Early Diagnosis of Dementia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Early Diagnosis of Dementia
KAREN S. SANTACRUZ, M.D., and DANIEL SWAGERTY, M.D., M.P.H.
University of Kansas Medical Center, Kansas City, Kansas
Until recently, the most significant issue facing a family physician regarding the diag-
nosis and treatment of dementia was ruling out delirium and potentially treatable eti- O A patient informa-
ologies. However, as more treatment options become available, it will become increas- tion handout on
ingly important to diagnose dementia early. Dementia may be suspected if memory dementia, provided by
an AAFP staff patient
deficits are exhibited during the medical history and physical examination. Informa- education writer, is
tion from the patient’s family members, friends and caregivers may also point to signs presented on page
of dementia. Distinguishing among age-related cognitive decline, mild cognitive 717.
impairment and Alzheimer’s disease may be difficult and requires evaluation of cogni-
tive and functional status. Careful medical evaluation to exclude treatable causes of
cognitive impairment is important. Patients with early dementia may benefit from for-
mal neuropsychologic testing to aid in medical and social decision-making. Follow-up
by the patient’s family physician is appropriate in most patients. However, a subspe-
cialist may be helpful in the diagnosis and management of patients with dementia
with an unusual presentation or following an atypical course. (Am Fam Physician 2001;
63:703-13,717-8.)
T
See editorial he prevalence of dementia is posed risk factors for dementia include a
on page 620. expected to increase dramati- family history of dementia, previous head
cally in future years as life ex- injury, lower educational level and female
pectancy continues to increase sex.2 Alzheimer’s disease is the most com-
and the baby-boomer popula- mon cause of dementia; many of the remain-
tion ages. The cumulative incidence of ing cases of dementia are caused by vascular
Alzheimer’s disease has been estimated to be disease and Lewy body disease. Vascular dis-
as high as 4.7 percent by age 70, 18.2 percent ease and Lewy body disease often occur in
by age 80 and 49.6 percent by age 90.1 Pro- combination with Alzheimer’s disease.3,4
TABLE 1
Signs and Symptoms That May Indicate the Need for Evaluation for Dementia
Cognitive changes Personality changes
New forgetfulness, more trouble understanding Inappropriate friendliness, blunting and disinterest,
spoken and written communication, difficulty social withdrawal, excessive flirtatiousness, easy
finding words, not knowing common facts such frustration, explosive spells
as the name of the current U.S. president, Problem behaviors
disorientation Wandering, agitation, noisiness, restlessness, being
Psychiatric symptoms out of bed at night
Withdrawal or apathy, depression, suspiciousness, Changes in day-to-day functioning
anxiety, insomnia, fearfulness, paranoia, abnormal Difficulty driving, getting lost, forgetting recipes
beliefs, hallucinations when cooking, neglecting self-care, neglecting
household chores, difficulty handling money,
making mistakes at work, trouble with shopping
Reprinted with permission from Rabins PV, Lyketsos CG, Steele CD. Practical dementia care. New York: Oxford
University Press, 1999:23.
FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 703diagnostic features are constant. They are well
Clinical Presentation described in the Diagnostic and Statistical
A practical approach to the diagnosis of Manual of Mental Disorders, 4th ed. (DSM-
dementia begins with the clinical recognition IV) and summarized in Table 2.6
of a progressive decline in memory, a decrease
in the patient’s ability to perform activities of HISTORY
daily living, psychiatric problems, personality The early diagnosis of dementia requires
changes and problem behaviors (Table 1).5 careful questioning to elicit clues to the pres-
While the clinical presentation of dementia ence of functional and cognitive impairment
may vary, depending on the etiology, the (Table 3).5 Interviewing friends as well as
TABLE 2
Criteria for the Diagnosis of Alzheimer’s Type Dementia
and Age-Related Cognitive Decline
The rightsholder did not
grant rights to reproduce
this item in electronic
media. For the missing
item, see the original print
version of this publication.
704 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp VOLUME 63, NUMBER 4 / FEBRUARY 15, 2001Early Dementia
family members is helpful, because family
members may have adopted coping strategies Testing for a variety of cognitive abnormalities, including
to help the patient with dementia, which
aphasia, apraxia, agnosia and executive functioning, may be
sometimes conceal the patient’s impairment,
making early diagnosis difficult. For example, useful in the evaluation of early dementia.
a caregiver may take on additional responsi-
bilities such as shopping and financial man-
agement, possibly masking the patient’s level evaluating cognitive function. Their use may
of impairment. or may not be required in the evaluation of
During the medical history-taking, ques- early dementia.
tions should be asked about forgetfulness
and orientation. Inquiries should also be PHYSICAL EXAMINATION AND COGNITIVE TESTING
made regarding activities of daily living, The findings of the physical examination
including instrumental activities such as may suggest an etiology for dementia. For
everyday problem solving and handling of example, dementia resulting from vascular
business and financial affairs. Independent disease may be accompanied by focal neuro-
functioning in community affairs, such as logic findings.
job responsibilities, shopping and participa- Physical examination should include
tion in volunteer and social groups, should assessment of cognitive domains, including
be assessed. Evidence of problems with speech (aphasia), motor memory (apraxia),
home activities, hobbies and personal care sensory recognition (agnosia) and complex
should also be sought. In the early stages of behavior sequencing (executive function-
dementia, the patient may show restricted ing). Aphasia may be detected by asking the
interest in hobbies and other activities, and patient to name body parts or objects in the
may require prompting to maintain per- room. Frequent use of vague terms such as
sonal hygiene. 7 “thing” and “it” may also signify deteriora-
A variety of rating scales are available for tion of language function. An example of a
TABLE 3
Symptom Checklist in the Evaluation of Dementia
The rightsholder did not
grant rights to reproduce
this item in electronic
media. For the missing
item, see the original print
version of this publication.
FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 705test for apraxia is to ask the patient to pan- his or her eyes and then placing an object,
tomime the use of a common object such as such as a key or a coin, in the patient’s hand
a hammer or a toothbrush. Agnosia can be and asking the patient to identify it without
evaluated by first asking the patient to close looking at it. Inability to recognize a com-
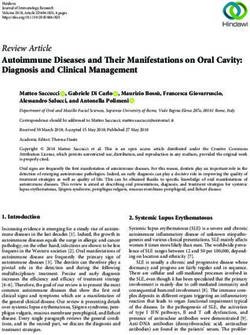
Mini-Mental State Examination
Maximum
score Score
Orientation
5 _____ What is the (year) (season) (date) (day) (month)?
5 _____ Where are we: (state) (county) (town or city) (hospital) (floor)?
Registration
3 _____ Name three common objects (e.g., “apple,” “table,” “penny”):
Take one second to say each. Then ask the patient to repeat all three after you
have said them. Give one point for each correct answer. Then repeat them until
he or she learns all three. Count trials and record.
Trials: ____
Attention and calculation
5 _____ Spell “world” backwards. The score is the number of letters in correct order.
(D___L___R___O___W___)
Recall
3 _____ Ask for the three objects repeated above. Give one point for each correct answer.
(Note: recall cannot be tested if all three objects were not remembered during
registration.)
Language
2 _____ Name a “pencil” and “watch.”
Repeat the following: “No ifs, ands or buts.”
1 _____ Follow a three-stage command:
3 _____ “Take a paper in your right hand, fold it in half and put it on the floor.”
Read and obey the following:
1 _____ Close your eyes.
1 _____ Write a sentence.
1 _____ Copy the following design.
Total
score: _____
FIGURE 1. The Mini-Mental State Examination, a useful tool for assessing cognitive function and
documenting subsequent decline. Scores of 24 or higher are generally considered normal; see
Table 4 for education and age norms.
Adapted with permission from Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method
for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:196-8, and Cockrell JR,
Folstein MF. Mini-mental state examination (MMSE). Psychopharm Bull 1988;24(4):689-92.
706 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp VOLUME 63, NUMBER 4 / FEBRUARY 15, 2001Early Dementia
mon object despite normal sensory function
signifies agnosia. Serial Mini-Mental State examinations (or other cognitive
Asking the patient to perform a series of
testing) can help document changes over time.
simple tasks is a way to evaluate executive
functioning. For example, the patient can be
asked to put a piece of paper in his or her
right hand, fold it in half and put it on the unnecessary medications and optimize treat-
floor. This task would be difficult for a patient ment of chronic diseases, physical examina-
with impairment in the ability to plan, initi- tion and laboratory tests are recommended to
ate, sequence and monitor complex behavior. rule out specific treatable causes of dementia.
Asking the patient to perform serial subtrac- Hearing or vision deficits, hypothyroidism,
tion of 7s (backward from 100 to 65), to spell vitamin B12 deficiency and depression are
the word “world” backward and to produce among the disorders that can cause symptoms
verbal word lists, such as names of animals or of dementia. Such disorders are relatively easy
items in a grocery store, are other ways to test to detect and should be excluded by appropri-
executive functioning and abstract thinking. ate laboratory tests, physical examination and
Although the Mini-Mental State Examina- psychologic tests. Electrocardiography and
tion (MMSE) is not diagnostic of dementia chest radiography can sometimes be useful to
and does not distinguish well between vari- rule out treatable systemic diseases, although
ous confusional states,8 it is useful for assess-
ing cognitive function and documenting
subsequent decline (Figure 1). Because judg- TABLE 4
ment and insight are not tested by the Median Scores on Mini-Mental State Examination
MMSE, many clinicians ask additional ques- by Age and Educational Level
tions to assess these aspects of cognition.
Judgment and insight can be assessed, for Educational level
example, by asking the patient, “What would
you do if you were in a crowded building and Age (years) 4th grade 8th grade High school College
smelled smoke?” 18 to 24 22 27 29 29
When conversational skills are well pre- 25 to 29 25 27 29 29
served, an early decline in memory may be 30 to 34 25 26 29 29
difficult to detect, especially during a short, 35 to 39 23 26 28 29
focused office visit. The MMSE can detect 40 to 44 23 27 28 29
cognitive impairment by evaluating orienta- 45 to 49 23 26 28 29
tion, attention, recall, language and ability to 50 to 54 23 27 28 29
follow commands. A score higher than 23 is 55 to 59 23 26 28 29
generally considered normal, although per- 60 to 64 23 26 28 29
formance varies with the patient’s age and 65 to 69 22 26 28 29
education (Table 4).9 70 to 74 22 25 27 28
75 to 79 21 25 27 28
Differential Diagnosis 80 to 84 20 25 25 27
Figure 2 summarizes an approach to the > 84 19 23 26 27
early diagnosis of dementia. If dementia is
suspected, a medication review and assess- Reprinted with permission from Crum RM, Anthony JC, Bassett SS, Folstein MF.
ment for chronic disease processes are war- Population-based norms for the mini-mental state examination by age and edu-
ranted. If no improvement occurs after appro- cational level. JAMA 1993;18:2386-91.
priate measures are taken to eliminate
FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 707Diagnostic Work-Up of Dementia
Presence of symptoms suggestive of dementia, including
changes in activities of daily living or caregivers’ concerns
Perform clinical assessment, including history, physical examina-
tion, functional status and cognitive testing such as MMSE.
Deficits detected on clinical assessment
Perform assessment for treatable causes of dementia, including
medication review, depression screening and laboratory testing.
Yes
Any treatable abnormalities present? Treat abnormalities and reassess.
No
Do symptoms of possible dementia remain?
Do the findings meet criteria
for diagnosis of dementia? Yes
No
Provide reassurance.
No Yes
Is mild cognitive impairment present? Are atypical features of dementia present?
No Yes No Yes
Provide reassurance; Consider referral to a Diagnose Alzheimer’s Consider referral to a
reassess in 6 months. subspecialist and/or disease, vascular subspecialist; provide
neuropsychologic testing; dementia, etc. close follow-up.
reassess in 6 months.
Provide counseling about expected
course and treatment options.
FIGURE 2. An approach to the early diagnosis of dementia. (MMSE = Mini-Mental State Examination)
their necessity should be guided by the history virus (HIV) status, urine check for heavy met-
and physical examination. als and toxicology screening may be indicated
Table 5 lists laboratory tests to consider in in a minority of cases (Table 6).5
the evaluation of dementia. Tests recom- Lumbar puncture is usually not necessary
mended for the diagnostic work-up of except when the onset of dementia occurs
dementia include a complete blood cell count before 55 years of age or when a specific con-
(to exclude anemia and infection), urinalysis dition such as infection, syphilis or vasculitis
(to exclude infection), serum electrolyte, glu- is suspected.10 However, in at least one
cose and calcium levels, blood urea nitrogen, prospective study it was found that cere-
serum creatinine level and liver function tests brospinal fluid analysis for the 42 amino acid
(to investigate metabolic disease).10 Syphilis form of -amyloid may be suggestive of
serology, erythrocyte sedimentation rate, Alzheimer’s dementia, although not diagnos-
serum folate level, human immunodeficiency tic.11 Further studies into the existence of bio-
708 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp VOLUME 63, NUMBER 4 / FEBRUARY 15, 2001Early Dementia
markers for the diagnosis of early Alzheimer’s
disease are ongoing. TABLE 5
The utility of computed tomography or Laboratory Tests for Evaluation of Dementia
magnetic resonance imaging to rule out vas-
cular disease, tumor, subdural hematoma or Urinalysis and microscopy Erythrocyte sedimentation rate*
normal-pressure hydrocephalus remains con- Complete blood cell count Serologic tests for syphilis (or similar)
Serum electrolyte levels, including Chest radiography*
troversial. Radiologic imaging of the central
magnesium Electrocardiography*
nervous system is probably not necessary in Serum chemistry panel, including liver Toxicology screening*
patients presenting with dementia, unless function tests Urine toxicology
localizing neurologic signs or symptoms are Thyroid function tests Serum toxicology (alcohol,
noted. Clearly, it is important to search for a Serum vitamin B12 salicylates, other)
reversible cause of dementia. However, in one
meta-analysis it was revealed that fewer than *—To be considered, not universally needed.
11 percent of patients with cognitive decline Reprinted with permission from Rabins PV, Lyketsos CG, Steele CD. Practical
had partially or fully reversible disease.12 dementia care. New York: Oxford University Press, 1999:46.
Diagnosis
DEMENTIA
DSM-IV criteria for the diagnosis of demen- criteria for dementia. In order to fulfill DSM-
tia require the presence of multiple cognitive IV criteria, cognitive impairment must be of
deficits in addition to memory impairment6 the degree that social or occupational function
(Table 1). Early in the disease, memory impair- is reduced, with the functional impairment
ment may be the only clinical finding, and this representing a decrease in the patient’s normal
single finding would not meet the diagnostic ability.
TABLE 6
Additional Tests to Consider in the Diagnostic Work-Up of Dementia
Test Indication
Electroencephalography Possible seizures; Creutzfeldt-Jakob disease
Lumbar puncture Onset of dementia within the preceding six months; dementia rapidly
progressive
Heavy metal screen History of potential exposure
Human immunodeficiency virus History of potential exposure
Lyme disease titer History of exposure and compatible clinical picture
Ceruloplasmin, arylsulfatase, Wilson’s disease, metachromatic leukodystrophy, multiple myeloma
electrophoresis
Slit lamp examination History and examination suggest Wilson’s disease
Apolipoprotein E Need to increase likelihood that diagnosis of Alzheimer’s disease is correct
Genetic testing for Alzheimer Family history is strong, and confirmation is clinically necessary
genes, other dementia genes
Reprinted with permission from Rabins PV, Lyketsos CG, Steele CD. Practical dementia care. New York: Oxford
University Press, 1999:47.
FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 709to describe a condition that may or may not
Referral to a subspecialist may be warranted when the eventually lead to dementia.13 One study
showed that patients with mild cognitive
presentation or clinical course is atypical of dementia.
impairment had a more rapid decline in cog-
nitive function than control patients, but a
less rapid decline than patients with mild
AGE-RELATED COGNITIVE DECLINE AND MILD Alzheimer’s disease.15
COGNITIVE DISORDER The definitions of and the distinctions
Age-related cognitive decline is character- between mild cognitive disorder, age-associ-
ized by memory loss without other cognitive ated cognitive decline and mild cognitive
problems (the DSM-IV criteria are described impairment are controversial. Referral for
in Table 2). If memory deficit is present but the more extensive neuropsychologic testing,
other diagnostic criteria for dementia are not, with follow-up intervals of six to nine
a diagnosis other than dementia should be months, is warranted in patients with mild or
considered.6 A disorder similar to age-related borderline cognitive deficits.16
cognitive decline is described as “mild cogni-
tive disorder” in the World Health Organiza- Referral
tions ICD-10 classification (International Sta- The decision to refer the patient with
tistical Classification of Diseases, 10th rev.).13 recently diagnosed dementia to a subspecialist
The diagnosis of mild cognitive disorder is influenced by both practical and medical
can be made if the cognitive decline is tempo- considerations. Many family physicians choose
rally related to cerebral or systemic disease. to follow their patients with dementia even
Otherwise, the diagnosis of age-related cogni- when clinical features are atypical or suggestive
tive decline should be considered. According of less common etiologies for the dementia.
to the DSM-IV, age-related cognitive decline However, a neurologist or psychiatrist can
represents cognitive changes that are within sometimes assist in the diagnosis and care of
normal limits given the person’s age. Age- patients with less common dementias, includ-
associated cognitive decline is characterized ing Pick’s disease, dementia of frontal lobe
by a decline in only one of the five broad neu- type, dementia with Lewy bodies, progressive
ropsychologic domains associated with supranuclear palsy, multiple-systems atrophy
dementia: memory and learning; attention and normal-pressure hydrocephalus. Consen-
and concentration; thinking; language; and sus criteria have been established for the diag-
visuospatial functioning.14 According to the noses of dementia with Lewy bodies and vas-
International Psychogeriatric Association,14 cular, or multi-infarct, dementia (Table 7).17,19
additional criteria should be met to make a Symptoms that may be helpful in identifying
diagnosis of age-related cognitive decline. the less common causes of dementia include
These criteria include the report of cognitive significant personality changes, extrapyrami-
decline from a reliable source, a gradual onset dal signs, rapid progression, gaze palsy,
of at least six months’ duration and a score of parasympathetic abnormalities, cerebellar
more than one standard deviation below the signs, early urinary incontinence and gait
norm on standardized neuropsychologic test- abnormalities. Other reasons for referral to a
ing such as the MMSE. neurologist or psychiatrist include rapidly
progressive dementia, dementia in a young
MILD COGNITIVE IMPAIRMENT patient or the presence of psychiatric comor-
The diagnosis of mild cognitive impair- bidities or severe behavior disturbances.
ment is difficult and controversial. The term In a nonresearch setting, neuropsychologic
“mild cognitive impairment” has been coined testing is not considered necessary if the diag-
710 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp VOLUME 63, NUMBER 4 / FEBRUARY 15, 2001Early Dementia TABLE 7 Features of Multi-Infarct Dementia and Dementia with Lewy Bodies Multi-infarct dementia The characteristic features include stepwise deterioration and patchy distribution of deficits, focal neurologic signs and evidence of vascular disease as indicated by history, physical examination and laboratory testing. MODIFIED HACHINSKI ISCHEMIA SCORE: POINTS Abrupt onset . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Stepwise progression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Fluctuating course . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Nocturnal confusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Relative preservation of personality . . . . . . . . . . . . . . . . . . . . . . . . 2 Depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Somatic complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Emotional incontinence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 History of hypertension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 History of stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Focal neurologic signs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Focal neurologic symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 SCORING:Dementia is not likely to be due to vascular causes if the total score is 4 or less; dementia is likely to be due to vascular causes if the total score is 7 or more. Dementia with Lewy bodies The central feature is progressive cognitive decline with resultant functional impairment. Persistent memory impairment may occur with disease progression. Deficits on tests of attention, frontal–subcortical skills and visuospatial ability may be prominent. ESSENTIAL FEATURES FOR DIAGNOSIS: Two of the following core features are essential for a diagnosis of probable dementia with Lewy bodies; one is essential for possible dementia with Lewy bodies. • Fluctuating cognition and pronounced variations in attention and alertness • Recurrent visual hallucinations that are typically well formed and detailed • Spontaneous motor features of parkinsonism FEATURES SUPPORTIVE OF THE DIAGNOSIS: Repeated falls Syncope Transient loss of consciousness Neuroleptic sensitivity Systematized delusions Hallucinations SCORING:A diagnosis of dementia with Lewy bodies is less likely in the presence of the following: Stroke disease, evident as focal neurologic signs or on brain imaging Evidence of any physical illness or other brain disorder sufficient to account for the clinical picture Modified Hachinski ischemia score adapted with permission from Rosen WG, Terry RD, Field PA, et al. Patho- logical verification of ischemic score in differentiation of dementias. Ann Neurol 1980;7:486-8. Criteria for dementia with Lewy bodies adapted with permission from McKeith IG, Galasko D, Kosaka K, et al. Consen- sus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the con- sortium on DLB international workshop. Neurology 1996;47:1113-24. FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 711
nosis of dementia can be made using standard labeled for the symptomatic treatment of
criteria. In general, neuropsychologic testing is Alzheimer’s disease. Acetylcholinesterase in-
indicated when patients with abnormal find- hibitors act by delaying neurotransmitter de-
ings on the mental state examination show gradation, thereby enhancing cortical cholin-
normal physical functioning and when the ergic activity.
index of suspicion is clinically high but screen- Clinical trials in patients with mild to mod-
ing tests are normal.16 Neuropsychologic tests erate dementia suggest that symptomatic
evaluate a wide variety of intellectual domains, improvement is possible.20,21 Cholinergic side
including the level of arousal, attention and effects, such as nausea, vomiting and diar-
orientation, recent and remote memory, lan- rhea, are usually transient but may be intoler-
guage, praxis, visuospatial function, calcula- able to some patients. Monitoring of serum
tions and judgment. Although there are pub- transaminase levels is recommended with use
lished norms for most of the commonly used of tacrine because of potential hepatotoxicity.
standardized tests, the tests are not always Experimental treatment options, some with
definitive. Serial examination may be neces- potentially fewer side effects than those asso-
sary. Neuropsychologic tests may also be useful ciated with currently available agents, may
in determining competency for legal purposes, soon be available for the treatment of
in distinguishing dementia from depression Alzheimer’s disease.
and in helping the patient make important The primary management strategy for pro-
decisions regarding jobs and finances. gressive dementia is to preserve function and
independence, and to maintain quality of life
Management and Treatment for as long as possible. Frequent (every three
Early diagnosis and intervention allow the to six months) clinic visits may be indicated to
patient to compensate for the disability, mini- achieve these goals by maximizing the
mize disease-related and medication compli- patient’s general health and interacting with
cations, improve quality of life and optimize caregivers to optimize the patient’s social envi-
the use of resources. While new experimental ronment. Nonpharmacologic interventions,
cholinergic drugs for the treatment of Alz- including measures to ensure safety at home
heimer’s disease are introduced periodically, and long-term decisions regarding finances, a
tacrine (Cognex) and donepezil (Aricept) are living will and nursing home placement, are
the only cholinesterase inhibitors currently often important considerations.
The management of vascular dementia
consists of controlling risk factors such as
The Authors hypertension and smoking. The use of anti-
coagulants is indicated in many of these
KAREN S. SANTACRUZ, M.D., is an assistant professor in the departments of pathol-
ogy and neurology at the University of Kansas School of Medicine, Kansas City. She patients. Because of its safety, aspirin is the
completed a residency at the University of California, Irvine, Medical Center, where she most commonly used agent. Use of warfarin
trained in anatomic pathology and neuropathology. She developed an interest in (Coumadin) may also be considered in a lim-
dementia through her interaction with the Alzheimer’s Disease Research Center at the
University of California, Irvine. ited number of patients, such as those with-
out a significant risk of falling but with a def-
DANIEL SWAGERTY, M.D., M.P.H., is an assistant professor in the departments of fam-
ily medicine and internal medicine in the University of Kansas School of Medicine. He inite history of stroke.
is also associate director of the Center on Aging at the University of Kansas. Dr. Swa- The treatment of dementia with Lewy bod-
gerty completed medical school, a family practice residency and a geriatric medicine ies has not been well studied. However, it is
fellowship at the University of Kansas School of Medicine. He also completed a mas-
ter’s degree in public health at the University of Kansas School of Medicine. important to note that parkinsonian features
in these patients rarely respond to dopamin-
Address correspondence to Karen S. SantaCruz, M.D., Department of Pathology, Uni-
versity of Kansas School of Medicine, 3901 Rainbow Blvd., Kansas City, KS 66160- ergic drugs, and that adverse responses to
7410. Reprints are not available from the authors. neuroleptic agents may occur.22
712 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp VOLUME 63, NUMBER 4 / FEBRUARY 15, 2001Early Dementia
state”: a practical method for grading the cogni-
Final Comment tive state of patients for the clinician. J Psychiatr
Res 1975;12:189-98.
Physicians and patients can obtain infor- 9. Crum RM, Anthony JC, Bassett SS, Folstein MF.
mation about potential experimental treat- Population-based norms for the Mini-Mental State
Examination by age and educational levels. JAMA
ment options and ongoing clinical trials at the 1993;18:2386-91.
Alzheimer’s Disease Education and Referral 10. Report of the Quality Standards Subcommittee of
(ADEAR) Center Web site (www.alzheimers. the American Academy of Neurology. Practice
parameter for diagnosis and evaluation of demen-
org) or through an Alzheimer’s disease infor- tia. Neurology 1994;44:2203-6.
mation specialist at ADEAR (800-438-4380). 11. Andreason N, Hesse C, Davidson P, Minthon L,
The ADEAR Center is a service of the Wallin A, Winblad B, et al. Cerebrospinal fluid
beta-amyloid(1-42) in Alzheimer’s disease: differ-
National Institute on Aging (NIA). ences between early- and late-onset Alzheimer dis-
Although no method of curing or arresting ease and stability during the course of disease.
Alzheimer’s disease is currently available, Arch Neurol 1999;56:673-80.
12. Clarfield AM. The reversible dementias: do they
early diagnosis is important for several rea-
reverse? Ann Intern Med 1988;109:476-86.
sons. The most compelling reason is that 13. World Health Organization. The ICD-10 classifica-
early diagnosis allows the patient and family tion of mental and behavioral disorders. Geneva:
to plan for the future and identify outside World Health Organization, 1992:64-5.
14. Levy R. Aging-associated cognitive decline. Work-
sources of assistance. Moreover, as potentially ing Party of the International Psychogeriatric Asso-
useful and proven treatments become avail- ciation in collaboration with the World Health
able, early diagnosis of dementia will become Organization. Int Psychogeriatr 1994;6:63-8 [Pub-
lished erratum in Int Psychogeriatr 1994;6:133].
increasingly important. Although screening 15. Peterson RC, Smith GE, Waring SC, Ivnik RJ, Tan-
all elderly patients for dementia is not war- gelos EG, Kokmen E. Mild cognitive impairment:
ranted,23 being alert for cognitive and func- clinical characterization and outcome Arch Neurol
1999;56:303-8 [Published erratum in Arch Neurol
tional decline is a prudent way of recognizing 1999;56:760].
dementia in its early stage. 16. Daly MP. Diagnosis and management of Alzheimer
Disease. J Am Board Fam Pract 1999;12:375-85.
17. McKeith IG, Galasko D, Kosaka K, Perry EK, Dick-
REFERENCES
son DW, Hansen LA, et al. Consensus guidelines
1. Hebert LE, Scherr PA, Beckett LA, Albert MS, Pil- for the clinical and pathologic diagnosis of demen-
grim DM, Chown MJ, et al. Age-specific incidence tia with Lewy bodies (DLB): report of the consor-
of Alzheimer’s disease in a community population. tium on DLB international workshop. Neurology
JAMA 1995;273:1354-9. 1996;47:1113-24.
2. Larson EB, Kukull WA, Katzman RL. Cognitive 18. Chui HC, Victoroff JI, Margolin D, Jagust W,
impairment: dementia and Alzheimer’s disease. Shankle R, Katzman R. Criteria for the diagnosis of
Annu Rev Public Health 1992;13:431-49. ischemic vascular dementia proposed by the State
3. Bachman DL, Wolf PA, Linn R, Knoefel JE, Cobb J, of California Alzheimer’s Disease Diagnostic Treat-
Belanger A, et al. Prevalence of dementia and ment Centers. Neurology 1992;42:473-80.
probable senile dementia of the Alzheimer type in 19. Rosen WG, Terry RD, Fuld PA, Katzman R, Peck A.
the Framingham Study. Neurology 1992;42:115-9. Pathological verification of ischemic score in differ-
4. Collerton D, Davies C, Thompson P. Lewy body entiation of dementias. Ann Neurol 1980;7:486-8.
dementia in clinical practice. In: Perry RH, McKeith 20. Rogers SL, Farlow MR, Doody RS,Mohs R, Friedhoff
IG, Perry EK, eds. Dementia with Lewy bodies: clin- LT. A 24-week, double-blind, placebo-controlled
ical, pathological, and treatment issues. New York: trial of donepezil in patients with Alzheimer’s dis-
Cambridge University Press, 1996:171-86. ease. Neurology 1998;50:136-45.
5. Rabins PV, Lyketsos CG, Steele CD. Practical demen- 21. Sano M, Ernesto C, Thomas RG, Klauber MR, Schafer
tia care. New York: Oxford University Press, 1999. K, Grundman M, et al. A controlled trial of selegiline,
6. American Psychiatric Association. Diagnostic and alpha-tocopherol, or both as treatment for Alz-
statistical manual of mental disorders. 4th ed. heimer’s disease. N Engl J Med 1997;336:1216-22.
Washington, D.C.: American Psychiatric Associa- 22. McKeith I, Fairbairn A, Perry R, Thompson P, Perry E.
tion, 1994:123-63,684. Neuroleptic sensitivity in patients with senile
7. Morris JC. The clinical dementia rating (CDR): cur- dementia of Lewy body type. BMJ 1992;305:673-8.
rent version and scoring rules. Neurology 1993; 23. U.S. Preventive Services Task Force. Guide to clini-
43:2412-4. cal preventive services. 2d ed. Baltimore: Williams
8. Folstein MF, Folstein SE, McHugh PR. “Mini-mental & Wilkins, 1996.
FEBRUARY 15, 2001 / VOLUME 63, NUMBER 4 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 713You can also read