COVID 19: La Questione Sanitaria - Gianni Di Perri Clinica di Malattie Infettive Università degli Studi di Torino Ospedale Amedeo di Savoia ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID‐19: La Questione Sanitaria
Gianni Di Perri
Clinica di Malattie Infettive
Università degli Studi di Torino
Ospedale Amedeo di Savoia
Ospedale Amedeo di Savoia
CORONAVIRUS
Coronavirus
Coronavirus sp.
Fino al 2002 è stato ai margini dell’interesse scientifico, in quanto causa di episodi infettivi per lo più banali a
carico delle vie aeree superiori (rinite o raffreddore).
Ciononostante, per ragioni di ordine classificativo, ne erano stati caratterizzati 4 tipi su base molecolare:
HCoV 229E
HCoV OC43
HCoV NL63
HCoV HKU1
Malessere Generale
HCoV 229E Cefalea
HCoV OC43 Rinorrea Incubazione: Letalità:
HCoV NL63 Starnuti 2 – 5 giorni nd
HCoV HKU1 Faringodinia
Febbre & Tosse (10 – 20%)
Febbre Malessere Generale Cefalea Rinorrea
Mialgie Starnuti Faringodinia
Cefalea
SARS‐CoV Malessere GeneraleFebbre & Tosse (10 – 20%) Letalità:
Incubazione:
Brividi 2 – 29 giorni 9%
Tosse secca
Dispnea / ARDS
Diarrea (30 ‐ 40%)
Febbre
Tosse
Brividi
MERS‐CoV Faringodinia Incubazione: Letalità:
Mialgie / Artralgie 2 – 13 giorni 35 %
Dispnea / Polmonite
Diarrea / Vomito (30%)
Insufficienza renale acuta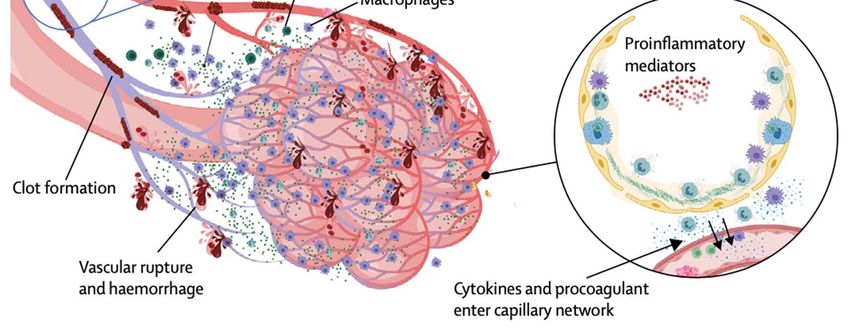
Severe Acute Respiratory Syndrome
(SARS)
Da un punto di vista clinico la SARS è
definibile come una pneumopatia virale
acuta classificabile fra le cosiddette
“Polmoniti Atipiche”, entità già note e
caratterizzate sia in termini eziologici che
fisiopatologici e clinici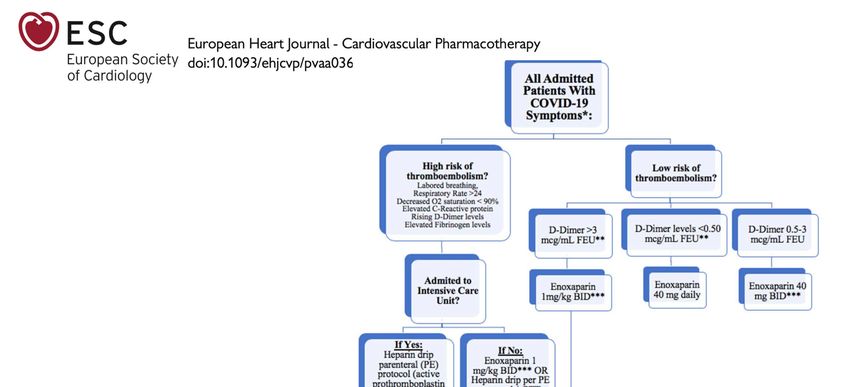
29 marzo 2003: il Dr. Carlo Urbani muore in Thailandia dopo aver contratto la SARS, insieme a 5 infermieri, in Viet Nam, assistendo un malato che ne era affetto. Il Dr. Urbani è stato fra i primi ad accorgersi che si trattava di una nuova entità nosologica ed a redigere in tal senso un rapporto scientifico dettagliato che ne ha permesso una prima definizione medica.
A Chinese doctor who tried to issue the first warning about the deadly coronavirus outbreak has died, the hospital treating him has said. Li Wenliang contracted the virus while working at Wuhan Central Hospital. He had sent out a warning to fellow medics on 30 December but police told him to stop "making false comments". There had been contradictory reports about his death, but the People's Daily now says he died at 02:58 on Friday (18:58 GMT Thursday).
L’origine delle nuove specie di
Coronavirus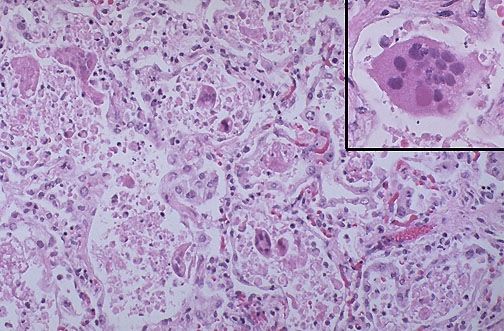
GENETIC RECOMBINATION AMONG DIFFERENT VIRAL STRAINS
Intra‐ and Inter‐Species Transmission of Human Corona‐viruses. Red, yellow, green, blue, brown, and purple arrows represent transmission of MERS‐CoV, SARS‐CoV, NL63, HKU1, OC43, and 229E, respectively, between bats, camels, cows, humans, and masked palm civets (shown in a legend on the side of the figure). Unbroken arrows represent confirmed transmission between the two species in question, and broken arrows represent suspected transmission.
Figure 5. Hypothesis of emergence of type II FCoV. Terada Y, Matsui N, Noguchi K, Kuwata R, Shimoda H, et al. (2014) Emergence of Pathogenic Coronaviruses in Cats by Homologous Recombination between Feline and Canine Coronaviruses. PLOS ONE 9(9): e106534. https://doi.org/10.1371/journal.pone.0106534 https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0106534
Images of the Wuhan Market
from the Web…….it is likely not a matter of if, but when, the next recombinant CoV will emerge and cause another outbreak in the human population……
Il nuovo Coronavirus: SARS‐Cov‐2 il virus, Covid‐19 la malattia
L’evoluzione nel caso di una forma clinica progressiva
Cronologia di un’epidemia familiare
CASO ASINTOMATICO
PUR CON INFEZIONE
DOCUMENTATA80.9% of infections are mild 13.8% severe 4.7% critical Men are more likely to die (2.8%) than women (1.7%). Ranking of death risk according to comorbidity: 1. cardiovascular disease, 2. diabetes, 3. chronic respiratory disease, 4. hypertension. 1716 HCWs infected: 5 died by Feb 11
Epidemiologia
COMMUNITY ACQUIRED INFECTIONS
RESPIRATORY TRACT
INFECTIONS
• Upper RTI‐mostly viral
(Adenovirus, Rhinovirus,
Coronavirus etc.)
• Lower RTI‐mostly bacterial
(Strep pneumoniae,
Haemophilus influenzae,
Mycoplasma pneumoniae,
Legionella pneumophila etc.)
• Acquired from other patients
through droplet infection
• Strep pneumoniae‐from
oropharynx1 2
3Zou L, et al. Higher viral loads (inversely related to Ct value) were detected soon after symptom onset, with higher viral loads detected in the nose than in the throat. The viral load that was detected in the asymptomatic patient was similar to that in the symptomatic patients, which suggests the transmission potential of asymptomatic or minimally symptomatic patients. These findings are in concordance with reports that transmission may occur early in the course of infection and suggest that case detection and isolation may require strategies different from those required for the control of SARS‐CoV.
Zhanwei Du, et al.
Emerg Infect Dis. 2020 Jun
The serial interval of COVID-19 is defined as the time duration between a primary case-patient (infector) having
symptom onset and a secondary case-patient (infectee) having symptom onset.
We estimate a mean serial interval for COVID-19 of 3.96
(95% CI 3.53–4.39) days, with an SD of 4.75 (95% CI
4.46–5.07) days, which is considerably lower than
reported mean serial intervals of 8.4 days for severe
acute respiratory syndrome to 14.6 days for Middle East
respiratory syndrome.
Fifty-nine of the 468 reports indicate that the infectee had
symptoms earlier than the infector. Thus,
presymptomatic transmission might be occurring.
Gray bars indicate the number of infection events with
specified serial interval, and blue lines indicate fitted
normal distributions. Negative serial intervals (left of the
vertical dotted lines) suggest the possibility of COVID-19
transmission from asymptomatic or mildly symptomatic
case-patients.The meeting that infected the world One meeting held in a luxury hotel in mid‐ January spawned several coronavirus cases around the world. More than 100 people attended the sales conference, including some from China.
Un esempio di contagio da SARS‐CoV‐2: Ristorante in Cina
CASO INDICE
Asintomatico, malattia
conclamatasi in serata
CASI SECONDARIFace Shied or Protective Closed Eye Glasses
Head Cover
2‐bed Rooms
2‐bed Rooms
2‐bed Rooms
FFP2 / FFP3 Masks
2‐bed Rooms
Water Repellent Gown
2‐bed Rooms
2‐bed Rooms
Double Gloves Undressing Dressing
OUT IN
OvershoeUntil May 13th, 2020:
163 Doctors died of COVID‐19
Until May 1st, 2020:
41 nurses died + 2 suicided (?)
Until April 29th, 2020:
30 died among Socio‐sanitary staff Members and Pharmacists
Until today (May 14th, 2020) total n. of infections officially recorded
in Italy: 222.104
Nearly 11% (24.431) are HCWsPopolazione: 1,386 miliardi (2017) (1960: 0.65 miliardi, 1980: 1 miliardo)
Cinesi in Italia: 299.823 su 5.255.503 stranieri in Italia
(5,7%)
Superficie del Territorio: 9.597.000 km²La Distribuzione della Popolazione Cinese in Italia al 1° Gennaio 2019 Questi dati riflettono in maniera indiretta anche la distribuzione della popolazione italiana che frequenta la Cina per motivi professionali
1° Gennaio 2019 % su Pop. Variaz.
Totale % Straniera Anno Prec.
1. Lombardia 34.182 34.930 69.112 23,1% 5,85% +3,7%
2. Toscana 28.467 27.617 56.084 18,7% 13,44% +7,5%
3. Veneto 17.831 17.883 35.714 11,9% 7,13% +3,1%
4. Emilia‐Romagna 15.132 15.024 30.156 10,1% 5,51% +1,8%
5. Lazio 12.503 12.741 25.244 8,4% 3,69% +1,8%
6. Piemonte 78.9% 10.053 10.038 20.091 6,7% 4,70% +0,8%
7. Campania 7.455 6.360 13.815 4,6% 5,21% ‐1,9%
8. Marche 4.839 4.674 9.513 3,2% 6,95% ‐0,3%
9. Sicilia 3.788 3.618 7.406 2,5% 3,70% ‐0,5%
10. Puglia 3.139 2.969 6.108 2,0% 4,40% +3,9%
11. Liguria 2.684 2.724 5.408 1,8% 3,70% +8,5%
12. Abruzzo 2.217 2.160 4.377 1,5% 4,90% +1,6%
13. Friuli Venezia Giulia 1.903 1.958 3.861 1,3% 3,50% +2,6%
14. Sardegna 1.779 1.658 3.437 1,1% 6,15% +1,9%
15. Calabria 1.556 1.472 3.028 1,0% 2,68% ‐3,8%
16. Umbria 1.281 1.311 2.592 0,9% 2,66% ‐0,1%
17. Trentino‐Alto Adige 1.220 1.186 2.406 0,8% 2,46% +0,5%
18. Basilicata 476 430 906 0,3% 3,90% +9,7%
19. Valle d'Aosta 154 160 314 0,1% 3,79% +2,3%
20. Molise 130 121 251 0.1% 1.81% ‐ 0.8%
Cinesi in Italia: 299.823 su 5.255.503 stranieri in Italia (5,7%)0‐14 years: 17.22%
15‐24 years: 12.32%
25‐54 years: 47.84%
55‐64 years: 11.35%
65 years and over: 11.27%
0‐14 years: 13.3 %
15‐24 years: 9.7 %
25‐54 years: 40.9 %
55‐64 years: 13.3%
65 years and over: 22.5 %Age Distribution 2018:
ITALY & China
100 %
90 %
80 %
70 %
60 %
50 %
40 %
30 %
20 %
10 %
0%
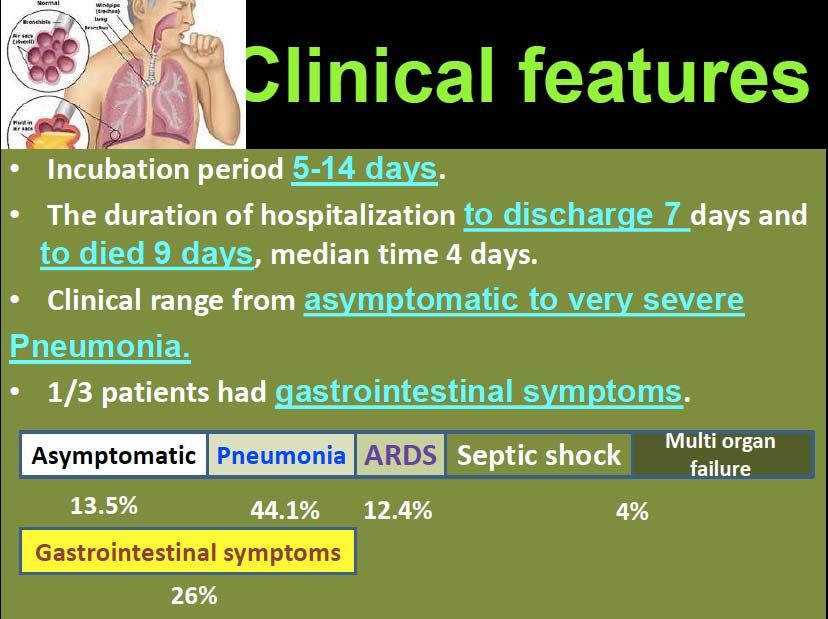
0 – 14 yrs 15 – 24 yrs 25 – 54 yrs 55 – 64 yrs > 65 yrsAspetti Clinici
Zhe Xu, et al. A 50‐year‐old man was admitted to a fever clinic on Jan 21, 2020, with symptoms of fever, chills, cough, fatigue and shortness of breath. He reported a travel history to Wuhan Jan 8– 12…….
Zhe Xu, et al.
The right lung showed evident The left lung tissue displayed pulmonary
desquamation of pneumocytes and hyaline oedema with hyaline membrane formation,
membrane formation, indicating acute suggestive of early‐phase ARDS.
respiratory distress syndrome (ARDS).
Interstitial mononuclear inflammatory
infiltrates, dominated by lymphocytes, were
seen in both lungs.Early Phases of
COVID‐19 in a
Patient who is
now waiting for
lung
transplantationMild COVID‐19 disease in a Patient who has now completely recovered
Late Phases of
COVID‐19 in a
Patient who died
inspite of
mechanical
ventilation
(intubation)Mildly symptomatic COVID‐19 disease, recovered after a week, managed than on an outpatient basis
CT Scan after 15 days: Patient fully recovered no symptoms, saturation 98%Measles in a 40‐year‐old male; He recovered after prolonged mechanical ventilation (intubation)
Development of Pneumococcal Pneumonia – Recovered (Husband of a no‐vax Wife…)Pulmonary involvement without generalised lymphoid organ
hyperplasia is typical of COVID-19 pneumonia.
Haemophagocytosis, albeit intrapulmonary, has also been
reported in coronavirus family infection.12 However, in the early
stages systemic coagulopathy is not a feature. Such
intrapulmonary haemophagocytosis, which then drains to regional
nodes, indicates removal of extravascular red blood cells
mediated by activated macrophages, secondary to vascular injury.
Some coronavirus family members gain access to
the lungs via the ACE2 receptor that is expressed
most abundantly on a subpopulation of type II
pneumocytes. Shaded boxes indicate the much
greater capability for immunothrombosis given the
alveolar tropism of SARS-CoV-2.Scheme showing how extensive COVID-19 lung involvement with large anatomical interface between infected type II pneumocytes, extensive interstitial immunocyte activation similar to macrophage activation syndrome, and the extensive pulmonary microvascular network, triggers diffuse pulmonary bed extrinsic inflammation with immunothrombosis. This inflammation causes microthrombotic immunopathology that leads to right ventricular stress and contributes to mortality. Diffuse type II pneumocyte centric pathology with extension into the interstitium leads to extensive pulmonary macrophage recruitment and activation, resulting in a clinical picture similar to local macrophage activation syndrome. Proinflammatory and procoagulants gain access to the capillary network (lower circle). The low pressure nature of the vascular system and thin vessel walls in and proximal to the alveolar network triggers immunothrombosis by various mechanisms (eg, local elevations in proinflammatory cytokines), vessel wall tissue damage with tissue factor production, and direct injury to small vessels. Vigorous fibrinolytic activity (detected early by D-dimer elevation) might not keep in check the extensive microthrombi formation, leading to the evolution of pulmonary infarction, haemorrhaging, and pulmonary hypertension induced by pulmonary intravascular coagulopathy, all of which are driven by COVID-19 inflammation. Thus, risk factors for cardiovascular disease might increase the likelihood of death in severe COVID-19 inflammation.
DIAGNOSTICA MOLECOLARE
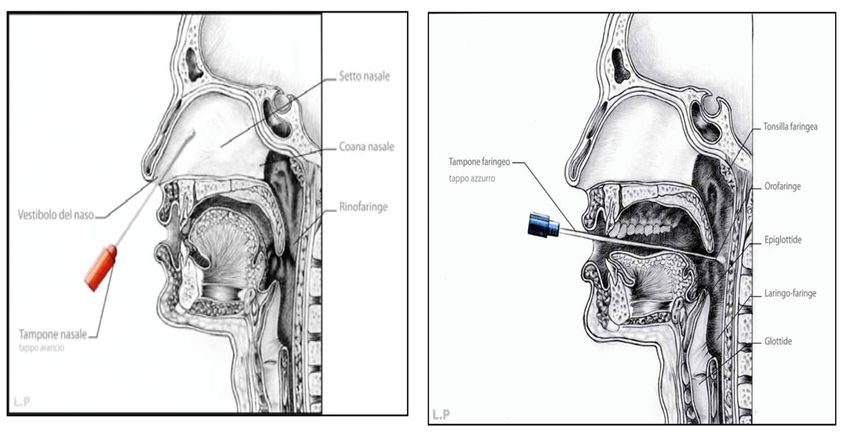
Diagnosi di laboratorio di SARS-CoV-2 MATERIALI BIOLOGICI SU E’ POSSIBILE ESEGUIRE IL TEST Alte vie respiratorie • Tampone nasale • Tampone faringeo Basse vie respiratorie • Escreato • Broncoaspirato • Lavaggio Broncoalveolare • Sierologia per ricerca anticorpi IN ALLESTIMENTO
Diagnosi di laboratorio di SARS-CoV-2
TEST MOLECOLARE COSTRUITO SULLE SEQUENZE DEL
GENOMA VIRALE DEPOSITATE SU GISAID
Screening: Real-time Reverse Transcription (RT)-Polymerase Chain
Reaction (PCR)
Conferma: sequenziamento genomico
12 gennaio 2020:
•pubblicazione del genoma dei
primi 5 pazienti
•sequenze tutte uguali sia cinesi
che non cinesi:
VIRUS GIOVANE
https://www.gisaid.org/Laboratorio di Microbiologia e Virologia – ASL Città di TORINO
C+ C+
POSITIVO C+
Valore soglia
NEGATIVO SARS‐CoV‐2
campioni
BSL 2 (circa 2 ore)Definizione di Caso adottata: Bin Lou, et al. Serology characteristics of SARS‐CoV‐2 infection since
1) Febbre e/o sintomi respiratori; the exposure and post symptoms onset
2) alterazioni radiografiche del torace; Preprint by medRxiv, March 26th, 2020
3) tampone positivo per SARS-CoV-2.
Esordio dei Sintomi * In altri report mediana = 4 giorni,
Contagio range = 2 – 7 giorni
Mediana = 5 giorni
Range (IQ) = 2 – 10 giorni*
SINTOMI / SEGNI
Positività RNA SARS‐CoV‐2 (tampone): mediana = 20 giorni, range da 8 a 37 giorni
0 5 10 15 20 25. 30 35 40 giorni
94.2 % + al 37° giorno
IgM post‐esposizione
+ 10 giorni
dall’esordio
96.7 % + al 37° giorno
IgG post‐esposizione
+12 giorni
dall’esordioLa Gestione Terapeutica
FARMACI SPERIMENTALI
Antivirali: Antiinfiammatori
Idrossiclorochina
Tocilizumab
Remdesivir
(già in sperimentazione per RSV & Ebola) Sarilumab
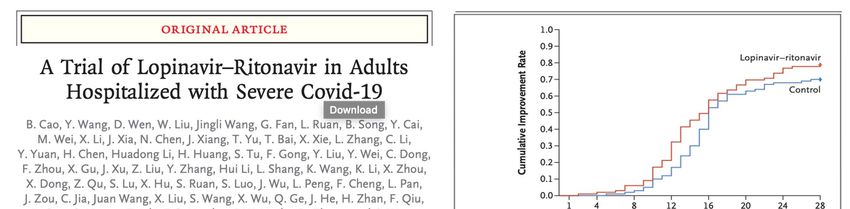
Lopinavir/Ritonavir (anti‐HIV)
Siltuximab
Darunavir/Ritonavir (anti‐HIV)
Anakinra
Umifenovir (anti‐influenzale)
Plasma da Pazienti Baricitinib
Favipiravir
guariti dal COVID‐19METHODS We conducted a randomized, controlled, open‐label trial involving hospitalized adult patients with confirmed SARS‐CoV‐2 infection, which causes the respiratory illness Covid‐19, and an oxygen saturation (Sao2 ) of 94% or less while they were breathing ambient air or a ratio of the partial pressure of oxygen (Pao2 ) to the fraction of inspired oxygen (Fio2 ) of less than 300 mm Hg. Patients were randomly assigned in a 1:1 ratio to receive either lopinavir–ritonavir (400 mg and 100 mg, respectively) twice a day for 14 days, in addition to standard care, or standard care alone. The primary end point was the time to clinical improvement, defined as the time from randomization to either an improvement of two points on a seven‐category ordinal scale or discharge from the hospital, whichever came first.
Wang Y, et al. Lancet 2020; April 29, 2020 https://doi.org/10.1016/ S0140-6736(20)31022-9 Between Feb 6, 2020, and March 12, 2020, 237 patients were enrolled and randomly assigned to a treatment group (158 to remdesivir and 79 to placebo)
Beigel JH, et al. NEJM 2020; May 28: DOI: 10.1056/NEJMoa2007764
METHODS
We conducted a double-blind, randomized, placebo-controlled trial of intravenous remdesivir in adults hospitalized
with Covid-19 with evidence of lower respiratory tract involvement. Patients were randomly assigned to receive
either remdesivir (200 mg loading dose on day 1, followed by 100 mg daily for up to 9 additional days) or placebo
for up to 10 days. The primary outcome was the time to recovery, defined by either discharge from the hospital or
hospitalization for infection- control purposes only.
538 assigned to remdesivir and 521 to placebo
CONCLUSIONS
Remdesivir was superior to placebo in
shortening the time to recovery in
adults hospitalized with Covid-19 and
evidence of lower respiratory tract
infection.
The Kaplan- Meier estimates of mortality by 14 days were 7.1% with
remdesivir and 11.9% with placebo
(hazard ratio for death, 0.70; 95% CI, 0.47 to 1.04).NEJM May 7, 2020
DOI:
10.1056/NEJMoa2012410
Among 1376 patients with Covid-19 admitted to a
New York City hospital, 59% were treated with
hydroxychloroquine. Patients selected for treatment
were more severely ill. After adjustment for patients’
baseline characteristics, there was no significant
association between hydroxychloroquine use and the
composite end point of intubation or death.Lancet 2020; May 22, 2020 https://doi.org/10.1016/
This article was published on May 1, 2020, and updated on
May 8, 2020, at NEJM.org.
Observational database from
169 hospitals in Asia, Europe,
and North America
Of the 8910 patients with Covid-19 for whom discharge status was available at the
time of the analysis, a total of 515 died in the hospital (5.8%) and 8395 survived to
discharge.Atallah B, et al. Tailored algorithm/protocol for the management of coagulopathy in COVID-19 patients. *High bleeding risk patients are excluded. Also exclude patients with platelet count 2. **FEU, fibrinogen equivalent unit. ***Adjust enoxaparin dose for renal failure.
COVID – 19: La tempesta Perfetta….. • Altamente contagioso • Contagioso per settimane • Contagioso allo stato Asintomatico (50% delle Infezioni) • Letalità attribuibile fra l’1% ed il 2% (abbastanza alta da riempire gli Ospedali, abbastanza bassa da far litigare gli Umani…)
You can also read