Streamlined method for anchoring cataract surgery and intraocular lens centration on the patient's visual axis - Zepto Cataract
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
528
TECHNIQUE
Streamlined method for anchoring
cataract surgery and intraocular lens
centration on the patient’s visual axis
Vance Thompson, MD
I describe an intraoperative method for the consistent anchoring serves as a reference marker for the visual axis and IOL place-
of the intraocular lens (IOL) and cataract surgery and on the pa- ment, with even capsule overlap, which results in IOL centration
tient’s visual axis using coaxial microscope optics, surgeon- on this axis landmark. This method might help address the high
guided patient fixation, the precision pulse capsulotomy (PPC) variability in angle k from patient to patient and provide visual
device (Zepto) and utilizing the first (and fourth) Purkinje images. benefits in cases of implantation of multifocal IOLs and other
During surgery using a microscope with coaxial lights and optics, IOLs.
the patient is instructed to fixate on a given microscope light
J Cataract Refract Surg 2018; 44:528–533 Q 2018 Published by Elsevier
while the surgeon looks through the corresponding coaxial Inc. on behalf of ASCRS and ESCRS
eyepiece. Then, the PPC device is centered on the Purkinje I im-
age and a capsulotomy is performed. The resulting capsulotomy Online Video
S
urgeons vary in their approach to capsulotomy and This paper describes an intraoperative method for the
intraocular lens (IOL) centration during cataract sur- consistent anchoring of cataract surgery and IOL centra-
gery. Some do not consider the anatomic or func- tion on the patient’s visual axis using coaxial microscope
tional axes of the eye and do not routinely practice lights and optics, brief patient fixation, and a precision
centration. Others commonly use the center of the dilated pulse capsulotomy (PPC) device (Zepto, Mynosys
pupil because if its convenience as an easily visible land- Cellular Devices, Inc.)9–11 to center on the first Purkinje
mark. In these cases, a manual continuous curvilinear cap- image as it becomes aligned with the fourth Purkinje im-
sulorhexis (CCC) is created to approximate a circular age. This technique is based on the subject-fixated coax-
capsule opening centered on the pupillary center and the ially sighted corneal light reflex as described by Chang
IOL is positioned to achieve capsule overlap as evenly as and Waring2 paired with the use of the PPC device. In
possible. Imprecision comes about as a result of the this technique, the PPC device serves a dual function.
inherent deviation from roundness and centration of a The first is to assist the surgeon in establishing coaxial
capsulotomy created by hand and the potential asymmetry sighting along the patient’s visual axis. The second is
of the dilated pupil. In addition, the pupillary axis is dis- the conversion of the patient’s individual visual axis
placed with respect to the visual axis by angle k,1,2 which into a visual axis–centered capsulotomy that is then
is highly variable in pseudophakic patients.3 This high de- used as a reference marker later in surgery. During sur-
gree of variability in angle k between patients translates gery, with the transparent PPC suction cup inserted
into a high degree of variability in chord mu,2 which into the anterior chamber, the patient is instructed to
closely approximates the distance between the location of fixate on a microscope light selected by the surgeon while
the visual axis and the pupillary center on the capsule the surgeon looks through the corresponding coaxial
plane. Chord mu variability might contribute to inconsis- eyepiece. The PPC device is then centered on the Pur-
tent or suboptimum outcomes when the pupillary center is kinje I (PI) image, which marks the patient’s visual
used for alignment, in particular in cases using aspheric, axis, and a capsulotomy is performed. The fourth Pur-
toric, and multifocal IOLs.4–8 kinje image should be aligned and mostly hidden behind
Submitted: October 18, 2017 | Final revision submitted: February 21, 2018 | Accepted: February 23, 2018
From Vance Thompson Vision, Sioux Falls, South Dakota, USA.
Supported in part by surgical devices provided by Mynosys Cellular Devices, Inc., Fremont, California, USA.
Corresponding author: Vance Thompson, MD, Vance Thompson Vision, 3101 West 57th Street, Sioux Falls, South Dakota 57108, USA. E-mail: vance.thompson@
vancethompsonvision.com.
Q 2018 Published by Elsevier Inc. on behalf of ASCRS and ESCRS. 0886-3350/$ - see frontmatter
https://doi.org/10.1016/j.jcrs.2018.02.013
TECHNIQUE: VISUAL AXIS ANCHORING 529
PI when the patient is fixating on the co-axial light and Results
can also be a very helpful guide. The resulting capsulot- Intraoperative PPC visual axis anchoring was performed in
omy preserves the visual axis information and acts as a 86 patients having routine cataract surgery with monofocal
surrogate reference marker to guide IOL centration on or multifocal IOL implantation. All patients were able to
this axis. fixate as instructed and received individualized PPC capsu-
lotomies anchored on their specific visual axis. Monofocal
SURGICAL TECHNIQUE and multifocal IOLs were then centered on the visual axis
Figure 1, A, shows the commonly used methods of creating by alignment with the round PPC capsulotomy to achieve
the CCC at a convenient location on the capsule or approx- even 360-degree capsule overlap.
imately around the center of the dilated pupil without pre- A series of photographs from a typical case in which
specified patient fixation. Figure 1, B, shows the technique anchoring to the visual axis using PPC was performed is
of using patient fixation to determine the true visual axis shown in Figure 3 and Video 1 (available at http://
followed by the creation of a PPC capsulotomy precisely jcrsjournal.org). At the beginning of surgery, with the
on this axis. The technique requires the use of a surgical mi- patient lightly sedated, the surgeon practices fixation with
croscope with lights that are coaxial to the eyepieces. First, the patient (Figure 3, A and B). The PPC device was
the surgeon selects 1 eyepiece through which the visual axis removed from its packaging and inspected (Figure 3, C).
alignment procedure will be viewed (panel 1). Next, the The device push rod was extended forward to elongate
PPC device is inserted into the eye and opened to its circular the PPC capsulotomy ring and suction cup to facilitate
shape. The patient is then instructed to fixate on the micro- insertion into the eye (Figure 3, D and E). Once in the ante-
scope light through the transparent PPC device; the light is rior chamber, the push rod was retracted and the PPC tip
coaxial to the selected eyepiece (panel 2). After fixation is regained its original circular shape (Figure 3, F). At this
accomplished, the surgeon identifies the PI image and the point, the patient was instructed to fixate on the selected
center of the PPC device is maneuvered to coincide with microscope light coaxial with the left eyepiece, which is
the position of the PI image (Figure 1, B, panel 3, and visible through the transparent PPC suction cup. As the pa-
Figure 2). The PI image under these coaxial lighting, patient tient maintained fixation, the center of the PPC device was
fixation, and surgeon viewing conditions is the subject- maneuvered by the surgeon to coincide with the PI
fixated coaxially sighted corneal light reflex described by (Figure 3, G). The capsulotomy ring itself can also be
Chang and Waring2 and is very near the patient’s visual used as a circular guide for centering the device on PI. Dur-
axis in the virgin eye. The surgeon viewing through the ing positioning, it was helpful to ensure that the push rod
selected eyepiece at PI is looking along this axis. After was left in the silicone neck with the tip of the push rod
PPC device centering on PI has been completed, a PPC cap- left just proximal to the capsulotomy ring (Figure 3, G,
sulotomy is performed. The center of the PPC capsulotomy arrow) to provide stiffness in the neck region and facilitate
corresponds exactly to that specific patient’s visual axis, and device maneuverability.
the capsulotomy edge serves as a reference marker that can Once PPC suction cup centration on PI was achieved,
be used later in surgery for IOL centration. suction was activated and the push rod then fully retracted
Figure 1. A: Schematic depicting a surgical scenario in which the approximate center of a manual CCC is created around the center of
the dilated pupil and patient fixation is not specified. B: Schematics showing the steps in creating a visual axis centered capsulotomy using
precision pulse capsulotomy (CCC Z continuous curvilinear capsulorhexis; PI Z Purkinje image I; PPC Z precision pulse capsulotomy).
Volume 44 Issue 5 May 2018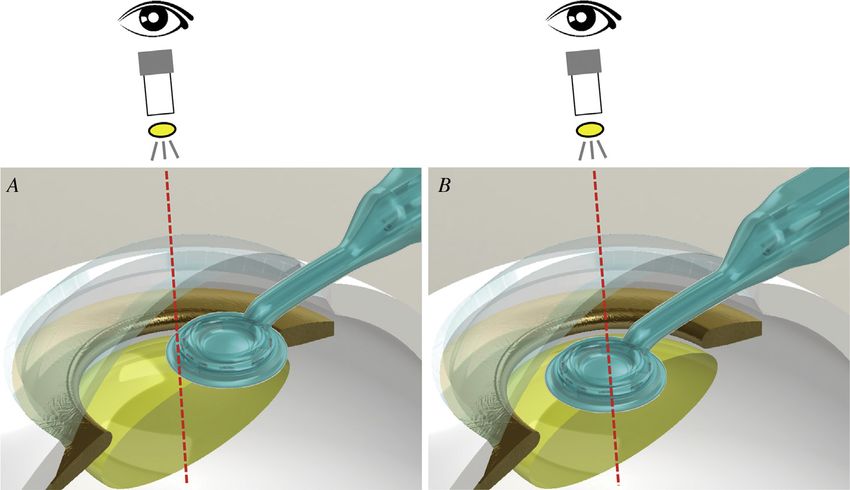
530 TECHNIQUE: VISUAL AXIS ANCHORING
Figure 2. A: With the patient look-
ing through the transparent PPC
suction cup and fixating on a spec-
ified light in a microscope with co-
axial lights and optics, the surgeon
views through the eyepiece coaxial
with that microscope light and
identifies the Purkinje I (PI) image.
B: The PPC device is maneuvered
so that the center of the PPC suc-
tion cup is coincident with the PI
image. A PPC capsulotomy is per-
formed at this location. The result-
ing PPC capsulotomy is centered
on the patient’s visual axis (PPC Z
precision pulse capsulotomy).
to its limit (Figure 3, H, arrow) to ensure adequate suction. Commercially available femtosecond laser platforms
The PPC capsulotomy was then performed (Figure 3, I). place the capsulotomy on the center of the pupil or use
The ophthalmic viscosurgical device (OVD) originally imaging to approximate and center on the capsular
removed during suction was reintroduced back into the bag.12 Capsulotomy centration on the capsular bag centers
PPC suction cup along with a small amount of a balanced on the eye’s optical axis, which is offset from the eye’s vi-
salt solution to float the PPC suction cup and capsulotomy sual axis (reviewed by Chang and Waring2). The present
ring off the capsule (Figure 3, J). The PPC device was then method of visual axis anchoring using patient fixation
removed from the eye (Figure 3, K), and hydrodissection and PPC capsulotomy cannot be performed with a femto-
and phacoemulsification performed per routine. The IOL second laser because interface docking inhibits patient fix-
was positioned using the PPC capsulotomy as a surrogate ation and likely moves the eye as docking is performed.
marker for the patient’s true visual axis (Figure 3, L). Furthermore, the use of an air or liquid interface for the
Even, 360-degree capsule overlap was used to guide IOL docking process might also complicate attempts at
positioning directly on the patient’s visual axis. fixation.
Figure 4, A, shows the IOL position at the end of the sur- The described method of visual axis anchoring requires
gery (the 2 dimmer reflections below (arrows) are from the only a surgical microscope with coaxial lights and optics
IOL surface. Figure 4, B shows the dilated pupil (blue circle) and a small disposable PPC device. It uses the built-in trans-
and the PPC capsulotomy (green circle) are displaced with parency of the PPC suction cup, and no preoperative im-
respect to one another. The linear distance between the cen- aging or heads up display of images are needed. Given
ter of the pupil and the center of the PPC capsulotomy that patient fixation is used to inform the surgeon on
centered on PI (chord mu) is directly proportional to the PPC placement, patient sedation must be adjusted to allow
patient’s angle k. Angle k has been documented to vary for patient cooperation during the process. Additional
significantly between patients. sedation can be given once the capsulotomy has been
completed. Patients who cannot follow surgeon instruc-
DISCUSSION tions for fixation, have higher grade cataracts or ocular pa-
The method described here uses surgeon-guided patient thologies limiting vision, or those requiring full anesthesia
fixation to identify the patient’s visual axis intraoperatively. are not candidates for the procedure.
The optically clear PPC device is then used to convert this The present study describes a cataract surgery centration
axis location into an individualized capsulotomy centered method using a PPC device that was recently approved by
on the patient’s visual axis, preserving this visual axis infor- the U.S. Food and Drug Administration PPC.9–11 It has
mation that is lost once cataract surgery commences. The been reported that the PPC device is easy to use for creating
PPC capsulotomy in turn acts as a visual axis reference round, consistent capsulotomies in simple and challenging
marker that is then used later in the surgery for IOL centra- cases of cataract surgery.11 Well-constructed capsulotomies
tion on that particular patient’s visual axis. The PPC de- with even capsular overlap are thought to minimize poste-
vice10,11 provides an optically clear window during patient rior capsule opacification, asymmetric anterior capsule
fixation and capsulotomy. Any obstruction limiting the pa- contraction, IOL tilt, late decentration of the optic, and
tient’s ability to fixate on the coaxial light eliminates the encourage a stable IOL position. The visual axis anchoring
opportunity to perform visual axis anchoring as described. technique described here extends the PPC’s role beyond
Volume 44 Issue 5 May 2018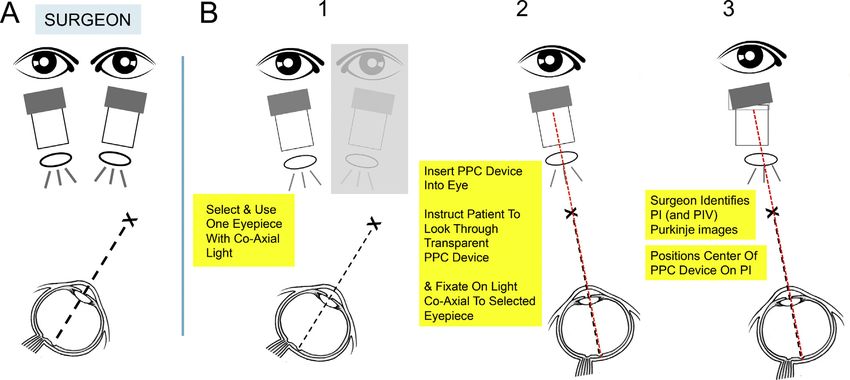
TECHNIQUE: VISUAL AXIS ANCHORING 531
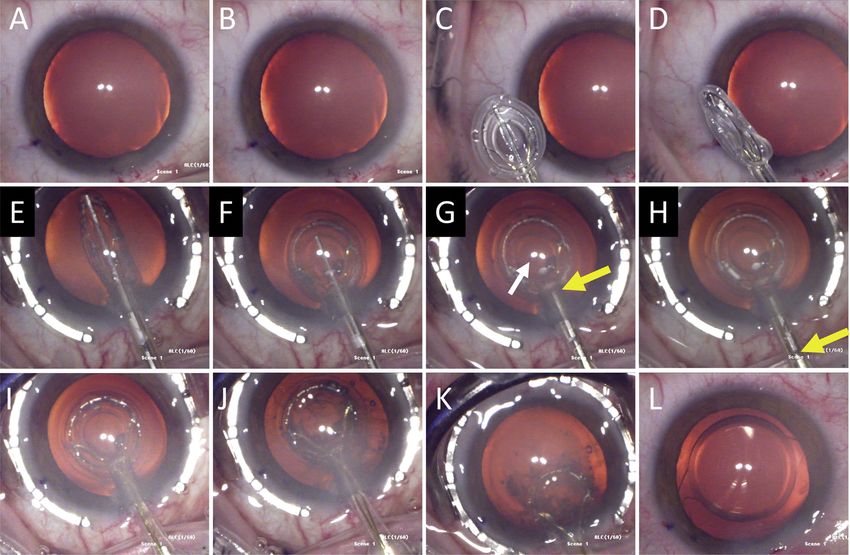
Figure 3. A typical case in which a personalized cataract surgery anchored on the patient’s visual axis is performed using the PPC device. A and
B: At the start of surgery, the patient practices fixating on the surgical light selected by the surgeon. C: The protective covering is removed from
the PPC device and the device is inspected according to manufacturer’s instructions. D: The PPC suction cup and capsulotomy ring are elon-
gated using the finger slider to extend the push rod forward. E: The PPC tip is inserted through the primary incision into the anterior chamber.
F: The push rod is retracted and the suction cup and capsulotomy ring spontaneously open to their original circular shapes. G: The tip of the
push rod (yellow arrow) is left just proximal to the capsulotomy ring. The presence of a rigid push rod in the PPC silicone neck aids in maneu-
vering the PPC suction cup in the anterior chamber and lining up its center with the Purkinje I image. In this case, the patient was instructed to
fixate on the light (white arrow) coaxial with the left eyepiece. H: After PPC positioning is achieved, suction is activated and simultaneously the
push rod is retracted all the way out of the device neck so as to not interfere with the development of suction required for consistent capsu-
lotomy. I: The PPC capsulotomy is performed centered on the patient’s visual axis. J: The OVD that was removed from the suction cup during
the suction step is reintroduced back into the suction cup along with a small amount of a balanced salt solution. K: The PPC device is removed
from the eye and the surgeon continues with hydrodissection, phacoemulsification, and irrigation/aspiration. L: An IOL (Symphony, Johnson &
Johnson Vision) positioned to achieve 360-degree even overlap with the visually centered PPC capsulotomy (IOL Z intraocular lens;
OVD Z ophthalmic viscosurgical device; PPC Z precision pulse capsulotomy).
Figure 4. A: The IOL was aligned using
the PPC as a reference marker. The
360-degree even overlap with the visually
centered PPC capsulotomy places the
IOL on the patient’s visual axis. The 2
dimmer light reflections below (white
arrows) are from the IOL surface. B: The
blue circle demarcates the pupil. The
green circle demarcates the PPC capsu-
lotomy. Note that the blue and green
circles are not concentric. The displace-
ment of their respective centers from
one another corresponds to chord mu
and is proportional to angle k in this pa-
tient (IOL Z intraocular lens; PPC Z
precision pulse capsulotomy).
Volume 44 Issue 5 May 2018
532 TECHNIQUE: VISUAL AXIS ANCHORING
being an automated capsulotomy device into a surgical tool center of the capsular bag as a result of the properties of the
that might bring additional visual benefits related to IOL haptics. An automated capsulotomy that can serve as a
centration on the visual axis. reference marker for centering IOLs on the visual axis could
Purkinje images are very helpful in centering cataract sur- encourage the development of IOLs with adjustable haptics
gery on the patient’s visual axis. (See Chang and Waring or other technologies for positioning in the horizontal
20142 for a complete discussion of the Purkinje images and plane. Edge-captured IOLs, such as the Femtis IOL (Ocu-
their relative positions as seen by the surgeon during patient lentis GmbH) available in Europe, have been used in
fixation on the co-axial light.) In addition to locating the PI conjunction with PPC capsulotomies. Because the horizon-
image during patient co-axial fixation, the fourth Purkinje tal position of these IOLs in the eye is dictated solely by the
image may be very helpful as it should be mostly hidden location of the capsulotomy, the present method of intra-
behind PI if proper patient fixation on the co-axial light is operative capsulotomy centration on the visual axis might
achieved. For certain patients with difficulty fixating on the be useful.
co-axial light as instructed, the surgeon can use a second in- The nature of any visual benefit must await formal
strument to move the eye and align the first and forth Pur- controlled studies of an appropriate number of patients.
kinje images and then center the PPC capsulotomy on PI. The intent of this paper is to introduce a method whereby
Visual axis anchoring of cataract surgery using PPC re- surgeons can routinely anchor cataract surgery and center
quires minimal equipment, provides seamless integration the IOL on the visual axis. This form of individualized
into routine cataract surgery, and is easy to learn. A recent cataract surgery in which the patient’s personal visual
study of a large number of pseudophakic patients3 found a axis is used might help optimize outcomes and benefit
high degree of variability in angle k from individual to in- patients.
dividual.3 In addition, multiple researchers have examined
the relationship between angle k and the occurrence of un-
desired photic phenomena and concluded that consider-
WHAT WAS KNOWN
ation of angle k is important for optimizing the quality of
Cataract surgery commonly involves the creation of a
vision and patient satisfaction.6–8 An easy-to-perform
manual CCC approximately centered on the dilated pupil.
methodology for true visual axis alignment intraoperatively Because pupil dilation is often asymmetric and the mainte-
that is based on fundamental principles might therefore nance of a precise central point during CCC is exceedingly
provide more consistent and better outcomes for patients. difficult, surgeons have little reference to important functional
This is likely the case for those receiving aspheric, toric, axes in the eye, including the visual axis, once surgery has
and multifocal IOLs3,4 but might also be true for the general started.
population of cataract surgery patients. Given the limita- There is substantial variability in angle k among pseudo-
phakic patients.
tions in the size of the light in current surgical microscopes
and the current lack of a visual aid for centration on the WHAT THIS PAPER ADDS
PPC device limiting the surgeon’s ability to manually place The combination of patient fixation on a light from a micro-
the center of the PPC device onto the PI image, a certain scope with coaxial lights and optics and surgeon viewing
lack of precision is inherent in this method. However, it is through the corresponding coaxial eyepiece allows the
likely to be an improvement over guessing the location of creation of a PPC capsulotomy that is centered precisely on
a patient’s visual axis, especially given its high variability the patient’s visual axis.
This individualized PPC capsulotomy can act as a reference
among patients.3 Furthermore, for surgeons who place dif-
marker for IOL implantation on the visual axis, and may
fractive optics somewhere between the center of the pupil provide benefits in implantation of toric, multifocal, or other
and the visual axis, the specific localization of the patient’s IOLs.
visual might may be helpful and the location of the capsu-
lotomy can be adjusted accordingly.
At present, many surgeons place the capsulorhexis
slightly nasally to account for angle k and correspondingly REFERENCES
manually move the optic nasally in the horizontal plane to 1. Tabernero J, Benito A, Alco n E, Artal P. Mechanism of compensation of ab-
errations in the human eye. J Opt Soc Am A Opt Image Sci Vis 2007;
achieve optimum capsulotomy overlap. This is often per- 24:3274–3283
formed using 1-piece acrylic IOLs with the haptics oriented 2. Chang DH, Waring GOIV. The subject-fixated coaxially sighted corneal light
at 6 o’clock and 12 o’clock. The surgeon nudges the optic reflex: a clinical marker for centration of refractive treatments and devices.
Am J Ophthalmol 2014; 158:863–874
nasally to move the haptic–capsular bag contact points, tak- 3. Harrer A, Hirnschall N, Tabernero J, Artal P, Draschl P, Maedel S,
ing advantage of the ability of the haptic’s geometric design Findl O. Variability in angle k and its influence on higher-order aberra-
to be accommodated at a range of locations within the tions in pseudophakic eyes. J Cataract Refract Surg 2017; 43:1015–
1019. Available at: http://www.jcrsjournal.org/article/S0886-3350(17)30
capsular bag off the vertical axis. This IOL positioning pro- 467-4/pdf. Accessed March 12, 2018
cedure can be used with the visual axis–centered PPC cap- 4. Tabernero J, Piers P, Benito A, Redondo M, Artal P. Predicting the optical
sulotomy described here. However, this ability to position performance of eyes implanted with IOLs to correct spherical aberration.
Invest Ophthalmol Vis Sci 2006; 47:4651–4658. Available at: http://iovs
the IOL in the horizontal plane is not universally accepted .arvojournals.org/article.aspx?articleidZ2124955. Accessed March 12,
because others believe the optic will always center in the 2018
Volume 44 Issue 5 May 2018TECHNIQUE: VISUAL AXIS ANCHORING 533
5. Tchah H, Nam K, Yoo A. Predictive factors for photic phenomena 11. Waltz K, Thompson VM, Quesada G. Precision pulse capsulotomy: initial
after refractive, rotationally asymmetric, multifocal intraocular lens implanta- clinical experience in simple and challenging cataract surgery cases.
tion. Int J Ophthalmol 2017; 10:241–245. Available at: https://www.ncbi J Cataract Refract Surg 2017; 43:606–614
.nlm.nih.gov/pmc/articles/PMC5313547/pdf/ijo-10-02-241.pdf. Accessed 12. Grewal DS, Schultz T, Basti S, Dick HB. Femtosecond laser–assisted cata-
March 12, 2018 ract surgerydcurrent status and future directions. Surv Ophthalmol 2016;
6. Park CY, Oh SY, Chuck RS. Measurement of angle kappa and centration in 61:103–131
refractive surgery. Curr Opin Ophthalmol 2012; 23:269–275
7. Prakash G, Prakash DR, Agarwal A, Kumar DA, Agarwal A, Jacob S. Pre- Disclosure: Dr. Thompson has received research support from
dictive factor and kappa angle analysis for visual satisfactions in patients
Mynosys Cellular Devices, Inc., in the form of 20 surgical devices
with multifocal IOL implantation. Eye 2011; 25:1187–1193. Available at:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3178249/pdf/eye201115
0a.pdf. Accessed March 12, 2018
8. Moshirfar M, Hoggan RN, Muthappan V. Angle kappa and its importance
in refractive surgery Oman. J Ophthalmol 2013; 6:151–158. Available at:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3872563/?reportZprint First author:
able. Accessed March 12, 2018 Vance Thompson, MD
9. Thompson VM, Berdahl JP, Solano JM, Chang DF. Comparison of manual,
femtosecond laser, and precision plus capsulotomy edge tear strength in Vance Thompson Vision, Sioux Falls,
paired human cadaver eyes. Ophthalmology 2016; 123:265–274 South Dakota, USA
10. Chang DF, Mamalis N, Werner L. Precision pulse capsulotomy; preclinical
safety and performance of a new capsulotomy device. Ophthalmology
2016; 123:255–264
Volume 44 Issue 5 May 2018You can also read

















































