COVID-19 Monoclonal Antibody Therapy - Policy Number: PG0493 Last Review: 07/26/2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19 Monoclonal Antibody Therapy
Policy Number: PG0493 ADVANTAGE | ELITE | HMO
Last Review: 07/26/2021 INDIVIDUAL MARKETPLACE |
PROMEDICA MEDICARE
PLAN | PPO
GUIDELINES
This policy does not certify benefits or authorization of benefits, which is designated by each individual
policyholder terms, conditions, exclusions and limitations contract. It does not constitute a contract or
guarantee regarding coverage or reimbursement/payment. Paramount applies coding edits to all medical
claims through coding logic software to evaluate the accuracy and adherence to accepted national
standards. This medical policy is solely for guiding medical necessity and explaining correct procedure
reporting used to assist in making coverage decisions and administering benefits.
SCOPE
X Professional
_ Facility
DESCRIPTION
Antibodies are proteins that people's bodies make to fight viruses, such as the virus that causes COVID-19.
Monoclonal antibodies are mass-produced in a laboratory and are designed to recognize a specific component of a
virus — the spike protein on its outer shell. Antibodies made in a laboratory act a lot like natural antibodies to limit
the amount of virus in your body.
The Secretary of HHS on March 27, 2020, declared that circumstances exist justifying the authorization of
emergency use of drugs and biological products during the COVID-19 pandemic, pursuant to Section 564 of the
Federal Food, Drug, and Cosmetic Act (the Act) (21 U.S.C. 360bbb-3), subject to terms of any authorization issued
under that section. The FDA indicated that the EUA authorization of these monoclonal antibody therapies may
assist in avoiding hospital admissions and the COVID-19 burden on the present health care system.
POLICY
HMO, PPO, Individual Marketplace, Elite/ProMedica Medicare Plan, Advantage
Paramount will follow CMS and CDC guidance and cover the administration of the COVID Monoclonal
Antibody Therapy when furnished consistent with the EUA, procedures M0243, M0244, M0245, M0247,
M0248, M0249, M0250, Q0243, Q0244, Q0245, Q0247 and Q0249.
o Note: effective 04/17/2021 coverage for procedures M0239 and Q0239 has been end-dated.
o Note: Intravenous infusion, sotrovimab, includes infusion and post administration monitoring (FDA
approved 5/26/2021) The government won’t provide this drug for free; visit the COVID-19
Vaccines and Monoclonal Antibodies webpage for pricing information (available soon)
Elite/ProMedica Medicare Plan
During the COVID-19 public health emergency (PHE), Medicare will cover and pay for approved COVID-
19 Monoclonal Antibody Therapy (when furnished consistent with their respective EUAs) the same way it
covers and pays for COVID-19 vaccines. All cost share will be covered through 12/31/2021 but must be
billed to original Medicare fee-for-service.
o Note: Medicare will only cover and pay for bamlanivimab (administered alone) if it was furnished,
consistent with the terms of the EUA, between November 10, 2020 - April 16, 2021.
HMO, PPO, Individual Marketplace
All cost share for approved COVID-19 Monoclonal Antibody Therapy (when furnished consistent with
their respective EUAs) will be waived through the duration of the PHE.
PG0493 – 07/26/2021o Note: Paramount will only cover and pay for bamlanivimab (administered alone) if it was
furnished, consistent with the terms of the EUA, between November 10, 2020 - April 16, 2021.
Advantage
All cost share for approved COVID-19 Monoclonal Antibody Therapy (when furnished consistent with
their respective EUAs) will be waived per the Ohio Department of Medicaid
o Note: Paramount will only cover and pay for bamlanivimab (administered alone) if it was
furnished, consistent with the terms of the EUA, between November 10, 2020 - April 16, 2021.
Note: Paramount will not provide payment for the COVID-19 monoclonal antibody products that
health care providers receive free, as is the case upon the product’s initial availability in
response to the COVID-19 PHE.
COVERAGE CRITERIA
HMO, PPO, Individual Marketplace, Elite/ProMedica Medicare Plan, Advantage
The following FDA Emergency Use Authorization (EUA) Monoclonal Antibody Therapy is considered medically
necessary for the treatment, prevention or management of COVID-19 and related symptoms.
The use of approved FDA Emergency Use Authorization (EUA) Monoclonal Antibody Therapies must be in
accordance with the dosing regimens as detailed in the authorized Fact Sheets.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore
throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have
shortness of breath, dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who show evidence of lower respiratory disease during clinical assessment or
imaging and who have saturation of oxygen (SpO2) > 94% on room air at sea level.
Bamlanivimab and Etesevimab
The administration of bamlanivimab and etesevimab combination is covered when administered for the treatment
of COVID-19 when the specific criteria are met:
Member is 12 years of age or older and weighs at least 40kg
Member is diagnosed with mild to moderate COVID-19
Member has a positive result of direct SARS-CoV-2 viral testing (for example, molecular [PCR], or antigen
[ELISA] laboratory methods)
Member is at high risk for progressing to severe COVID-19 and/or hospitalization, not all-inclusive;
o Obesity or being overweight (for example, adults with BMI >25 kg/m2, or if 12 to 17 years of age,
have BMI ≥85th percentile for their age and gender based on CDC growth charts,
https://www.cdc.gov/growthcharts/clinical_charts.htm),or
o have chronic kidney disease, or
o have diabetes, or
o have immunosuppressive disease, or
o are currently receiving immunosuppressive treatment, or
o sickle cell disease, or
o neurodevelopmental disorders (for example, cerebral palsy) or other conditions that confer medical
complexity (for example, genetic or metabolic syndromes and severe congenital anomalies), or
o pregnancy, or
o are > 65 years of age, or
o are > 55 years of age AND have
cardiovascular disease (including congenital heart disease), or
hypertension, or
PG0493 – 07/26/2021 chronic lung diseases (for example, chronic obstructive pulmonary disease, asthma
[moderate-to-severe], interstitial lung disease, cystic fibrosis and pulmonary hypertension)
Etesevimab may only be administered together with bamlanivimab
Bamlanivimab and etesevimab may only be administered together in settings in which health care providers
have immediate access to medications to treat a severe infusion reaction, such as anaphylaxis, and the
ability to activate the emergency medical system (EMS), as necessary.
The use of bamlanivimab and etesevimab covered by this authorization must be in accordance with the
dosing regimens as detailed in the authorized Fact Sheets.
Bamlanivimab and Etesevimab are NOT authorized by this EUA for use in the following populations:
o adults or pediatric patients who are hospitalized due to COVID-19
o adults or pediatric patients who require oxygen therapy due to COVID19
Casirivimab and Imdevimab
The administration of Casirivimab and Imdevimab combination is covered when administered for the treatment of
COVID-19 when the specific criteria are met:
Member is 12 years of age or older and weighs at least 40kg
Member is diagnosed with mild to moderate COVID-19
Member has a positive result of direct SARS-CoV-2 viral testing (for example, molecular [PCR], or antigen
[ELISA] laboratory methods)
Member is at high risk for progressing to severe COVID-19 and/or hospitalization, not all-inclusive;
o Obesity or being overweight (for example, adults with BMI >25 kg/m2, or if 12 to 17 years of age,
have BMI ≥85th percentile for their age and gender based on CDC growth charts,
https://www.cdc.gov/growthcharts/clinical_charts.htm),or
o have chronic kidney disease, or
o have diabetes, or
o have immunosuppressive disease, or
o are currently receiving immunosuppressive treatment, or
o sickle cell disease, or
o neurodevelopmental disorders (for example, cerebral palsy) or other conditions that confer medical
complexity (for example, genetic or metabolic syndromes and severe congenital anomalies), or
o pregnancy, or
o are > 65 years of age, or
o are > 55 years of age AND have
cardiovascular disease (including congenital heart disease), or
hypertension, or
chronic lung diseases (for example, chronic obstructive pulmonary disease, asthma
[moderate-to-severe], interstitial lung disease, cystic fibrosis and pulmonary hypertension)
Casirivimab and imdevimab may only be administered together
Casirivimab and imdevimab may only be administered in settings in which health care providers have
immediate access to medications to treat a severe infusion reaction, such as anaphylaxis, and the ability to
activate the emergency medical system (EMS), as necessary
The use of casirivimab and imdevimab covered by this authorization must be in accordance with the dosing
regimens as detailed in the authorized Fact Sheets
Casirivimab and imdevimab is NOT authorized for use in the following patient populations:
o Adults or pediatric patients who are hospitalized due to COVID-19
o Adults or pediatric patients who require oxygen therapy due to COVID-19
o Adults or pediatric patients who require an increase in baseline oxygen flow rate due to COVID-19 in
those patients on chronic oxygen therapy due to underlying non-COVID-19-related comorbidity
PG0493 – 07/26/2021Sotrovimab
The administration of Sotrovimab is covered when administered for the treatment of COVID-19 when ALL of the
following criteria are met:
Member is 12 years of age or older and weighs at least 40kg
Member is diagnosed with mild to moderate COVID-19
Member has a positive result of direct SARS-CoV-2 viral testing (for example, molecular [PCR], or antigen
[ELISA] laboratory methods)
Member is at high risk for progressing to severe COVID-19 and/or hospitalization, not all-inclusive;
o Obesity or being overweight (for example, adults with BMI >25 kg/m2, or if 12 to 17 years of age,
have BMI ≥85th percentile for their age and gender based on CDC growth charts,
https://www.cdc.gov/growthcharts/clinical_charts.htm),or
o have chronic kidney disease, or
o have diabetes, or
o have immunosuppressive disease, or
o are currently receiving immunosuppressive treatment, or
o sickle cell disease, or
o neurodevelopmental disorders (for example, cerebral palsy) or other conditions that confer medical
complexity (for example, genetic or metabolic syndromes and severe congenital anomalies), or
o pregnancy, or
o are > 65 years of age, or
o are > 55 years of age AND have
cardiovascular disease (including congenital heart disease), or
hypertension, or
chronic lung diseases (for example, chronic obstructive pulmonary disease, asthma
[moderate-to-severe], interstitial lung disease, cystic fibrosis and pulmonary hypertension)
Sotrovimab may only be administered in settings in which health care providers have immediate access to
medications to treat a severe infusion reaction, such as anaphylaxis, and the ability to activate the
emergency medical system (EMS), as necessary.
Sotrovimab is NOT authorized for use in the following patient populations:
o Adults or pediatric patients who are hospitalized due to COVID-19
o Adults or pediatric patients who require oxygen therapy due to COVID-19
o Adults or pediatric patients who require an increase in baseline oxygen flow rate due to COVID-19 in
those patients on chronic oxygen therapy due to underlying non-COVID-19-related comorbidity
Tocilizumab (Actemra)
The U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the drug Actemra
(tocilizumab) for the treatment of hospitalized adults and pediatric patients (2 years of age and older) who are
receiving systemic corticosteroids and require supplemental oxygen, non-invasive or invasive mechanical
ventilation, or extracorporeal membrane oxygenation (ECMO). Actemra is not authorized for use in outpatients with
COVID-19.
Tocilizumab is a monoclonal antibody that reduces inflammation by blocking the interleukin-6 receptor. In the case
of COVID-19 infection, the immune system can become hyperactive, which may result in worsening of disease.
The use of Actemra (tocilizumab) covered by this authorization must be in accordance with the dosing
regimens as detailed in the authorized Fact Sheets
Regulatory Status
The U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) on November 9,
2020 to permit the emergency use of the unapproved product bamlanivimab for the treatment of mild to moderate
coronavirus disease 2019 (COVID-19) in adults and pediatric patients with positive results of direct SARS-CoV-2
viral testing who are 12 years of age and older weighing at least 40 kg, and who are at high risk for progressing to
PG0493 – 07/26/2021severe COVID-19 and/or hospitalization. This EUA does not constitute FDA approval of bamlanivimab and the NIH
has declined to endorse the use of bamlanivimab.
The U.S. FDA issued an EUA on November 21, 2020 to permit the emergency use of the unapproved products
casirivimab and imdevimab for the treatment of mild to moderate COVID-19 in adults and pediatric patients with
positive results of direct SARS-CoV-2 viral testing who are 12 years of age and older weighing at least 40kg and
who are at high risk for progressing to severe COVID-19 and/or hospitalization. This EUA does not constitute FDA
approval of casirivimab and imdevimab and the NIH has declined to endorse the use of casirivimab and
imdevimab.
The U.S. FDA issued an EUA on February 9, 2021 to permit the emergency use of the unapproved products
bamlanivimab and etesevimab administered together only by healthcare providers to treat mild to moderate
COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results
of direct SARS-CoV-2 viral testing, and who are at high risk for progressing to severe COVID-19 and/or
hospitalization. This EUA does not constitute FDA approval of bamlanivimab and etesevimab and the NIH has
declined to endorse the use of bamlanivimab and etesevimab.
On April 16, 2021, the FDA revoked the EUA for bamlanivimab, when administered alone, due to a sustained
increase in COVID-19 viral variants in the U.S. that are resistant to the solo product.
COVID-19 Update: FDA Revoked the EUA for Bamlanivimab When Administered Alone
On April 16, the FDA revoked the Emergency Use Authorization (EUA) for bamlanivimab, when
administered alone, due to a sustained increase in COVID-19 viral variants in the U.S. that are resistant to
this antibody therapy. The FDA determined that the known and potential benefits of bamlanivimab, when
administered alone, no longer outweigh the known and potential risks.
Medicare will cover and pay for bamlanivimab, when administered alone, for dates of service from
November 10, 2020 – April 16, 2021.
The FDA indicates that alternative monoclonal antibody therapies remain appropriate to treat COVID-19
patients, and health care providers may continue using these authorized therapies when administered
together:
Casirivimab & Imdevimab
Bamlanivimab & Etesevimab
Importantly, although the FDA revoked the EUA for bamlanivimab, when administered alone; alternative
monoclonal antibody therapies remain available under EUA, including REGEN-COV (casirivimab and imdevimab,
administered together), and bamlanivimab and etesevimab, administered together, for the same uses as previously
authorized for bamlanivimab alone. The FDA indicates that alternative monoclonal antibody therapies remain
appropriate to treat COVID-19 patients, and health care providers may continue using these authorized therapies:
Casirivimab and imdevimab, administered together
Bamlanivimab and etesevimab, administered together
The FDA indicates using these other therapies may reduce the risk of treatment failure for patients infected with a
COVID-19 viral variant that’s resistant to bamlanivimab when administered alone. For details about specific
variants and resistance, review the Antiviral Resistance information in Section 15 of each of the Fact Sheets listed
above.
On May 26, the FDA released an Emergency Use Authorization (EUA) for sotrovimab, a COVID-19 monoclonal
antibody product. CMS created new HCPCS codes, effective May 26, for sotrovimab and to administer sotrovimab
in health care settings and the home.
On June 3, the FDA released a revised Emergency Use Authorization (EUA) for Regeneron’s COVID-19
monoclonal antibody combination product casirivimab and imdevimab. The updated EUA includes a new dosing
regimen (1200 mg vs. 2400 mg) and allows a new route of administration. In response to this change, CMS created
a new HCPCS code, effective June 3, and updated the short and long code descriptors for 2 codes: Q0244, M0243
and M0244.
PG0493 – 07/26/2021On June 24, the FDA released an Emergency Use Authorization (EUA) for tocilizumab, a COVID-19 monoclonal
antibody product. CMS created new HCPCS codes, effective June 24, for tocilizumab and to administer it in the
inpatient setting.
CODING/BILLING INFORMATION
The inclusion or exclusion of a code in this section does not necessarily indicate coverage. Codes referenced in
this clinical policy are for informational purposes only.
Codes that are covered may have selection criteria that must be met.
Payment for supplies may be included in payment for other services rendered.
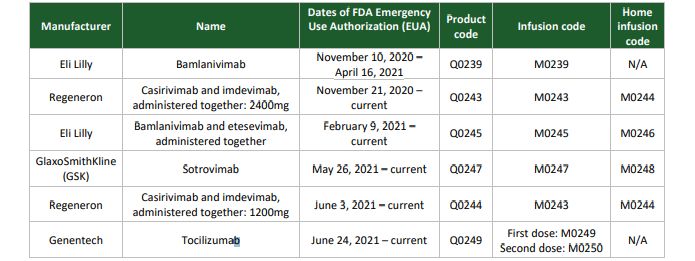
CPT/HCPCS CODE
Intravenous infusion, bamlanivimab-xxxx, includes infusion and post administration monitoring
M0239 (Effective 11/10/2020) (Eli Lilly) Coverage November 10, 2020 - April 16, 2021 Note: On April
16, 2021, the FDA revoked the EUA for bamlanivimab when administered alone.
Intravenous infusion or subcutaneous injection, casirivimab and imdevimab includes infusion or
M0243
injection, and post administration monitoring (Effective 11/21/2020) (Regeneron)
Intravenous infusion or subcutaneous injection, casirivimab and imdevimab includes infusion or
injection, and post administration monitoring in the home or residence; this includes a beneficiary’s
M0244
home that has been made provider-based to the hospital during the COVID-19 public health
emergency* (FDA approved 6/3/2021)
Intravenous infusion, bamlanivimab and etesevimab, includes infusion and post administration
M0245
monitoring (FDA approved 2/9/2021)
Intravenous infusion, sotrovimab, includes infusion and post administration monitoring (FDA
M0247 approved 5/26/2021) The government won’t provide this drug for free; visit the COVID-19 Vaccines
and Monoclonal Antibodies webpage for pricing information (available soon)
Intravenous infusion, sotrovimab, includes infusion and post administration monitoring in the home
or residence; this includes a beneficiary’s home that has been made provider-based to the hospital
M0248 during the COVID-19 public health emergency (FDA approved 5/26/2021) The government won’t
provide this drug for free; visit the COVID-19 Vaccines and Monoclonal Antibodies webpage for
pricing information (available soon)
Intravenous infusion, tocilizumab, for hospitalized adults and pediatric patients (2 years of age and
older) with covid-19 who are receiving systemic corticosteroids and require supplemental oxygen,
M0249
non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO)
only, includes infusion and post administration monitoring, first dose
Intravenous infusion, tocilizumab, for hospitalized adults and pediatric patients (2 years of age and
older) with covid-19 who are receiving systemic corticosteroids and require supplemental oxygen,
M0250
non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO)
only, includes infusion and post administration monitoring, second dose
Injection, bamlanivimab-xxxx, 700 mg (Effective 11/10/2020) (Eli Lilly) Coverage November 10,
Q0239 2020 - April 16, 2021 Note: On April 16, 2021, the FDA revoked the EUA for bamlanivimab
when administered alone.
Q0243 Injection, casirivimab and imdevimab, 2400mg (Effective 11/21/2020) (Regeneron)
Q0244 Injection, casirivimab and imdevimab, 1200 mg (FDA approved 6/3/2021)
Q0245 Injection, bamlanivimab and etesevimab, 2100mg (FDA approved 2/9/2021)
Q0247 Injection, sotrovimab, 500 mg (FDA approved 5/26/2021)
Injection, tocilizumab, for hospitalized adults and pediatric patients (2 years of age and older) with
Q0249 covid-19 who are receiving systemic corticosteroids and require supplemental oxygen, noninvasive
or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) only, 1 mg
Paramount reserves the right to review and revise our policies periodically when necessary. When
there is an update, we will publish the most current policy to
https://www.paramounthealthcare.com/services/providers/medical-policies/ .
PG0493 – 07/26/2021REVISION HISTORY EXPLANATION
ORIGINAL EFFECTIVE DATE: 02/18/2021
Date Explanation & Changes
02/19/2021 Policy created
On April 16, 2021, the FDA revoked the EUA for bamlanivimab, when administered
alone, due to a sustained increase in COVID-19 viral variants in the U.S. that are resistant
04/21/2021
to the solo product. Procedures M0239 and Q0239 are non-covered effective April 17, 2021
forward.
On May 26, the FDA released an Emergency Use Authorization (EUA) for sotrovimab, a
COVID-19 monoclonal antibody product. CMS created new HCPCS codes, effective May
07/01/2021
26, for sotrovimab and to administer sotrovimab in health care settings and the home,
Q0247, M0247, M0248.
On June 24, the FDA released an Emergency Use Authorization (EUA) for tocilizumab, a
07/26/2021 COVID-19 monoclonal antibody product. CMS created new HCPCS codes, effective June
24, for tocilizumab and to administer it in the inpatient setting, Q0249, M0249, M0250
REFERENCES/RESOURCES
National Institute of Health (NIH).(2020) COVID-19 Treatment Guidelines. The COVID-19 Treatment
Guidelines Panel Statement on the Emergency Use Authorization of Bamlanivimab for the Treatment of COVID-19.
Last Update November 18, 2020. Accessed at https://www.covid19treatmentguidelines.nih.gov/statement-on-
bamlanivimab-eua/
National Institute of Health (NIH).(2020) COVID-19 Treatment Guidelines. The COVID-19 Treatment
Guidelines Panel Statement on the Emergency Use Authorization of Casirivimab plus Imdevimab Combination for
the Treatment of COVID-19. Last Update December 2, 2020. Accessed at
https://www.covid19treatmentguidelines.nih.gov/statement-on-casirivimab-plus-imdevimab-eua/
Clinical fact sheet and dosage information can be found at https://www.fda.gov/media/143603/download
Centers for Medicare and Medicaid Services, CMS Manual System and other CMS publications and
services
CMS.gov Centers for Medicare & Medicaid Services, COVID-19 Vaccines and Monoclonal Antibodies.
Accessed at
file:///K:/Claims/Medical%20Policies/REVISED%20Medical%20Policies/PG0493%20COVID-
19%20Monoclonal%20Antibody%20Therapy/COVID-
19%20Vaccines%20and%20Monoclonal%20Antibodies%20_%20CMS.html
PG0493 – 07/26/2021Ohio Department of Medicaid
American Medical Association, Current Procedural Terminology (CPT®) and associated publications and
services
Centers for Medicare and Medicaid Services, Healthcare Common Procedure Coding System, HCPCS
Release and Code Sets
U.S. Preventive Services Task Force, http://www.uspreventiveservicestaskforce.org/
Industry Standard Review
Hayes, Inc.
Industry Standard Review
PG0493 – 07/26/2021You can also read

















































