Insulin resistance: a global epidemic in need of effective therapies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Heart Journal Supplements (2003) 5 (Supplement C), C13—C18
Insulin resistance: a global epidemic in need of
effective therapies
R.M. Califf
Duke Clinical Research Institute, Durham, North Carolina, U.S.A.
There is a worldwide rapid increase in the prevalence of type 2 diabetes, due to
KEYWORDS
Cardiovascular risk; factors such as improved affluence, longevity, and obesity. To prevent the
impaired glucose development of diabetes, individuals must be identified at an early stage of risk and
tolerance; targeted with preventive measures such as lifestyle advice and pharmacological
metabolic syndrome; therapy. A key indicator of risk is impaired glucose tolerance. We have recently begun
nateglinide; the Nateglinide And Valsartan in Impaired Glucose Tolerance Outcomes Research
valsartan (NAVIGATOR) trial to gather epidemiological data and provide insight into the
Downloaded from by guest on May 7, 2015
protective effects of the angiotensin receptor blocker valsartan in patients with
improved glucose intolerance.
© 2003 The European Society of Cardiology. Published by Elsevier Science Ltd. All
rights reserved
Introduction Improved longevity, affluence and
obesity
The worldwide prevalence of diabetes, primarily
type 2 diabetes, has exploded in recent years. This As access to technology spreads across the world,
epidemic is growing most rapidly in the developing people are living longer and are more functional.
world, where type 2 diabetes and its ‘partner in Life expectancy, as estimated by the Global
crime’ — obesity — are increasing in prevalence at Burden of Disease Study, will be almost 90 years
unprecedented rates.1 There is reason to be for women and over 80 years for men in the
concerned that the substantial gains that have been foreseeable future.2 At the same time, the
made in reducing the incidence of coronary disease improvement in functionality in this older popu-
mortality and morbidity will be lost as a result of lation is improving more rapidly than longevity.3
this global epidemic. Because the epidemic appears However, along with this dramatic improvement in
to be the unintended consequence of good global the public health has come access to greater
outcomes, and concomitant spread of longevity and amounts of food and the ability to use technology
affluence, approaches to treating the problem will to reduce the amount of exercise.
inevitably require greater understanding of the
implications of lifestyle and its alteration. In
addition, these complexities open the door to Impaired glucose tolerance
consideration of the use of complex pharmacology
in the context of a long-term chronic disease. We are increasingly aware that overt type 2
diabetes occurs only after years of metabolic
alterations that are measurable but not
symptomatic. Information on this metabolic
Correspondence: Robert M. Califf, Duke Clinical Research substrate for diabetes can be gained by giving a
Institute, Box 3850, Durham, NC 27710, U.S.A. glucose load to people without outright diabetes.
01520-765X/03/0C00013 + 06 $35.00/0 © 2003 The European Society of Cardiology, Published by Elsevier Science Ltd. All rights reserved.C14 R.M. Califf
The diagnostic criteria of the American Diabetes
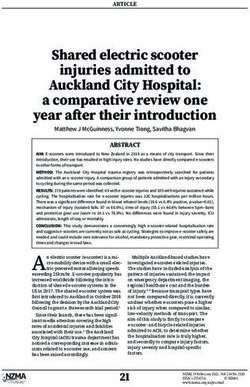
Association4 define diabetes as fasting plasma 2000: 26·5
2010: 32·9
2000: 14·2 2000: 84·5
glucose of 126 mg dl —1 or greater, or plasma 2010: 17·5 2010: 132·3
glucose levels of 200 mg dl —1 or greater 2 h after
oral intake of 75 g glucose. Impaired glucose
2000: 9·4
tolerance (IGT) is defined as 2-h plasma glucose 2010: 14·1
levels between 140 and 200 mg dl —1, and impaired 2000: 15·6
2010: 22·5
fasting glucose is defined as fasting plasma glucose 2000: 1·0
2010: 1·3
levels of 110—126 mg dl —1. As shown in Fig. 1, it is
possible to identify patients who fit into these Global increase: 46%
categories, and this categorisation provides insight 2000: 151 million
2010: 221 million
into the potential to prevent the overt future
complications of diabetes. Fig. 1 Estimated numbers of patients with diabetes in millions
Indeed, IGT is strongly predictive of future in the years 2000 (top values) and 2010 (bottom values). Data
type 2 diabetes;5 approximately two-fifths of from Zimmet et al.8
diagnosed individuals develop diabetes over 5—
10 years. Accordingly, it is sensible for measures which is the largest clinical research study of
directed at preventing the development of type 2 type 2 diabetes ever conducted.14—17 In that trial,
diabetes to focus on people with IGT.6,7 and in other studies such as the Hypertension
People with insulin resistance are often Optimal Treatment (HOT) trial,18 there was a clear
hypertensive, and particularly in follow-up those correlation between the degree of blood pressure
with normal blood pressure at baseline are likely reduction and cardiovascular risk reduction. In the
to develop hypertension. Whether this concor- UKPDS study, tight blood pressure control (target
dance, in addition to the other components of the 144/82 mmHg) reduced the risk for diabetes-
Downloaded from by guest on May 7, 2015
metabolic syndrome, is due to the ‘cross-talk’ related end-points by 24% as compared with less
between the two problems, or whether it is due to tight control (target 154/87 mmHg).17 Tight blood
a common genetic predisposition remains pressure control also reduced strokes by 44%
speculative. By attempting to treat both under- (P=0.013) and microvascular end-points by 37%
lying problems, insight will be gained into the (P=0.0092). In the diabetic subgroup in HOT, lower-
aetiological issues that are common to both. ing diastolic blood pressure from 90 to 80 mmHg
Diabetes has long been known to be a strong reduced the incidence of major cardiovascular
predictor of atherosclerosis, which is the main events (stroke and heart attack) by 50%.18
cause of morbidity and mortality in these Hypertension is also a risk factor for the
patients.8 However, we have become aware in development of type 2 diabetes, and IGT appears
recent years that the increase in cardiovascular to be more common in hypertensive patients than
risk is present with the state of IGT, long before in normotensive people.19 Some types of
the manifestation of type 2 diabetes. Although it antihypertensive therapy have been shown to
does not represent fully blown diabetes, IGT is reduce the development of new-onset diabetes in
associated with increased risk for macrovascular groups at risk for the disease. Intriguingly, recent
disease. In particular, the combination of IGT with clinical trials have suggested specific benefits
known cardiovascular risk factors such as from treatments that interfere with the renin—
hypertension, dyslipidaemia, visceral obesity or angiotensin system (RAS) in delaying the onset of
hypercoagulability — a condition known as the diabetes. The Losartan Intervention for Endpoint
‘metabolic syndrome’5 — greatly increases the Reduction (LIFE) study20 showed that blood
prognostic implications of the condition.9,10 pressure control with the angiotensin receptor
blocker (ARB) losartan reduced the risk for
developing type 2 diabetes by 25% (relative risk
Hypertension 0.75, 95% confidence interval 0.63—0.88; P=0.001)
as compared with the beta-blocker atenolol in
Hypertension is an important component in the hypertensive patients with left ventricular
metabolic syndrome and it is more prevalent in hypertrophy. The Study on COgnition and Prognosis
type 2 diabetes patients than in the general in Elderly hypertensives (SCOPE)21 indicated
population.11—13 The benefits of controlling similar benefits (20% reduction in risk) with the
hypertension in diabetes have been shown in a ARB candesartan as compared with other therapies
number of landmark trials, most prominently in (mainly hydrochlorothiazide), although that study
the U.K. Prospective Diabetes Study (UKPDS), suffered from several weaknesses because of aInsulin resistance C15
change in treatment regimen during the course of • Randomized, placebo-controlled trial, 2×2 factorial design
the trial. Reports from the Heart Outcomes
Prevention Evaluation (HOPE) study22 with the nateglinide/valsartan placebo/valsartan
n = 1875 n = 1875
angiotensin-converting enzyme (ACE) inhibitor
ramipril claim that the relative risk for developing nateglinide/placebo placebo/placebo
n = 1875 n = 1875
diabetes was 0.66 (95% confidence interval 0.51—
0.85; PC16 R.M. Califf
Table 1 Comparison between DREAM and NAVIGATOR
DREAM NAVIGATOR
Numbers randomized (planned) 4000 7400—11,000
Patient characteristics Age >30 years; IGT [2-h plasma glucose post Age >50 years (two-thirds >55 years);
75 g glucose challenge of 7.8—11.0 mmol l—1 IGT [2-h plasma glucose post 75 g glucose
(140—199 mg dl—1) inclusive]; no uncontrolled challenge of 7.8—11.0 mmol l—1
hypertension; no history of diabetes (140—199 mg dl—1) and fasting plasma
glucose ≥5.2 mmol l—1 (≥95 mg . dl—1) butInsulin resistance C17
ramipril and rosiglitazone).37 That trial has 10. Perry RC, Baron AD. Impaired glucose tolerance. Why is it
similarities to NAVIGATOR, because it will study not a disease? Diabetes Care 1999;22:883—5.
11. Hypertension in Diabetes Study Group. Hypertension in
whether treatment of IGT can prevent the
Diabetes Study (HDS): I. Prevalence of hypertension in
development of type 2 diabetes. In DREAM, 4000 newly presenting type 2 diabetic patients and the associa-
individuals with IGT will be given ramipril or the tion with risk factors for cardiovascular and diabetic com-
oral antidiabetic rosiglitazone, or both. The plications. J Hypertens 1993;11:309—17.
treatments have different modes of actions to 12. Harris M, Cowie C, Stern M et al. Diabetes in America.
Washington, DC, National Institutes of Health, National
those included in NAVIGATOR: rosiglitazone
Institute of Diabetes and Digestive and Kidney Diseases,
increases insulin sensitivity whereas nateglinide 1995.
increases insulin secretion; and ramipril is an ACE 13. Prescott-Clarke P, Primatesta P. Health survey for England
inhibitor whereas valsartan specifically blocks the 1995. London, HMSO, 1997.
angiotensin subtype 1 receptor. Table 1 compares 14. Adler AI, Stratton IM, Neil HA et al. Association of systolic
blood pressure with macrovascular and microvascular com-
the key qualities of NAVIGATOR and DREAM.
plications of type 2 diabetes (UKPDS 36): prospective
Whereas both trials will study prevention of type 2 observational study. BMJ 2000;321:412—9.
diabetes, only NAVIGATOR is designed to study the 15. Stratton IM, Adler AI, Neil HA et al. Association of gly-
highly relevant question of whether treatment will caemia with macrovascular and microvascular complica-
also protect against cardiovascular outcomes. tions of type 2 diabetes (UKPDS 35): prospective
observational study. BMJ 2000;321:405—12.
Particularly following LIFE and SCOPE, there is
16. UK Prospective Diabetes Study Group. Efficacy of atenolol
an urgent need to determine the role of ARBs in and captopril in reducing risk of macrovascular and microvas-
diabetes prevention and in risk reduction in cular complications in type 2 diabetes: UKPDS 39. UK
individuals with IGT. NAVIGATOR is currently the Prospective Diabetes Study Group. BMJ 1998;317:713—20.
only such trial ongoing. We know from Val-HeFT 17. UK Prospective Diabetes Study Group. Tight blood pressure
control and risk of macrovascular and microvascular com-
and other studies that valsartan is not only an
plications in type 2 diabetes: UKPDS 38. UK Prospective
antihypertensive drug but also a cardiovascular
Downloaded from by guest on May 7, 2015
Diabetes Study Group. BMJ 1998;317:703—13.
drug. It will be intriguing to see whether 18. Hansson L, Zanchetti A, Carruthers SG et al. Effects of
nateglinide is demonstrated to be not only a intensive blood-pressure lowering and low-dose aspirin in
glucose-sensitizing drug but also a drug that patients with hypertension: principal results of the
Hypertension Optimal Treatment (HOT) randomised trial.
prevents vascular events.
HOT Study Group. Lancet 1998;351:1755—62.
19. Johnson KC, Graney MJ, Applegate WB et al. Prevalence of
undiagnosed non-insulin-dependent diabetes mellitus and
impaired glucose tolerance in a cohort of older persons
References with hypertension. J Am Geriatr Soc 1997;45:695—700.
1. Zimmet P. Globalization, coca-colonization and the chronic 20. Dahlöf B, Devereux R, Kjeldsen S et al. Cardiovascular mor-
disease epidemic: can the Doomsday scenario be averted? bidity and mortality in the Losartan Intervention For
J Intern Med 2000;247:301—10. Endpoint reduction in hypertension study (LIFE): a ran-
2. Mathers CD, Sadana R, Salomon JA, Murray CJ, Lopez AD. domised trial against atenolol. Lancet 2002;359:995—1003.
Healthy life expectancy in 191 countries, 1999. Lancet 21. Hansson L, Lithell H. The study on cognition and prognosis
2001;357:1685—91. in elderly hypertensives (SCOPE). Data presented at the
3. Manton KG, Land KC. Active life expectancy estimates for 19th Scientific Meeting of the International Society of
the U.S. elderly population: a multidimensional continu- Hypertension and 12th European Meeting on Hypertension —
ous-mixture model of functional change applied to com- European Society of Hypertension. Prague, Czech Republic,
pleted cohorts, 1982—1996. Demography 2000;37:253—65. June 23—27, 2002.
4. The Expert Committee on the Diagnosis and Classification 22. Yusuf S, Gerstein H, Hoogwerf B et al. Ramipril and the
of Diabetes Mellitus. Report of the Expert Committee on development of diabetes. JAMA 2001;286:1882—5.
the Diagnosis and Classification of Diabetes Mellitus. 23. Svensson P, de Faire U, Sleight P, Yusuf S, Ostergren J.
Diabetes Care 1997;20:1183—97. Comparative effects of ramipril on ambulatory and office
5. World Health Organization. Diabetes mellitus: report of a blood pressures: a HOPE Substudy. Hypertension 2001;38:
WHO study group. Geneva, World Health Organization, E28—32.
1985. 24. Paolisso G, Tagliamonte MR, Gambardella A et al. Losartan
6. Pan XR, Li GW, Hu YH et al. Effects of diet and exercise in mediated improvement in insulin action is mainly due to an
preventing NIDDM in people with impaired glucose toler- increase in non-oxidative glucose metabolism and blood
ance. The Da Qing IGT and Diabetes Study. Diabetes Care flow in insulin-resistant hypertensive patients. J Hum
1997;20:537—44. Hypertens 1997;11:307—12.
7. Tuomilehto J, Lindstrom J, Eriksson JG et al. Prevention of 25. Top C, Cingozbay BY, Terekeci H et al. The effects of val-
type 2 diabetes mellitus by changes in lifestyle among sub- sartan on insulin sensitivity in patients with primary hyper-
jects with impaired glucose tolerance. N Engl J Med 2001; tension. J Int Med Res 2002;30:15—20.
344:1343—50. 26. Haffner S, Holman R, Califf R et al. Targeting post-prandial
8. Zimmet P, Alberti KG, Shaw J. Global and societal implica- hyperglycemia to prevent type 2 diabetes: rationale and
tions of the diabetes epidemic. Nature 2001;414:782—78. design of the NAVIGATOR trial. Presented at the 38th annu-
9. Alberti KG. Impaired glucose tolerance: what are the clinical al of the European Association for the Study of Diabetes.
implications? Diabetes Res Clin Pract 1998;40(suppl):S3—8. Budapest, Hungary, September 3, 2002.C18 R.M. Califf
27. Sato Y, Nishikawa M, Shinkai H, Sukegawa E. Possibility of 32. Markham A, Goa KL. Valsartan. A review of its pharmacolo-
ideal blood glucose control by a new oral hypoglycemic gy and therapeutic use in essential hypertension. Drugs
agent, N-[(trans-4-isopropylcyclohexyl)-carbonyl]-D-pheny- 1997;54:299—311.
lalanine (A-4166), and its stimulatory effect on insulin 33. Burnier M, Brunner HR. Angiotensin II receptor antagonists
secretion in animals. Diabetes Res Clin Pract 1991;12:53—9. in hypertension. Kidney Int 1998;68(suppl):107—10.
28. Hanefeld M, Bouter KP, Dickinson S, Guitard C. Rapid and 34. Hedner T, Oparil S, Rasmussen K et al. A comparison of the
short-acting mealtime insulin secretion with nateglinide angiotensin II antagonists valsartan and losartan in the
controls both prandial and mean glycemia. Diabetes Care treatment of essential hypertension. Am J Hypertens 1999;
2000;23:202—7. 12:414—7.
29. Cohn JN, Tognoni G, the Valsartan Heart Failure Trial 35. Wadden TA. Treatment of obesity by moderate and severe
Investigators. A randomized trial of the angiotensin-recep- caloric restriction. Results of clinical research trials. Ann
tor blocker valsartan in chronic heart failure. N Engl J Med Intern Med 1993;119:688—93.
2001;345:1667—75. 36. Wing RR, Venditti E, Jakicic JM, Polley BA, Lang W. Lifestyle
30. Viberti G, Wheeldon NM, for the MARVAL study investiga- intervention in overweight individuals with a family history
tors. Microalbuminuria reduction with valsartan in patients of diabetes. Diabetes Care 1998;21:350—9.
with type 2 diabetes mellitus: a blood pressure independ- 37. Gerstein HC. Reduction of cardiovascular events and
ent effect. Circulation 2002;106:672—8. microvascular complications in diabetes with ACE inhibitor
31. Horton ES, Clinkingbeard C, Gatlin M et al. Nateglinide treatment: HOPE and MICRO-HOPE. Diabetes Metab Res
alone and in combination with metformin improves Rev 2002;18(suppl 3):S82—5.
glycemic control by reducing mealtime glucose levels in
type 2 diabetes. Diabetes Care 2000;23:1660—5.
Downloaded from by guest on May 7, 2015You can also read