DOH GUIDELINES for 2019 Edition
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DOH GUIDELINES for LEPTOSPIROSIS for HOSPITALS 2019 Edition
DOH GUIDELINES for
LEPTOSPIROSIS for HOSPITALS
2019 EditionDOH Guidelines for Leptospirosis for Hospitals
iDOH Guidelines for Leptospirosis for Hospitals
FOREWORD
iiDOH Guidelines for Leptospirosis for Hospitals
iiiDOH Guidelines for Leptospirosis for Hospitals
TECHNICAL WORKING GROUP
Research Institute for Tropical Medicine
Celia C. Carlos, MD
Arthur Dessi E. Roman, MD
National Kidney and Transplant Institute
Romina A. Danguilan, MD
Mel-Hatra I. Arakama, MD
CONTRIBUTORS
Amang Rodriguez Memorial Medical Center Imelda M. Mateo, MD
Dr.Jose Fabella Memorial Hospital Esmeraldo T. Ilem, MD
East Avenue Medical Center Alfonso G. Nuñez III, MD
Jose R. Reyes Memorial Medical Center Emmanuel F. Montaña Jr., MD
National Center for Mental Health Alan Baquir, MD
National Children’s Hospital Epifania S. Simbul, MD
National Kidney and Transplant Institute Rose Marie R. Liquete, MD
Joselito R. Chavez, MD
Philippine Orthopedic Center Jose Brittanio S. Pujalte Jr., MD
Quirino Memorial Medical Center Evelyn Victoria E. Reside, MD
Rizal Medical Center Relito M. Saquilayan, MD
San Lazaro Hospital Edmundo B. Lopez, MD
Benjamin D. Estrella Jr., MD
Rontgene M. Solante, MD
Tondo Medical Center Maria Isabelita M. Estrella, MD
Dr. Jose N. Rodriguez Memorial Hospital Alfonso Victorino H. Famaran, MD
Las Piñas General Hospital and Rodrigo H. Hao, MD
Satellite Trauma Center
San Lorenzo Ruiz Women’s Hospital Marilou T. Nery, MD
Valenzuela Medical Center Maria Estrella B. Litam, MD
DOH-TRC Bicutan Alfonso A. Villaroman, MD
DOH-NCR Corazon I. Flores, MD
Ma. Paz P. Corrales, MD
DOH-FICT NCR Emmanuel A. Tiongson, MD
Ruben C. Flores, MD
Francisco A. Valdez, MD
A Project of FICT Team NCR in cooperation with NKTI under the supervision of
Asec. Elmer G. Punzalan.
iiiDOH Guidelines for Leptospirosis for Hospitals
ivDOH Guidelines for Leptospirosis for Hospitals
TABLE OF CONTENTS
Chapter 1: MANAGEMENT PROTOCOL FOR LEPTOSPIROSIS
I. Introduction 1
II. Criteria for Diagnosis 5
III. Indications for Admission and Guidelines on
Site-of-Care Decisions 5
IV. Laboratory Work Up
Leptospiral Tests 7
Non-Leptospiral Tests 8
V. General Guidelines in the Management of Leptospirosis 9
VI. Antibiotic Management 9
VII. Steroid Therapy 11
VIII. Pulmonary Complications of Leptospirosis
Diagnosis of Pulmonary Complications of Leptospirosis 11
Management of Pulmonary Complications of Leptospirosis 12
Extracorporeal Membrane Oxygenation in leptospirosis 15
IX. Renal Complications of Leptospirosis 15
X. Prevention and Control 18
XI. Chemoprophylaxis
Pre-exposure Prophylaxis 18
Post-exposure Prophylaxis 19
XII. References 20
Appendices
Appendix A. Modified Faine’s Criteria (2012) 21
Appendix B. Guidelines in Specimen Collection, Storage,
Transport and Submission 22
ivDOH Guidelines for Leptospirosis for Hospitals
Chapter 2: UPSURGE POLICIES AND PROCEDURES
I. Statement of Purpose and Scope
Purpose 25
Scope 25
II. Key Policies
Criteria for Activation of Leptospirosis Emergency Policy 25
Person Responsible for Activation of the Leptospirosis Upsurge Policy 26
During Office Hours 26
After Office Hours 27
Activation of the Leptospirosis Upsurge Management Team 27
Critical Bed Status Procedure 28
Standards for Admission of Leptospirosis Patients 28
III. Roles and Responsibilities of the Various Departments/ Divisions/Sections
in the Management of a Leptospirosis Upsurge
Emergency Room 29
Division of Internal Medicine 30
Divisions of Adult and Pediatric Nephrology 31
HEMB Team 32
Division of Organ Transplantation and Vascular Surgery 32
Department of Pathology and Laboratory Medicine 32
Section of Pulmonary Medicine 32
Department of Medical Imaging and Therapeutic Radiology 32
Nursing Services 33
Hemodialysis Unit 33
Peritoneal Dialysis Unit 34
Infection Prevention and Control Committee 35
Medical Social Services Division 35
Pharmacy Division 35
Housekeeping Section 36
Procurement and Supply Management Divisions 36
Central Supply and Sterilization Unit 37
Billing and Claims Division 37
Admitting and Discharge Section 37
Information Resource Management Division 38
Nutrition and Dietetics Division 38
vDOH Guidelines for Leptospirosis for Hospitals
IV. Setting up a Leptospirosis Ward 39
V. Staffing Requirements in the Leptospirosis Ward
Medical Staffing 40
Nurses Staffing 41
VI. Health Care Provider Network 42
VII. Antibiotic Prophylaxis for Leptospirosis
For Adults 43
For Pregnant Women 43
For Children 43
Appendices
Appendix A. Treatment Algorithm for Leptospirosis 45
Appendix B. Leptospirosis Prophylaxis Survey 47
Appendix C. Treatment Algorithm for Leptospirosis (Pediatric Patients) 48
Appendix D. Leptospirosis Census Format for Reporting 51
Appendix E. Criteria for Assisted Ventilation for Leptospirosis Patients 52
viDOH Guidelines for Leptospirosis for Hospitals
Chapter 1: MANAGEMENT PROTOCOL FOR LEPTOSPIROSIS
I. INTRODUCTION
Leptospirosis is a zoonotic infection caused by pathogenic spirochetes of the
genus Leptospira. Ten (10) out of the 22 identified species under this genus are
considered pathogenic, while the remaining 7 and 5 are non-pathogenic, free-living
saprophytes (e.g. Leptospira biflexa) or of unclear pathogenicity, respectively.1 An
older system has been used to classify them into serovars (based on serology) so
isolates are currently identified using two systems, e.g. Leptospira
icterohemorrhagiae serovar manilae. Over 250 serotypes of pathogenic leptospires
have been recognized and the severe form of leptospirosis have been reported to
be caused by all of these.2 Leptospira icterohaemorrhagiae, by far, has been
commonly associated with severe disease. In the Philippines, earlier studies
reported that the major serovars affecting humans in Metro Manila and neighboring
provinces were Manilae, Losbanos, Tarassovi, and Poi.3
In Philippines, leptospirosis tends to occur frequently in urban flood-prone
areas such as Metro Manila. This disease gained much attention after an outbreak
following typhoon Ondoy in October of 2009. About two weeks following this heavy
rainfall typhoon that left many areas of Metro Manila flooded, the Department of
Health reported 2,894 probable and confirmed cases of leptospirosis with 210
deaths.4
From January 1, 2018 to December 31, 2018, a total of 5,232 cases were
reported to the Department of Health with a case fatality rate of 9.65%. This is a
71% increase in the total number of cases compared to 2017.5 In fact, in July of
2018, the Department of Health has declared an outbreak of leptospirosis in certain
areas of Metro Manila. Outbreaks of leptospirosis in the Philippines are expected to
occur with increasing incidents of heavy rainfall, rapid urbanization (dramatic
increase in populations), deforestation, increasing number of flood-prone areas,
poor infrastructures, among many other factors.
Leptospirosis is primarily a disease of domesticated and wild animals. Humans
are infected through direct and indirect contact with these animals. The source of
infection is water or soil contaminated with infected urine, infected urine or tissues
from infected animals. The leptospires enter through cuts and abrasions in the skin
or mucosal surfaces, the conjunctiva, or by inhalation (into the lungs) of droplets or
aerosols of fluid containing leptospires. After penetrating intact mucous membranes
or abraded skin, leptospires enter the blood stream and are rapidly carried to all
1DOH Guidelines for Leptospirosis for Hospitals
parts of the body (including the cerebrospinal fluid [CSF] and the eyes) presenting
as an acute, systemic disease is characterized by extensive vasculitis.
The incubation generally is 5-14 days but a range of 2 to 30 days has been
noted. The incubation period does not vary significantly among serotypes. It may
present as influenza-like illness with headache and myalgia in its mild form and may
present with jaundice, renal dysfunction and hemorrhage (Weil’s Syndrome) when it
presents as severe form.
Leptospirosis presents in two (2) forms: anicteric (mild) or icteric (severe)
leptospirosis. Anicteric (mild) leptospirosis is often characterized by abrupt onset
of fever, headache, severe muscle aches, malaise and prostration. High intermittent
fever, chills, persistent headache, severe myalgias, abdominal pain and nausea and
vomiting persist for 4-7 days. Death almost NEVER occurs during this stage. In
anicteric infections, the second stage may not occur. On the other hand, icteric
(severe) leptospirosis or Weil Syndrome may present with impaired renal and
hepatic function, hemorrhage, vascular collapse, and even severe alterations in
consciousness. This form has a high mortality rate.
The clinical course of leptospirosis varies but it is generally predictable. Both
forms of leptospirosis follow a biphasic course:
1. The LEPTOSPIREMIC PHASE (or ACUTE stage) is characterized by an
acute systemic infection. The onset of symptoms is abrupt and resolves
after 4-7 days. Symptomatic improvement and lysis of the fever coincide
with the disappearance of leptospires from the blood, cerebrospinal fluid
and all other tissue with the EXCEPTION of the aqueous humor (resolves
in 4-30 days) and renal parenchyma (persists for 1-4 weeks in the urine).
Antibody titers to leptospires develop rapidly. This immune response
heralds the second or immune stage of the illness.
2. The IMMUNE PHASE (sometimes LEPTOSPIRURIC PHASE,
CONVALESCENT STAGE) is the second stage and lasts 4-30 days.
Occasionally, there is a brief asymptomatic period of 2-3 days between the
two stages. Leptospiruria continues for 1 week to 1 month. Generally, this
phase is not affected by antibiotic therapy. This phase is characterized by
the presence of circulating antibody and development of meningitis, uveitis,
rash, and (in severe cases) hepatic and renal involvement. In icteric cases,
leptospires can sometimes be isolated from the blood for 24-48 hours after
the appearance of jaundice.1
2DOH Guidelines for Leptospirosis for Hospitals
In the Philippines, majority of the symptoms of Leptospirosis is non-specific,
which indicates that the initial impression could be viral rather than bacterial. Table 1
lists down the percentage frequencies of signs and symptoms of leptospirosis seen
in our local setting. A comparison of two studies from the Philippine 2009 outbreak
reported that the most common clinical features include fever, myalgia, conjunctival
suffusion, malaise, headache, abdominal pain, oliguria, and jaundice.
Table 1. Clinical Features of Leptospirosis after a flood, National Capital Region, 2009
Sign or Symptom 9 Manila Hospitals, 20096 San Lazaro Hospital, 20097
Number of patients 259 confirmed leptospirosis cases 471 cases
Fever 98.5 100*
Myalgia/calf-tenderness 78.1 76.7
Malaise 74.9 44.2
Headache 55.6 52.2
Chills 44.8 NR
Conjunctival suffusion 59.3 78.1
Hypotension 23.6 NR
Abdominal pain 52.7 61.2
Nausea/vomiting 52.0 57.8
Diarrhea 39.0 40.8
Jaundice 38.0 47.8
GI bleeding 16.1 NR
Oliguria 56.6 60.7
Hematuria 22.3 33.1
Cough 30.5 17.6
Dyspnea 21.6 NR
Crackles/rales 23.3 NR
Hemoptysis 14.9 3.2
Hemorrhagic signs 14.6 0.4
*part of inclusion criteria; NR – no report
These clinical findings are consistent with prior local studies done in Metro
Manila since the 1970s (Table 2).
3Table 2. Clinical features of seasonal leptospirosis admitted at various hospitals in Metro Manila compared with the 2009 outbreak 8
DOH Guidelines for Leptospirosis for Hospitals
4DOH Guidelines for Leptospirosis for Hospitals
II. CRITERIA FOR DIAGNOSIS
Leptospirosis should be suspected in an individual with:
An acute febrile illness of at least 2 days AND
Two or more of the following symptoms: myalgia, calf tenderness,
conjunctival suffusion, chills, abdominal pain, headache, jaundice, or
oliguria AND
Any risk factor for acquiring the disease which includes:
- residing in a flooded area
- wading or swimming in floods and contaminated water, with or
without cuts or wounds
- contact with animal fluids especially carcass
- ingestion of contaminated water
A checklist for diagnosing leptospirosis for frontliners have been developed
(See Appendix A). The checklist consists of three parts: Clinical data,
Epidemiologic factors and Bacteriologic and laboratory findings. Using paired MAT
as the gold standard, the estimated sensitivity and specificity of the WHO criteria
were 33% and 66% respectively.9 Studies on the clinical utility of this criteria are
were probably limited by the small sample size.
III. INDICATIONS FOR ADMISSION AND GUIDELINES ON
SITE-OF-CARE DECISIONS
Patients with suspected leptospirosis presenting with MILD symptoms can be
managed on an OUT-PATIENT SETTING. These include patients with stable vital
signs, anicteric sclerae, no jaundice, with good urine output, no evidence of
meningismus/ meningeal irritation, no dyspnea, no tachypnea, no hemoptysis, no
bleeding, not in sepsis / septic shock, and can take oral medications.
On the other hand, patients with suspected MODERATE to SEVERE
LEPTOSPIROSIS should be admitted in a healthcare facility for proper diagnosis
and appropriate monitoring and management. The presence of the following signs
and symptoms will classify a patient to have moderate to severe leptospirosis and
will require admission:
Unstable vital signs
Jaundice / Icteric sclerae
Abdominal pain
Nausea, vomiting and diarrhea
5DOH Guidelines for Leptospirosis for Hospitals
Oliguria or anuria
Bleeding
Meningismus / meningeal irritation
Sepsis / septic shock
Altered mental status
Difficulty of breathing or hemoptysis
Patients with leptospirosis who are suspected to have pulmonary
complications such as pulmonary hemorrhage or acute respiratory distress
syndrome (ARDS) require special attention because these conditions have been
consistently associated with increased mortality. These patients present with
dyspnea, tachypnea, chest x-ray findings of localized or multilobar infiltrates or
pleural effusion. The decision to admit a leptospirosis patient with pulmonary
complications will depend on the level of hypoxemia (see Table 6).
Moderate hypoxemia: 100DOH Guidelines for Leptospirosis for Hospitals
PRESUMPTIVE diagnosis of Leptospirosis may be based on the following
findings:
positive dark field examination;
presentation of clinical symptoms that are compatible with leptospirosis and a
microscopic agglutination titer of 1:100 or greater;
a positive macroscopic agglutination slide test reaction on a single specimen
obtained after the onset of symptoms; and
stable microscopic agglutination titer of 1:100 or greater in two or more serum
specimens obtained after the onset of symptoms
A. LEPTOSPIRAL TESTS
1. Microbiologic Test: Culture Method (definitive)
Culture of leptospires can be done using blood or cerebrospinal fluid (CSF)
obtained during the septicemic stage of illness or urine during the immune
and convalescent stage. Additionally, tissue sections obtained by biopsy or
at necropsy, can be submitted for culture of Leptospira. The media used
for culture are Fletcher semisolid medium or Ellinghausen-McCullough -
Johnson-Harris (EMJH) semisolid medium or Tween 80 - albumin medium
(OAC) or Korthoff medium. Cultures are incubated at 28-30oC in the dark
for 6 weeks or longer.
2. Microbiologic Test: Non-culture Method
a. Dark field microscopy – recommended as an aid that may suggest BUT
NOT establish the diagnosis of Leptospirosis
b. PCR for detection of leptospiral nucleic acid in blood or urine (definitive)
3. Serologic Tests
a. Microscopic Agglutination Test (MAT) – detects agglutinating antibodies
against live leptospires using darkfield microscopy. The 21-serovar MAT
is considered the "reference standard" or cornerstone of serodiagnosis
of leptospirosis. However, a genus-specific MAT using a non-
pathogenic Leptospira patoc I strain are being performed by some
centers.
Interpretation:
Single specimen: Titer > 1:800 (probable)
Paired specimen (using acute and convalescent sera): four-fold increase
(definitive)
7DOH Guidelines for Leptospirosis for Hospitals
b. Rapid leptospiral diagnostic kits (i.e. immunochromatographic tests or
ICTs) - useful rapid tests in the early diagnosis of leptospirosis among
patients with compatible signs and symptoms. There is an increasing
number of tertiary healthcare facilities that are offering these rapid tests
already.
c. IgM ELISA- simple, with acceptable sensitivity that is quite variable
depending on the method of ELISA performed
Table 3. Appropriate timing of Specimen collection for specific leptospiral tests
Timing 0-7 days 7-14 days 14-28 days
(from onset of illness)
Specimen and leptospiral CSF for culture or darkfield
test microscopy
Dialysate for leptospiral
culture
Heparinized blood for
culture and or PCR
Serum (acute specimen) Serum for serologic tests (rapid ICTs, IgM
for MAT ELISA) and MAT (convalescent specimen)
Urine for culture
Refer to Annex B: Guidelines on Specimen collection, storage and transport
for leptospiral tests.
B. NON-LEPTOSPIRA TEST
a. MILD
1. CBC with quantitative platelet count
2. Urinalysis
3. BUN and Creatinine
4. Liver function tests (SGPT, SGOT)
b. MODERATE to SEVERE (request each test if clinically indicated)
1. Serum sodium and potassium
2. Bilirubins (Total Bilirubin, direct and indirect bilirubin)
3. PT/PTT
4. Total protein with A/G, Alkaline phosphatase
5. Chest X-ray
6. 12-Lead ECG
7. Arterial blood gas (ABG) - severe metabolic acidosis (ph< 7.2,
HCO3DOH Guidelines for Leptospirosis for Hospitals
V. GENERAL GUIDELINES IN THE MANAGEMENT OF LEPTOSPIROSIS
Most cases of leptospirosis will be mild and self-limited. A suspicion of
leptospirosis should warrant management as such even without evidence from
leptospiral diagnostics.
Supportive management with hydration and analgesic/antipyretic therapy with
paracetamol are recommended.
Correct electrolyte derangements.
Knowledge on the clinical indicators of progression from an undifferentiated
fever to severe leptospiral disease is very limited. Thus, it is recommended
that any illness [regardless of severity, duration or phase of the disease] that
prompts a patient to seek medical consult and leptospirosis is suspected,
antibiotic therapy should be administered to shorten the duration of illness
and reduce shedding of organisms in the urine.
When the disease is classified as severe, the management is generally the
same as in the management of organ failure from sepsis. Supportive care
with renal replacement therapy, ventilatory support, and blood products may
be required. Consequently, timely referrals to specialists and facilities who
can provide such services are also recommended to prevent delays and
progression of anticipated complications.
The subsequent chapters will discuss the specific recommendations in the
various aspects of leptospirosis management.
VI. ANTIBIOTIC MANAGEMENT
All patients with suspected leptospirosis should be started on antimicrobial
therapy regardless of the phase of the disease of duration of symptoms to shorten
the duration of illness. While there is insufficient evidence on the use of antibiotics
in preventing death from leptospirosis, its use has been shown to have beneficial
effects on several clinically relevant and important outcomes (e.g. decreased the
duration of clinical illness by 2-4 days).10
Treatment with effective antibiotics should be initiated as soon as the
diagnosis of leptospirosis is suspected. Antibiotic administration should not be
delayed regardless of the need for renal replacement therapy.
Doxycycline 5 mg/kg/day PO in 2 divided doses (max 200mg/day) x 1 week.
9DOH Guidelines for Leptospirosis for Hospitals
Table 4. Recommended Antibiotic Regimens for Leptospirosis
MILD LEPTOSPIROSIS
ADULT CHILDREN
First line
Doxycycline 100 mg BID PO for 10 days Amoxicillin 30-50 mg/kg/day in 3 divided
doses. Maximum of 2 grams per day
Alternative
Amoxicillin 500mg QID or 1g q8h
Azithromycin dihydrate 1 g initially, Erythromycin 10 mg/kg/day orally in four
followed by 500 mg OD for 2 more divided doses for 1 week
days
SEVERE LEPTOSPIROSIS (WEIL SYNDROME)
ADULT CHILDREN
Penicillin G 1.5 million units IV q 6 Aqueous penicillin G 6-8 million U/m2/day
regimen
Primary
hrs for 7 days in 6 divided doses for 1 week
Ceftriaxone 1gm q24h for 7 days Ampicillin 100 mg/kg/day IV every 6 hours
Ampicillin 0.5-1.0 gm q6h Tetracycline 25-50 mg/kg/day orally in four
Azithromycin dihydrate 500 mg OD divided doses or IV tetracycline 10-
for 5 days 20mg/kg/day IV in four divided doses, max
Cefotaxime 1 gm q6h 3 g/day, avoid in children < 9 years
Alternative
Doxycycline 5 mg/kg/day PO in 2 divided
doses (max 200mg/day) x 1 week
Ampicillin 100 mg/kg/day IV every 6 hours
or
Erythromycin 10 mg/kg/day orally in four
divided doses for 1 week
Note: Step-down therapy can be instituted once patient is clinically stable and able to tolerate oral
medication. Any oral antibiotic can be selected.
Table 5. Dosage of Antibiotics in Adults with Renal Impairment
Antibiotic Dose for Adjustment for renal failure
Normal Renal Function Estimated creatinine clearance (CrCl), ml/min
50-90 10-50DOH Guidelines for Leptospirosis for Hospitals
VII. STEROID THERAPY
Steroids have been reported to reduce or delay the need for ventilator support,
improve PTT or mortality among patients with leptospirosis. While the evidence for
its use is not overwhelming, steroid therapy has found relevance in clinical practice
given the devastating complications of severe leptospirosis, particularly pulmonary
hemorrhage. Thus, steroid therapy is suggested for:
(1) patients at high-risk of pulmonary hemorrhage, and
(2) AKI PLUS any of the following:
platelet countDOH Guidelines for Leptospirosis for Hospitals
On top of the clinical factors, findings from important laboratory tests aid in the
diagnosis of ARDS. The severity of pulmonary involvement can be assessed by
abnormalities on chest radiograph and arterial blood gas.
1. Radiographic findings commonly accompany pulmonary symptoms. All
patients have bilateral pulmonary infiltration and maybe seen as early as the
first 24 hours of the systemic stage of leptospirosis.
2. Hypoxemia and hypocarbia are common blood gas abnormalities. Elevated
PCO2 is seen in severe cases. Continuous monitoring of oxygen saturation is
recommended in the presence of pulmonary complications.
The table below are parameters that can be used for the diagnosis of ARDS
and for risk stratification to identify site-of-care, particularly the level of oxygenation.
Table 6. American-European Consensus Conference Criteria for ARDS11
Timing Within 1 week of a known clinical insult or new/worsening respiratory
symptoms
Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid
overload; Need objective assessment (e.g., echocardiography) to
exclude hydrostatic edema if no risk factor present
Mild Moderate Severe
Oxygenation 200DOH Guidelines for Leptospirosis for Hospitals
Figure 1. Algorithm for the Diagnosis and Management of Leptospirosis with Pulmonary
Complications
13DOH Guidelines for Leptospirosis for Hospitals
Non-invasive ventilation (NIV) vs. Invasive ventilation
A trial of NIV can be done in most patients who do not require emergent
intubation. The presence of the following conditions, however, are contrainidication
to NIV and therefore warrant invasive ventilation:
Table 7. Contraindications To Non-Invasive Positive Pressure Ventilation12
Non-respiratory organ failure that is acutely life-threatening
Severe encephalopathy (eg, GCSDOH Guidelines for Leptospirosis for Hospitals
This maneuver requires 3-5 people, paying close attention to endotracheal
tube (ETT) and central lines. Make sure that patient has an empty stomach. Steps
in prone positioning:
1. Pre-oxygenation
2. Suction endotracheal tube and oral cavity
3. Remove ECG leads and reattach to back after shifting position.
4. Turn over the patient to the prone position.
5. Do repeated zeroing of hemodynamic transducers
6. Support and frequently reposition pressure points: face, shoulder, anterior
pelvis
Successful trials evaluating prone positioning in ARDS used at least 16 hours
of daily proning. When PaO2/FiO2 remained > 150 mm Hg 4 h after supinating
(with PEEP < 10 cm H2O and FiO2 < 0.6), stop prone positioning.
C. Extracorporeal Membrane Oxygenation (ECMO) in leptospirosis
The benefits of ECMO use in severe pulmonary form of leptospirosis and
associated ARDS are still under evaluation.
ECMO has been used more extensively as a potential bridge therapy in
patients with severe ARDS and/or massive hemoptysis.
The best outcome in ECMO for adult respiratory failure occurs when ECMO is
instituted early after the onset (1-2 days).
ECMO is done in a highly specialized center with a trained multi-disciplinary
team. Should ECMO be considered, prompt referral and close coordination
should be done to such centers who can perform the procedure.
IX. RENAL COMPLICATIONS OF LEPTOSPIROSIS
Renal complications of leptospirosis may present in a spectrum which may
span from sterile pyuria , tea colored urine, mild proteinuria to severe anuric acute
renal failure.
Commonly it may present as non-oliguric renal failure with mild hypokalemia.
Oliguria with hyperkalemia may reflect the severity of AKI and may connote poor
prognosis. Oliguria is defined as urine output < 0.5 mL/kg/hr orDOH Guidelines for Leptospirosis for Hospitals
The following are the list of diagnostic tests that should be performed when
AKI is suspected:
CBC with platelet count
BUN, creatinine, sodium, potassium, AST, ALT, bilirubins
Urinalysis
Chest x-ray – check for congestion and/or signs of pulmonary hemorrhage
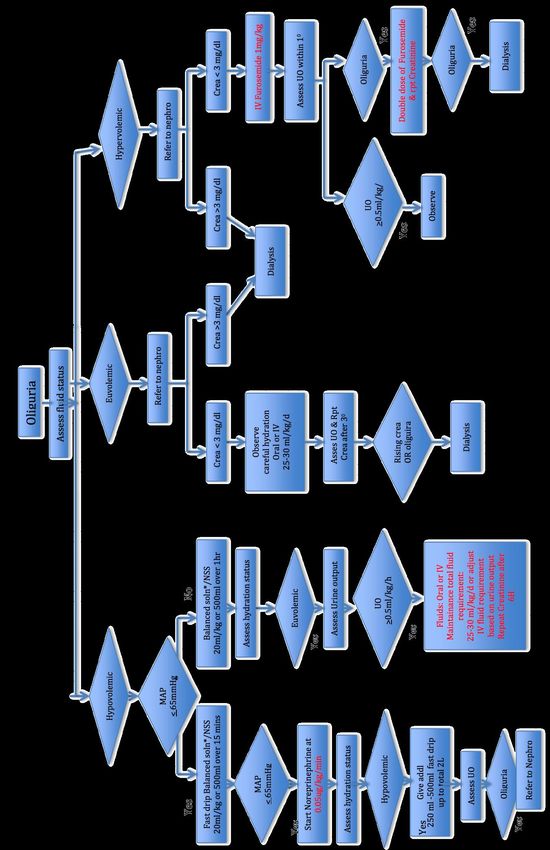
The algorithm below (Figure 2) is a guide in the management of leptospirosis
patients that present with oliguria.
The recommended initial fluid resuscitation for Leptospirosis patient is
Balanced crystalloids. If potassium is in the high normal value or with hyperkalemia,
Isotonic saline is recommended. Hydroxyethyl starch should be NOT be given
because it is associated with increased risk of Acute Kidney Injury, need for Renal
Replacement and mortality.
The recommended initial fluid resuscitation rate is 20ml/kg/h or 500ml of crystalloids
within 15- 30mins Patients with Leptospirosis are prone to ARDS due to
downregulation of the Na transport via Epithelial Sodium Channel (ENaC),
NaKATPase as well as decrease in Aquaporin P5.
Any one of the following are indications for dialysis:
Uremic symptoms- nausea, vomiting, altered mental status, seizure, coma
pH 3 mg/dl in ABG
Serum K >5 meq in an oliguric patient
ARDS, pulmonary hemorrhage (GRADE: moderate)
Hemodialysis is preferred over peritoneal dialysis in patients with AKI secondary to
Leptospirosis. The latter is a valid option if hemodialysis machine is not readily
available.
Daily dialysis is suggested to maintain strict control of azotemia and fluid volume
which can improve survival for those patients with severe Leptospirosis especially if
with pulmonary hemorrhage.
16Figure 2. Algorithm for leptospirosis patients with oliguria
DOH Guidelines for Leptospirosis for Hospitals
17DOH Guidelines for Leptospirosis for Hospitals
X. PREVENTION AND CONTROL
A. Hygienic conditions should be encouraged in slaughterhouses, farmyard
buildings and bathing pools
B. Avoidance of exposure to urine and tissues from infected animals such as
wading in flooded areas. Likewise, activities in possible contaminated bodies
of water should be prevented.
C. Vaccination of animals against leptospirosis
D. Rodent control
E. When a potential exposure to contaminated water is anticipated, individuals
should wear protective clothing (boots, gloves, spectacles), cover skin
lesions with waterproof dressings, wash or shower after exposure to
contaminated water, and wash and clean wounds.
F. Avoid drinking water from possible contaminated water sources.
G. Chemoprophylaxis (see next section)
XI. CHEMOPROPHYLAXIS
The use of chemoprophylaxis requires prior consult with a physician. It should
not be taken unless prescribed and fully explained by a physician, including
common side-effects and contraindications. Since antibiotic prophylaxis is not 100%
effective, individuals should continue to monitor themselves for fever and other flu-
like symptoms and should continue to wear personal protective measures when
contact with contaminated water is anticipated.
A. Pre-exposure Prophylaxis
Pre-exposure antibiotic prophylaxis is NOT ROUTINELY RECOMMENDED.
However, this may be considered for short-term exposures in those individuals who
intend to visit highly endemic areas AND are likely to get exposed, including but not
limited to:
Travelers
Soldiers
People who engage in water-related recreational and occupational
activities
Disaster relief workers deployed to flooded or post-typhoon areas
Doxycycline 200mg orally once a week, to begin 1 to 2 days before exposure
and continued throughout the period of exposure.
18DOH Guidelines for Leptospirosis for Hospitals
B. Post-exposure prophylaxis
Post-exposure prophylaxis is given following contact with contaminated
sources such as flood water, animal carcasses, infected body fluids, etc. The post-
exposure prophylactic regimens depends on the risk for leptospirosis following the
exposure (see Table 7).
Table 8. Post-exposure prophylaxis for leptospirosis in adults and children
ADULTS
MILD MODERATE HIGH RISK
single exposure, non-mucosal, no mucosal exposure, presence or When there is repeated or
breaks in the skin wound continuous exposure
Doxycycline 200mg single dose, Doxycycline 200 mg once daily Doxycycline 200 mg once
immediately within 24 to 72 hours for 3-5 days to be started weekly until the end of
from exposure immediately within 24 to 72 hours exposure
from exposure
CHILDREN13
First-line: Doxycycline 4 mg/kg single dose, max dose: 200 mg
Alternative:
Azithromycin 10 mg/kg single dose, max dose: 500 mg*
Amoxicillin 50 mg/kg/day q 6 hrs for 3-5days, max dose: 500 mg q6 hrs**
Note: * Efficacy for prevention of leptospirosis was seen in vitro and animal models
** No clinical trial for prevention of leptospirosis, but amoxicillin is a known alternative for the treatment of disease
Doxycycline has been known to cause permanent discoloration or enamel
hypoplasia in developing teeth (among fetuses and children). There are currently no
good quality evidence on pre- or post-exposure prophylaxis among children and
pregnant patients. However, the American Academy of Pediatrics recently released
a new statement saying that short course doxycycline therapy (i.e.DOH Guidelines for Leptospirosis for Hospitals
XII. REFERENCES
1. Marquez A, Djelouadji Z, Lattard V, Kodjo A. Overview of laboratory methods to diagnose
Leptospirosis and to identify and to type leptospires. Int Microbiol. 2017;20(4):184-193.
doi:10.2436/20.1501.01.302
2. World Health Organization Southeast Asia Regional Office. Leptospirosis - Fact Sheet.
http://www.searo.who.int/about/administration_structure/cds/CDS_leptospirosis-
Fact_Sheet.pdf. Accessed July 4, 2019.
3. Yanagihara Y, Villanueva S, Yoshida S, Okamoto Y, Masuzawa T. Current status of
leptospirosis in Japan and Philippines. Comp Immunol Microbiol Infect Dis. 2007;30:399-413.
4. United Nations Office for the Coordination of Humanitarian Affairs. Philippines Typhoon
Season 2009 Situation Report#14 (30 October 2009).; 2009.
5. Republic of the Philippines Department of Health. Leptospirosis Quarterly Surveillance Report
No. 4 (2018).; 2018.https://portal2.doh.gov.ph/sites/default/files/statistics/
2018_Leptospirosis_QSR_N4.pdf. Accessed July 4, 2019.
6. Roxas EA, Alejandria MM, Mendoza MT, Roman ADE, Leyritana KT, Ginete-Garcia JKB.
Leptospirosis Outbreak after a Heavy Rainfall Typhoon in the Philippines: Clinical Features,
Outcome and Prognostic Factors for Mortality. Acta Med Philipp. 2016;50(3):121-128.
https://www.actamedicaphilippina.org/article/6866-leptospirosis-outbreak-after-a-heavy-
rainfall-typhoon-in-the-philippines-clinical-features-outcome-and-prognostic-factors-for-
mortality. Accessed July 4, 2019.
7. Amilasan A-ST, Ujiie M, Suzuki M, et al. Outbreak of leptospirosis after flood, the Philippines,
2009. Emerg Infect Dis. 2012;18(1):91-94. doi:10.3201/eid1801.101892
8. Collaborative Statement of the Philippine Society for Microbiology and Infectious Diseases,
Philippine Society of Nephrology and the Philippine College of Chest Physicians Council on
Critical Care and Pulmonary Vascular Diseases. The Philippine Clinical Practice Guidelines
on the Diagnosis, Treatment and Prevention of Leptospirosis in Adults 2010. 2010.
9. Brato D, Mendoza M, Cordero C, et al. Validation of the World Health Organization (WHO)
Criteria Using the Microscopic Agglutination Test (MAT) as the Gold Standard in the
Diagnosis of Leptospirosis. PJMID. 27(4):125-128.
10. Brett-Major DM, Coldren R. Antibiotics for leptospirosis. Cochrane Database Syst Rev.
2012;(2):CD008264. doi:10.1002/14651858.CD008264.pub2
11. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et al. Acute Respiratory Distress
Syndrome. JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
12. Organized jointly by the American Thoracic Society, the European Respiratory Society, the
European Society of Intensive Care Medicine, and the Société de Réanimation de Langue
Française, and approved by ATS Board of Directors, December 2000. International
Consensus Conferences in Intensive Care Medicine: Noninvasive Positive Pressure
Ventilation in Acute Respiratory Failure. Am J Respir Crit Care Med. 2001;163(1):283-291.
doi:10.1164/ajrccm.163.1.ats1000
13. Pediatric Infectious Disease Society of the Philippines. POST DISASTER INTERIM ADVICE
ON THE PREVENTION OF LEPTOSPIROSIS IN CHILDREN. 2012.
14. American Academy of Pediatrics Committee on Infectious Diseases, Kimberlin D, Brady M,
Jackson M, Long S. Red Book 2018-2021 Report of TheCommittee on Infectious Diseases.
31st ed.; 2018. https://redbook.solutions.aap.org/book.aspx?bookid=2205. Accessed July 4,
2019.
20DOH Guidelines for Leptospirosis for Hospitals
APPENDICES
Appendix A. Modified Faine’s Criteria (2012)
This check-list is designed for those who deal directly with the patient. It may
be used even before results of leptospiral diagnostic tests are available. To use the
this, give the appropriate score if the parameter is present for the patient and
compute for the sum.
MODIFIED FAINE’S CRITERIA (2012)
Clinical data Epidemiological Bacteriological and laboratory
(Part A) factors (Part B) findings (Part C)
Headache 2 Rainfall 5 Isolation of leptospira in
culture - Diagnosis certain
Fever 2 Contact with 4 PCR 25
contaminated
Environment
Temperature >39°C 2 Animal contact 1 Serology
Conjunctival suffusion 4 ELISA IgM positive* 15
Meningism 4 SAT positive* 15
Conjunctival suffusion 10 Other rapid tests** 15
+ Meningism
+ Myalgia
Jaundice 1 MAT – single positive in 15
high titer
Albuminuria/Nitrogen retention 2 MAT – rising 25
titer/seroconversion
Hemoptysis/Dyspnea 2 * Any one of the tests only
should be scored
** Latex agglutination
test/Lepto dipstick/Lepto
Tek lateral flow/Lepto Tek
Dri-Dot test
Presumptive diagnosis of leptospirosis is made if:
Part A or Part A and Part B score: 26 or more
Parts A, B, C (Total): 25 or more
A score between 20 and 25 suggests leptospirosis as a possible diagnosis.
Table adapted from: Shiva Kumar, S. Indian Guidelines for the Diagnosis and Management of
Human Leptospirosis (2013), p. 26. Accessed on 4 July 2019 from
http://www.apiindia.org/medicine_update_2013/chap07.pdf
21Appendix B: Guidelines in Specimen Collection, Storage, Transport and Submission
DOH Guidelines for Leptospirosis for Hospitals
22DOH Guidelines for Leptospirosis for Hospitals
23DOH Guidelines for Leptospirosis for Hospitals
24DOH Guidelines for Leptospirosis for Hospitals
Chapter 2: UPSURGE POLICIES AND PROCEDURES
I. STATEMENT OF PURPOSE AND SCOPE
A. Purpose
It is the purpose of this manual to define the actions and roles necessary to
provide a coordinated response during an upsurge in leptospirosis cases in the
HEALTHCARE FACILITY. This manual provides guidance to all the Departments
within the HEALTHCARE FACILITY, with a general concept of potential Upsurge
assignments before, during, and following a Leptospirosis Upsurge. It also
provides for the systematic integration of Upsurge resources when activated
including purchasing of necessary supplies and materials for renal replacement
therapy, supporting the provision of necessary services, and even upgrading the
facilities of the areas assigned to become temporary “leptospirosis wards.”
Important as well is the allocation of financial support or resources from
government agencies such as the Department of Health (DOH), specifically the
Health Emergency Management Bureau (HEMB) and the Field Implementation
and Coordination Team for NCR. It also includes activation of communications
networking with relevant government, non-government agencies and media
focusing on the prophylaxis, prevention and early treatment of leptospirosis.
B. Scope
This plan applies to all participating Divisions/Departments within the
HEALTHCARE FACILITY.
II. KEY POLICIES
A. Criteria for Activation of the Leptospirosis Upsurge Policy
The Leptospirosis Upsurge Policy will be activated when there is a surge in the
number of leptospirosis patients requring admission to the HEALTHCARE
FACILITY to ensure that patients receive appropriate and timely medical care,
renal replacement and respiratory support using the HEALTHCARE FACILITY
criteria to guide health care:
Opening of a Leptospirosis Ward
The HEALTHCARE FACILITY will identify the CRITICAL NUMBER OF
PATIENTS BEING ADMITTED FOR LEPTOSPIROSIS PER DAY that will
activate the policies and procedures in this handbook. When this critical number
of patients who require more than simple hydration (i.e. renal replacement
25DOH Guidelines for Leptospirosis for Hospitals
therapy, blood component transfusion or requiring respiratory support) is
reached, a Leptospirosis Ward will be identified and opened for these patients.
Stable patients who do not require ventilatory support will be placed in the
Leptospirosis Ward, while toxic patients who are unstable, requiring inotropic
support, ventilatory support or who require intensive monitoring as they are likely
to need intubation, will be admitted to the regular wards. Unstable patients will be
placed in a special identified ward with a higher nurse to patient ratio.
B. Person Responsible for Activation of the Leptospirosis Upsurge Policy
DURING OFFICE HOURS from Monday-Friday, 8:00AM - 5:00PM, the
Head Nurse and Head Consultant of the Emergency Room (ER) will inform the
Executive Office if the criteria for activation of the Leptospirosis Upsurge Policy
has been met. Any one of the Deputy Executive Directors or the Chief of Hospital
will activate the Leptospirosis Upsurge Policy.
Upon Activation of the Leptospirosis Upsurge Policy, the Secretary of any of
the Deputy Executive Directors or Chief of Hospital will send out a memorandum
through Outlook, and will notify the Heads of the following Departments /
Divisions:
Divisions of Adult and Pediatric Nephrology
Division of Internal Medicine
Division of Organ Transplantation and Vascular Surgery
Nursing Services
- All Head Nurses or Charge Nurses in all Clinical Wards
- Operating Room (OR)
Department of Pathology and Laboratory Medicine
Section of Pulmonary Medicine
Pharmacy, Procurement, Supply, Central Supply and Sterilization Unit
(CSSU), Housekeeping, Billing and Claims, Admitting and Discharge
Medical Social Services Division (MSSD)
Information Resource Management Division (IRM)
- Upload Hospital Memorandum regarding the activation of the
Leptospirosis Upsurge Policy to all concerned departments through
OUTLOOK
- Inform all Heads of the concerned Department/Division including the
Chief of Hospital and Deputy Executive Directors through SMS
HEALTHCARE FACILITY-HEMB
26DOH Guidelines for Leptospirosis for Hospitals
AFTER OFFICE HOURS from Monday-Friday, weekends and holidays, the
ER Charge Nurse will contact the Senior House Officer (SHO) who will activate
the Leptospirosis Upsurge Policy and inform IRM to disseminate the information.
(See Diagram I)
ER
Chief of Hospital and Senior House All Other
Deputy Executive Directors Officers (SHO) Departments
IRM All Medical Nursing
Depts/Divisions
Deploy Memo through All Nursing
OUTLOOK to all those Departments
on Duty and all the their
Heads by SMS
Diagram I: Activation of Leptospirosis Upsurge Policy
after Office Hours
C. Activation of the Leptospirosis Upsurge Management Team
Once the Leptospirosis Upsurge Policy is activated, the Chief of Hospital or
any of the Deputy Executive Directors will call on a meeting of the Leptospirosis
Upsurge Management Team, to coordinate efforts on ensuring adequate
provisions of necessary services for the leptospirosis patients. Meetings can be
called on daily to update the entire team of the needs of the Leptospirosis ward
and other areas. A Leptospirosis Upsurge Management Team Head will be
assigned by the Chief of Hospital.
This team is composed of the following:
Chief of Hospital/Deputy Executive Director/s – Head
Chair, Departments/Divisions of Adult and Pediatric Nephrology, Internal
Medicine, Vascular, Laboratory Medicine
Deputy Executive Director for Nursing Services
ER Head
Head Nurse of ER, Clinical Wards, HD Unit, PD Unit, Operating Room
Head of Housekeeping, Purchasing, Warehouse, Pharmacy, CSSU,
PBSD, MSSD, IRM, HEALTHCARE FACILITY-HEMB
27DOH Guidelines for Leptospirosis for Hospitals
D. Critical Bed Status Procedure – HEALTHCARE FACILITY Leptospirosis Upsurge
Policy
It is the goal of this Policy to provide a systematic method for identifying the
available hospital beds, to unload the ER, to ensure that beds are being
appropriately used during critical bed status, and to prevent the denial of
transfers from other government hospitals during a Leptospirosis Upsurge. This is
to ensure that patients receive proper medical care.
Procedure:
The post duty Senior Adult Nephrology Fellow will report on the total bed
status and availability, to the Head of the Leptospirosis Upsurge Management
Team by 8:00AM every morning.
The Chief Fellow / Resident will prioritize admissions of the Leptospirosis
patients especially those who need RRT or require ventilator support.
E. Standards for Admission of Leptospirosis Patients
All patients with a presumptive diagnosis of Leptospirosis will be triaged
under the Division of Internal Medicine with the following criteria:
1. Serum Creatinine: < 3 mg/ dl
2. Absence of Criteria for Pulse Therapy
All patients with a presumptive diagnosis of Leptospirosis will be triaged
under the Division of Adult Nephrology (Patients > 19 yo) or Pediatric
Nephrology (Patients < 18 yo and 364 days) with the following criteria:
1. Serum Creatinine: > 3 mg/ dl
2. Presence of any ONE of the Criteria for Pulse Therapy (See Appendix A)
28DOH Guidelines for Leptospirosis for Hospitals
III. ROLES AND RESPONSIBILITIES OF THE VARIOUS DEPARTMENTS /
DIVISIONS / SECTIONS IN THE MANAGEMENT OF A LEPTOSPIROSIS
UPSURGE
A. Emergency Room (ER)
Provide emergency medical treatment, triage patients and ensure
administrative or clinical backup for the ER.
Stamp clinical charts with “LEPTOSPIROSIS” so that the Pharmacy, CSSU
and other concerned areas will be alerted that the requests should be
provided, without pre-approval by MSSD.
Refer patients who fulfill the criteria for Leptospirosis immediately to
Nephrology or Internal Medicine. Patients developing acute kidney injury, who
fulfill the criteria for renal replacement will be treated without delay. This
should be provided to all patients and will not require MSSD pre-approval.
The Head of the ER should ensure that the Leptospirosis Prophylaxis Survey
2013 is completed for all patients and placed in the clinical chart of the patient.
The Chief Fellow of the Division of Adult Nephrology should collect the survey
forms including forms from Pediatric Nephrology and Internal Medicine. (See
Appendix B)
The Head Nurse of the ER shall ensure that the ER Procedure Room is
adequately prepared for use and will maintain adequate sterility for dialysis
access procedures. The appropriate measures to maintain sterility of the area
especially between procedures will be applied.
ER Nephrology fellows shall refer patients requiring access placement for
either hemodialysis (HD) or peritoneal dialysis (PD) to the Department of
Vascular Surgery / General Surgery. Placement of a temporary HD catheter
will be done either in the ER Procedure Room or Operating Room (OR) to
ensure that there is no delay in dialysis access placement. Placement of HD
access may also be performed by the Nephrology Fellow as per Division of
Adult Nephrology protocol. Placement of a temporary PD catheter will be done
in the OR only.
The Head Nurse of the ER shall ensure that there are enough supplies for
either HD or PD access placement, sufficient number of cut-down sets and
other supplies necessary at the ER. These should be provided to all patients
and will not require MSSD pre-approval. Any problems with supplies should be
communicated immediately to the Head of the Leptospirosis Upsurge
Management Team, Head of Warehouse, CSSU, and Purchasing.
- For HD access – use triple lumen catheters
- For intubation – use ET tube with subglottic suction
29DOH Guidelines for Leptospirosis for Hospitals
Residents and fellows shall refer patients to MSSD for completion of clinical
information for inclusion as a service patient, and for possible application for
the PhilHealth Leptospirosis benefit or other funding agencies to assist the
HEALTHCARE FACILITY in sourcing funds for these patients.
Residents and fellows shall refer patients who will require admission to the
clinical wards (for patients on inotropes, require ventilator support, or who are
clinically unstable) to the appropriate Medical Department/Division for
facilitation of admission, while all other patients will be admitted to the
Leptospirosis Ward.
B. Division of Internal Medicine
Assess patients and ensure that they are given adequate hydration,
appropriate antibiotics and that patients are monitored. The Division is also
responsible for following the Leptospirosis algorithm for proper diagnosis,
management and documentation. The ER Medical Residents on duty are in
charge of providing an efficient patient flow, consultation, and disposition at the
ER.
◊ Patients will be admitted to the appropriate pay or service beds as necessary.
The total daily number of patients admitted under the IM Service will be
reported to the post duty Senior Adult Nephrology Fellow who will be
responsible for consolidating the DAILY CENSUS of patients with
Leptospirosis.
Medical service residents will manage, monitor and provide proper medical
disposition of patients admitted under IM service. If necessary, the service
resident will transfer patients to nephrology service once the patient requires
intravenous methylprednisolone pulse therapy and renal replacement therapy.
Subspecialty service rotators will work in conjunction with nephrology fellows
to manage difficult and complicated Leptospirosis cases. Rotators are also
responsible for referring cases to the subspecialty consultant of the month.
Medical service residents assigned to the Leptospirosis Ward will be
responsible for answering urgent calls for patients admitted under IM service
in the Leptospirosis Ward, in the absence of a nephrology fellow, and promptly
refer to the service consultant.
Medical Staffing of the Leptospirosis Ward is seen in Section V.
30DOH Guidelines for Leptospirosis for Hospitals
C. Divisions of Adult and Pediatric Nephrology
Assess patients, provide renal replacement therapy / hydration as needed,
and ensure that appropriate medications are administered. Nephrology fellows
prioritize admissions based on the medical needs of patients. The NKTI is the
tertiary referral center for renal disease for all DOH hospitals and will accept
referrals from these hospitals for renal replacement. DOH hospitals with RRT
services referring patients to NKTI will be reported to the Head of the
Leptospirosis Upsurge Management Team and to DOH.
Patients who fulfill the criteria for renal replacement will be allocated to either
HD or PD according to the algorithm in Appendix A and C.
Since the patients are diagnosed with acute kidney injury, this illness is
reversible and all the needs for dialytic therapy, antibiotics and other
therapeutics will be provided.
The Division of Adult Nephrology will serve as the lead Department in
consolidating the census for all patients seen at the ER and admitted,
including basic demographics, treatment and outcome. (See Appendix D)
The post duty Senior Adult Nephrology Fellow will be responsible for
consolidating the 24-hour daily census of patients with Leptospirosis from all
Departments at 12:00AM using the appropriate form (See Appendix D). This
will be emailed to the Chief of Hospital, the Head of the Leptospirosis Upsurge
Management Team, the Chair of the Division of Adult Nephrology, and to the
Epidemiology Bureau and HEMB Operations Center, under the Department of
Health.
The PD Fellow 1 will be in charge of the Leptospirosis Ward and all the other
Leptospirosis patients during office hours. After office hours, the PD Fellow 2
will take over and endorse the patients back to PD Fellow 1 in the morning.
Nephrology Staffing of the Leptospirosis Ward is seen in Section V.
The Head of the Leptospirosis Upsurge Management Team will coordinate
with any of the concerned Departments/Divisions/Sections of HEALTHCARE
FACILITY, as needed, to ensure that patients are treated in a timely manner,
and to ensure that all the patients' needs are provided. The Head of the
Leptospirosis Upsurge Management Team will update the Chief of Hospital /
Deputy Executive Directors as necessary.
The Head of the Leptospirosis Upsurge Management Team and/or the Chief
of Hospital / Deputy Executive Directors, will attend the DOH-HEMB meetings,
as necessary, to provide updates on the status of patients admitted at the
HEALTHCARE FACILITY and to request for logistical support, if necessary.
Nephrology Staffing of the Leptospirosis Ward is seen in Section V.
31DOH Guidelines for Leptospirosis for Hospitals
D. HEALTHCARE FACILITY-Health Emergency Management Bureau (HEMB)
Team
The HEALTHCARE FACILITY-HEMB Team will be included in the
Leptospirosis Management Team. They will facilitate requests for augmentation
of staffing and resources as necessary from the DOH-HEMB Office or the Field
Implementation Coordination Team DOH-NCR. They will coordinate with the
Head of the Leptospirosis Upsurge Management Team for any other needs.
E. Division of Organ Transplantation and Vascular Surgery
Responsible in providing timely insertion of temporary HD catheters or PD
catheters and their removal, prior to patient’s final discharge and other surgical
procedures if deemed necessary.
F. Department of Pathology and Laboratory Medicine
Responsible for processing of blood chemistry, hematology, transfusion
requirements, microbiology, coagulation, and urinalysis available 24/7 for
patients with Leptospirosis.
Responsible for storage of blood for MAT, and to find out where these tests
can be done at the lowest possible price. Shall ensure that the required clinical
information is completed for the MAT tests.
G. Section of Pulmonary Medicine
Responsible for pulse oximetry, nebulization, arterial blood gas, and providing
mechanical ventilatory support in a timely manner.
The ECMO TEAM, headed by a Pulmonary consultant will decide whether or
not referred leptospirosis patients fulfill the criteria for ECMO therapy. Once a
patient is identified then the ECMO Team Head will activate the
HEALTHCARE FACILITY multi-disciplinary ECMO Team to provide the
necessary services for the patient. The ECMO Team head ensures the
availability of ECMO supplies such as oxygenator, cannulaes and various
tubings.
Medical criteria for assisted ventilation and ECMO therapy is seen in
Appendix E.
H. Department of Medical Imaging and Therapeutic Radiology
All radiologic services should be readily available to the ER, Leptospirosis and
medical wards for all diagnostic studies and services utilizing the portable x-
ray machine, ultrasound or CT scan as necessary.
32DOH Guidelines for Leptospirosis for Hospitals
I. Nursing Services
Assures that there is adequate nursing staffing complement, equipment,
medications and supplies, and that proper nursing care is provided.
In preparation for the activation of the Leptospirosis Upsurge Policy a 1-week
learning and development intervention on HD will be facilitated and scheduled
at least once a year or as necessary. A similar workshop for PD will be
facilitated at least once a year or as necessary to ensure that there are
sufficient nurses in the ward adept at PD. This comprises 8-hours of a lecture
workshop program and 40 hours of practicum.
Senior staff nurses will be identified from each ward to undergo the HD and/or
PD training as above. These nurses will be assigned to the Leptospirosis
Ward once opened, and new staff nurses will be assigned to replace them in
their respective units.
Nurse Staffing of the Leptospirosis Ward is seen in Section V.
J. Hemodialysis (HD) Unit
The HD Unit Head will determine whether HD machines will be placed in the
Leptospirosis Ward to facilitate HD treatments, so as not to disrupt the in-
patients and ER patients requiring urgent HD. The guideline is when there are
at least 16 patients requiring HD from the Leptospirosis Ward, 4-HD machine
stations will be set-up in the Ward with portable reverse osmosis machines.
Once a decision is made to set-up an HD Unit in the Leptospirosis Ward, the
HD Unit Supervisor will contact the HEALTHCARE FACILITY’s HD provider to
augment the number of HD machines and portable RO machines to be placed
in the Leptospirosis Ward, and contact the Provider’s Facility. Engineer and
Biomedical Engineer on duty to assess the area for setting up an HD Unit,
such as the water and power source.
The HD Unit Supervisor or Assistant will coordinate with all the wards where
there are Leptospirosis patients to determine how many patients need HD and
to schedule their treatments according to the prioritization level given by the
Division of Adult Nephrology, and where the patients will have their HD
treatments, ie. in the Leptospirosis Ward or in the HD Main Unit.
If an HD Unit will be set-up in the Leptospirosis Ward, the following will be put
in place:
- 1 Computer Station
- 1 Telephone Line
- Sufficient HD supplies and on and off dressing kits
33DOH Guidelines for Leptospirosis for Hospitals
The HD Charge Nurse and HD technicians will prepare and set-up the HD
Unit. The HD Unit Supervisor or Assistant will arrange for additional HD staff if
necessary, to ensure that the provision of HD is not disrupted.
An HD fellow should be present at all times when there are patients
undergoing HD in the Leptospirosis Ward.
All prescriptions for medications, supplies, dialysis orders and laboratories
shall be stamped with “LEPTOSPIROSIS” so that the Pharmacy and CSSU
will be alerted that the requests should be provided, without pre-approval by
MSSD.
K. Peritoneal Dialysis (PD) Unit
Once the Leptospirosis Upsurge Policy is activated, the PD Unit Supervisor
will contact the HEALTHCARE FACILITY’s PD Provider to augment the
number of PD cycler machines as needed, to accommodate the increased
number of patients who will be requiring PD and to request for additional PD
Nurses to assist the PD Unit in providing PD services.
The PD Unit Supervisor will ensure that there are sufficient supplies of PD
catheters, solutions and accessories at all times, in coordination with
Warehouse and Purchasing in all areas where Leptospirosis patients are
admitted, especially in the Leptospirosis Ward.
The PD Nurses will monitor all Leptospirosis patients who are started on PD
therapy, whether manual or cycler-assisted.
Patients will not be allowed to do their own PD exchanges while admitted in
the wards.
The PD nurses will ensure that PD is performed in a sterile manner and that
there is no PD-related infection.
The PD nurses will ensure that PD is done as prescribed, according to the
prescription of the Nephrologist.
The PD Nursing Attendant will assist the PD nurses in all activities related to
PD.
Once the patient is ordered discharged by Nephrology, the PD Nurse will
ensure that the patient is referred back to Vascular Surgery for removal of the
PD catheter prior to discharge. This should be performed in the OR. The PD
Nurse will ensure that the appropriate charges for PD catheter removal are
made.
34You can also read