
amber, green or blue)
Yes and had Yes and No
Was the patient offered a DNACPR
one declined
Yes and had Yes and No
Was the patient offered an advance care plan?
one declined
Did the patient have an EPaCCS record? Yes No
Was preferred place of death (PPD) recorded in the notes? Yes No
If Yes, did the patient die in the preferred place of death? Yes No
What was the PPD?
Hospice or Home (patient choose
Care / Nursing Home both)
Pt unable to express preference
Home
Patient declined discussion
Hospice
Hospital
If PPD recorded but not achieved, please indicate why?
Admitted to hospice for specialist care - died in
hospice
Admitted to hospital by paramedics / 111 / OOH
Bed unavailable at hospice
Other
Unable to remain at home - rapid deterioration
Unavoidable hospital admission - died in hospital
THE REMAINDER OF THE TOOL ONLY NEEDS COMPLETING IF PATIENT DIED WITHIN
30 DAYS OF DISCHARGE FROM ACUTE HOSPITAL
37What was the date of discharge?
What was the cause of death?
What was the main diagnosis for admission?
Were these related? Yes No
If the discharge was related to End of Life, was a clear End of
Yes No
Life plan in the discharge letter?
Was the admission potentially avoidable? Yes No
Note that the tool will be available on GP clinical system
Additional guidance for the Post Death Audit tool can be found below:
For SystmOne Practices – D6a Additional Guidance for Post Death Audit tool - SystmOne
For Emis Practices – D6b Additional Guidance for Post Death Audit tool - EMIS
38Item D7 – Post Death Audit Access Guidance
Understanding the Post Death Audit Report.
Access to the Post Death Audit report can be found on the CCG website link below
D7a Post Death Audit report
Guidance on how to read and use the Post Death Audit, can be found on the CCG website link below
D7 Post Death Audit Access Guidance
39This page left intentionally blank
40Item D8 – Dementia Care Planning Guidance
Dementia Care Planning Guidance
Ensure Care Plans are in place and shared for all patients diagnosed with dementia and
they are being reviewed annually.
Rationale
Patients diagnosed with dementia require robust care plans (and advanced care plans) developed
in primary care.
Who are cohort within this CFF element?
Patients diagnosed with dementia.
Practices are being asked to provide the following to assess impact:
Practices to identify patients diagnosed with dementia who have a care plan in place that
has been shared and has been reviewed annually
1) Identify patients diagnosed with Dementia;
2) Patient to have personalised care planning in place that has been shared with partner
organisations/carers
3) Patients with a personalised care plan have had the care plan reviewed within preceding 12
months
How do I record the information?
SystmOne – Ardens SystmOne – Non Ardens EMIS Web
Users Users
Use the Dementia Continue to use the same Continue to use the same
template to capture key Personal Care Plan that Personal Care Plan that
information. you used for 17/18 and you used for 17/18 and
- Click on Care Plan have used in previous have used in previous
- Click on Generic Care years as part of the years as part of the
Plan make sure you avoiding unplanned avoiding unplanned
select the code from admissions DES. admissions DES.
the drop down box
Signpost patients (where Signpost patients (where
Signpost patients (where appropriate) to self- appropriate) to self-
appropriate) to self- management support on management support on
management support on the Health in Herts the Health in Herts
the Health in Herts webpages webpages.
webpages
41Reporting Requirements/Frequency
Practices to complete Dementia Register and submit data on a quarterly basis:
1) number of patients on register
2) number of patients on register with a care plan
3) number of patients who have had a review within the preceding 12 months
CCG to review submissions quarterly and report to the Dementia Strategy Group.
Agreed payment for care planning
This payment is for those patients who are not moderately or severely frail and who therefore would be
unlikely to otherwise meet the criteria for payment for care plans. Dementia plans will be reimbursed at a
rate of £50 and SMI checks will be reimbursed at a rate of £30.
Sharing the care plan
Once you have identified your cohort and completed the care plans, you need to ask for consent
from the patient to share information.
With the patient:
Print or email the documents to the patient
With other professionals
With the permission of the patient, practices can add additional information about specific
conditions to the summary care record to make it an enhanced summary care record.
Once you have selected this read code and saved the record, there is nothing further for
you to do as the system will automatically upload the information.
Patients at S1 practices can consent to having their whole record shared with other S1
users e.g. hospices and this will give a more in depth picture to other health care
professionals.
More information can be found here: http://www.hblict.nhs.uk/scr/#toggle-id-8
The sharing of patient records and care plans/treatment plans is part of the wider “My Care
Record” project
42Read Codes
SystmOne EMIS & SNOMED Concept
(CTV3 Vision (v2 ID Code (SNOMED
Code) Code) replaces Read
CTV3 & v2 in all GP
systems during
2018)
Dementia care plan XaaBZ 8CMZ 869791000000101
Dementia care plan agreed XacIx 8CMZ0 956841000000106
Dementia care plan declined XacIz 8CMZ2 956881000000103
Dementia care plan reviewed XacIy 8CMZ1 956861000000107
Dementia care plan review declined XacJ0 8CMZ3 956901000000100
Dementia advance care plan XacLx 8CMe0 959361000000105
Dementia advance care plan agreed XabEk 8CSA 713600001
Dementia advance care plan declined XabEi 8IAe0 956881000000103
Dementia advance care plan review
declined XacM2 8IAe2 959461000000102
Review of dementia advance care plan XabEl 8CMG2 956861000000107
END
43This page left intentionally blank
44Item D9 – Physical Health Checks Guidance for SMI Patients
Improving physical health checks for people with severe
mental illness (SMI) in primary care
Rationale
In the Five Year Forward View for Mental health1 NHS England committed to lead work to ensure
that by 2020/21, people living with severe mental illness (SMI) have their physical health needs
met by increasing early detection and expanding access to evidence based physical care
assessment and intervention each year. This element of the CFF is to incentivise practices to
undertake appropriate and timely physical health assessments to reduce the risk of poor physical
health in this population and evidence they have supported patients using available health
information and advice services to take up tests and interventions that reduce the risk of
preventable health conditions.
Who are the people with SMI?
Patients who are diagnosed with schizophrenia, bi-polar affective disorders and other psychotic
disorders. Please note people with SMI may also be identified under other care planning elements
of the CFF.
Practices are being asked to provide the following to assess impact:
4) Identify patients on SMI register;
5) Complete the recommended physical health assessments metrics (not covered via QOF
and/or NHS check) annually for patients with SMI:
a. Whose care has always been solely in primary care, or
b. Who have been discharged from secondary care back to primary care; or
c. Who have been in contact with secondary care mental health teams (with shared
care arrangements in place2) for more than 12 months and whose condition has
stabilised.
6) Follow-up: offer, delivery of or referral to appropriate NICE recommended interventions:
“don’t just screen, intervene”
7) Follow-up: ensure personalised goals and action plan, engagement and psychosocial
support are in place to support physical health
What are the health check requirements?
There is overlap with physical health checks currently being incentivised through different funding
streams that are offered by primary are i.e. Mental Health Quality Outcomes Framework (QOF)
and NHS Health Check for adults between 40-70 years old who have not been diagnosed at risk
of specific conditions.
1
https://www.england.nhs.uk/publication/the-five-year-forward-view-for-mental-health/
https://www.england.nhs.uk/publication/improving-physical-healthcare-for-people-living-with-
severe-mental-illness-smi-in-primary-care-guidance-for-ccgs/
2
HPFT Shared care protocol for physical health checks for patients with SMI
http://www.hpft.nhs.uk/media/1842/item-13a-physical-health-strategy-final-board-paper.pdf
45For the purpose of payment, for this element of the CFF, practices will only receive payment to
complete the outstanding physical health check elements for patients with SMI, that are not
covered by QOF and for those patients not eligible for the NHS Health Check. The purpose of
the CFF payment is to incentivise primary care to annually deliver the following checks
For patients with SMI aged 40-70 years old eligible for NHS Check - metrics
Full blood count*
ECG before starting anti-
psychotic medication if:
(there is family or personal
history of CVD, if a
physical health check
indicates possible risk
(e.g. blood pressure
monitoring, if they are
taking medication known
to cause ECG
abnormalities or if they are
admitted as an inpatient).
Liver function tests*
Prolactin*
Thyroid function tests
Kidney function tests (urea
and electrolytes)
Serum calcium levels
Sexual health and
contraception
Oral health
(* The following results will be accessible to all clinicians and practitioners via ICE or Pathweb)
For patients with SMI NOT eligible for NHS Health Check - metrics
Family History
Smoking Status
Illicit Substance misuse
BMI or other obesity
measure (weight and waist
circumference),
exercise and diet
Total cholesterol, LDL
cholesterol, HDL
cholesterol and
triglycerides
HbA1c and fasting glucose
or random blood glucose*
Full blood count*
ECG before starting anti-
psychotic medication if:
(there is family or personal
history of CVD, if a
physical health check
46You can also read